
Abstract
Maternal depression may have a significant impact on multiple aspects of parenting throughout childhood, leading to negative outcomes for children. However, the impact of depression on parenting perceptions, practices, and involvement may differ among mothers, particularly when protective factors are present. Using data from the Fragile Families and Child Wellbeing Study, we compared three aspects of parenting (perceptions, practices, and involvement) between depressed and non-depressed mothers, and then investigated the influence of interpersonal supports and community resources on these aspects of the parenting, specifically for depressed mothers. Findings indicated that mothers with depression were equally involved with the child at home, but were more likely to hold negative perceptions of parenting. Furthermore, interpersonal supports and community resources had an indirect impact on parenting practices and involvement through perceptions of parenting, highlighting the importance of interventions for mothers with depression that address the appraisal and expectations of parenting stress and competencies.
Keywords
Introduction
Mothers play a significant role in the developmental trajectories and outcomes of their offspring, with the maternal–child relationship representing one of the first and most influential social bonds a child will form in their life (Laible, Thompson, & Froimon, 2015). With that said, being a mother is challenging in itself; however, engaging in parenting becomes more difficult if also experiencing the symptoms of depression. Depression is a chronic, functionally debilitating psychiatric disorder characterized by persistently occurring dysphoria and/or anhedonia and other somatic, psychological, and behavioral symptoms (American Psychiatric Association, 2013). Maternal depression represents a significant public health concern, with a rate of 1 in 10 mothers and over 7 million children affected in a given year (Ertel, Rich-Edwards, & Koenen, 2011; Pratt & Brody, 2014). Of note, the rate of depression among mothers is highest during the first year after childbirth (up to 20%), but is a condition that remains prevalent well beyond the postpartum period (Ertel et al., 2011; Pratt & Brody, 2014). While there is a large body of literature has examined the impact of postpartum depression on maternal parenting, very few studies have considered the impact of maternal depression occurring later in childhood on parenting perceptions, practices, and involvement (Bernard et al., 2018; Field, 2010).
Maternal depression occurring across childhood has been consistently identified as an adverse childhood experience that increases the risk of immediate and long-term consequences related to physical health and psychological wellbeing outcomes for youth (Danese & McEwen, 2012; Felitti, 2009; Gilbert et al., 2015). Extant literature has documented that children of depressed mothers have higher levels of psychopathology and behavioral problems, as well as increased rates of poor physical health, like overweight, asthma, or frequent somatic complaints (Dow-Fleisner & Hawkins, 2018; Goodman & Gotlib, 1999; Lampard, Franckle, & Davison, 2014; Turney, 2011). One of the most well-documented mechanisms through which maternal depression negatively impacts child health and wellbeing is through disruptions in the maternal–child relationship, which may be related to differences in parenting perceptions, practices, and involvement (Dow-Fleisner & Hawkins, 2018; Farmer & Lee, 2011; Field, 2010; Gladstone et al., 2015; van Doorn et al., 2016; Villodas et al., 2018).
Maternal Depression and the Maternal Parenting
In general, depression is associated with impairments in daily living activities and social interactions, including those between mother and child. Thus, depression among mothers may negatively impact three important aspects of parenting, including the mother’s perception of parenting abilities, types of parenting practices employed, and involvement with the child (Dunst, Trivette, & Hamby, 2014; Farmer & Lee, 2011; van Doorn et al., 2016). Achieving parenting self-efficacy and mastery, maintaining consistent parenting practices, and meeting the daily emotional and physical needs of the child may be hindered as a result of the symptoms associated with depression (Farmer & Lee, 2011; Field, 2010). More specifically, mothers with depression may view parenting as more stressful and themselves as less competent as parents (Farmer & Lee, 2011; Hardie & Turney, 2017). Increased rates of stress and decreased rates of mastery may then lead to ineffective parenting behaviors, including an increased risk of harsh parenting practices and decreased parent involvement (Farmer & Lee, 2011; Gladstone et al., 2015; Reupert & Maybery, 2007). Finally, depression may lead to difficulty in attending to daily parenting tasks, including maintaining regular household routines or being involved in the child’s school environment. The symptoms associated with maternal depression increase the risk for impaired caretaking capacity, leading to a 10-fold greater odd of a poor maternal–child interaction (Goodman et al., 2011; Hardie & Turney, 2017; van Doorn et al., 2016).
However, not all mothers with depression will experience a break down in their parenting, underscoring the importance of examining differences in mother–child interactions for mothers with depression. Maintaining functional maternal–child interactions through positive parenting perceptions, practices, and involvement may act as a protective factor, thereby mitigating some of the negative effects maternal depression has on child health and wellbeing (Reuben & Shaw, 2015; Reupert, Drost, Nicholson, & van Doesum, 2014). Positive perceptions of parenting ability, consistent parenting practices, and regular parent involvement are important elements impacting the maternal–child relationship, and the ongoing health and wellbeing of both mother and child. Importantly, few studies have examined the mechanisms that support these aspects of parenting in the context of maternal depression (Goodman et al., 2011; Turney, 2012; van Doorn et al., 2016; Villodas et al., 2018). Identifying which factors support resilience in the parenting relationship is essential for informing policy and practices geared at supporting mothers with maternal depression, and by extension preventing poor child health and wellbeing.
Theoretical Framework: Resilience and Ecological Systems Perspectives
From a resilience perspective, individuals experiencing adversity, like depression, have the potential to withstand and thrive in spite of the presence of risk factors (Liebenberg & Ungar, 2009; Masten, 2015). This perspective suggests that not all individuals experiencing risk will go on to have negative outcomes, particularly when protective factors are present. Thus, a resilience framework supports that not all mothers experiencing depression will have difficult in parenting, especially if they have access to protective factors, like interpersonal supports and community resources. In order to identify potential protective factors, the resilience perspective is often utilized in conjunction with the ecological systems theory.
From an ecological systems theory perspective, individuals are understood in the context of mutually reciprocal systems that directly and indirectly influence developmental trajectories and outcomes (Bronfenbrenner, 1986; Bronfenbrenner & Morris, 2006). An ecological systems perspective includes five major systems that surround the child: 1) microsystem, 2) mesosystem, 3) exosystem, 4) macrosystem, and 5) chronosystem. The microsystem includes those with a direct relationship to the child and the mesosystem represents the relationships between the child and those in the microsystem (Bronfenbrenner, 1986). Maternal depression is a risk factor that exists within the microsystem that may negatively impact both the child and maternal–child interactions (mesosystem). However, exosystem factors including interpersonal supports and community resources impact both the mother and child, individually, as well as the ways in which the mother parents (Bronfenbrenner & Morris, 2006; Zhang, Eamon, & Zhan, 2015).
Importantly, research has identified that a negative neighborhood context (e.g., lack of cohesion or safety) and limited interpersonal supports increase the risk of negative outcomes for mothers and children, especially when coupled with other risk factors like maternal depression (Dunst et al., 2014; World Health Organization, 2014; Zhang et al., 2015). Higher levels of neighborhood disorder and a lack of social support can lead to increases in parenting stress, specifically for single mothers (Zhang et al., 2015). Furthermore, lower levels of social support and community order lead to an increased risk of negative parenting practices, including child maltreatment (Abner, 2014). Research has specifically focused on how a lack of social support and negative environmental experiences increase risk, but few have examined the impact of noted protective factors (Dunst et al., 2014; World Health Organization, 2014; Zhang et al., 2015). For example, interpersonal support and community resources may promote positive maternal–child interactions and mitigated the impact of depression on parenting perceptions, practices, and involvement. Given the importance of maternal–child interactions, it is important to identify factors supporting mothers with depression in the ways in which they parent.
Study Purpose and Aims
Framed by the resilience and ecological systems perspectives, this study focused on how parenting perceptions, practices, and involvement were impacted by perceived interpersonal support and community resources, with a specific focus on mothers experiencing depression. First, the current study examined the differences between depressed and non-depressed mothers on three aspects of parenting, including 1) perceptions of parenting stress and abilities, 2) parenting discipline practices, and 3) parent academic and home involvement for children aged 9 years old. Second, this study explored how interpersonal supports (e.g. instrumental and emotional supports) and community resources (e.g. neighborhood cohesion and safety) impacted those three aspects of the parenting, specifically among mothers with depression.
Methods
Data for these analyses were drawn from the Fragile Families and Child Wellbeing (FFCWB) study, a longitudinal, cohort study of 4898 children born in medium to large US cities between 1998 and 2000 to mainly single mothers (Reichman et al., 2001; Waldfogel et al., 2010). The FFCWB study conducted interviews with biological mothers at or around the time of the child’s birth, and then followed up 1, 3, 5, and 9 years after baseline (Bendheim-Thoman Center for Research on Child Wellbeing (Bendheim-Thoman, 2008, 2bib_btcrcw_2011011)). The FFCWB study includes data related to child health and wellbeing, maternal health and wellbeing, economic status, parenting practices, social support and neighborhood cohesion, and other demographic characteristics (Bendheim-Thoman, 2011).
There were two study samples utilized for these analyses. Initial bivariate analyses utilized a study sample that included 3212 observations from mothers who completed the 9-year follow-up with valid data for maternal depression. Observations were excluded if the child had a serious physical disability (e.g. Cerebral Palsy, Down’s Syndrome, n = 109) or did not live with the mother at least halftime at the 9-year follow-up (n = 208). In total, 613 mothers met criteria for past-year depression at the 9-year follow-up. However, 28 were excluded because their child had a serious physical disability and 66 were excluded because the mother was not the primary caregiver, with some mothers meeting both criteria. Subsequent multivariate analyses were conducted with 522 mothers with depression at the 9-year follow-up.
Measurement
Maternal Depression
Past 12-month depression diagnosis for mothers was assessed using the World Health Organization (WHO) Composite International Diagnostic Interview-Short Form (CIDI-SF) (World Health Organization, 1994). Past 12-month major depressive disorder was present if the mother endorsed either dysphoria or anhedonia on most days for at least 2 weeks and at least 3 additional symptoms (e.g. weight loss, suicidality, etc.). Mothers reporting taking medications for depression at the 9-year follow-up (n = 10) were not asked about symptoms, but were coded as having a depressive disorder (Bendheim-Thoman, 2011).
Maternal Parenting
The maternal parenting included items related to three broad areas: 1) perceptions of parenting; 2) parenting practices, and 3) parent involvement. Perceptions of parenting included two scales: 1) mother-reported parenting stress and 2) mother-reported parenting competence. Parenting stress was measured using the summed scaled score of four items from the Parenting Stress Inventory, related to difficulty of parenting, feeling trapped by parenting responsibilities, a lack of pleasure in parenting tasks, and feeling worn out by parenting responsibilities (Abidin, 1995). Items were measured on a 4-point Likert scale (0 = strongly disagree to 3 = strongly agree), with a higher score indicating greater stress related to being a parent. The Cronbach’s alpha for the final study sample was 0.70. Parenting competence was measured using a summed scaled score of three items related to perceptions of self as a good parent, feelings of closeness to the child, and ability to communicate with the child (Blumberg et al., 2005). Items were from the caregiver–child relationship scale taken from the Family Functioning section of the National Survey of Child Health (NSCH) and have strong face validity (Bendheim-Thoman, 2011). Items were measured on a 4-point Likert scale (0 = not at all to 3 = extremely well), with a higher score indicating greater levels of competence. The Cronbach’s alpha for the study sample was 0.59.
Parenting practices related to types of disciplinary techniques mothers may employ was measured using the three subscales of the Parent–Child Conflict Tactics Scale (Straus, 1979): 1) nonviolent discipline, 2) physical assault, and 3) psychological aggression. The nonviolent discipline subscale has four items, with items like putting the child in “time out” or taking away privileges (Cronbach’s alpha = 0.81). The physical assault subscale consists of five items, including whether the mother ever pinched, slapped, or shook the child (Cronbach’s alpha = 0.75). The psychological aggression subscale had five items, including items related to cursing at the child or threatening to hit the child (Cronbach’s alpha = 0.60). Item responses were initially on a 7-point scale, with 0 (never or not in the past year) to 6 (more than 20 times). Items were coded using the yearly frequency method, which produces a summed scaled score of frequency estimates for disciplinary techniques ranging from 0 to 100 for nonviolent discipline scale and 0–125 for psychological aggression and physical assault scales (Bendheim-Thoman, 2011).
Finally, parent involvement was measured using two scales, one focusing on involvement at home and the other at school. Home involvement included 10-items related to past-month interactions between the mother and child in the home. Mothers were asked how often she engaged in activities with her child related to household routines (e.g. doing chores together), recreational activities (e.g. playing outside together), and academic support at home (e.g. helped with homework). Responses were on a 5-point Likert scale (0 = not once in past month to 4 = everyday), and were used to generate a summed scaled score, with a higher score representing more parent involvement at home. The Cronbach’s alpha for the study sample was 0.70. School involvement included 6-items related to past-year interactions between the mother and the child’s school. Mothers were asked how often she attended school functions (e.g. open house, class/school event), volunteered at the child’s school, and visited the child’s classroom. Of note, items related to potential academic problems (e.g. conference with school counselor or principal) were excluded. Responses were on a 3-point Likert scale (0 = never to 2 = more than once) and were used to generate a summed scaled score, with a higher score representing more parent involvement at school. The Cronbach’s alpha for the study sample was 0.72.
Interpersonal Support
Interpersonal support included two count variables related to perceived instrumental and emotional support. Perceived instrumental support was measured using the 5-item Instrumental Social Support Measure (Reid & Taylor, 2015). Mothers indicated whether or not she could count on someone to provide different types of financial support (e.g. loan $200 or cosign for bank loan), a place to live if homeless, and emergency child care if needed. Items were summed to create count variable ranging from 0 (no supports) to 5 (all supports listed), with a higher value indicating more perceived instrumental supports. Perceived emotional support included whether or not the mother could get help or advice from 5 different potential supports: 1) her parents, 2) the child’s father, 3) the child’s father’s parents or relatives, 4) friends, neighbors, coworkers, or 5) other relatives. Items were used to generate a summed score ranging from 0 (no supports) to 5 (all supports listed), with a higher value representing access to more social supports for help or advice.
Community Resources
Community resources included two measures related to neighborhood cohesion and safety. Neighborhood cohesion was measured using the validated 5-item Social Cohesion and Trust Scale (Sampson et al., 1997). Items asked mother’s level of agreement on the following statements: 1) willingness of neighbors to help, 2) neighborhood is viewed as close-knit, 3) people generally do not get along with each other, 4) people do not share the same values, and 5) gangs are a problem in the neighborhood, using a 4-point Likert scale (0 = strongly disagree to 3 = strongly agree). Items 3, 4, and 5 were reverse coded so that a lower level of agreement was indicative of more cohesion. After recoding, a summed scaled score was generated, with higher score representing higher levels of neighborhood social cohesion. The Cronbach’s alpha for the study sample was 0.78. Finally, neighborhood safety was a dichotomous single-item indicator. Mothers were asked if they were afraid to let the child go outside because of violence in the neighborhood, which was recoded so a yes response indicates neighborhood safety.
Covariates
These analyses also controlled for child, maternal, and family factors. Child factors included child sex (0 = male, 1 = female) and child age in years. Maternal factors included age in years, race/ethnicity (0 = Non-Hispanic white, 1 = Non-Hispanic Black, 2 = Hispanic or other), education (0 = less than high school, 1 = high school, 2 = more than high school), current marital status (0 = married, 1 = single), and the number of children in the household. Finally, current family income-to-poverty ratio based on the annual poverty thresholds established by the US Census Bureau was included (Bendheim-Thoman, 2011). Covariates were selected based on recommendations by Bendheim-Thoman Center for Research on Child Wellbeing (2011) to account for sampling design, which oversampled for Black and unmarried mothers.
Analytic Approach
These analyses were conducted in two phases. First, we examined differences in perceptions of parenting, parenting practices, and parent involvement between mothers with past 12-month depression as compared to those without a current diagnosis of depression. For all significant tests, we estimated the effect size for t-test and chi-square analyses by calculating Cohen’s d (Cohen, 1988) or Cramer’s V (Tomczak & Tomczak, 2014), respectively. Cohen’s d of 0.20 indicates a small effect size, 0.50 indicates medium effect size, and 0.80 indicates a large effect size (Cohen, 1988). For Cramer’s V, effect size is determined in conjunction with the degrees of freedom (df). For a df equal to 1, Cramer’s V of 0.10 indicates small effect size, 0.30 indicates medium effect size, and 0.50 indicates a large effect size, whereas when the df is equal to 5, Cramer’s V of 0.07 indicates small effect size, 0.21 indicates medium effect size, and 0.35 indicates a large effect size. Second, we narrowed the sampling frame to focus only on mothers with depression. Initially, we conducted a series of multivariate regression analyses to examine the relationship between each outcome related to parenting perceptions, practices, and involvement with interpersonal and community resources for mothers with depression, adjusting for covariates. We then examined the association between perceptions of parenting with parenting practices and involvement for depressed mothers, adjusting for covariates. All adjusted regression models were assessed for multicollinearity using tolerance and variance inflation factor (VIF). Tolerance ranged between 0.843 and 0.977 and the VIF ranged between 1.02 and 1.18 across all models, which meets the accepted levels of tolerance and VIF (values closest to 1 indicate no problems with multicollinearity) (Hair et al., 1995). Next, we conducted structural equation model (SEM) analyses to examine the impact of interpersonal and community resources on parenting perceptions, and then perceptions on parenting practices and involvement. All models controlled for the covariates described above. SEM model fit indices included the overall model chi-square, comparative fit index (CFI), root mean square error of approximation (RMSEA), and standardized root mean square residual (SRMR). A nonsignificant chi-square, a CFI of 0.95 or greater, an RMSEA of 0.05 or lower, and an SRMR of 0.05 or lower indicate acceptable model fit (Kline, 2015). Finally, Little’s Missing Completely at Random (MCAR) test showed that missing data for key variables were missing completely at random (χ2 (65) = 81.3, p = 0.084). Based on the data being MCAR, missing data were treated with maximum likelihood estimation (Acock, 2005). Although survey weights were not used, the variables used to generate survey weights were included in multivariate regression and SEM analyses and robust standard errors were estimated per recommendation by the Fragile Families investigators (Bendheim-Thoman, 2008). All analyses were conducted in Stata 13/SE (StataCorp, 2013).
Results
Descriptive Statistics for Key Variables by Maternal Depression.
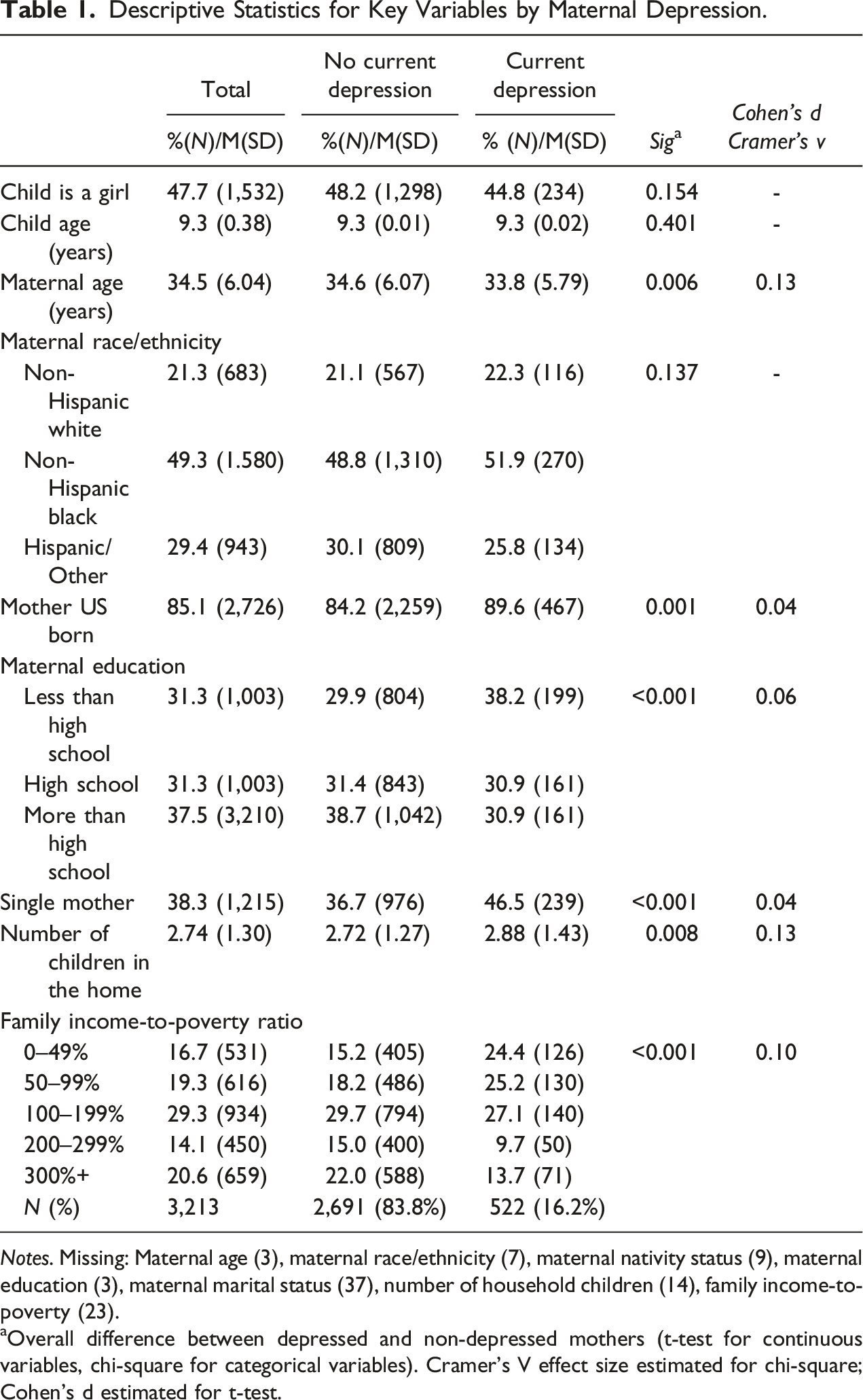
Notes. Missing: Maternal age (3), maternal race/ethnicity (7), maternal nativity status (9), maternal education (3), maternal marital status (37), number of household children (14), family income-to-poverty (23). aOverall difference between depressed and non-depressed mothers (t-test for continuous variables, chi-square for categorical variables). Cramer’s V effect size estimated for chi-square; Cohen’s d estimated for t-test.
Maternal parenting factors, interpersonal supports, and community resources by depression.
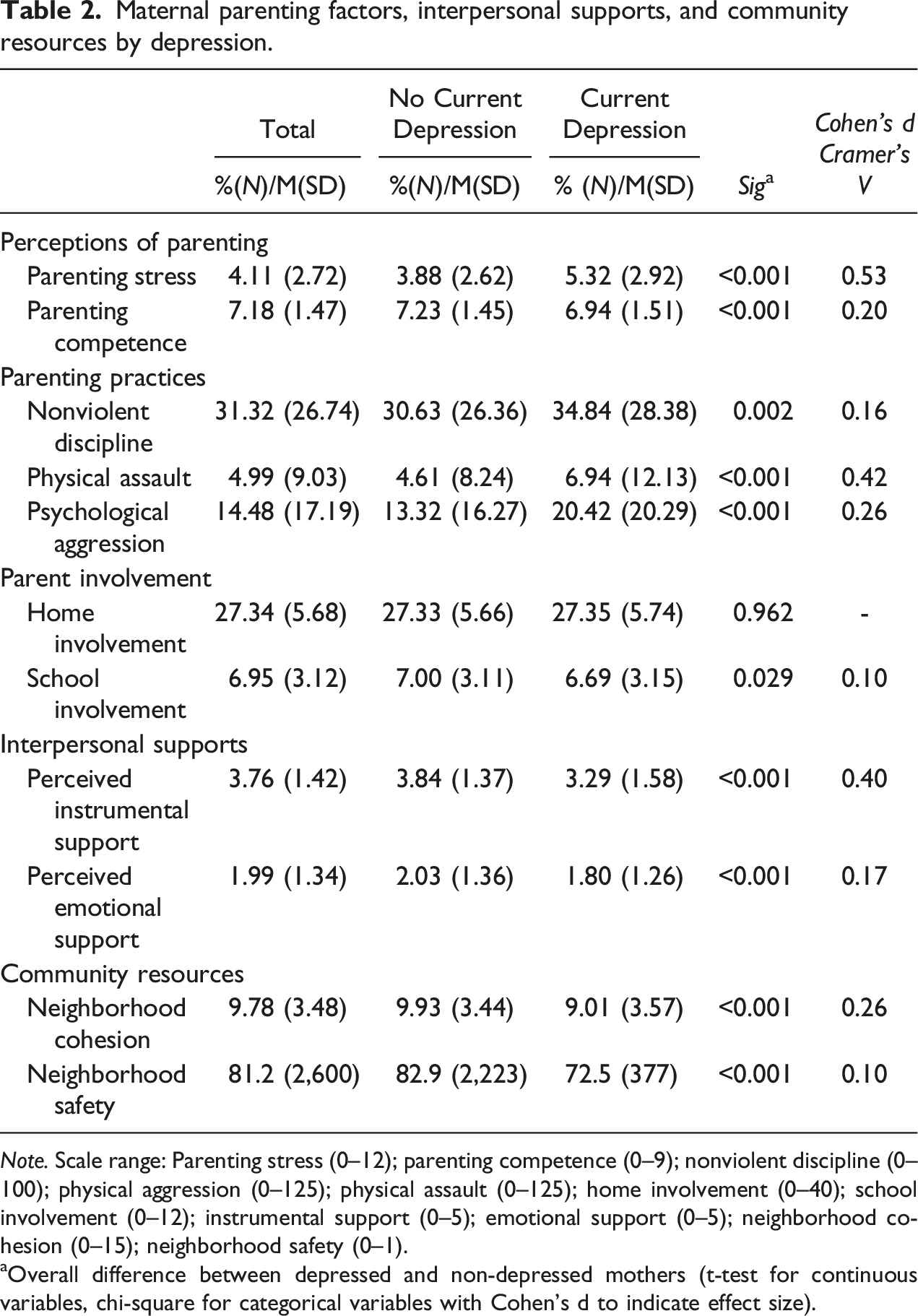
Note. Scale range: Parenting stress (0–12); parenting competence (0–9); nonviolent discipline (0–100); physical aggression (0–125); physical assault (0–125); home involvement (0–40); school involvement (0–12); instrumental support (0–5); emotional support (0–5); neighborhood cohesion (0–15); neighborhood safety (0–1).
aOverall difference between depressed and non-depressed mothers (t-test for continuous variables, chi-square for categorical variables with Cohen’s d to indicate effect size).
Independent Associations Between Maternal Parenting Perceptions, Practices, and Involvement with Interpersonal Supports and Community Resources Reporting Standardized Coefficients and Robust Standard Errors.
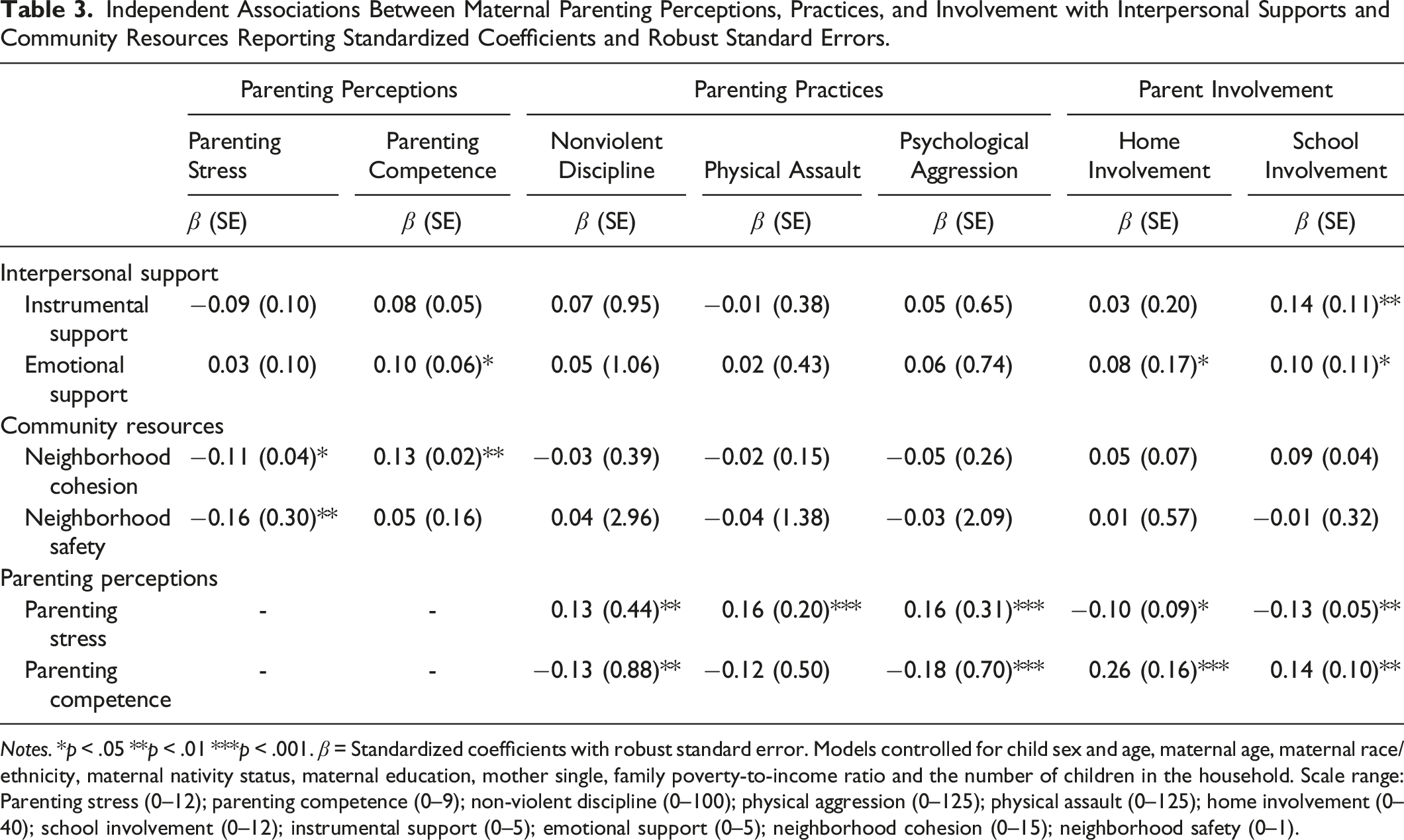
Notes. *p < .05 **p < .01 ***p < .001. β = Standardized coefficients with robust standard error. Models controlled for child sex and age, maternal age, maternal race/ethnicity, maternal nativity status, maternal education, mother single, family poverty-to-income ratio and the number of children in the household. Scale range: Parenting stress (0–12); parenting competence (0–9); non-violent discipline (0–100); physical aggression (0–125); physical assault (0–125); home involvement (0–40); school involvement (0–12); instrumental support (0–5); emotional support (0–5); neighborhood cohesion (0–15); neighborhood safety (0–1).
For depressed mothers, greater parenting stress was associated with higher rates of nonviolent discipline (b = 1.22, p = 0.005), physical assault (b = 1.08, p = 0.001), and psychological aggression (b = 0.68, p = 0.001), with lower rates of home (b = −0.19, p = 0.031) and school involvement (b = −0.14, p = 0.003), controlling for covariates. Conversely, greater parenting competence was related to lower rates of nonviolent discipline (b = −2.49, p = 0.005) and psychological aggression (b = −2.35, p = 0.001), with higher rates of home (b = 0.98, p < 0.001) and school involvement (b = 0.30, p = 0.002), adjusting for covariates.
Finally, an SEM model was conducted to simultaneously estimate interpersonal support and community resources on parenting perceptions, and then parenting perceptions on parenting practices and involvement (Figure 1). The final model had acceptable fit, with a nonsignificant chi-square (χ2(6) = 8.11, p = 0.230), an RMSEA of 0.028, 90% CI [0.00–0.71], a CFI of 0.997, and an SRMR of 0.007. The model allowed for covariance of the error terms between each aspect of the parent–child relationship (i.e. parenting perceptions, parenting practices, and parenting involvement, separately). Overall, the model explained 46.7% of the variance in all estimated endogenous outcomes (perceptions of parenting, parenting practices, and parent involvement) related to the parent–child relationship (R
2
= 0.47). By outcome, the model accounted for 5.6% of the variance of parenting stress, 8.1% of parenting competence, 15.2% of nonviolent discipline, 10.0% of physical assault, 17.3% of psychological aggression, 18.3% of home involvement, and 12.7% of school involvement. Structural model for the effect of interpersonal support and community resources on parenting perceptions and behaviors. Notes. χ2 (6) = 8.11, p = 0.230; RMSEA = 0.028, 90% CI [0.00–0.07]; CFI = 0.997; SRMR = 0.007; R2 = .463. N = 460; non-significant paths between interpersonal and community resources and parenting practices/involvement are not pictured. Model controls for: child sex, child age, maternal age, maternal race/ethnicity, maternal education, maternal marital status, number of children in the home, and family income-to-poverty ratio.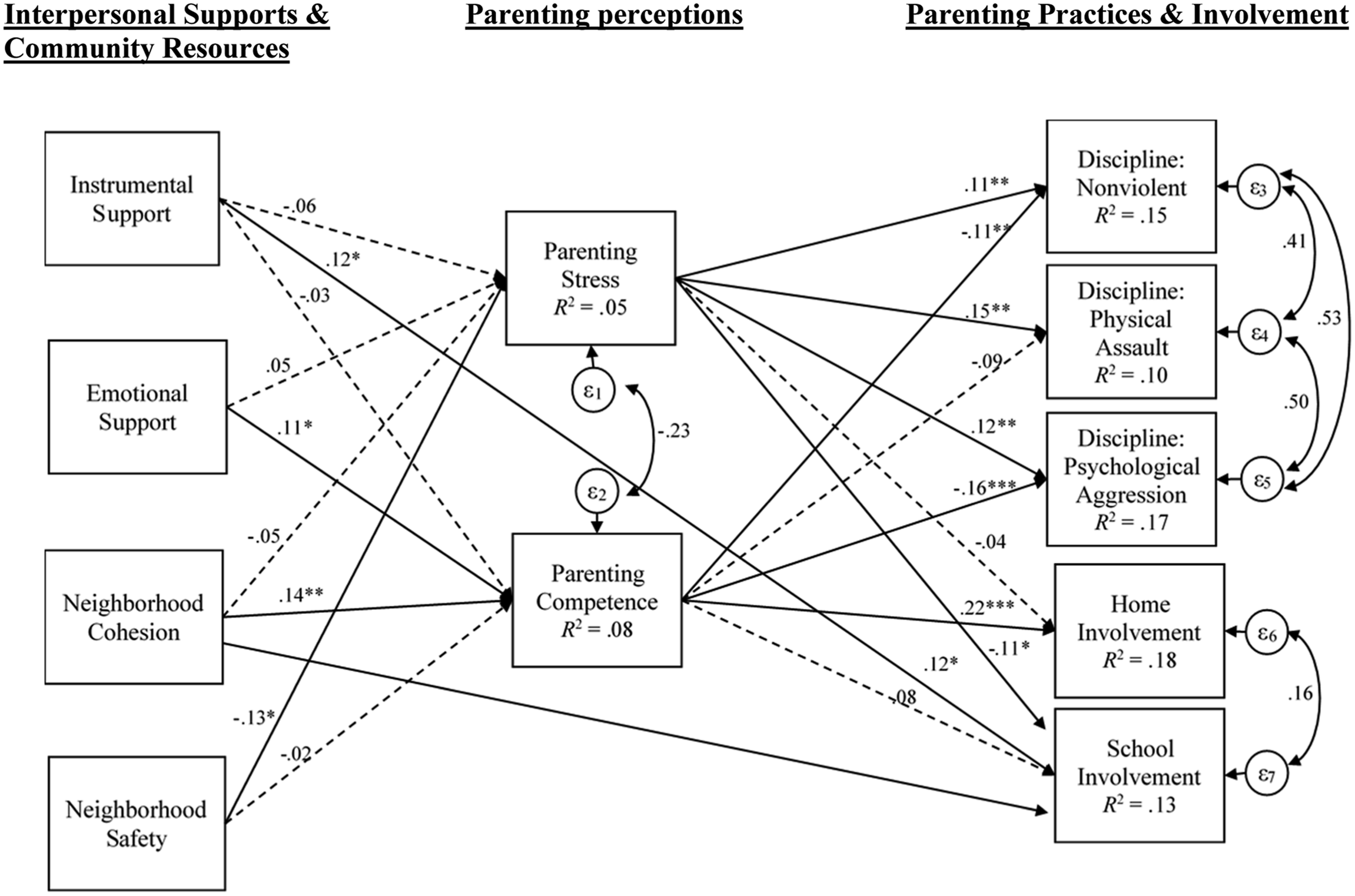
When controlling for covariates, results indicated that higher levels of both emotional support and neighborhood cohesion were associated with greater parenting competence. On the other hand, only neighborhood safety was associated with lower parenting stress. Additionally, parenting stress was associated with increased rates of nonviolent discipline, physical assault, and psychological aggression, and lower rates of academic involvement, but was not associated with home involvement. Parenting competence was associated with decreased rates of nonviolent discipline and psychological aggression, and higher rates of home involvement, but did not predict physical assault or school involvement.
Finally, instrumental support and neighborhood cohesion were related to an increased rate of school involvement. No other interpersonal supports or community resources were directly associated with parenting practices or involvement. Finally, we estimated the indirect effects of interpersonal supports and community resources on parenting practices and involvement through perceptions of parenting. Neighborhood cohesion had a significant indirect effect on psychological aggression (β = −0.16, p = .035) and home involvement (β = 0.05, p = .019). There were no other significant indirect effects.
Discussion
The overall aim of this study was to examine three aspects of parenting for mothers with depression and explore the influence of protective factors, with the understanding that a disruption to this social bond is a critical factor for child health and wellbeing (Gladstone et al., 2015; Reuben & Shaw, 2015; Reupert et al., 2014). Findings suggest that mothers with depression were less likely to hold positive parenting perceptions, were at a greater risk of engaging in negative parenting practices, and were less likely to be involved at the child’s school as compared to non-depressed mothers. Yet, there was no difference in involvement at home between mothers with or without current depression, suggesting that mothers with depression are engaging with their child’s home routines at the same level as mothers without depression. Furthermore, mothers with depression reported fewer interpersonal supports and community resources than non-depressed mothers, which is consistent with extant literature (World Health Organization, 2014).
When examining the impact of these protective factors among depressed mothers, we found that interpersonal supports and community resources did not have a direct impact on parenting practices and, separately, community resources were not associated with parent involvement. However, interpersonal supports were associated with increased home and school involvement. Notably, parenting perceptions were the greatest predictors of practices and involvement. Specifically, parenting competence was associated with fewer disciplinary practices, whereas parenting stress indicated the opposite, highlighting the importance of parenting perceptions for mothers with depression. These findings were consistent with previous literature (Farmer & Lee, 2011; Turney, 2012; van Doorn et al., 2016) and suggest that the perceptions mothers holds about parenting stress and competence plays an important role in the way they discipline and interact with their children.
Our findings extend the current literature by examining the influence of positive environmental factors on the aspects of parenting for mothers with depression. We found that neighborhood cohesion and interpersonal supports directly impacted perceptions of parenting. Consistent with research focusing on single and low-income women (Abner, 2014; Dunst et al., 2014; Zhang et al., 2015), we found that higher levels of support and cohesion were associated with positive outcomes in mothers with depression. In particular, these factors were related to higher levels of parenting competence and lower levels of parenting stress. Furthermore, higher levels of neighborhood cohesion were associated with decreased rates of psychological aggression and increased rates of home involvement indirectly through perceptions of parenting. Utilizing an SEM approach provided important information as to the interplay between these protective factors and three aspects of maternal parenting. Grounded in ecological systems and resilience perspectives, these findings provide empirical support underscoring the importance of external resources, like instrumental or emotional support, neighborhood cohesion, and neighborhood safety, for the supporting positive parenting in the context of maternal depression.
Limitations
This study had some notable limitations. First, the maternal parenting was measured using scales related to parenting perceptions, practices, and involvement, but did not include a measure parenting quality (e.g. warmth or hostility). Maternal warmth and hostility are common quality indicators that may impact the degree to which involvement is beneficial or detrimental to the child (van Doorn et al., 2016), but were not available in these data. Additionally, the maternal–child relationship was measured exclusively using self-report, and did not take into account the child’s perception of the relationship or include interviewer observations. Future research should include a measure of relationship quality, as well as reports from other respondents. It is also important to note the maternal competence scale had only three items and used a four point scale, suggesting the need for a more comprehensive and sensitive measure. Second, our analyses focused on a sample of mothers with depression, but did not include a measure of symptom onset, severity, or chronicity, which may impact the maternal–child relationship. Symptom onset that occurs during the postpartum period may negatively impact early attachment, leading to difficulties that persist throughout childhood. Future analyses should take into account the timing, severity, and onset of symptoms. Finally, it is important to note that these indicators were measured concurrently and do not include the temporal order necessary to establish causality. Future studies should replicate these findings at different time points, and utilize a longitudinal approach to examine change overtime.
Implications
Given the importance of the parenting across childhood and the potential negative effects of maternal depression, understanding how mothers maintain a positive relationship with their children is essential for supporting optimal child health and wellbeing (Farmer & Lee, 2011; van Doorn et al., 2016). This study extends the literature by utilizing a strengths-based approach to examine the impact of protective factors on parenting in the context of maternal depression later in childhood, which has been rarely considered (Farmer & Lee, 2011; Feldman, 2007; Field, 2010; van Doorn et al., 2016). Study findings contribute to our understanding of three aspects of parenting (perceptions, practices, and involvement) for mothers with depression, and highlight the pathways through which interpersonal support and community resources impact parenting perceptions, practices, and involvement. Of note, these aspects of the maternal–child relationship examined are ones that social workers and clinical practitioners may have the greatest influence.
Importantly, these findings emphasis the need for continued screening for maternal depression and other mental illnesses during well-child check-ups throughout childhood, and not just during the recommended first year of life (Kerker et al., 2016). Findings from this study provide support for a two-generation approach to address maternal depression and improve child health and wellbeing (Schmit, Matthews, & Golden, 2014). Children experiencing maternal depression with a more positive maternal–child relationship may be at less of a risk of developing negative outcomes (Farmer & Lee, 2011; Feldman, 2007; Hardie & Landale, 2013; Repetti, Taylor, & Seeman, 2002). Utilizing a two-generation approach in primary care settings could provide important opportunities to support children and mothers experiencing risk. Two-generation programs (e.g. Head Start) have been successful in meeting the needs of both child and mother (Schmit et al., 2014), yet many of them focus only on very young children, which may fail to meet the needs of older children.
Of note, we found depressed mothers were equally involved with their child at home, but more likely to hold negative views of their parenting competency and perceived parenting as more stressful. Thus, primary care setting should provide mothers who screening positive for depression with psychoeducation related to typical parenting experiences that address the appraisal of parenting stress and competence. In addition, mothers with depression should be referred to programs that provide training for more adaptive parenting practices and offer guidance in how mother should engage with their offspring. Importantly, these programs must be developmentally informed, taking into account the changing social, emotional, and physical needs across childhood. Furthermore, referrals through child primary care settings may be most beneficial, as mothers experiencing depression may not seek help specifically related to their mental health concerns, but may be involved in their child’s healthcare needs (Coiro, 2015; Mishina & Takayama, 2009).
Additionally, these results showed that external supports have an important influence on perceptions of parenting, yet mothers with depression reported fewer interpersonal supports and community resources that non-depressed mothers. Thus, mothers with depression should be provided with support in identifying interpersonal supports, developing community resources, and building social capital. These programs should go beyond just addressing problems (i.e. preventing maltreatment), and instead should incorporate capacity-building (Dunst & Trivette, 2009). Again, noting that mothers may not independently seek out help related to their depression, parenting program should be incorporated into other community events. Community-based parenting support groups may provide mothers with the opportunity to build interpersonal supports and community resources, thereby supporting the potential for a positive maternal–child relationship despite maternal depression (England & Sim, 2009). In particular, programs like Promising Neighborhoods (Abner, 2014) are intended to build community support systems and improve resources for at-risk neighborhoods, and should include specific elements related to depression among mothers.
Finally, future studies should consider how the quality of the maternal–child relationship impacts parenting perceptions, practices, and involvement, as well as the degree to which negative perceptions impact the quality of this bond. Research should examine qualitatively how depressed mothers see themselves as parents, which may provide important context as to the pathways through which maternal depression impacts child health and wellbeing. Additionally, it is important to consider there may be differences in parenting experiences across mothers with diverse ethno-racial identities. Future research should more fully examine parenting experiences for Black, Indigenous, and Mothers of Color, taking into account the complex relationship between mental health, parenting, and systemic oppression. Furthermore, future research should consider the role of other family members. From a family systems and ecological systems perspective, a positive father–child or sibling relationship may mitigate the impact of a negative maternal–child relationship. Research in this area should continue to utilize a resilience perspective that focuses on identifying the impacts and interplay of both risk and protective factors.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.