
Abstract
Unpaid carers play a vital role in supporting individuals with life-limiting conditions, yet without adequate support, they risk poor health and burnout. Respite care offers carers a temporary reprieve, helping them to sustain their caregiving responsibilities. Existing literature primarily focuses on respite in the context of adult day care and dementia care rather than its role for carers of individuals with other life-limiting conditions. This study seeks to address this gap. Ten in-depth interviews were conducted with carers who had used temporary institutional respite services in Scotland. Participants cared for individuals with multiple sclerosis or conditions resulting from a stroke. Reflexive thematic analysis was employed to explore their experiences of taking a break and its impact on their caregiving role. Six key themes emerged: ‘Caring is all-consuming’; ‘Caring changes sense of self’; ‘Relief, recovery, repair’; ‘Breaks give carers their lives back (briefly)’; ‘A break doesn’t solve everything’; and ‘Trust in the respite centre is crucial’. Findings indicate that institutional respite care provides overwhelmingly positive experiences for most carers, offering them essential relief and recovery from the demanding nature of caregiving. However, the benefits were often short-lived, with carers expressing a need for longer and more frequent breaks. Additionally, trust in the respite centre was paramount for a positive experience. To better support carers, policy initiatives should focus on expanding access to respite care, ensuring that services meet carers’ needs effectively.
Introduction
It is estimated that there are currently 5.7 million carers in the UK (Carers UK, 2023a). Carers can be partners, spouses, siblings, parents, children, friends, or neighbours and are often described as unpaid, family, or informal carers (referred to as ‘carers’ forthwith). They provide a wide range of support to the person they are caring for, including personal and domestic care as well as healthcare. They differ from professional carers, who are paid to provide such services. Those being cared for include people with a wide range of diseases, conditions, and disabilities. It would cost the UK Government £162bn per year to replace the hours of unpaid care provided by carers (Carers UK, 2023b).
Caring almost always has a significant impact on carers’ health and well-being (Mason et al., 2007). It can be both a positive and overwhelming experience (Harkin, et al., 2020). Caring can impact negatively on carers’ emotional well-being, evoking feelings of anxiety, stress, fear, hopelessness, and exhaustion, as well as a deterioration of their physical health (Wu et al., 2022; Wakefield, 2020). Carers also face considerable health inequities compared to non-carers, including higher levels of depression, anxiety, and stress, as well as greater prevalence of disease and higher risk of premature death (Spiers et al., 2021).
In the UK, many carers need to stop caring because of physical and/or mental breakdown largely due to a lack of support from the state (Paddison, 2021). The demand on carers is predicted to increase significantly in future years as the population ages with additional health needs (Government Office for Science, 2016). This demand will result in greater pressure on healthcare services, which is unlikely to be met, creating yet more demands on carers (Petrie & Kirkup, 2018).
The expressions ‘respite’ or ‘a break from caring’ are often used interchangeably to refer to an intervention that supports the cared-for person to enable the carer to have a temporary break. Respite care services include day-care (Maffioletti et al., 2019), temporary institutional respite care (Phillipson & Jones, 2011), or in-home respite care (Wakefield, 2020). A break can allow a few hours to several days to rest; participation in other personal tasks; activities or interests; time away from the emotional and physical stress associated with caring; and looking after their own health (Harkin et al., 2020; Wu et al., 2022; O’Connell et al., 2012).
The aim of this study is to explore carers’ experiences of breaks enabled by temporary institutional respite. The existing literature shows conflicting findings regarding the benefits of such breaks. Some evidence suggests that carers’ experiences are positive, leading to reduced stress, improved quality of life, and a more positive outlook on their caring role, although these effects may be short-lived (Phillipson & Jones, 2011; Harkin et al., 2020; Mason et al., 2007; McNally, 2008). However, Vandepitte et al. concluded in their systematic review that the results of temporary institutional care ‘are rather mixed and show unexpected adverse effects’ on carers such as leading to increased stress immediately following a break (Vandepitte et al., 2016, pp. 1286).
More research on temporary institutional respite is therefore needed to understand how effective it is at supporting carers to have a break. This study sought to explore the experiences of carers of adults in a home setting who have had a recent break (4–11 days) from caring using a temporary institutional respite service and the impact it had on their caring role.
Methodology
This paper describes an interview study exploring the perspectives of carers having a break from caring by using a temporary institutional respite service for their cared-for-person.
Participants and Recruitment
Participants were users of a national respite centre in Scotland, which offers respite breaks of four, seven, or eleven nights for those with long-term neurological conditions such as multiple sclerosis, stroke, and Parkinson’s. Following ethical approval by the University of Edinburgh Usher Institute Masters Research Ethics Group in December 2022 (Ref: UM23119), a purposive sample of carers were contacted by the management of the respite centre. Carers contacted were registered on the centre’s database and had experienced a break from caring in the last twelve months. Potential participants were emailed information about the study and consent forms and asked to email the researcher directly if interested in participating. Signed consent forms were returned electronically before interviews, and consent was verbally reaffirmed before interviews commenced.
Data Collection
Semi-structured interviews were conducted by the first author, RM – a director of a national charity supporting carers and a trustee of the respite centre – using a topic guide developed using Bevan’s (2014) phenomenological interviewing approach. Carers were asked about their caring circumstances, their recent experiences of a break, what they did with their time, how it made them feel, and the impact it has on their well-being. They were also asked about what led them to take a break and if they would continue to take them in this way.
Interviews took place between March and April 2023 and lasted 45 minutes on average. Nine out of the ten interviews were held virtually using Microsoft Teams and one interview by telephone (due to lack of access to the computer software). Participants were informed that the researcher was a trustee of the respite centre and assured them that their taking part was confidential and that anything they said about the service would not be attributed to them.
Data Analysis
Interviews were recorded and transcribed via Microsoft Teams or directly by RM, from a recording of the telephone interview. All transcripts were checked by RM. RM led the analysis, using a reflexive thematic analysis approach developed by Braun and Clarke (2006, 2019, 2021, 2022) following their six steps: (1) familiarisation with the data; (2) generating codes; (3) developing themes; (4) reviewing potential themes; (5) defining and naming themes; and (6) writing the report (Braun & Clarke, 2022). RM and the co-investigators then discussed the transcripts and identified themes more widely.
Each line of the transcripts was scrutinised for meaning and relevance to the research aims and then coded accordingly. Analysing the codes led to the generation of ten themes, which were refined to six, through continued reflection, revision, and discussion. The analysis was further informed by a research diary maintained by the researcher to allow continuous reflection and to interrogate and mediate how personal experience, perceptions, and values shaped the research.
Findings
Details of participants and their cared-for-person
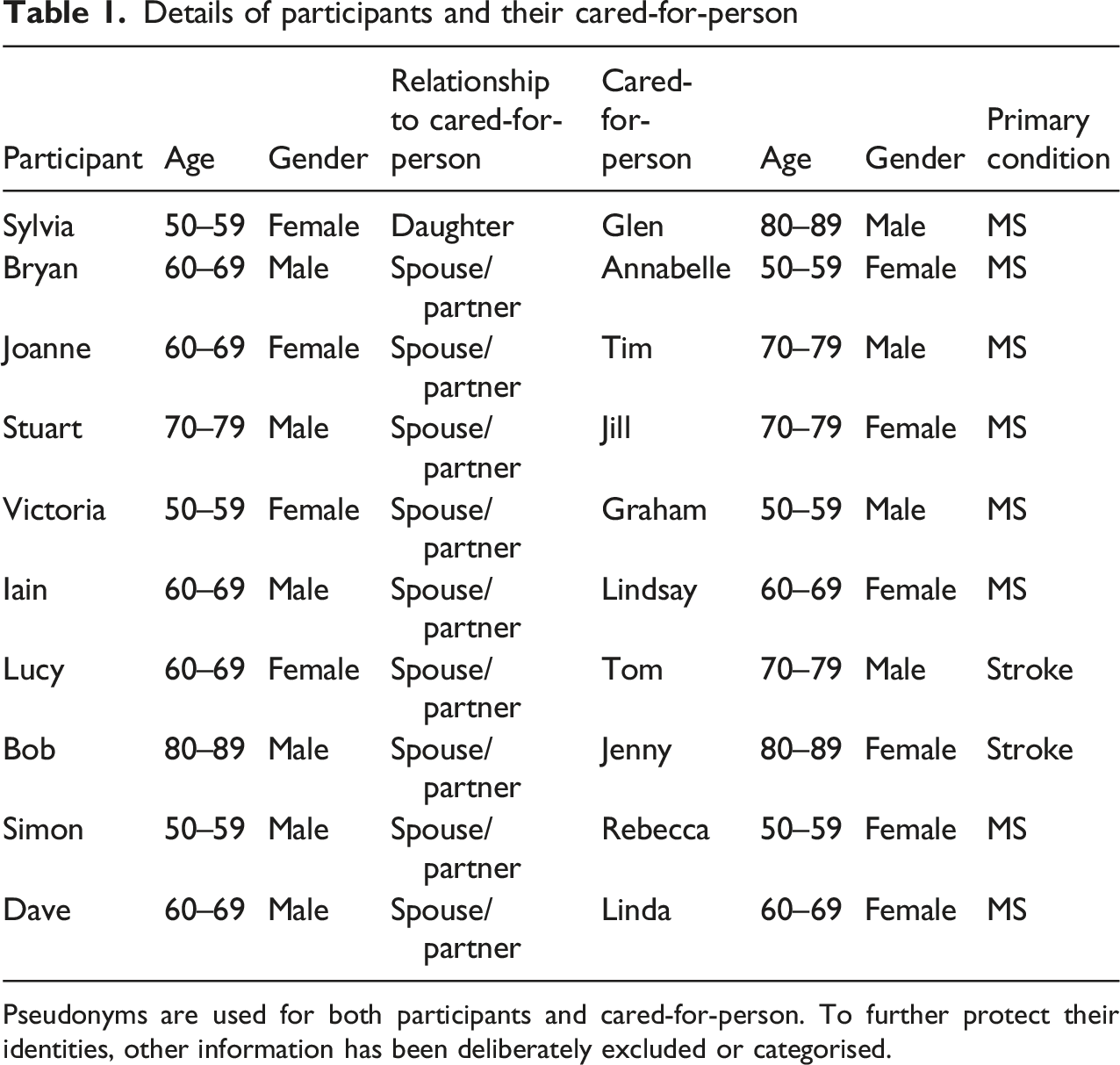
Pseudonyms are used for both participants and cared-for-person. To further protect their identities, other information has been deliberately excluded or categorised.
Reflective thematic analysis generated six key themes: (1) Caring is all-consuming; (2) Caring changes sense of self; (3) Relief, recovery, repair; (4) Breaks give carers their lives back (briefly); (5) A break doesn’t solve everything; and (6) Trust in the respite centre is crucial. The first two themes reflected the impact of caring on carers and demonstrate why they needed a break from caring.
Caring is All-Consuming
Carers reported finding caring a constant activity that they cannot switch off from, that is all-consuming, and substantially impacts on their health and well-being. They described physical injuries and aches and pains that result from caring, as well as challenges with sleeping and recovery. This led to a high level of physical, but mostly mental, exhaustion that carers described experiencing daily. The impact on their mental health was often stated as the greatest consequence of their caring role. The demands of caring were often expressed as something beyond what would be considered acceptable or even normal in other non-caring roles, such as employment. […] mentally the exhaustion which is, you know, um, extreme (Bryan). I’ve always said it's the hardest job in the world. I mean I worked full time up till I was 61. And this is, this is the hardest thing […] I say you've ever got to do is look after somebody […] It’s really a hard thing to do mentally, maybe not physically, but mentally it's hard (Joanne).
Carers reported that caring leads to little time for anything else. Physically, there was no time for anything other than the caring role, but mentally they never switched off from caring even when they were not carrying out the physical demands of caring. It dominated their thoughts. I mean, there was very little time for anything other than that (Bryan). […] you're just on edge the whole time if he drops something, if he needs to go to the toilet, which you know, erm, if you know, I'm never relaxed, even if I go out, I'm watching my, my watch all the time and I’m never totally relaxed (Joanne).
Carers often described being pushed to the point where they struggled to cope with their caring role, suggesting they could not care indefinitely. Carers realised these limits and the risks of physical and/or mental breakdown that came with the all-consuming nature of caring. They described ultimately knowing they might have to stop. […] it's like now I feel like, I think you can cope for so long, but I think all of a sudden it's like, whoa, the body's just not working properly (Sylvia). […] there are times when I'm like […] I get down and generally speaking my cup’s always half full, you know, but there are times when I'm like, I don't know how long I can do this for, you know (Dave).
Participants reported that the caring relationship was imbalanced, with the needs of the cared-for-person always prioritised, either through choice of the carer or the demands and needs of the cared-for-person. In some instances, the cared-for-person was said to expect that their needs would be put ahead of the carer. Carers often described feeling that their own needs were not recognised or valued. Participants sometimes suggested an expectation that they will carry on regardless of their feelings and health, reinforcing the all-consuming nature of caring. […] I think he's that used to getting everything done for him, you know, and I do, I do, I mean put him first for everything. He gets, he gets put first in everything […] (Joanne). […] we've never had major rows and stuff like that, and, but we've had the odd, when you know, if she's got into a lot of pain and I'm in pain, but she seems to think her pain is more important than the pain I am in […] (Simon).
Carers’ accounts expressed a tremendous sense of responsibility, compounding the all-consuming nature of their caring role, often in the context of dealing with their own mental and physical health problems. Participants often linked this responsibility with a duty to care, because of the nature of their relationship, partner/spouse or child, with the cared-for-person. […] I had all the responsibility, everything was me (Lucy). But there's a loyalty in there […] and I will look after him. I will look after him as long as I can. But it does take its toll […] (Victoria).
Carers described finding it difficult to switch off this responsibility, no matter their feelings or circumstances, pointing to the relentless nature of caring. The responsibility, alongside the physical demands of caring, was often borne solely by them. […] there’s days where you know I've just not felt great at all, but I don't have an option. I've got to get her to bed. I've got to put her to bed. I've, you know, I don't like the weekends (less professional support). I've gotta get her up if she needs to go to the loo. I've got to put her on the loo and stuff for that. So, I've gotta get her then redressed and all this. And no matter how bad I feel, I've still got to do it cause nobody else will do it (Simon).
Caring Changes Sense of Self
Participants reported that the caring role is so physically and mentally hard and so consuming that many carers started to experience some psychosocial consequences that significantly impacted their mental health and their sense of self. Dave’s quote below demonstrates this, as in conversation he moves on from the effect of caring on his health to the concept of his independence. […] I know it's the caring role that I'm doing that's starting to drain me, starting to drain me of my health. It starting to drain me of my, my independence (Dave).
The erosion of independence and the restrictions on their lives because of caring has a significant impact, as Simon stated: ‘[…] that’s where you start to feel trapped’.
It is clear in this data that the caring role does start to impact on individuals’ identities. In the extract below, Simon put his identity as a husband before that of a carer, which suggests that this identity is more important to him. However, the caring role is clearly starting to impact on that identity and perhaps the two are starting to merge. I actually don’t see myself as a carer. I see myself as the husband and, but just lately it's like it becomes a burden that you know, I'm now having to look after her (Simon).
Relationship status appeared to be an important aspect of participants’ sense of selves. This is evident in Simon’s quote above, as he tries to hold on to his identity as a husband. For some carers, however, this identity was reportedly lost completely, especially where the condition of the cared-for-person altered their personality and behaviour. I think what people don't understand is it’s a very lonely place to be a carer, because you're no longer part of a, in reality, you're no longer part of a couple. […] because the person I'm looking after now is a shadow of the person that I married […] (Victoria).
Carers shared that important parts of themselves were missing because of caring, which affects their sense of self and leaves them mourning for it, as Victoria stated sombrely: ‘It’s sad, to see the life you had’.
For many carers, the chance to address matters of self or reflect was simply not possible, as Sylvia put it: ‘I don’t have any time to myself’. Bryan compares the all-consuming nature of caring to being at war, where any notion of emotional or self-care is a casualty to manage the demands of caring. […] it’s like being in the trenches […] there's no space for paying attention to things like mood […] (Bryan).
Caring is deemed to directly affect many carers’ personality and behaviour. Most suggested that changes in the way they behave were driven by their caring role, particularly referring to what could be considered negative behaviours. It just so kind of piles up. So, there are times when, uh, I can get sort of quite argumentative (Stuart). Yeah, because I used to be quite a sociable person (Sylvia).
For those carers who had the chance to socialise, there was a perception that their caring role was of less value and interest than non-carers’ lives, describing a diminished self that led to social withdrawal. Others suggested that non-carers might not understand or be willing to share the ‘burden’ of what they are experiencing, leading to social awkwardness, loneliness, isolation, and leaving the carer unwilling to talk about their caring lives. The tone of Bryan’s extract below demonstrates the sadness this can bring. […] because to your social life you usually talk about what you're up to. And what I’ve been up to is a constant repetition of the same things. But, and it feels like a burden on other people to talk about that. People tend to be quite uncomfortable in talking about it […] (Bryan).
Carers also talked about loss of their personal space at home due to the constant need for professional caring services and medical equipment, having a knock-on effect on sense of self. As Victoria said: ‘Your house is no longer your own’. Caring disrupted and changed the way of life for the carer and the cared-for-person. According to Lucy, ‘You lose control when you’ve got (professional) carers coming in’. It impacts on their privacy and intimacy, as Lucy continued, ‘Our lives were just taken away really […]’.
Relief, Recovery, Repair
There was a clear pattern in the data which showed a substantial change in mood and a sense of relief for carers when getting a break. The data suggests that a break allowed many carers to switch off for a period from their caring role, as Lucy articulated, ‘I didn’t have to think about it (caring)’.
Narratives shared about breaks from caring suggested that a break allowed carers to experience a release of the pressure built up from the all-consuming nature of caring. For most, breaks were beneficial as a result, and something they enjoyed. The tone and body language displayed by many carers during the interviews when asked about the meaning of a break showed the palpable sense of relief, drawing out a smile or a physical display of relief; giving a sense of how important those breaks were. But when she's gone it's like I'm decompressed. I can relax. […] it's like a weight lifted off your shoulder and you relax. […] (Simon). […] when I wave him away, it's just a complete (author: she gestures a huge sigh of relief) (Victoria).
Many of the carers recognised the importance of looking after their mental health, which they described as suffering because of caring. Breaks were often highlighted as being beneficial to their mental health, which may be why they are perceived as positive. So that's (the break) taking all of that away [she gestures hand to indicate something relating to pressure on her head] as well as the physicality of it as well as, so I would say it is probably more of an emotional break. There's an emotional break happens as well as a physical break (Victoria).
Carers conveyed an understanding that breaks were about meeting their needs, and they can use a break in whatever way to meet those needs, constituting a ‘good break’. […] this time I've decided that actually I just want to be in my house on my own with nobody coming in. Erm, so again equally therapeutic, but actually just thinking I just want to shut the door and be in my pyjamas and not have to get up and let people in (Victoria).
Many carers described the huge responsibility and sense of burden that they can constantly experience in their caring role. A break can release them from those feelings of burden and responsibility, and to great effect giving them ‘Peace of Mind’ (Bob). The responsibility basically of Rebecca, […] if she's been looked after by somebody else and it sounds terrible, but she's no longer my problem for 11 days (Simon). […] it's night and day. Black and white. Um, because instead of carrying concern, […], it's just like the burden is removed (Bryan).
A break was about recovery for participants, and they recognised the importance of that in helping them to continue being able to care. Exhaustion was frequently described as a consequence of caring. Participants related exhaustion not only to the physical and mental demands of caring, but also to a lack of sleep due to caring. For many, breaks gave many carers the opportunity of getting a good night’s sleep to enable the body to recover. The other thing I did was sleep. […] A long time to catch up on (Bryan).
Many of these carers worried about their ability to continue caring if they could not get a break, including the prospect of a complete breakdown in care. They suggested that this would result in significant consequences, with the cared-for-person likely to be admitted to a care home. This was something that neither the carer nor the cared-for-person wanted. Breaks brought the carers back from the point of possible breakdown to a place where they could physically and mentally continue to care. What it meant for me was the ability to keep on…Um. You know on each occasion I was, um, you know, a hair’s breadth away from busted. [...] Without it (a break) I would have been an absolute basket case (Bryan). I'm really worried because if I go sick, then what will happen to her, and all they say (social care) is they'll just fire her into a care home. And that's the last thing that I would ever want for her to happen (Simon).
Breaks Give Carers Their Lives Back (Briefly)
Carers shared stories of how a break can help, albeit temporarily, to give them a glimpse of their old self, the ability to reconnect with who they are, or the person they could be but for their caring role.
Carers greatly appreciated ‘[…] that bit of freedom’ (Bob) and a return of their independence via a break. In the interviews, talking about a break reminded the carers of just how restrictive caring is. The use of the word freedom by many to describe a break shows how they feel ‘trapped’ (Simon) in their caring role. Breaks offered temporary relief from this entrapment. […] it's where you, you have an opportunity to go to a cafe or a restaurant and not have to feed somebody. Yeah, it's a time when you can do that. Those things completely on your own. And decide you know when to get up, when to go to bed. Umm, all the things that you would do if you, you had the total freedom (Stuart). I can just relax and get up in the morning when I want to, go to my bed when I want, and cook what I want for myself, you know, it's a completely different thing altogether (Joanne).
Carers reported wanting a complete break from their caring lives. They said it was not just the physical and mental demands of caring but every aspect, including a break from the professional services coming into their homes and the visible reminders of caring, including medical equipment, such as hoists. For carers, this constituted a true break, experience a caring-free life, and a sense of normality for a short period. What I do when Graham goes into respite is clean all the house. I put all their equipment into one room and shut the door (Victoria). I just got space to myself and that was lovely. That was lovely. It was the house, and it was what was important to me, I could just kind of chill […] (Lucy).
From these accounts, breaks gave carers the chance to rediscover and focus on their own needs. It gave them the rare opportunity to put themselves first, which was important for their mental health. […] it's just having time on my own at the time to think. The ability to, to think (Stuart). […] get yourself together and just do something for yourself […] (Sylvia).
The effect of a break appeared to go much deeper than the opportunity to do what they want or be by themselves. It helped carers regain important aspects of themselves and their identity that they lost while caring. Absolutely, absolutely it (a break) reminds me of who I am (Joanne). I pretty much got back to being myself (Bryan).
Carers frequently used breaks to reconnect with those social aspects of their lives that are often lost or limited due to caring. Family and wider social connections were important to carers, providing social and emotional support to them throughout their caring role. They also acted as focal point of a break, where they can support the carer to have a ‘normal life’ during that time. Carers were often determined to maintain those social connections and breaks provided the opportunity to do this. I'll be able to go and meet friends that I used to work beside, erm, my sister-in-law has said we could go, maybe through to [city] and stay a night and do a bit of shopping, you know, just things that I can't do, erm, when Tim's here (Joanne). I made a point of maintaining some kind of social contacts myself, because it's so important (Victoria).
A Break Doesn’t Solve Everything
The benefits of taking a break came across strongly from the data. However, a break did not benefit every carer and for some carers the break did not resolve all their concerns. A break could be quickly followed by a return of the mental and physical health challenges they had faced prior to their break.
Iain’s experience was in stark contrast to the accounts of the other carers in this study, as he described experiencing few if any benefits of having a break that others described. He reported not feeling the need for a break, despite not having one for ten years. Iain’s experience was one of loneliness and isolation. Surprisingly lonely sounds trite. But it was surprisingly lonely. It didn’t, it didn’t feel right. […] I’m sure some people you’ve interviewed […] might have said, yes it was great freedom at last, go and do my own thing. That’s not how I felt at all (Iain).
It is worth noting that Iain’s experience did not give him much of a break, as he still performed caring-related tasks despite his partner being at the respite centre. It was a bit of a disaster really, so I spent most of that week while Lindsay was at [respite centre] on the phone trying to arrange a replacement Motability car, and not doing much else, not least because the temperature, the weather was so ghastly, and the replacement Motability car […] was delivered at home about 30 minutes before I had to set off to pick her up [..]. So, it was a how can I put it, a stressful week. No, not the way it was planned (Iain).
Iain’s experience is important to consider as it demonstrates that carers have different needs and wants in relation to how they receive breaks and respite from caring, and different carers will experience the same service in different ways.
For others, breaks were not as positive as expected or hoped for because of a difficulty adjusting to being separated from the cared-for-person. From participant accounts, it seemed that caring took up so much time that they struggled to fill it when not caring, and perceptions of missed opportunities and time not well spent. Rebecca is a massive part of my life and when she goes away, that part has then gone so I am like twiddling my thumbs, thinking, right, what do I do? (Simon). At that point (time of break) my back was out, so that didn't help anything (Bryan).
Some carers also talked about experiencing guilt from leaving their cared-for-person in a respite facility, which impacted on their ability to fully benefit from the break. This was particularly the case if the cared-for-person isn’t fully agreeable to going into a respite facility. […] you’re relaxing and you’re enjoying yourself, and you’ve kind of, it’s not that you’ve got rid of him, that’s not right […] but he’s not with you. […] it is still quite difficult to relax and not feel guilty (Lucy). Well, I'm going to be honest with you, the first two or three days wasn't that great because Tim, he wasn’t communicating with us. We knew when we left him at [respite centre] that my daughter and myself, he didn't say cheerio to us and I knew that he wasn’t happy about it and, and so it was, it was about the Wednesday, Thursday that he started to communicate with us, and that's, that's when I started to relax a wee bit (Joanne).
A strong pattern in the data was that any positive effect experienced by a break was often ‘fairly short lived’ (Lucy) resulting in either a gradual or quick return to a carer’s previous physical and mental state. At the end of a break, some carers experienced a sense of dread about the length of time before their next one, impacting on their mental well-being when returning to caring and diminishing some of the mental health improvements gained during their break. […] it's amazing because I said to them that the pain had actually gone and come back. […] And it was about that time that I had that 11-day break and there you go. And then eventually it come back (Sylvia). When Rebecca comes back it's a case of its six months until she goes away again and that's the first thing that hits you. I've got six months of this again, and all I want to do is try and recharge my batteries as much, but within the first couple of weeks, you're back to the same old, same old (Simon).
This suggests breaks are effective in the moment and do restore carers to enable them to continue to care, but can be a temporary fix, and are often perceived as not long or frequent enough. In terms of, of my sort of equanimity, it's limited because there's just a lot of work to do either side to get […] away (Stuart).
Trust in the Respite Centre is Crucial
Carers were unwilling or reluctant to take their cared-for-person to just any respite facility and emphasised that the right facility is crucial for multiple reasons.
Trust and confidence were paramount to participants, as they allowed them to truly relax and experience the benefits of a break. Many carers commented on their ability to fully relax when they completely trusted the respite service where their cared-for-person was staying. Earlier themes highlighted that the impact on mental health had the biggest effect on the carer’s well-being, and a break can be most beneficial in improving this. The role the respite centre played in enabling this was fundamental. […] it's just relaxing knowing that he is somewhere that somebody is, you know, looking after him well and I can just relax […] and it was relaxing because I didn't have to worry about Tim, I knew he was getting well looked after (Joanne). […] it just makes me feel very comfortable and like I say relaxed that I don't have to worry about her (Simon).
From carers’ accounts, trust and confidence in a respite facility also helped alleviate some of the more deep-seated emotions and feelings carers carried with them such as guilt and burden of care, even for a temporary period. However, not all respite facilities can provide this, especially if the service is deemed as inadequate by the carer or cared-for-person. There's this sort of certain amount of guilt in taking the person you care for somewhere to be looked after by someone else […] especially if you don't think that place is the best place for the person you're looking after, the good thing about [respite centre] is you don't have those sort of feelings, uh, you know, don't feel sort of guilty dropping her off. And so, it's a huge relief (Stuart).
A clear link emerged between the cared-for-person’s experience of respite and the carer’s experience of a break. If the cared-for-person was unhappy, it was very unlikely that the carer had a positive break. If the cared-for-person was happy and even enjoyed the break, then it empowered the carer to enjoy theirs too. The respite facility played a crucial role, as Bryan’s two contrasting experiences of different respite facilities for his cared-for-person show. […] that was actually brutal because first week she was so unhappy being there [respite facility]. I visited her, erm, probably four or five days, urm, and zoomed in between times, erm, but, she was someone who was so unhappy. Erm, really knocks the stuffing out of you, as well (Bryan). [Respite centre], uh, that's a very different environment. […] The level of care in [respite centre] is just fantastic, and so she was happy in [respite centre] […] so at that point I was able to let go. I had confidence that she was OK. […] so that releases, um, everything, you know, it removes that kind of burden of responsibility (Bryan).
For many carers, the ability to have a break depended on the willingness of the cared-for-person to go to a respite service, which in turn is built on the cared for person’s experience of the facility. Yes, I mean if she says that she didn't want to go, she wouldn't go and therefore she wouldn't get any breaks […]. She wants to go there, and she knows that if she goes there, I get the break from her (Simon).
Throughout the interviews, it was apparent that for many carers their relationship with the cared-for-person was hugely significant. For some carers, the ability to use a respite centre allowed them to stay together with their cared-for-person. For these carers, however, using a respite centre could go much further than allowing a shared break. Carers also benefitted from the attention they received from the service, and in a sense, they become cared for as well, having their every need met in a similar fashion to the cared-for-person. And for me it is a good break, you know, I know that some carers don't particularly like going, but I like it. You know, I like, I like the attention that I get. You know, I don't have to do anything (Dave). […] it’s a form of relaxation and that, you know that care’s there for both of us […] (Bob).
Discussion
This analysis demonstrates that breaks facilitated by temporary institutional care are, for most carers, overwhelmingly positive experiences. They support a carer’s well-being, enabling them to recover sufficiently from the all-consuming nature of caring, to continue to provide care after the break. It also allows carers to reconnect with aspects of themselves that are neglected through caring, which is hugely valued by them. A break doesn’t solve everything though, with carers finding the positive effect of breaks short-lived and wanting longer and more frequent breaks to support them. Furthermore, for breaks to be a positive, guilt-free experience for carers, the right respite centre must be used to support the cared-for-person, and be a positive experience for them as well.
The current literature relating to respite care leans on research relating to dementia and day care, which limits an understanding of the wider picture. Many academics have called for more research in this field, with other types of respite services investigated and with cared-for-people of other conditions considered (Vandepitte et al., 2016; Jardim & Pakenham, 2010). This research makes a novel contribution to the literature, as it explores temporary institutional care instead of day-care services, and carers of those with conditions other than dementia. It adds critical new insights to the knowledge base on respite and further demonstrates the importance of ensuring carers and cared-for-people have access to the right services to maximise the positive experiences and benefits of breaks.
Importantly, this research extends the evidence base exploring support for carers, by demonstrating that many of the challenges faced by carers of those with MS and stroke are similar to those caring for someone with dementia. The all-consuming nature of caring and the resulting physical and mental health challenges; the need for a break; the trust required of the respite service; and that breaks are good overall for carers, but have a short-term effect, are all issues shared between carers of these conditions (Vandepitte et al., 2016; Maffioletti et al., 2019). This suggests that research of those carers of people with dementia is potentially transferrable to other settings and contexts.
The reported experience of caring as all-consuming in this study is consistent with existing literature in this field (Harkin et al., 2020). The substantial impact reported by carers on every aspect of their well-being, including the significant detrimental impact it had on their mental health (Shaw, 2009), and the subjective burden and responsibility created by caring is also consistent with existing findings exploring issues relating to caring (van Exel et al., 2006; O’Connell et al., 2012).
Phillipson and Jones (2011) found that carers using temporary institutional respite services had a critical need for a break. Many of the carers in this study described being at the point of breakdown in periods before receiving a break, suggesting transferability of this finding.
Like other studies (Phillipson & Jones, 2011; Harkin et al., 2020), this research echoes the positive impact on physical and mental health that carers can experience from a break by using temporary institutional care. For many carers, a break helped them to recover sufficiently to continue to care and prevent a possible breakdown in care, as well as postponing a potential care home admission of the cared-for-person.
This study also presents rich experiences of what recovery, relief, and repair looks like for some carers and how a break addresses those physical and mental health concerns, which isn’t always present in other studies. Carers described being relieved of their responsibilities or burden of caring, enabling them to address the mental exhaustion that had accumulated before their break. The complete removal of any aspect of their caring lives, being able to live something of a normal life away from caring, and attaining a sense of independence even for a while were important experiences that led to these reported improvements in well-being, also a novel contribution to the literature.
This research found carers describing experiences of loss relating to their sense of self because of the demands of caring. This was experienced in many ways, including through a lack of independence or freedom. Independence is an innate psychological need and any loss of it can have a detrimental impact on mental and physical health (Ryan & Deci, 2000). Identity theory suggests that a person’s sense of identity can change because of a situational change, such as illness; people see themselves as different than before (Heshmat, 2019). This was evident in this study as carers described the negative impact on their well-being, as well as a social withdrawal and shift in their personal and social identity.
Breaks did not appear to restore all their former social identities, or completely return them to a pre-caring state, but did allow them to continue to be part of important social groups which significantly improved their well-being. It is possible that more and longer breaks could allow carers to maintain more of those important aspects of self and social identities, leading to sustained mental well-being.
Carers are often concerned about the quality of care received by the cared-for-person in a temporary respite institution, which can affect their experience of a break (Maayan et al., 2014). Temporary institutional care settings need to be of good quality and provide good care for the carer to enjoy a complete physical and mental break (Shaw 2009). Trust in the respite facility is crucial (Shaw, 2009; Maffioletti et al., 2019, van Exel, 2006). This was consistent with the experiences of carers in this study, who identified the importance of trust and quality of care as being paramount to enable them to have the confidence to relax and enjoy their breaks, often with little or no guilt.
Carers also described experiences where respite facilities had not offered these assurances or quality, and as a result they had described breaks with little benefit and poorer outcomes. This is again consistent with other research, where experience of sub-standard care has been found to negatively impact the carer and reduce the effect of the respite service; in some cases, even leading to increased feelings of burden (Schoenmakers et al., 2010; Phillipson & Jones, 2011; Vandepitte et al., 2016; O’Connell et al., 2012).
This study found, similarly to existing literature, that positive effects from a break can sometimes be short-lived (Jardim & Pakenham, 2010). Despite being beneficial, the positive effects of the break did not last long, with some carers describing a deterioration in their mental and physical health beginning immediately following resumption of caring. This suggests that the all-consuming nature of caring can quickly impact on the quality of life of a carer even following a beneficial intervention such as a break. A break from caring should also be part of a wider package of support to enable the carer to keep caring. Understanding how all the various interventions interact with each other to effectively support carers is worthy of further study.
Many carers also talked about needing longer and more frequent breaks, and gaps between breaks being too long. This is something that is not present in the literature, perhaps due to the lack of in-depth research in this field to identify this issue. It is an important finding, as it demonstrates the value to the carer of experiencing a break, but also suggests that many carers’ needs are not being met through existing provision. This has implications for policy and practice, as breaks are often funded via public services. It raises questions around available resources and capacity for breaks and suggests that more should or could be done to provide much-needed breaks for carers.
The wider literature also suggests that breaks do not always benefit every carer, as was the experience of Iain in our study (Vandepitte et al., 2016). This demonstrates that policy interventions are rarely universally effective, and different models of respite should be explored and tailored to individual situations.
This study adds much needed carer perspectives on the experiences of breaks made possible by temporary residential care and extends the evidence base to include carers for people with conditions other than dementia.
It is important to consider that participants were recent and mostly regular users of the respite centre and knew of the role of the researcher as a trustee. This may have shaped the narrative they chose to share. However, the practice of reflexivity and transparency throughout the conduct of the research helped to ensure a rigorous approach, with use of non-leading questions, reassurances of confidentiality, and open sharing of stories, making full use of the dataset and allowing the data to speak for itself.
The purposive sample in this study includes carers from a range of backgrounds and circumstances (e.g. age, gender, disease, and relationship). There is limited diversity in terms of socio-economic status of participants, and further work is warranted to explore the needs of carers in more deprived circumstances.
Conclusions
This research reinforces the idea that breaks enable carers to continue in their caring role. Without breaks, carers are at risk of complete breakdown in their ability to carry on caring and the potential consequences that bring for themselves, the cared-for person, and the wider health and social care system. This study builds on the case for investment by policymakers in services that support carers to get a break. Such investments could address the emerging public health crisis facing carers as they struggle to get the support they need and want.
Footnotes
Ethical Approval
Certification of Institutional Favourable Ethical Opinion (with Modifications): The Usher Masters Research Ethics Group (UMREG), Usher Institute, University of Edinburgh has reviewed and given a favourable assessment to the following Master’s level student (Vandepitte et al., 2019) research project: Ethics ID: UM23119 on the 16th December 2022. Principal Investigator: Richard Meade. Supervisor(s): Debbie Cavers and Steph Grohmann. Study Title: ‘Understanding a break from caring: perspectives of informal carers’. Sponsor: ACCORD. Sponsor Number: AC22159. The UMREG operates in accordance with the guidelines set out by the Edinburgh Medical School Research Ethics Committee (EMREC).
Consent to Participate
All participants provided written informed consent prior to participating in the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article: This study was not funded. It was carried out by a student, the researcher, as part of their Master of Public Health requirements.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The lead Researcher was a trustee of the respite centre that supported the study at the time of the research being carried out. The respite centre’s database of clients/carers was where the sample of carers for this study was drawn from. The researcher took mitigations to manage this conflict of interest, which is described in the paper. Further details can be provided.
Data Availability Statement
The data that support the findings of this study are available on reasonable request from the corresponding author. The data are not publicly available as it may contain information that could compromise the privacy of research participants.