
Abstract
Raising a child with autism spectrum disorder (ASD) can be a very stressful experience, impacting parents and their ability to take care of their child. We examined the relationship between parenting stress and child, and parent and contextual factors in a sample of 61 families of children with ASD recruited in a centre for ASD assessment and treatment. Results showed that mothers had a higher level of stress related to their parental role when compared to fathers. Data also showed the importance of considering the specific role of parental emotion regulation, family functioning and educational level in influencing maternal stress and the specific role of couple adjustment in influencing fathers’ parental distress. This study pointed out the importance of employing a vision that embraces different domains of family life in cases of children with ASD and in parents’ intervention programmes because these factors may contribute to parental stress.
Introduction
Raising a child with autism spectrum disorder (ASD) can be a stressful experience that impacts the entire family system (DePape & Lindsay, 2015; Karst & Van Hecke, 2012; Pisula & Porębowicz-Dörsmann, 2017; Smith, Greenberg, & Mailick, 2014). Taking care of a child with ASD can increase general stress levels beyond the stress levels associated with parenting typically developed children and children with other neurodevelopmental disabilities (e.g. Estes et al., 2013; Hayes & Watson 2013; Ilias, Cornish, Kummar, Park, & Golden, 2018). These high levels of stress can significantly compromise the parent–child relationship, showing the strain related to caring for a child with ASD (Bonis, 2016; Shepherd, Landon, Taylor, & Goedeke, 2018).
According to Abidin’s model (1995), parental cognitions and perceptions may influence the development of parental stress, which in turn increases negative parenting behaviours. The contributions to parenting stress are manifold and can be divided into child, parent and contextual factors. Within this framework, our study aimed to determine whether mothers and fathers report similar or different levels of parenting stress and also to clarify the role of gender; chronological age and ASD severity among the child factors; the role of parents’ educational level and emotion regulation among the parent factors; and the role of couple satisfaction, family functioning and length of ASD intervention among the contextual factors in influencing parenting stress.
Parental Gender
The literature investigating differences in parental stress with respect to the gender of the parents is not entirely in agreement. A number of studies have concluded that mothers of children with ASD experience significantly greater levels of stress than fathers (Ang & Loh, 2019; Dabrowska & Pisula, 2010; Jones, Totsika, Hastings, & Petalas, 2013; McStay, Dissanayake, Scheeren, Koot, & Begeer, 2014; Pisula & Porębowicz-Dörsmann, 2017; Tehee, Honan, & Hevey, 2009). On the contrary, some studies (Hastings, 2003; Davis & Carter, 2008; Nikmat, Ahmad, Oon, & Razali, 2008) found no differences in parental stress between mothers and fathers. Finally, Rivard and colleagues (Rivard, Terroux, Parent-Boursier, & Mercier, 2014) stated that fathers reported a significantly higher level of stress than mothers but, to our knowledge, this result was not replicated in subsequent studies. However, most of the studies recruited samples of mothers, failing to investigate the father’s perspective in parenting a child with ASD (Johnson & Simpson, 2013; Rankin, Paisley, Tomeny, & Eldred, 2019) and highlighting the importance of further studies in this field.
Child Factors
Regarding the relationship between children’s age and parental stress, some studies suggested that higher levels of stress in parents were related to younger ages of children with ASD (Lounds, Seltzer, Greenberg, & Shattuck, 2007; Smith, Seltzer, Tager-Flusberg, Greenberg, & Carter, 2008), but other studies found opposite results, showing lower levels of stress in parents of younger children with ASD (Rivard et al., 2014; Tehee et al., 2009). Furthermore, some studies found a significant relationship between children’s gender and parental stress: fathers of girls reported higher levels of stress compared to fathers of boys in the study by Rivard et al. (2014) and parents of girls reported higher levels of stress than parents of boys in the study by Zamora, Harley, Green, Smith, and Kipke. (2014). In other studies on children with ASD, neither children’s gender nor age was found to be significantly related to parenting stress (Amireh, 2019; McStay et al., 2014; Peters-Scheffer, Didden, & Korzilius, 2012; Valicenti-McDermott et al., 2015).
Research on the associations between parental stress and ASD severity showed significant relationships in numerous works (Ilias et al., 2018; Ingersoll & Hambrick, 2011; Miranda, Berenguer, Rosello, & Baixauli, 2019; Pastor-Cerezuela, Fernández-Andrés, Pérez-Molina, & Tijeras-Iborra, 2020; Rivard et al., 2014; Tomeny, 2017), but one article (Xue, Ooh, & Magiati, 2014) showed relatively low levels of stress and a mild interference of ASD symptoms in parental lives, and other studies showed no significant relationships between these two variables (Manning, Wainwright, & Bennet, 2011; Peters-Scheffer et al., 2012). Therefore, the link between the child factors examined and parental stress showed contrasting results, paving the way for subsequent studies.
Parent Factors
As stated above, parenting stress depends on a set of variables that includes the personal characteristics of parents, among which we focused on educational level and emotion regulation.
Literature on the relationship between parents’ level of education and parental stress is still weak, with some studies showing no differences between the level of maternal/parental education and stress (Nikmat et al., 2008; Valicenti-McDermott et al., 2015) and only one study (Rivard et al., 2014), to our knowledge, showing that maternal level of education (but not paternal) and waiting times for services predicted mothers’ scores on stress related to parent–child interaction.
Furthermore, despite substantial agreement about the relationship between parental emotion regulation and parental well-being (Costa, Steffgen, & Ferring, 2017; Hirschler-Guttenberg, Golan, Ostfeld-Etzion, Feldman, 2015; Predescu & Şipoş, 2017), there are no studies that clarify the relationship between emotion regulation and parental stress in families of children with ASD. In particular, more studies are needed to better understand the nature and predictors of these factors on parental stress.
Contextual Factors
The contextual factors included within this study are couple satisfaction, family functioning and length of ASD intervention.
Significant results have been found concerning the relationship between parenting stress and couple outcome in families of children with ASD (Hartley, Papp, & Bolt, 2016; Weitlauf, Vehorn, Taylor, & Warren, 2014). Regarding the specific relationship between stress and couple satisfaction, a 2016 review (Sim, Cordier, Vaz, & Falkmer, 2016) showed that child behaviour, parenting stress and psychological well-being represent risk factors for relationship satisfaction in families raising children with ASD. These data are confirmed by more recent studies showing a negative association between relationship satisfaction and family stress in families of children with ASD (Brown, Whiting, Kahumoku‐Fessler, Witting, Jensen, 2020; Guerriero, Fioravanti, Petrillo, Di Renzo, & Zavattini, 2017; Sim, Cordier, Vaz, Parsons, & Falkmer, 2017, 2018), supporting the hypothesis that relationship satisfaction could represent a protective factor in the process of parental adaptation to an autism diagnosis.
Regarding family functioning, several studies have found a significant relationship between parental stress and other aspects such as the isolation of mothers (Johnson & Simpson, 2013), quality of life (Pisula & Porębowicz-Dörsmann, 2017), children’s behavioural problems, coping strategies and social support (Zaidman-Zait et al., 2017). Two years after the first evaluation, this study also found that family functioning, maternal coping strategies and social support predicted parental stress levels.
Finally, researchers have demonstrated extensively that interventions for children and/or families can improve several outcomes for both children with ASD and their parents (e.g. (Di Renzo et al., 2015; Leaf et al., 2017; Parsons et al., 2019; Prata, Lawson, & Coelho, 2018; Zhou et al., 2018). Nevertheless, to our knowledge, no study has considered whether the length of treatment might affect parental stress.
Summary
Given the literature presented above on parents of children with ASD, we have found that numerous studies show greater levels of stress in mothers than fathers; however, further studies are needed to better understand the specific role of fathers. The relationship between children’s gender, chronological age and parental stress is still unclear at present, whereas studies on ASD severity show a significant positive relationship with parental stress. Among the parent factors, there is still weak evidence supporting the relationship between parents’ level of education and parental stress, with no studies investigating parental emotion regulation or stress. Among the contextual factors, there is consensus among all the presented studies investigating the relationship between couple satisfaction and parental stress and between family functioning and parental stress in parents of children with ASD. Nevertheless, to our knowledge, the results on the relationship between parental stress and length of treatment are still unclear. In light of these considerations, further research is needed to deepen the connection between parental stress and all these factors taken together.
Our aim was to examine whether child (gender, age and ASD severity), parent (educational level and emotion regulation strategies) and contextual variables (family functioning, couple satisfaction and length of treatment) are related to parenting stress. Specifically, it may be useful to examine more closely the variables influencing parental stress for mothers and fathers separately. Our first hypothesis is to determine if mothers and fathers report different levels of parenting stress, and our second hypothesis is to examine the relationship of child, parent and contextual variables on maternal and paternal stress.
Method
Participants
Descriptive Statistics.
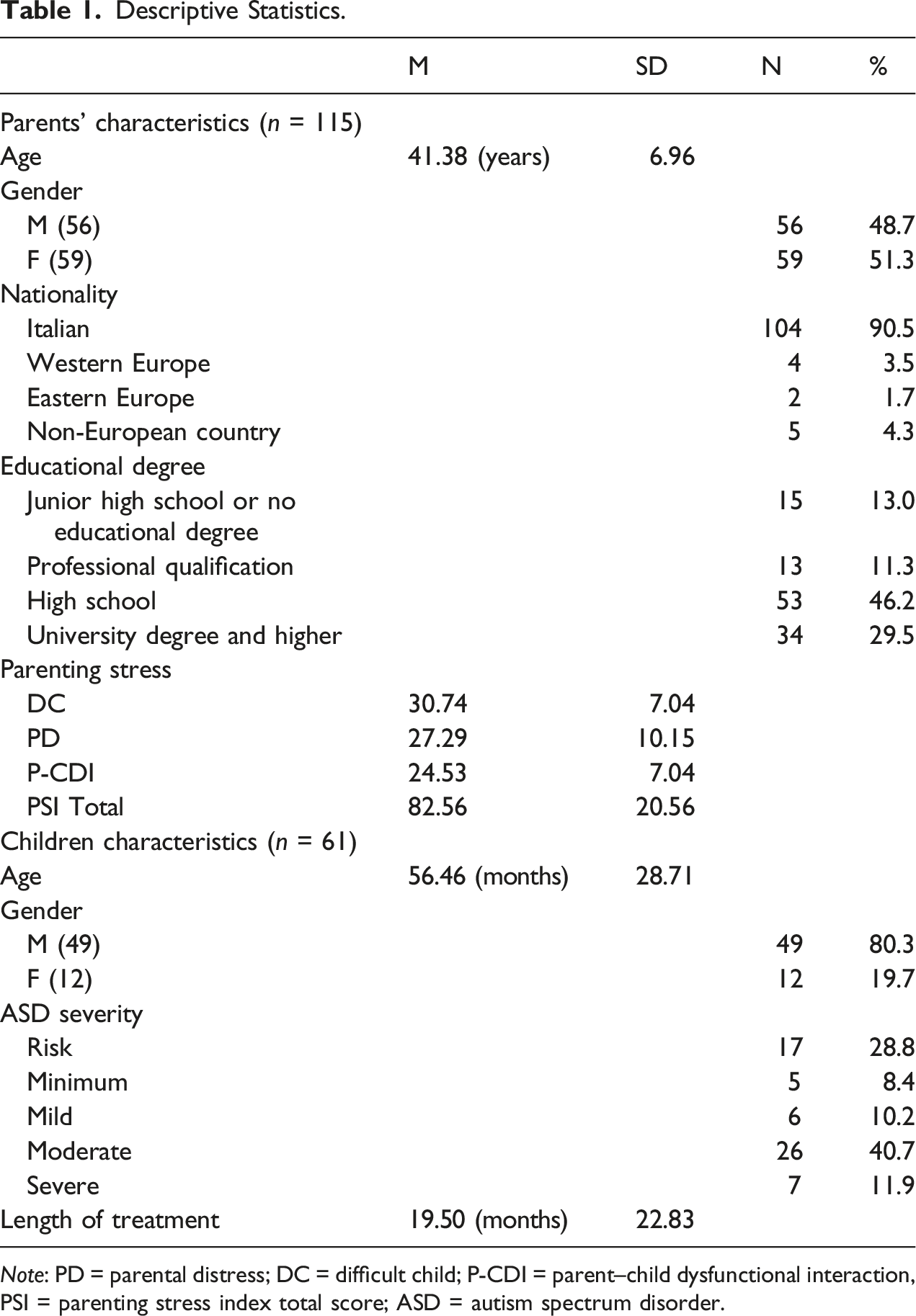
Note: PD = parental distress; DC = difficult child; P-CDI = parent–child dysfunctional interaction, PSI = parenting stress index total score; ASD = autism spectrum disorder.
Procedure
During their access to the Institute of Orthophonologi (IdO) of Rome, parents were asked to complete a set of questionnaires and an anagraphic sheet. On first access and every 2 years after the first evaluation, child diagnosis and ASD severity were evaluated according to the diagnostic criteria of the DSM-5 and the ADOS-2 scores as standard procedure. According to the ADOS-2 diagnosis, children were divided into five groups: those at risk of autism and those with minimum, mild, moderate or severe autism. All children and parents were included in an intervention programme that provided for specific interventions aimed at children and parents. The intervention programme, called the Turtle Project, was based on the DERBBI model: Developmental, Emotional regulation, Relationship and Body-Based Intervention for children with ASD (Di Renzo et al., 2020). The Turtle Project includes a first year of intervention centred on the affective–relational area, providing child therapy within small homogeneous groups, an animal-assisted intervention, counselling and therapy for parents and meetings with children’s teachers (working groups for students with disabilities). The second year of therapy focuses on the psychomotor/communicative–relational area, adding graphic–expressive activities and music therapy to the above interventions. In the third year, child therapy focuses on the psychomotor–cognitive–linguistic area. In the fourth year of therapy and beyond, the intervention is centred on the autonomy and cognitive–linguistic areas, including speech therapy. The parental intervention provides periodic counselling meetings with child therapists, dyadic parent–child therapy and group therapy (for mothers and fathers separately). The Turtle Project includes a total of 10 hours of therapy per week and requires an initial child global assessment, repeated every 2 years after starting treatment. Before the survey administration, parents were informed about this study’s aims and procedure and were asked to freely express their written informed consent to participate in this research project, in accordance with the Helsinki Declaration. This research project meets American Psychological Association ethical principles and guidelines. The study was approved by the Internal Review Board of the Institute of Orthophonology (IdO) of Rome.
Measures
The Parenting Stress Index – Short Form (PSI-SF: Abidin, 1995; Italian version: Guarino, Di Blasio, D’Alessio, Camisasca, & Serantoni, 2008) is a 36-item self-report measure on a five-point Likert scale ranging from 1 (completely disagree) to 5 (completely agree). The PSI-SF assesses parenting stress with three subscales: Difficult Child (DC: to what extent parents perceive their child to be easy or difficult to take care of), Parental Distress (PD: to what extent parents feel competent, restricted, conflicted, supported and/or depressed in their parental role), and Parent–Child Dysfunctional Interaction (P–CDI: to what extent parents feel satisfied with their child and their interactions with him/her), plus a control subscale, Defensive Responding (RD), that indicates whether the parent is presenting a minimizing or ‘look good’ bias to responses. The Italian adaptation of the PSI-SF (Guarino et al., 2008) shows good internal consistency, with Cronbach’s α values of 0.92, 0.84 and 0.88 for subscales PD, P–CDI and DC, respectively.
The Difficulties in Emotion Regulation Scale (DERS: Gratz & Roemer, 2004; Italian version: Giromini, Velotti, de Campora, Bonalume, & Cesare Zavattini, 2012) is a 36-item self-report measure on a five-point Likert scale ranging from 1 (almost never) to 5 (almost always). The DERS assesses the difficulties in regulation of negative emotions through five subscales: Awareness (awareness and understanding of emotions), Non-acceptance (non-acceptance of emotions), Goals (inability to start goal-oriented behaviours), Impulse (the inability to control impulses and behave in accordance with goals in the presence of negative affects), Strategies (inaccessibility toward emotion-regulation strategies that are perceived to be effective for feeling better) and Clarity (lack of emotional clarity). The Italian adaptation of the DERS (Giromini et al., 2012) on three independent Italian samples shows good internal consistency (Cronbach’s α ≥ 0.77 for the subscales and 0.92 for the total score).
The Dyadic Adjustment Scale (DAS: Spanier, 1976; Italian version: Gentili, Contreras, Cassaniti, & D’Arista, 2002) is a 32-item self-report tool requesting 30 answers on a six-point Likert scale ranging from ‘always agree’ to ‘always disagree’ and two dichotomous answers. The DAS assesses the quality of the couple relationship according to four subscales: Dyadic Consensus, which measures the agreement between partners regarding important issues, such as money, religion or time spent together; Dyadic Cohesion, which refers to interests and activities in common between the members of the couple; Dyadic Satisfaction, measuring the level of couple satisfaction and the desire to continue the relationship; and Affective Expression, measuring couple satisfaction regarding expression of affects and sexual life. The Italian version (Gentili et al., 2002) has good internal coherence, with Cronbach’s α = 0.87 for Dyadic Satisfaction, 0.89 for Dyadic Consensus, 0.78 for Dyadic Cohesion, 0.63 for Affective Expression and 0.93 for the total score.
The Family Adaptability and Cohesion Scale-IV (FACES-IV: Olson, 2011; Italian version: Visani, Di Nuovo, & Loriedo, 2014) is a 62-item self-report measure on a five-point Likert scale ranging from ‘strongly disagree’ to ‘strongly agree’ and assessing family functioning according to the Olson Circumplex Model (Olson & Gorall, 2006). The main hypothesis of this model is that balanced families are characterized by balanced levels of cohesion and flexibility, whereas unbalanced/problematic families are characterized by unbalanced levels of cohesion and flexibility. The Family Adaptability and Cohesion Scale-IV consists of six scales: Flexibility (how well the family adapts to change), Cohesion (the emotional bond that family members have toward one another), Chaotic (lack of or limited leadership, impulsive decisions and unclear roles), Enmeshed (large consensus within the family and little independence), Disengaged (great independence of the family members) and Rigid (roles and rules are strictly defined and imposed by the leader of the family, who is highly controlling). In addition to these subscales, FACES-IV offers a score on Family Communication, which measures the communication skills used by the family system, and Family Satisfaction, which investigates the level of satisfaction about family functioning among family members. A ratio score of balanced–unbalanced scales was created according to Olson and Gorall (2006), where higher scores of the ratio correspond to a more balanced family system. The Cohesion Ratio is calculated by dividing the Cohesion score by the average of the Disengaged and Enmeshed scores, the Flexibility Ratio is calculated by dividing the Flexibility score by the average of the Rigid and Chaotic scores and the Circumplex Total Ratio is calculated by dividing the average of the balanced scales (Cohesion and Flexibility) by the average of the unbalanced scales (Chaotic, Enmeshed, Rigid and Disengaged). The Italian version (Loriedo, Di Nuovo, & Visani, 2013) has shown satisfactory values of internal coherence, with Cronbach’s α values of 0.78 for Cohesion, 0.72 for Flexibility, 0.75 for Chaotic, 0.70 for Enmeshed, 0.73 for Rigid, 0.69 for Disengaged, 0.90 for Communication and 0.91 for Satisfaction.
The Autism Diagnostic Observation Schedule – Second Edition (ADOS-2: Lord, Luyster, Gotham, & Guthrie, 2012; Lord, Rutter et al., 2012; Italian version: Colombi, Tancredi, Persico, & Faggioli, 2013) is a semi-structured standardized assessment of communication, social interaction, play and restricted and repetitive behaviour for children from 12 months old, consisting of activities that elicit behaviours directly related to a diagnosis of ASD. It consists of a Toddler Module for children up to 30 months old with absent or limited language and also modules 1–4, providing cut-off scores for autism and autism spectrum classifications. The ADOS-2 has good psychometric properties (Lord, Luyster et al., 2012; Lord, Rutter et al., 2012) with high interrater and test–retest reliability, as well as high validity, confirming its usefulness in distinguishing individuals with ASD from other clinical groups (Mazefsky & Oswald, 2006).
Analytical Plan
Initial descriptive analyses examined means and distribution of the variables of interest in this study. Paired sample t-tests were performed to compare mothers’ and fathers’ parenting stress total score and subscales (DC, PD and P–CDI). Multivariate analysis of variance was conducted to verify group differences of categorical variables (gender of children, parent’s educational level and ASD severity) on parenting stress total score and subscales. Bivariate correlations using Pearson’s correlation were performed to examine the relation between parenting stress total score and subscales with children’s age, length of treatment, emotion regulation, couple satisfaction and family functioning variables. Cohen’s d was calculated as a measure of effect size r interpreted in line with Cohen (1988): r ≥ 0.10, small effect; r ≥ 30, medium effect; r ≥ 50, large effect; and d ≥ 0.20, small effect; d ≥ 0.50, medium effect; d ≥ 0.80, large effect. Partial eta-squared ηp2 was interpreted as follows: ≥ 0.01, small effect; ≥ 0.06, medium effect; ≥ 0.14, large effect. Finally, hierarchical multiple regressions were performed to test variables predicting parenting stress total score and subscales. Statistical analyses were performed using SPSS Version 24.0 for Windows.
Results
Descriptive statistics are reported in the Participants section above and shown in Table 1.
T-test for Paired Couples: Differences in Parental Stress for Parents’ Gender.
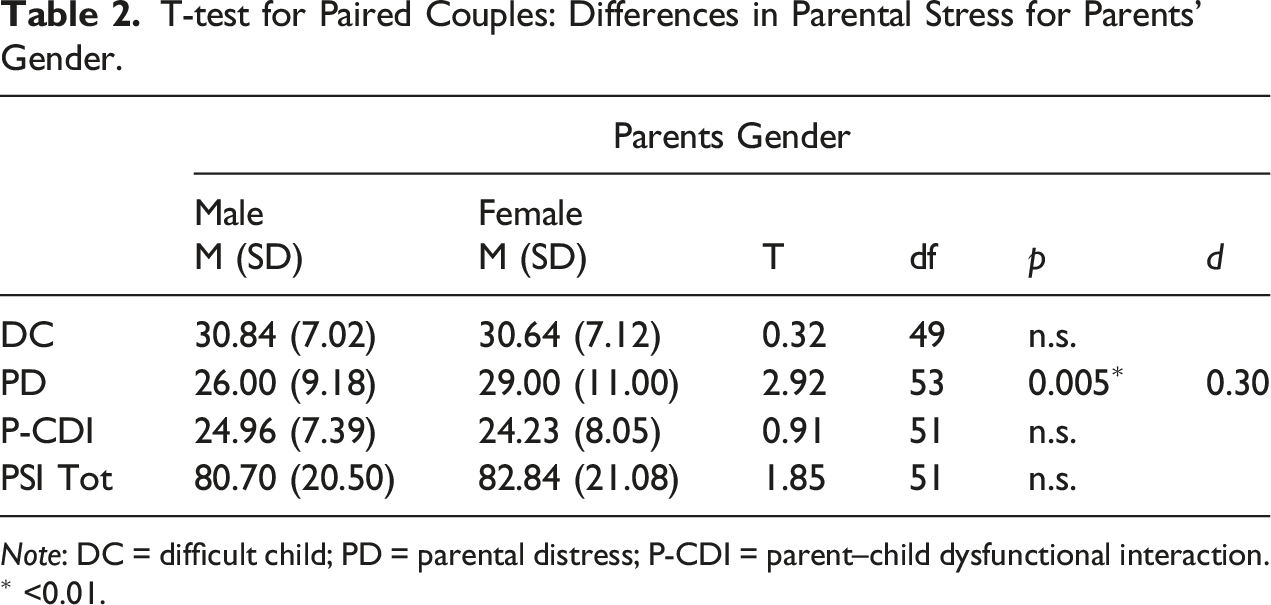
Note: DC = difficult child; PD = parental distress; P-CDI = parent–child dysfunctional interaction.
∗ <0.01.
MANOVAs: Differences in Parental Stress for Children Gender, ASD Severity and Parents’ Educational Level.
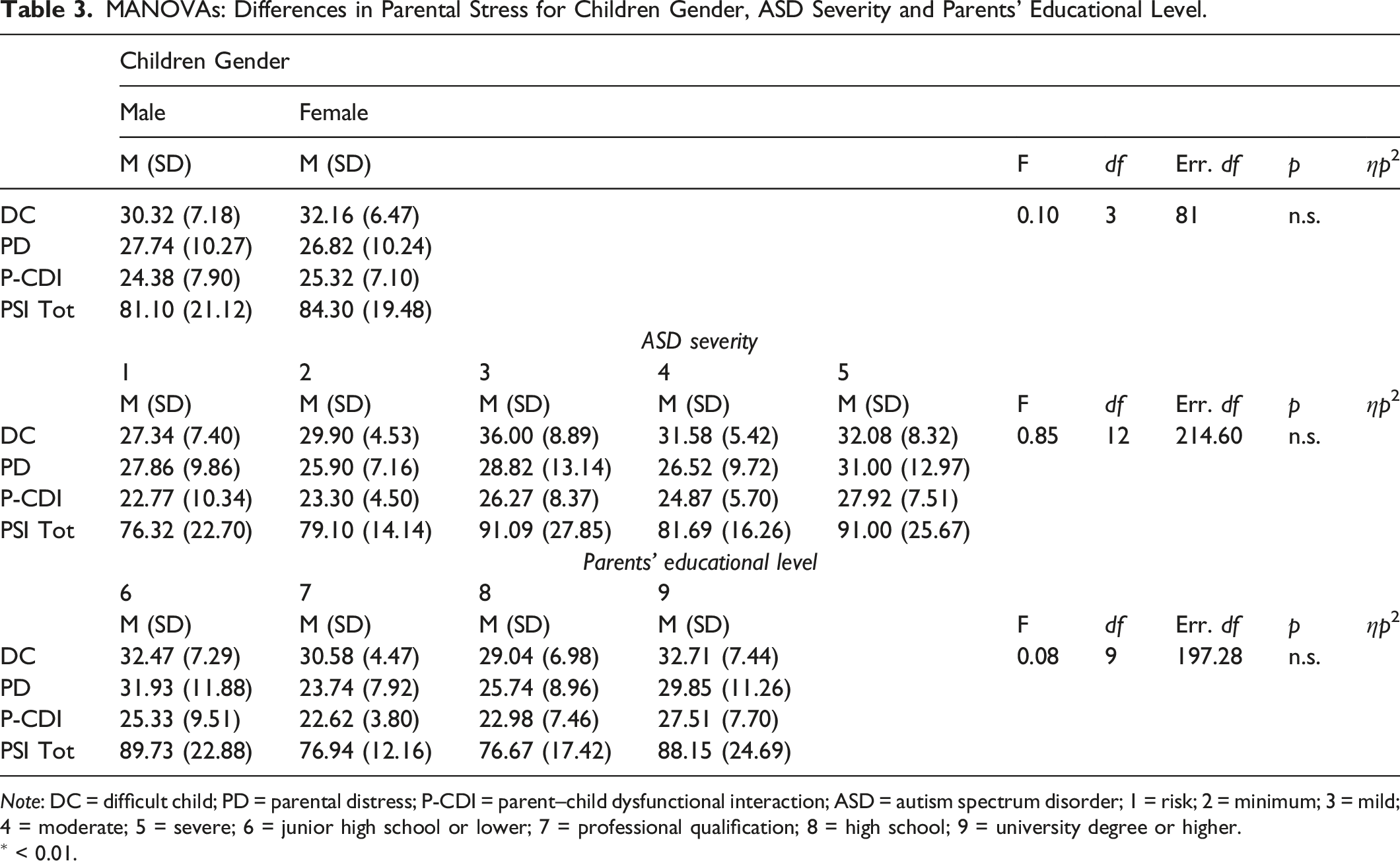
Note: DC = difficult child; PD = parental distress; P-CDI = parent–child dysfunctional interaction; ASD = autism spectrum disorder; 1 = risk; 2 = minimum; 3 = mild; 4 = moderate; 5 = severe; 6 = junior high school or lower; 7 = professional qualification; 8 = high school; 9 = university degree or higher.
∗ < 0.01.
Pearson’s Correlations Between Parenting Stress Subscales and Total with Children, Parents and Contextual Continuous Variables.
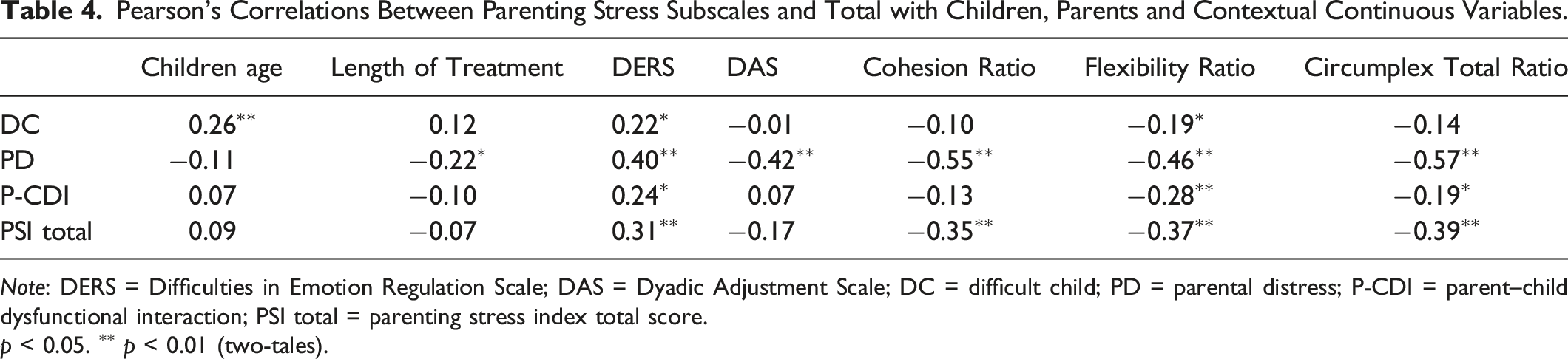
Note: DERS = Difficulties in Emotion Regulation Scale; DAS = Dyadic Adjustment Scale; DC = difficult child; PD = parental distress; P-CDI = parent–child dysfunctional interaction; PSI total = parenting stress index total score.
p < 0.05. ∗∗ p < 0.01 (two-tales).
Hierarchical Multiple Regressions Predicting Parenting Stress (Step 3) for Mothers.
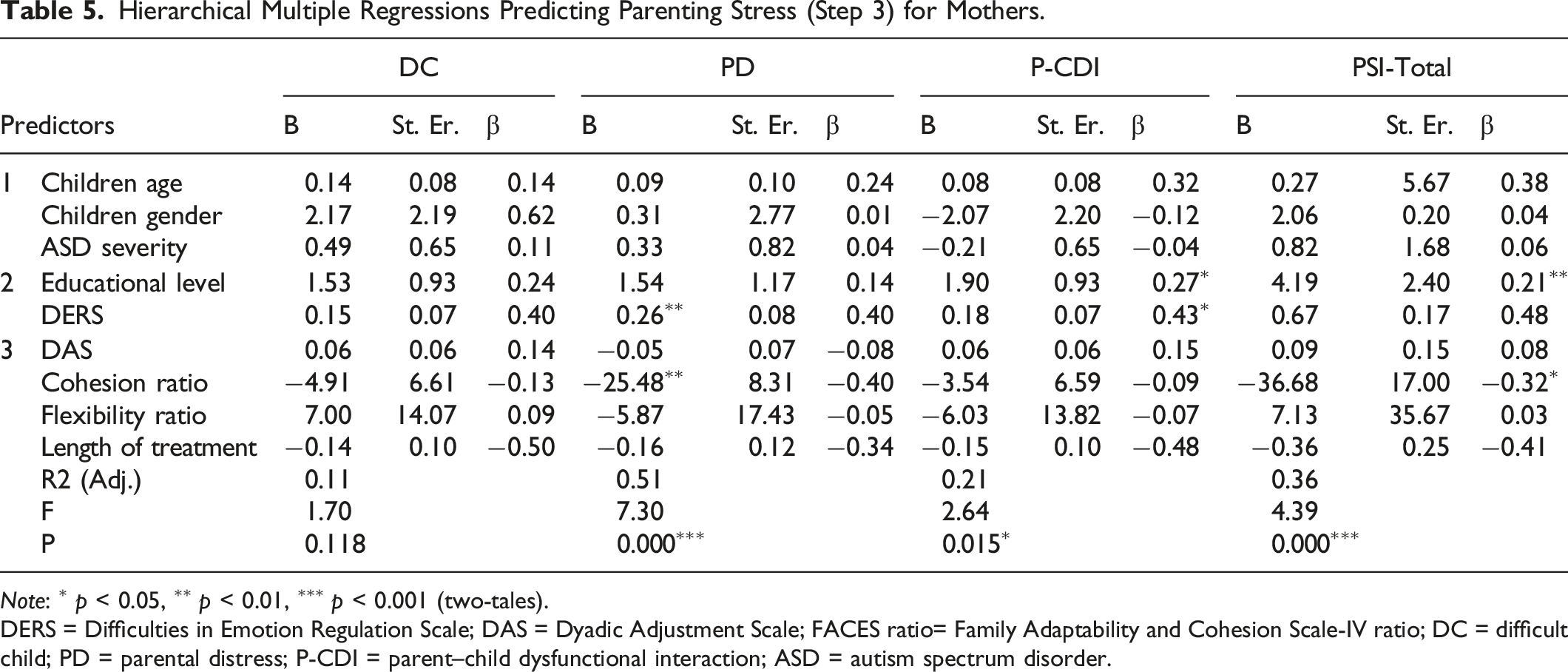
Note: ∗ p < 0.05, ∗∗ p < 0.01, ∗∗∗ p < 0.001 (two-tales).
DERS = Difficulties in Emotion Regulation Scale; DAS = Dyadic Adjustment Scale; FACES ratio= Family Adaptability and Cohesion Scale-IV ratio; DC = difficult child; PD = parental distress; P-CDI = parent–child dysfunctional interaction; ASD = autism spectrum disorder.
Hierarchical Multiple Regressions Predicting Parenting Stress (Step 3), for Fathers.
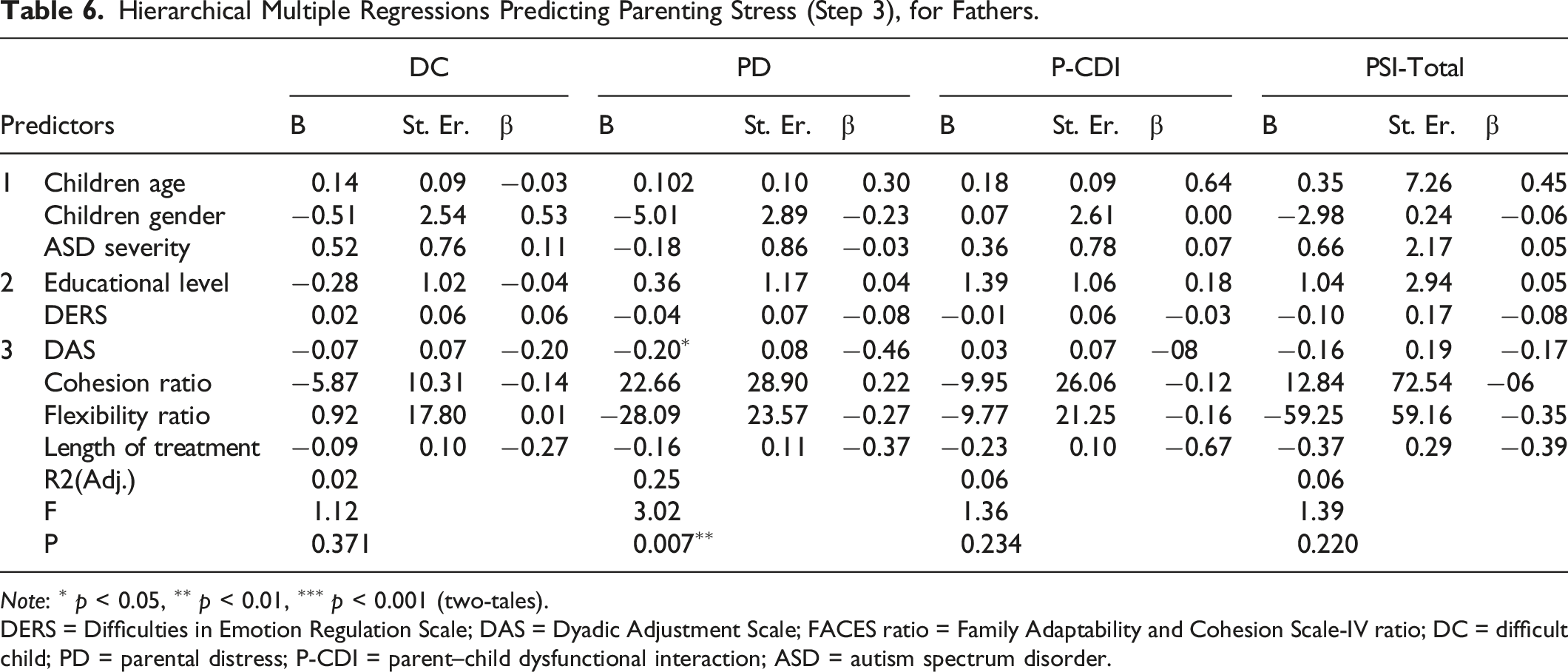
Note: ∗ p < 0.05, ∗∗ p < 0.01, ∗∗∗ p < 0.001 (two-tales).
DERS = Difficulties in Emotion Regulation Scale; DAS = Dyadic Adjustment Scale; FACES ratio = Family Adaptability and Cohesion Scale-IV ratio; DC = difficult child; PD = parental distress; P-CDI = parent–child dysfunctional interaction; ASD = autism spectrum disorder.
For mothers (Table 5), the hierarchical regression with DC as the dependent variable was not significant at Step 3 (F(9, 52) = 1.70, p = n.s.). For the hierarchical regression with PD as the dependent variable, Step 3 explained 51% of the variance for PD (R2 = 0.59, F(9, 54) = 7.30, p < 0.001). The individual predictors were examined further and indicated that parent’s emotion regulation and Cohesion Ratio were significant in predicting PD (β = 0.40, p < 0.01; β = −0.40, p < 0.01). The hierarchical regression with P–CDI as a dependent variable explained 21% of the variance at Step 3 (R2 = 0.35, F(9, 54) = 2.64, p < 0.05). The individual predictors were examined further and indicated that mothers’ educational level and emotion regulation were significant predictors in the model with P–CDI as the dependent variable (β = 0.27, p < 0.05; β = 0.43, p < 0.05). The hierarchical regression with PSI-SF total score as the dependent variable explained 36% of the variance at Step 3 (R2 = 0.47, F(9, 54) = 4.39, p < 0.001). Furthermore, parental emotion regulation and Cohesion Ratio were significant variables in predicting PSI-SF total score (β = 0.48, p < 0.01; β = −0.32, p < 0.05).
For fathers (Table 6), the hierarchical regression with DC as the dependent variable was not significant at Step 3 (F(9, 52) = 1.12, p = n.s.). For the hierarchical regression with PD as the dependent variable, Step 3 explained 25% of the variance for PD (R2 =.38, F(9, 54) = 3.02, p < 0.01), with couple adjustment as a significant variable in predicting PD (β = −.46, p < 0.05). The hierarchical regression with P–CDI as the dependent variable was not significant at Step 3 (F(9, 54) = 1.36, p = n.s.). The hierarchical regression with PSI-SF total score as dependent variable was not significant at Step 3 (F(9, 54) = 1.39, p = n.s.).
Discussion and Conclusions
Parental stress is an important risk factor for the parent–child relationship, and the parental ability to take care of the child, and mothers and fathers of children with ASD may be particularly vulnerable to experiencing very high levels of stress within this relationship. The literature (Ooi, Ong, Jacob, & Khan, 2016; Prata et al., 2018) on parents of children with ASD has studied the role of different variables in relation to parental stress, but much remains to be explored to understand which aspects, among the many suspected, have a main role in influencing parental stress.
Our first hypothesis examining the stress differences between mothers and fathers provides further evidence demonstrating similar stress experiences between the two parents except for PD. Indeed, our data showed that mothers could feel less competent and more restricted, conflicted and/or depressed compared to fathers when caring for their children with ASD. The hypothesis of gender differences in the perception of parental stress, therefore, was only partially confirmed. We assume that the choice of involving both parents in the Institute of Orthophonologi (IdO) of Rome process of evaluation and treatment (Di Renzo et al., 2019, 2020) could activate similar stress levels related to parent–child interactions and the perception of having a DC in both mothers and fathers and may also offer similar opportunities for elaborating this difficult situation and strengthening parental skills. However, this is not the case regarding stress related to the parental role, where the mothers seem to feel more stressed compared to fathers. It is most likely that, despite the many changes in our society concerning the father’s role, mothers are still the main caregivers in the household and, because of this responsibility, might experience more stress than fathers in their parental role.
Our second hypothesis was to examine more closely the variables influencing parental stress for mothers and fathers separately. For the mothers and fathers of our sample, the independent variables did not predict the parental stress related to having a DC. Further studies are needed to better understand which aspects may influence the extent to which parents perceive their child to be difficult to take care of, apart from those that we investigated. It could be useful, in this perspective, to use interviews and observational measures, such as the Insightfulness Assessment (Oppenheim & Koren-Karie, 2013) and the Dyadic Attunement Observation Schedule (DAOS; blinded for review process), for better understanding of the less conscious parental factors.
For both mothers and fathers, the stress related to PD was explained by our model, with parental ability to regulate negative emotions and the perception to have a balanced family cohesion significant in negatively influencing PD for mothers and the perception to have a better couple adjustment significant in negatively influencing PD for fathers. These data suggest that for fathers, raising a child with ASD would gain advantage from the beneficial role of having a satisfying relationship with their partner. This is in line with the literature revealing that a good quality of the couple relationship is associated with a better sense of parental competence for both parents, implying also a lower stress level in caring for the child (Brown et al., 2020; Florsheim et al., 2003; Guerriero et al., 2017; Hartley et al., 2016; Sim et al., 2016, 2017, 2018; Weitlauf et al., 2014). Our data, however, corroborate this relationship specifically for fathers, whereas for mothers, other factors seem to be more prominent, such as the regulation of emotions and the perception of having a balanced family preferring cohesion rather than enmeshed or disengaged functioning.
The stress related to the perception of having a difficult interaction with the child was explained by our model for mothers but not for fathers. For mothers, the extent to which they feel unsatisfied with their child and their interactions with him/her was influenced by their inability to regulate their negative emotions and by their educational level. This is in contrast with studies suggesting that lower levels of stress do not depend on a higher parental educational level (Nikmat et al., 2008; Valicenti-McDermott et al., 2015). Despite this, in a previous article (blinded for review process), we suggested that a higher level of education could function as a protective factor in understanding the child’s internal world and accepting the child diagnosis in cases of ASD. We can speculate that more insightful and accepting parents also may be less stressed during their child care and interactions. We could add that maternal ability to regulate negative emotion may serve as an additional protective factor for mothers, suggesting the need for more in-depth study of the relationship between these factors in future research projects.
Finally, for mothers but not fathers, our model was significant in explaining total parental stress, with parental emotion regulation and family-balanced cohesion as significant variables predicting total parental stress. This result is particularly interesting and emphasizes that when we consider a model in which child, parent and contextual factors are taken into consideration, the parental abilities to regulate negative emotions assume prominent importance together with the parental perception to have a family where the emotional bond between family members is stronger than having little or too much independence between family members. This means that parents experiencing higher levels of parenting stress also reported higher levels of unbalanced (problematic) aspects of family functioning than balanced (healthy) aspects of family functioning. These results are in line with studies showing an increased risk of stress for parents reporting lower levels of family functioning (Johnson & Simpson 2013; McStay et al., 2014; Pisula & Porębowicz-Dörsmann, 2017; Zaidman-Zait et al., 2017).
In particular, parents’ intervention programmes for families of children with ASD should focus on supporting maternal emotion-regulation strategies, and balanced family functioning and the paternal perception of the quality of their romantic relationship. It should be useful to think of specific interventions for mothers and fathers separately for supporting the specific protective factors emphasized in this study and to support the family system, as also supported by studies that have demonstrated the importance of offering intervention programmes for families of children with ASD (Factor et al., 2019).
Limitations
The present study has several limitations. Firstly, the study was cross-sectional, and therefore the direction of associations among the variables investigated could not be established definitively. The direction of these associations may be addressed in longitudinal designs. Secondly, the variables investigated were measured with questionnaires; thus, future research should include interviews and/or video recording of parent–child interactions to provide more complex and detailed data while also controlling for parental perceptions. Thirdly, there was variability of the participants in this study, such as age of the children and duration of treatment, that could be included in future studies. Fourthly, the sample size is relatively small, and we do not have a control group to check for exogenous factors affecting the reports of parental stress. Because of the small size of the sample, we could not investigate the relationship between the individual subscales of the measures used and parenting stress. Future studies should look deeper into these relationships and expand the analysis to other variables that seem to influence parental stress, such as children’s emotional–behavioural symptoms and parental perception of social support.
Footnotes
Acknowledgements
We thank all the parents and children who participated in this.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.