
Abstract
As the molecular pathobiology of immunologically based diseases, such as rheumatoid arthritis, has become clearer, pharmaceutical researchers have responded with highly efficacious and selective biological compounds. In contrast to older, nonspecific small-molecule therapeutics, the exquisite species sensitivity of monoclonal antibodies has introduced new challenges to preclinical safety studies. Repeated exposure of animals to biopharmaceutical compounds tends to be restricted in the species in which these compounds have pharmacological action, and it tends to stimulate antidrug immune responses with acceleration of clearance, thereby limiting the duration of repeat-dose studies and potentially resulting in hypersensitivity reactions. Thus, the safety testing of biopharmaceutical compounds has necessitated the use of relatively short-term studies in rodents, whereas nonhuman primates have become the primary tool for large-animal, repeat-dose studies. However, as the number of highly targeted and efficacious small-molecule immunomodulators rapidly increases, these molecules will be developed in a manner similar to that of other small molecules with regard to safety assessment. Because such approaches inherently push drug levels to achieve maximally tolerated doses, the pharmacologic specificity of these new small-molecule drugs may be lost as they affect additional receptors and pathways. Therefore, toxicologic pathologists must refamiliarize themselves with the consequences of profound immunosuppression in species other than nonhuman primates. The interrelationships of cytokine signaling and receptor biology are complex, highly integrated, and at times paradoxical, and the loss of specificity at high doses may result in unforeseen consequences caused by the impact on complex down-stream pathways that culminate in exaggerated and adverse responses. The species specificity of such responses may not be inherently familiar or anticipated.
The application of more sophisticated molecular techniques continues to rapidly broaden our understanding of the many complex and interwoven pathways involved in biological homeostasis. The recognition of highly specific molecular targeting of select biologic pathways is now the cornerstone identifying new efficacious drugs. Problematic to this rapidly evolving world of therapeutics is the challenge of finely tuning the specificity of sophisticated, targeted small-molecule compounds while avoiding excessive pharmacology and/or off-target effects.
Intentional therapeutic immunomodulation is the “poster child” of this dilemma. Researchers continue to attempt to carefully modify immune responses that have evolved to protect the host from microbe-mediated disease and cancer, but overactivation of these immune responses results can lead to highly destructive and sometimes life-threatening conditions. Further complicating the clear delineation of risk associated with intentional immunomodulation is the specter of classic immunotoxicology, a scientific discipline derived from the concerns of chronic environmental exposure of humans to chemicals that have a direct or indirect impact on the immune system. In fact, many of the assays that identify perturbed immune responses that we use today to categorize immunotoxicity may, in another venue, be used as indicators and measures of expected pharmacology.
The first step in dealing with this dilemma of unintended immunotoxicity versus intended immunomodulation is to review the basics and work from there. For example, in the case of intended immunomodulation, is the effect of such a therapeutic a hazard or a risk? Using the paradigm originally designed to address immunotoxicity of environmental and industrial chemicals, we can consider the following:
The “hazard” associated with a chemical is its intrinsic ability to cause adverse effects.
The “risk” is the probability that such effects will occur in the various applications in which the chemical will be used and discharged (exposure scenarios).
For a chemical, risk assessment takes into account both the hazards of that chemical and the exposure to it (both human and the environment).
In the case of intended immunomodulation it would appear that because we are intentionally reducing a biologically essential mechanism, we must also acknowledge the hazard and accept the risk as we pursue the intended pharmacological (PD) effect. But when does this intended PD go too far? Or put another way, what is too much immunomodulation? Simplistically, it is:
When it (immunomodulation) fulfills the definition for immunotoxicity
Or more importantly,
When the risk of immunotoxicity exceeds the benefits of immunomodulation
In the end, an immunomodulatory effect is considered adverse or immunotoxic if it impairs humoral or cellular immunity needed by the host to defend itself against infectious or neoplastic disease, or when it causes unnecessary and or unexpected tissue damage.
To help sort out this question, there are a number of in vivo animal studies that can be conducted. But as data are accumulated, additional questions need to be asked to guide the ultimate decision of proceeding with the therapy being considered, such as:
Are there species differences in either the structure and function of the immune system or metabolism, and how do such differences relate to risk assessment in humans?
Does immunological redundancy balance the ability of the host to maintain immunologic integrity when a single arm of the immune response is affected, thereby reducing the risk?
Do pharmacologically induced changes to the immune structure and function resulting from small molecules constitute significant risk?
Can an integrated assessment of all related data provide a meaningful perspective for risk assessment?
Building on the experiences of environmental or occupational exposure to chemicals, international debate and ultimately internationally recognized immunotoxicity guidelines for human pharmaceuticals have significantly contributed to our ability to address the question at hand. An often referenced guideline in this discussion is the ICH S8: Immunotoxicity Studies for Human Pharmaceuticals (2005). However, it must be remembered that this guideline does not address what must be done for intended immunomodulators, but rather it is focused on the unexpected and unintentional effects of new drugs on the immune system. To that end, the guidance states:
All new investigational drugs should be evaluated for the potential to produce unintended immunosuppression.
Methods include standard toxicity studies (STS) and additional immunotoxicity studies conducted as appropriate.
Whether additional immunotoxicity studies are appropriate should be determined by a weight of evidence review of cause(s) for concern.
During the debate concerning how best to identify, address, and predict the biological effects of immunomodulators, studies were ongoing with potent, relatively nonspecific and broadly immunosuppressive drugs such as corticosteroids and other potent drugs to prevent transplant rejection. Out of this clinical experience has come a grudging acceptance for opportunistic infections and cancer as potential secondary outcomes to be clinically managed, all the while maintaining a close eye on the risk-benefit balance. It has been assumed by some that with improved selectivity and targeting, the number and diversity of secondary complications will be reduced. However, the methods for preclinical safety assessment continue as before, including the mandate to perform high-dose and repeat-dose toxicity studies to evaluate for both on-target and off-target toxicity. At high doses, the exquisite selectivity designed into many small molecules by chemists can be lost and myriad unexpected consequences can occur as multiple overlapping pathways become affected. So despite optimism for improved clinical profiles, the toxicologist and pathologist must still deal with a plethora of outcomes, and hopefully they will be able to put them in the most appropriate category for establishing human risk. In fact, the ability to accurately observe, integrate, and understand the complex pathobiology of immune dysregulation rests in the hands of toxicologic pathologists more than anyone else.
To further complicate matters, the challenge of identifying the risk of excessive immunomodulation is different between large biological molecules and small molecules. Cynomolgus monkeys and other nonhuman primates (NHP) have been used as the large animal of choice in toxicity studies of large biological molecules in the hope that NHP genetic similarity with humans will more accurately demonstrate the desired biological activity of the molecule and allow accurate assessment of toxicity. However, repeated dosing with monoclonal antibodies may still result in immune-mediated clearance with accelerated elimination of drug, thus interfering with the ability to characterize the consequences of chronic, repeated exposure. The recent emergence of new, highly target-specific, small-molecule immunomodulatory drugs has allowed the use of dogs as an alternative to NHP because of the ability to pursue the full spectrum of repeat-dose chronic studies. Nevertheless, both species bring with them their own “baggage” of background flora and potentially opportunistic organisms. It is essential that the toxicologic pathologist be knowledgeable of the numerous pathogens, their biology, and how they are expressed for both species.
So what can observations in Specific Pathology Free rodents and/or colony-reared (as compared with free-ranging) animals tell us about the risk of specific infections and related outcomes in man? Is it possible to generically detect excessive immunomodulation? If we see increased incidences of opportunistic infections in animals, what does this increase say about the risk of the same thing happening in humans?
First Steps
The first steps in evaluating affects on the immune system are well described within published guidance, Best Practices, and review articles. Taken together, these documents form the backbone of an effective and rigorous approach to characterizing effects on immune structure and function.
For the sake of this discussion, we will focus on the ICHS8 Guidance and STP Position Paper: Best Practice Guideline for the Routine Pathology Evaluation of the Immune System. The ICH S8: Immunotoxicity Studies for Human Pharmaceuticals (2005) is designed to identify unexpected effects on the immune system (such a statement is clearly expressed in the document), but it is clear that it is possible to also use the approaches described therein to identify and semiquantify effects on the immune system, unintentional as well as intentional. When combined with the STP Position Paper: Best Practice Guideline for the Routine Pathology Evaluation of the Immune System (Haley et al. 2005), a thorough and stepwise approach that integrates histological examination of lymphoid tissues, organ weights, and clinical pathology end points emerges.
Rodents
It is perhaps in rodents that the aforementioned documents are most helpful. In addition to the documents noted above, every pathologist who examines lymphoid tissues should have a copy of A Monograph on Histomorphologic Evaluation of Lymphoid Organs (Maronpot 2006) next to his or her microscope. This entire issue is an excellent treatise on the normal and abnormal histopathology of lymphoid organs of rodents and integrates numerous histological examples with the techniques and terminology consistent with the STP Position Paper noted above.
Given the relative lack of opportunistic pathogens, the pathologist must rely on the approaches described therein to identify effects on the immune system and what their long-term impact may be. An integrated evaluation of changes in circulating lymphocytes, alterations of organ weights, and changes in lymph node and/or spleen cellularity can provide insight as to the possible adverse effects on the immune system.
Although there are many rodent pathogens, spontaneous infections should rarely be encountered in rodent colonies maintained under SPF conditions. Identification during a study is more likely to suggest a breach of animal room protocols rather than evidence of immunosuppression. However, most immunotoxicity protocols have been developed and standardized in rodents, including multiple host-defense models that use either viral or bacterial infections. In addition, there are a number of commonly used host resistance assays for rodents that target specific arms of the immune response (Burleson and Burleson 2008).
Nonhuman Primates
Some of the standardized immunotoxicity protocols have been adapted to large animals, especially NHP (Bussiere 2008), but unlike SPF rodents, dogs and NHP have numerous background infections and infestations that, although animal providers have worked hard to eliminate and/or control them to negligible levels, still persist (Sasseville and Diters 2008). In the case of NHP, the variability in the health status and quality may be affected by the source of animals (country of origin, purpose-bred vs wild caught, age, previous and/or ongoing subclinical infections), but the increasing stringency demanded by pharmaceutical companies has helped to enforce higher quality of animals placed on study.
Typical screening procedures by contract research organizations for handling of NHP include:
Complete and accurate medical histories.
Selection of naïve, healthy animals.
Deworming with ivermectin/albendazole.
Tested negative for tuberculosis within two weeks of shipping.
Body weight, physical examination within two weeks of shipping.
Clearly visible permanent identification.
Hepatitis A vaccinated, or positive titer.
Measles vaccinated, or positive titer.
Serology negative within thirty days of shipping for SIV, SRV, STLV-1.
Tested for BV within thirty days of shipping. BV+ animals can be shipped for most orders; some clients request BV−.
Salmonella- and Shigella-negative within forty-five days of shipping (rectal).
Negative for external parasites.
No surgeries (except for trauma or cesarean section).
Viral, bacterial, and parasitic organisms of NHP have been well characterized, and the reader is encouraged to consult such references for specific details (Sasseville and Diters, 2008). A listing of possible pathogens that might be encountered in NHP primates, and adapted from Sasseville and Diters 2008, is shown in Table 1.
Viral, bacterial and parasitic organisms encountered in nonhuman primates.
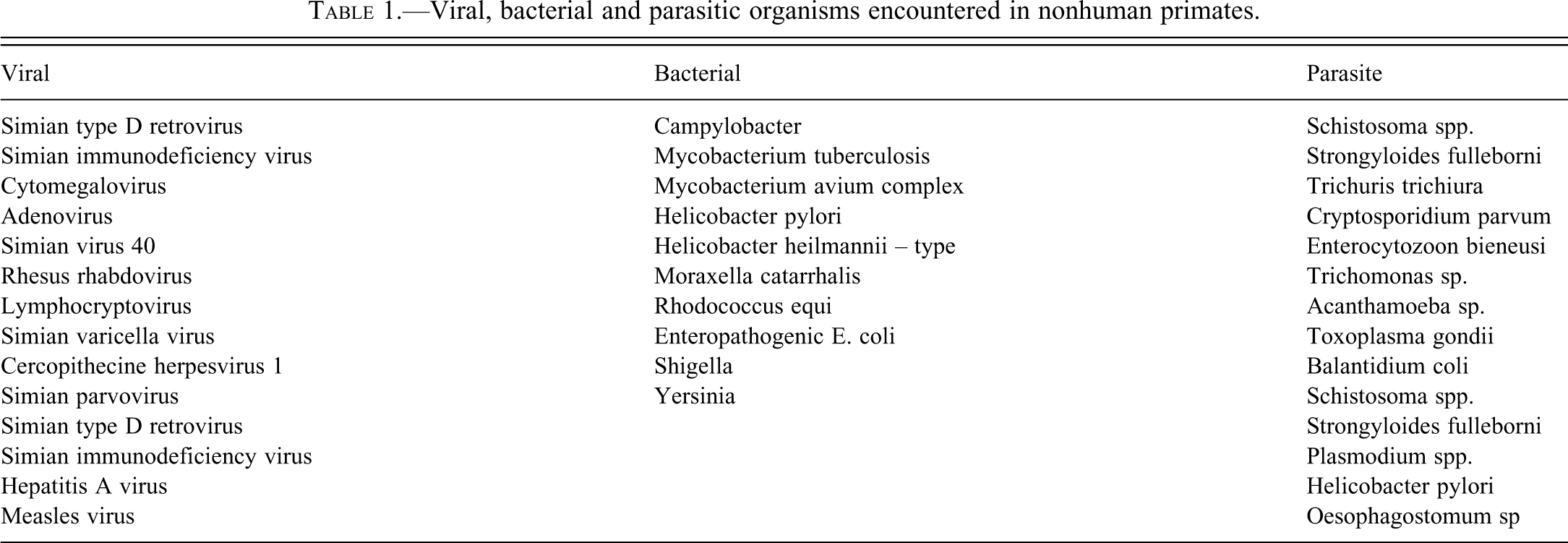
As noted above, NHP may still carry a number of viral, bacterial, or parasitic organisms that under conditions of immunosuppression can become fulminate, leading to moribundity and mortality (Olivier et al. 2010). Captive macaques have a high incidence of chronic enterocolitis because of the presence of opportunistic and/or obligate parasites. Recurring diarrhea from a number of bacterial species that include Camplyobacter spp., Shigella flexneri, Yersinia enterocolitica, adenovirus, and Strongyloides fulleborni is the leading cause of animal morbidity requiring veterinary care (Sestak et al. 2003). Thus, pathogens of the intestinal tract appear to be particularly troublesome for NHP and can quickly compromise a study.
Viral diseases are controlled by nonspecific (natural killer cells) and specific immune reactions (cell-mediated and humoral). Likewise, bacterial diseases are controlled by specific humoral immune responses and nonspecific phagocytosis (neutrophils and macrophages). The impact of a new immunomodulator on these immune functions can be predicted by a rigorous delineation of the pharmacological action of the drug. Indeed, immune function assays that are used to identify pharmacological (PD) effects can also be indicators of immunotoxicity if tested at high multiples of the therapeutic dose.
Of particular concern when testing immunomodulatory drugs in NHP is polyoma virus infection. The human polyoma virus JC virus (JCV) is the etiologic agent of progressive multifocal leukoencephalopathy (PML), a demyelinating disease of the central nervous system in man, which occurs in immunosuppressed individuals, including patients with AIDS. Simian virus 40 (SV40) has 69% homology with JCV and has been associated with a PML-like disease in immunosuppressed monkeys (Horvath et al. 1992). BK virus is closely related to JC virus. Immunosuppression of cynomolgus monkeys used in renal transplantation studies has been associated with BK-like virus nephritis, and polyoma virus infection has been seen in monkeys treated with immunosuppressive monocloncal antibodies (Hutto 2008; Hutto 2010). The emergence of polyoma virus infection in NHP has particular relevance because monkey PML appears to be similar to human PML.
Despite improvements in husbandry and collection techniques, many pathologists still encounter various helminth and protozoal parasites in the intestinal tract, liver, and biliary system of otherwise “normal” NHP in drug safety assessment studies. It may be difficult in such cases to determine whether the emergence of an otherwise quiescent parasite is a result of test article immunomodulation or happens to emerge from the stress of study procedures (release of endogenous corticosteroids resulting in immune suppression).
As was stated above, histopathology of the lymphoid system is a cornerstone of identification of effects on the immune system. But a challenge that becomes evident in NHP, especially those that have previously had viral, bacterial, or parasitic infections, is the remarkable anatomic variability of lymphoid tissues. For example, it is not uncommon to find large, irregular hyperplastic lymphoid nodules or numerous large, highly variable numbers of lymphoid follicles in the spleens of purpose-bred cynomolgus monkeys (personal observation). It is also not uncommon to find hyperplastic germinal centers filled with an amorphous, hyalinized eosinophilic material in splenic lymphoid follicles, considered by some to be antigen–antibody complexes. Knowledge of these background variants needs to be factored in when determining no-effect levels of targeted immunotherapeutic drugs. It is also important for the pathologist to annotate these lesions despite the conclusion that such background changes are “within normal limits,” so as to assist with the generation of more accurate historical control databases.
Dogs
Although dogs do not bring with them the large range of exotic pathogens that are seen in NHP, they do have background organisms that can readily compromise an immunosuppressed animal. One of the most challenging canine-associated organisms is Demodex canis. Demodex mites, which are part of the normal flora of canine hair follicles, may rapidly proliferate under conditions of immunosuppression. Mites are present on all dogs regardless of their normal clinical appearance, and they are passed from dam to nursing pups. The mites erupt first on the muzzle and forelimbs secondary to immunosuppression induced by poor nutrition, general stress, and immunosuppressive drugs (Baker et al. 1968; Barriga et al. 1992). Demodectic mites encased in granulomatous responses may be found in the lymph nodes (especially the mandibular nodes; personal observation) of normal dogs, attesting to their background presence, and large numbers may translocate to regional draining lymph nodes under conditions of fulminant mange. Demodectic mites are immunosuppressive in and of themselves and therefore, an eruption can lead to other secondary and serious cutaneous bacterial and/or fungal infections (Barriga et al. 1992). Cutaneous lesions rapidly become pyogranulomatous as bacterial and fungal organisms invade the epidermal ulcers and spread within the dermis. Eosinophils play a major role in controlling ectoparasites, and outbreaks of mange secondary to therapeutic compounds that suppress circulating eosinophils or their function can be expected (Legrand et al. 2007).
Having a thorough understanding of possible but unintended pharmacodynamic effects is also very important for study design, regardless of the species used. Despite the increasing specificity of new small molecules, we do not fully understand or always recognize the complexity of interacting and overlapping molecular pathways that are at play for each biological process. What is overlooked is that the specificity of most new small molecules is determined at therapeutic exposures, but as doses are increased in toxicology studies, the IC50 values for other receptors and pathways may be covered, resulting in unexpected pharmacological and toxicological outcomes. Although KO models tell us something about the worst case scenario of an altered pathway, they do not always give clear signals concerning overlapping and interwoven pathways perturbed by highly target-specific small molecules. For example, therapeutic compounds that target or suppress IL-5 or CCR3 may alter eosinophil function (Pazdrak et al. 1995; Stout et al. 2004), and as noted above, dogs may be put at risk of developing fulminant mange, which in turn may compromise the ability to complete the study as designed. Moreover, because cell biologists may be so focused on the specific cell receptors that they are targeting, it is possible that the role of that particular molecular pathway in other critical immune function cells may be missed. It rests on the shoulders of the toxicologic pathologist to extensively review and research the available literature to delineate such unanticipated pathobiological effects.
Another canine problem is interdigital dermatitis or pododermatitis, also called pedal folliculitis or interdigital furunculosis. This condition is frequently seen in caged beagle dogs and is a multifaceted disease (Duclos et al. 2008). The causes include exogenous foreign bodies, contact irritants, hypersensitivity reactions, parasitism (demodicosis), infections with yeast, fungi, and bacteria, and other disorders associated with immunosuppression. Once started, it is difficult to prevent dogs from chewing on the lesions, which then worsen as broken hair shafts are driven deep into the highly inflamed tissue. The design in cage flooring affects incidence and severity, which can be decreased with appropriate selection of flooring (Kovacs et al. 2005).
Another common parasite of the general canine population that may be encountered in purpose-bred beagles is Malassezia pachydermatis, a non-lipid–dependent species of yeast that is a commensal organism and occasionally an opportunistic secondary pathogen affecting the canine skin surface and ear canal (Morris 1999; Peano and Gallo 2008; Oliveira et al. 2008). In routine veterinary practice, infections of the external ear canal are often seen in otherwise healthy dogs, especially those with pendulous or ‘droopy’ ears (i.e., the beagle), particularly if the ear canal gets wet. In severe cases, Malassezia is capable of penetrating skin and becoming systemically distributed to viscera. Pneumocystis jirovecii, a fungal organism carried by normal, healthy dogs, may result in localized pulmonary inflammation in immunosuppressed dogs.
A viral infection that is highly likely to occur in immunosuppressed dogs is canine papillomavirus. This virus can induce localized proliferative lesions of the skin and mucous membranes in a wide range of vertebrate hosts. Each type of papillomavirus is species specific and shows a preference for specific tissues. Canine papillomatosis has been seen with systemic corticosteroids, cyclosporine, and in X-linked SCID dogs, and it may be seen on the feet and muzzle of dogs with severe demodecosis (Barriga et al. 1992; Miller 1979; Owen 1972).
A major decision that must be made regarding opportunistic infections in study animals on chronic studies is whether or not to treat the animal for the pathogen. Opinions as to the value of treating animals prophylactically and/or therapeutically for such infections/infestations are split among researchers. The pro position for such treatment supports minimizing discomfort (i.e., nonsteroidal anti-inflammatory drugs, antibiotics), holding the parasite in check (i.e., ivermectin), and keeping the animal on study long enough to assess non-PD effects (i.e., toxicities of organ systems other than the immune system). The contrary position is based on concern that the unknown drug–drug interaction between the test article (TA) and the therapeutic drug may generate its own set of target organs and confound study interpretation. Even when there are data documenting the potential toxicological effects of a given drug (i.e., nonsteroidal anti-inflammatory drugs), the unique combination of the TA with other drugs may cause unexpected toxicities of uncertain relationship to the TA. Other questions need to be considered, such as will the animal be treated longer than a typical therapeutic model because of protracted PD-mediated immunosuppression? Will standard dosages of the therapeutic be used? Are the clearance pathways (i.e., renal vs hepatobiliary) the same or different for the therapeutic and the test article? Should you treat only those with symptoms, or all animals on study? A careful and thorough review of the literature is essential for minimizing the confounding elements of adding a therapeutic regimen to the study, especially in chronic studies. However, at the end of the day, the decision of whether to treat or not to treat may be an animal welfare issue, and consulting and collaborating with the attending veterinarian is essential.
Despite species differences in the structure and function of the immune system, when trying to select one large animal species over another, it remains true that the basic responses are the same and there are no a priori benefits of one large animal species versus another. Populations of NHP and dogs are known to have both high and low immunologic responders in response to infectious stimuli. Identification of low versus high responders is not possible without extensive individual workups.
Importantly, there may be significant differences in the pharmacokinetic and pharmacologic effects across species. In fact, species differences in absorption, distribution, and excretion are often more pivotal in selection of the test species than are differences in immune structure or function. Also, pharmacologic activity should be demonstrated in at least one
Other essential questions that need to be addressed include:
What mechanisms of defense were compromised or altered in the preclinical studies?
What arm of the immune system is being affected?
What is the mechanism of action, and is it likely that the same mechanism of action will be affected in humans?
Does the opportunistic infection in animals have a correlate in humans?
Are the effects monitorable, treatable, and reversible?
Are there in vitro assays or biomarkers that accurately measure the PD affect of the drug?
In the end, one has to ask the question, what do preclinical toxicology study findings of intentional immunomodulatory drugs, both small molecules and large biologicals, mean for humans? Basically, such studies confirm the intended target of immunomodulation and identify the risk of excessive PD in general terms. The real difference between these two classes of drugs is that with small-molecule immunomodulators, one can achieve repeated and longer dosing at higher levels in multiple species. However, this study design benefit is accompanied by greater challenges in controlling species-specific pathogens and requires an understanding of both species-specific and general immune responses.
Footnotes
The author declared no potential conflicts of interests with respect to the authorship and/or publication of this article. The author received no financial support for the research and/or authorship of this article.