
Abstract
Research has taken important steps towards establishing values work in organizations as a performative phenomenon situated in practice. Yet, researchers have said little about the critical and creative nature of such work, including how it may build its agentic powers more so from what is ethically absent than from what is established. We approach this void by drawing from Dewey’s Pragmatism in a comparative analysis of how three value-laden issues tied to companionate love are handled in a faith-based hospital. We develop the notion of value inquiry, which we understand as a discovery-oriented and transformative constructing of the good that takes its originating creative desires from troublesome situations. Our findings suggest that ethically fruitful value inquiry involves opening such situations in a way that critically examines previous practice, enlists people in co-defining needs and engages them in sustained experimental action. By theorizing value inquiry, we relocate ethical agency as a responsive relational capacity emerging with coactive power in evolving situations. Such emergence highlights the relational processes of work on values in organizations. When inquiring together, people move beyond attending to the use of prescriptive value conceptions and into a creative mode of actively searching for and co-constructing the good.
There is, by implication, if not explicitly, a prevalent notion that values are already well known and all that which is lacking is the will to cultivate them in the order of their worth. In fact, the most profound lack is not the will to act upon goods already known but the will to know what they are.
In this situation [handling aggressive patients at an acute psychiatric clinic], we have found it useful to ask ourselves the following question: If this person in front of you was someone you loved very dearly, what do you think the next two minutes should be about, as seen by them?
In his essay ‘The Construction of the Good’, John Dewey (1929) took issue with the threat that quests for the human good may become quests for certainty and end up in dogmatic truth. Values need to ‘lose all pretence of finality – the ulterior source of dogmatism’ (Dewey, 1929, p. 264). Dewey’s (1929, 1939) quest to search for the good in a situated inquiry is a key tenet of Pragmatism, one that directs valuation and inquiry towards ends-in-view and a progressively improved imagining of human betterment (Alexander, 2013; Evans, 2000). The good is never given and can only be arrived at by continued inquiry into the factual matters of challenging situations, not through ‘ideals, ends, and obligations independent of concrete actualities’ (Dewey, 1922, p. 333).
In this study, we reconnect with the more radical intent of Dewey’s quest by conceptualizing and exploring constructing of the good as organizational value inquiry, understood as a discovery-oriented process originating from desires for transformation in troublesome situations where values are at stake. Research on ‘values work’ (Gehman, Trevino, & Garud, 2013) has taken important steps in furthering process theory for studying ethics in organizations. Examples include studies of maintaining professional values (Wright, Irving, & Selvan Thevatas, 2021; Wright, Zammuto, & Liesch, 2017), transmitting values through generations (Suddaby, Ng, Vershinina, Markman, & Cadbury, 2023), or mobilizing values for corporate entrepreneurship (Raitis, Sasaki, & Kotlar, 2021), social entrepreneurship (Chatterjee, Cornelissen, & Wincent, 2021) and social change (Daskalaki, Fotaki, & Sotiropoulou, 2019; Vaccaro & Palazzo, 2015). By emphasizing values work (Gehman et al., 2013) or valuation (Kornberger, 2017; Muniesa, 2011) rather than values, one avoids granting social structures (such as values and ideals) ontological existence apart from their constitutive acts and locates values in the concreteness of performed practices and their changing concerns (Gehman, 2021; Selznick, 2008).
These theoretical positions align well with Pragmatist maxims of avoiding dualisms and placing studies of social action at the centre of understanding organizations (Simpson & den Hond, 2022). Still, researchers have yet to unpack the critical and creative nature of values work. Dewey’s tying of valuation to inquiry is missing from research on values work and downplayed in the sociology of valuation. What is lacking is an account of the primacy of the troublesome situation as the driver of values work in terms of being the originating source of interest and desire – and hence the need for inquiry. Value inquiry is important because it provides the basis for understanding and developing organizational ethics as an emergent, responsive and collaborative phenomenon.
A key argument of Dewey’s Theory of Valuation (Dewey, 1939) is that ‘the value of values can only be appraised’ when ‘there is something lacking, wanting, in the existing situation as it stands’ (Dewey, 1939, p. 33), and when this absence triggers propositions regarding what to do. In short, values and valuation are primarily located through inquiry and from desires for transformation. It is an ethics of being receptive and actively constructing the new rather than preserving and using the established. And, as we will show, the ethical agency arising from inquiry into the indeterminate situation is sustained by the growth of collaborative forms of power, so-called coactive power (Follett, 1924 [1951], 1940). Such power contrasts with coercive power flowing from the maintenance and use of authoritatively sanctioned beliefs.
We develop the notion of value inquiry through a comparative study of the handling of three sets of value-related issues sampled from a larger longitudinal research project of a faith-based hospital. This organization was founded on deeply held commitments to provide skilled medical care and altruistic compassion to marginalized people. Throughout its 150-year history, people within the organization have embraced and debated ideals of companionate love amid shifting regulatory demands and new challenges regarding how to respond to patient needs in care situations. 1
The second quote at the beginning of this paper, by Tord, is from one such situation. Medical personnel at an acute psychiatric clinic in the hospital need to assess how to handle aggressive and potentially dangerous patients, with belt restraining being a controversial and often-used option. Accounts of how this situation was transformed became decisive to our interpretation. The process had a surprisingly strong positive effect within the organization, with an 85% reduction in belt restraining, and it brought forth much subsequent attention at the national level. This led us first to an empirical puzzle: How do we explain the radical transformation of a values-related practice, one which had been stuck for decades, in an organization where people are so articulate about their values? We noticed that beyond enacting agreed-upon ideals of companionate love, stemming from the hospital’s history, people were engaging in inquiry.
Yet, the dynamic of inquiry as a values-laden process was curiously absent from both the local language and current research on values work. The empirical puzzle thus transformed into a theoretical one. Drawing from the combined inspiration of Dewey and our empirical material, we ask: What makes value inquiry fruitful, both in terms of constructing the good in troublesome situations and the potential enrichment of organizational capacities for constructing the good?
The duality of this question reflects a recognition that, while we insist on the uniqueness of human needs in troublesome situations as the originating source of ethics, we also recognize that such an ethics needs a form of organization beyond a specific localizable phenomenon (Krüger & Reinhart, 2017) or a series of interactions with unique others (Rhodes, 2023). Value inquiry does not rule out centralized and coordinated responses across situations (Kraatz, Flores, & Chandler, 2020). To explore the formation of the organizational capacities for constructing the good, we thus attend to how inquiry may foster the emergence of agency and intelligent habits of a collective nature.
Theorizing Value Inquiry
To orient our empirical analysis, we develop an analytical framework for the dimensions of value inquiry that might make it ethically fruitful. We start by placing value inquiry in the larger body of research on values work, valuation and Deweyan Pragmatism. Our agenda is not to claim that all valuation or forms of values work must involve inquiry, which indeed can be drawn from a strong interpretation of Dewey. Rather, we want to explore how organizational research occupied with valuation and values work can be enriched by a language of creative discovery and desires for transformation. Such a language is key to understanding ethics as responsive and emergent from dealing with people’s needs in precarious situations, thus marking a creative and critical force rather than a compliant one.
From prescriptive ethics to troublesome situations and discovery
With values, researchers typically discuss emotionally laden ‘conceptions of the desirable’ (Hitlin, 2003, p. 123) that are ‘worth having, doing and being’ (Selznick, 1992, p. 60) and that seem relatively enduring and trans-situational (Bednarek-Gilland, 2016; Kraatz et al., 2020). The last decade of research has brought nuance to such positions, particularly in exploring values as verbs rather than nouns (Kraatz et al., 2020) and values work as distributed, interactive and ongoing processes (Espedal & Carlsen, 2021; Gehman et al., 2013). Turning away from the dominance of cognitive and cultural perspectives allows for a focus on practice as the site where values are constituted and performed on an ongoing basis (Gehman, 2021; Gehman et al., 2013). This focus parallels a broader turn to embedded ethics (Cunliffe & Ivaldi, 2021) and situated ethics (Banks, 2021) in organization studies, including the performative emphasis in the sociology of valuation taken more broadly (Kornberger, Justesen, Madsen, & Mouritsen, 2015; Muniesa, 2011; Stark, 2009).
The latter research stream has engaged significantly with Dewey’s work on valuation, though few scholars in this tradition have taken inspiration from the radical intent of Dewey’s work in terms of tying valuation to inquiry; – for exceptions, see Stark (2009) and Krüger and Reinhart (2017). In the literature on values work, such perspectives are lacking. This is amiss because disregarding inquiry means foregoing both the primary desires of values-related work and what makes it powerful. To see this, let us start by unpacking a key passage towards the end of Theory of Valuation (Dewey, 1939, pp. 54–55): Until there is actual or threatened shock and disturbance of a situation (. . .) [t]here is no need, no desire, and no valuation, just as where there is no doubt, there is no cause of inquiry. Just as the problem which evokes inquiry is related to an empirical situation in which the problem presents itself, so desire and the projection of ends as consequences to be reached are relative to a concrete situation and to its need for transformation.
Two sets of extensions of research on values work follow. First, value inquiry recognizes the troublesome situation as the originating force of ethical desire. Dewey explicitly and repeatedly rejected the notion that values as such should be original in the sense of being taken as finalized or starting points for valuation (Dewey, 1939, pp. 16, 19–21, 25, 54–55). This stance reflects Dewey’s (1929) critique of dogmatic certainties in religion and science as well as the separation of theory from practice – certainties that Dewey thought disabled the active coping with problematic conditions and constructing the good (Evans, 2000).
In contrast, while empirical studies on values work typically refer to a duality of values as abstract conceptions of the ideal and as something being performed in practice (Chatterjee et al., 2021; Daskalaki et al., 2019; Vaccaro & Palazzo, 2015; Wright et al., 2021), there is a clear tendency to start from the former. One example is a study of how nurses in an emergency department maintain and translate professional values that ‘exist at a macro-level’ in frontline work (Wright et al., 2017, p. 201), i.e. prior to and outside of practice. Another example is a study of how a new leader of a family firm used values to sustain entrepreneurship: ‘he [the leader] also introduced and insisted on the new business values (. . .) and [by] practicing these values he “walked the talk”’ (Raitis et al., 2021, p. 115). In this study, the values mentioned are merely labelled and taken for granted, never examined. A third example is from a study of values work as intergenerational transmission of values in a family firm (Suddaby et al., 2023). Here, the authors refer to values as ‘roadmaps’ for action and ‘cognitive blueprints’ that amount to forms of social control when internalized in taken-for-granted practices (Suddaby et al., 2023, p. 300).
These are ways of talking about values that somehow underline or imply their existence prior to practising and where performativity is cast in the language of top-down processes of maintaining, translating, using, spreading, or internalizing values. Values work risks becoming another set of terms for understanding how people attach broad labels of moral worth to their actions or maintain and apply preconceived, stable ethical principles set by others. Taking values as primary suggests a language of prescriptive ethics (Banks, 2021), as opposed to one originating from receptivity to specific others (Rhodes, 2023), and being alert to actors’ needs for transformation in particular situations. To paraphrase the opening quote from Dewey, these are ways of cultivating known goods rather than asking what the goods are.
Our second extension follows from the first. Value inquiry has a strong discovery orientation and highlights valuation as a form of social engineering of organizational activities (Lorino, 2018). To Dewey, the desire for valuation arises from inquiry into specific means–ends relationships. There are no desired ends ‘having value apart from valuation of the means by which they are reached’ (Dewey, 1939, p. 36), no values as ‘ends-in-themselves’. Ends realized become stepping stones to further discovery since the situation is then changed and more judgement is needed on whether something is good and how good it is (Krüger & Reinhart, 2017). From this perspective, a value such as companionate love achieves its meaning not as a set of fixed objective standards that are independent of situations. Rather, it emerges from people’s reflections on specific courses of action in specific troublesome situations and their interactional contexts.
In Dewey’s Pragmatism, valuation is not merely about realizing something predetermined and goes beyond problem-solving with final targets. Inquiry involves a creative search where people examine ambiguous situations and generate new possibilities through a probe-and-learn process (Ansell, 2012). Troublesome situations become resources for learning when they trigger search for the good ‘less as a process of finding what we already know to be valuable, than as distributed practices for recognizing opportunities’ (Stark, 2009, p. 9).
Dimensions of value inquiry
How can value inquiry be valuable in an ethical sense? In what follows, we refer to value inquiry as a continuously unfolding social process that relies on experimental methods (Evans, 2000) and may involve several loosely connected episodes of discovery (Golden-Biddle, 2020). We chart four dimensions of value inquiry that we subsequently discuss in our empirical analysis, drawing from key features of Dewey’s philosophy of social inquiry and, more selectively, the work of Mary Parker Follett. In many ways, Follett’s (1924 [1951], 1940) Pragmatism parallels Dewey’s approach to inquiry, but it has significant complementary conceptions, particularly regarding how people are brought into creative collaboration across differences of seeing, and the corresponding potential for the emergence of coactive power. These are relational processes that Dewey says very little about and that emerged as particularly salient from our empirical analysis.
The situation and how it is taken
In Deweyan thinking, valuation and inquiry start from the particulars of troublesome situations where prevailing habits have failed and from which creative action may emerge (Joas, 1996, p. 129). To inquire about something is to question a situation so that it is ‘taken, adjudged, to be problematic’ (Dewey, 1938 [1991], p. 111), including the further examination of the situation regarding the conditions that constitute lack and need, or potentialities. To Dewey, this was more a case of examining the inherent objective qualities of situations rather than constructing something that is not there. Inquiry must locate the uniqueness of doubt concerning what is ‘uncertain, unsettled, disturbed’ (Dewey, 1938 [1991], p. 109).
Follett, quite similar to Deweyan inquiry, started with the situation and repeatedly referred to the need to follow the ‘law of the situation’ and discover its integral order (Follett, 1924 [1951], p. 152; 1940, pp. 58–64, 106) so that facts are understood and the differences between people’s perspectives and desires are recognized and responded to.
Dynamics of situated learning
Dewey’s (1939, p. 30) valuation is essentially a dynamic of situated learning from experience through experimental testing, validation, and reflection – in itself a search that also involves understanding more of the situation, its nature and its opportunities. In Dewey’s (1938 [1991], pp. 112–121) patterns of inquiry, this is charted as a logic involving repeated acts of observation, reasoning, ideation and testing propositions in experimental action. Again, Follett parallels this line of thought when embracing systematic experiments as the precondition for ‘discovering possibilities now open to us’ (Follett, 1924 [1951], p. xii). Whereas Dewey saw situated learning as a circular shuttling between reflection and action, Follett (1924 [1951], pp. 53–77; 1940, pp. 44–59) emphasized the circular process of interactions between stakeholders’ initiatives and responses. For both, the result of such behaviour was a series of progressive integrations that were the basis for the next step of activity, with each step also altering the situation.
Dynamics of situated power
When striving to behave ethically, people act to meet the concerns of others, imagine and rehearse the responses of others, and are held responsible by others for the consequences of their actions (Dewey, 1922, pp. 814–816). Consequently, it cannot be taken for granted that all value inquiry is power-neutral or ethical in either intention or effect. In Follett’s (1924 [1951], 1940) language, the trickle-down ethics of implementing finalized values or the closing down of ethical deliberation through forms of domination represent the use of coercive power, that is, power over. In contrast, according to Follett (1924 [1951], 1940) real power is a relational and situated capacity, a power with. This coactive power results from facilitating interactive influence between levels and boundaries within the organization (Follett, 1940, p. 105). It is an ethics of attending to the situation and recognizing differences as the basis for resources produced in interactions.
Dewey’s work on social inquiry is less articulate about power relations per se. An implicit power perspective is fully aligned with Follett’s work in the sense that power potentially emerges from the field of inquiry as ‘a capacity to execute desired ends (. . .) not as a possession of agents but as a dynamic, fluid and relational field of forces’ (Hildreth, 2009, pp. 786, 790).
Outcomes of inquiry
Both Dewey and Follett emphasized the outcome of inquiry as twofold: one, the satisfaction of realizing desired ends, and two, the recognition of changed situations and new differences that foster continued inquiry. In Dewey’s terms, people need to rectify the situation as a settled and unified whole (Dewey, 1938 [1991], pp. 108–109) where a satisfying and valued end is reached, which in turn can be the means to other ends (Dewey, 1939, p. 49). In Follett’s writing, the fusion of viewpoints within and between groups is an active and emergent process of unifying, not a final achievement (Ansell, 2009, p. 476). Each new iteration of progressive integrations can spur opportunities and keep alive the ethical search.
Finally, this twofold outcome of satisfied and continued inquiry involves potential carryover to new situations, such as an enduring capacity for action resulting from how the situation’s alteration has strengthened the relations of the people involved in it (Follett, 1940, p. 49). Dewey (1939, p. 46) also opened for the development of general and abstract conceptions of values as desirable ends, using an example of a physician who might form such understanding based on repeated examination of patients who have variations of similar issues. This can then result in the seeding of intelligent habits (as opposed to non-reflective habits) through repeated bouts of empirical inquiry – broader dispositions for action that may be flexibly evoked to deal with new situations (Cohen, 2007; Dewey, 1922, pp. 40–44).
In summary, the fruitfulness of value inquiry may thus be examined from how it acts simultaneously on the situation and its conditions, the generation of new intelligent habits (Lorino, 2018, p. 102), and the continued broadening of inquiry into similar and related situations.
Research Setting and Method
This paper emerged from a larger study on values work and values-based leadership in a privately owned non-profit and faith-based hospital. The case organization has 150 years of persistent attention to values-related concerns and is a setting offering a compelling context for our research question. The hospital typifies a religious (Lutheran) non-governmental organization operating on a non-profit and independent basis to serve the common good. As of 2020, the hospital operated with a staff of approximately 1,600 persons, 230 beds, and an extensive outpatient facility that treats 180,000 patients annually. The hospital is fully financed by and operates within the framework of regional health authorities. Functioning as both a national and a local hospital, it serves approximately 200,000 city residents. The hospital has a large psychiatric and surgical department, receiving patients for scheduled operations from all parts of the country, and is one of the largest privately owned faith-based organizations in Scandinavia.
The hospital was founded on religious traditions in 1868 by a trained nurse who was widely credited with establishing nursing as a nationwide field of professional practice. As ‘the first deaconess’, she acted as the head of an educational institution associated with the hospital for more than 50 years. She left a heritage of fostering nursing practices that offered altruistic care and compassion for populations often marginalized, including those experiencing poverty, alcoholism, homelessness and prostitution. The hospital has kept its focus on the marginalized and its services have been extended to undocumented immigrants and people facing serious mental health challenges.
At the start of the millennium, a long series of health care reforms led to demands for a more business-like health care system through cost-effective treatment programmes, increased specialization, competition from lowest-cost providers, and new ownership structures. The hospital responded by emphasizing specialized health care services. The management of the hospital considers having a leading domestic position in several forms of advanced surgery key to the revenue stream. All strategy documents since 2002 have emphasized the quality of services as a superordinate value along with companionate love.
Overall approach and data collection
The research project is informed by a strong process orientation (Langley & Tsoukas, 2010) and forms of narrative inquiry (Kohler Riessman, 2008). The bulk of the research period lasted over five years from August 2013 to November 2018. We did a set of follow-up interviews and additional collection of archival data concerning the three focal issues until November 2022. The first author was positioned as an insider at the case organization for four years (2008–2012), employed as a professional educator and minister of students in the foundation that owns the hospital. Our data collection combined semi-structured and open-ended interviews with observations (both participant and non-participant) and extensive archival sources (see Table 1).
Overview of data in relation to issues.*
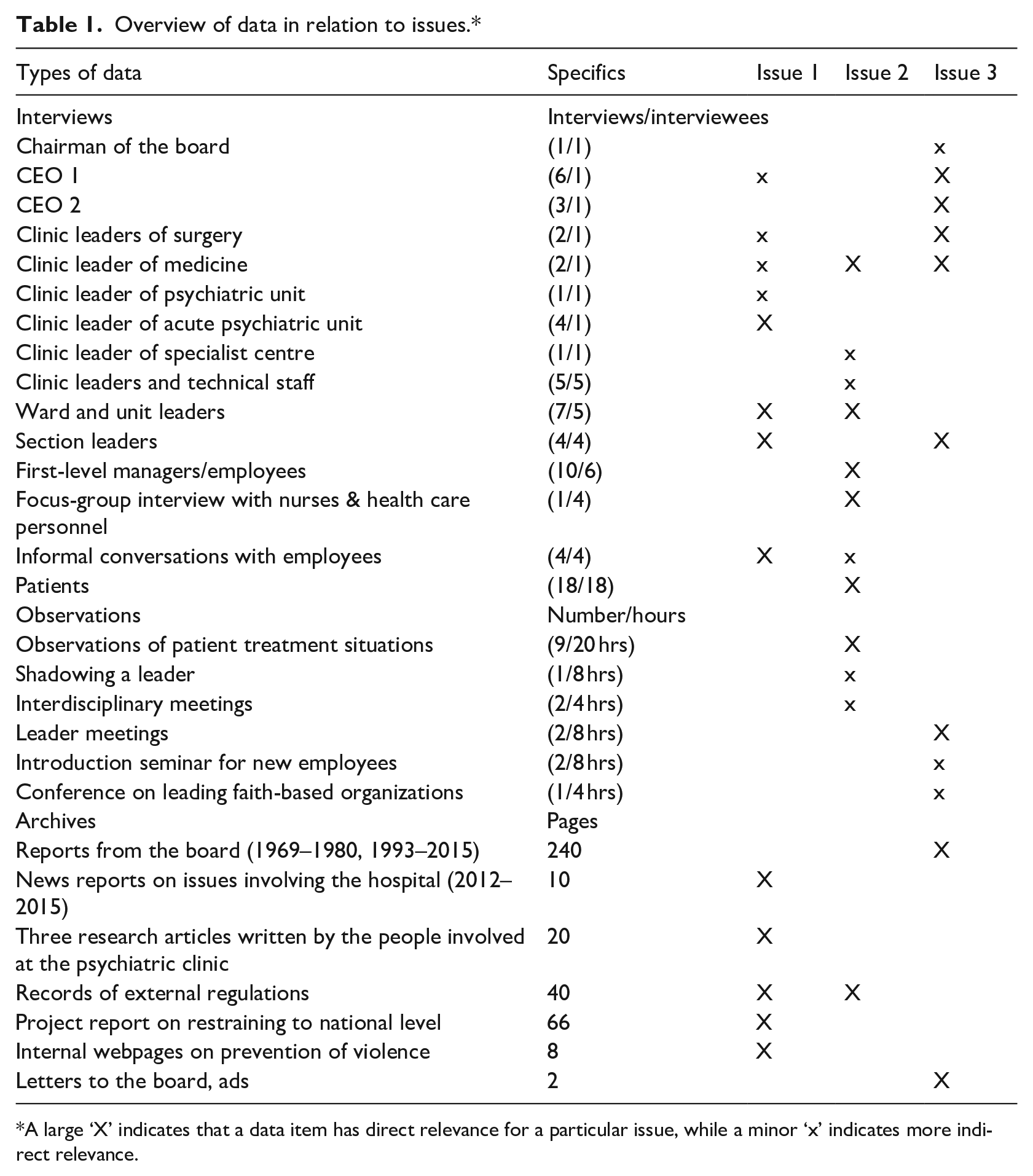
A large ‘X’ indicates that a data item has direct relevance for a particular issue, while a minor ‘x’ indicates more indirect relevance.
Interviews
We conducted 69 interviews with 54 persons, of whom 36 were organization members and outside stakeholders while 18 were patients. The selection of interviewees was based on a stratified purposive within-case sampling, heeding the criteria of relevance and variation (Patton, 2002, p. 240). We targeted persons with assumed proximity to value-related issues from different levels (top-level managers, mid- and first-level managers, and employees) that represented a broad variation in professional backgrounds (physicians, psychiatrists, nurses, dentists and administrative personnel). Repeat interviews were motivated by a need to follow up and deepen our understanding of emergent values-laden issues, such as a contested leadership change and the handling of regulatory challenges. The first author interviewed 18 patients from different wards within the internal medicine department, a unit chosen because of its proximity to patients and the low complexity of treatment situations. Most of the interviews lasted approximately one hour. Interviews with patients were often shorter depending on their condition. 2 All but eight interviews were taped and transcribed verbatim (four had technical issues and another four were more informal interviews made on the spot, from which we took notes).
Observations
To complement and capitalize on data acquired during interviews, the first author proceeded to collect ethnographic data. This included patient observations of treatment situations (9) and interdisciplinary meetings (2), shadowing a middle management leader (1), using participant observation as well as observations from top leader meetings (2), and a seminar for new employees (1). Notes were made during the observation events, with a structured reflection guide to enrich the field notes. 3
Archives
Table 1 specifies archival data pertaining to the three issues in focus. The larger study included additional archival data of roughly 2,800 pages that shaped our contextual understanding of the organization and its institutional history. These included annual reports, strategy plans, anniversary books, biographies, internal employee surveys, a national patient survey and media entries, as well as letters from patients and the founder.
Data analysis
Our data analysis for this paper combined an inductive and comparative approach from grounded theory (Charmaz, 2006) with narrative analysis (Kohler Riessman, 2008) while working iteratively and abductively to link tentative categories to empirical material and new theoretical frameworks (Locke, Feldman, & Golden-Biddle, 2022). The overall interpretive journey had three distinct steps.
The first author started with an open round of coding across all data while heeding the voices of the informants. These early coding themes charted accounts of values work in response to emergent concerns. During the sharing and discussion of this material, we noticed that interviewees and observations were calling attention to situations that highlighted controversies and questions such as ‘How are we living our value foundation given these new challenges?’ or ‘What does companionate love mean in this type of patient situation?’
In the second step of interpretation, we returned to examine the data and identified 27 ongoing issues of this form of value questioning that were mentioned by two or more persons. One such issue gained salience in our interpretation during a three-hour feedback session in January 2017 with seven of the leaders in the organization. This issue, now labelled issue 1, seemed to tell of an intriguing mix of patient perspective taking, a questioning of previous practice and systematic inquiry. From the 27 processes identified, we next sampled two other issues that could provide analytical contrasts (Patton, 2002) in terms of having a similar intensity of value questioning but showing variation in situations and handling (issue 2 and issue 3). We subsequently went back to the field for follow-up interviews on all three chosen issues. 4
In the third and final step of interpretation, we followed a narrative approach to theorize from the three chosen issues. Briefly, we mapped triggering events across a timeline in the institutional field (see Figure 1) and identified preliminary themes of how the issues were handled as a form of social inquiry. During this stage, we also revisited the work of Dewey and Follett in more depth and subsequently refined our interpretation.
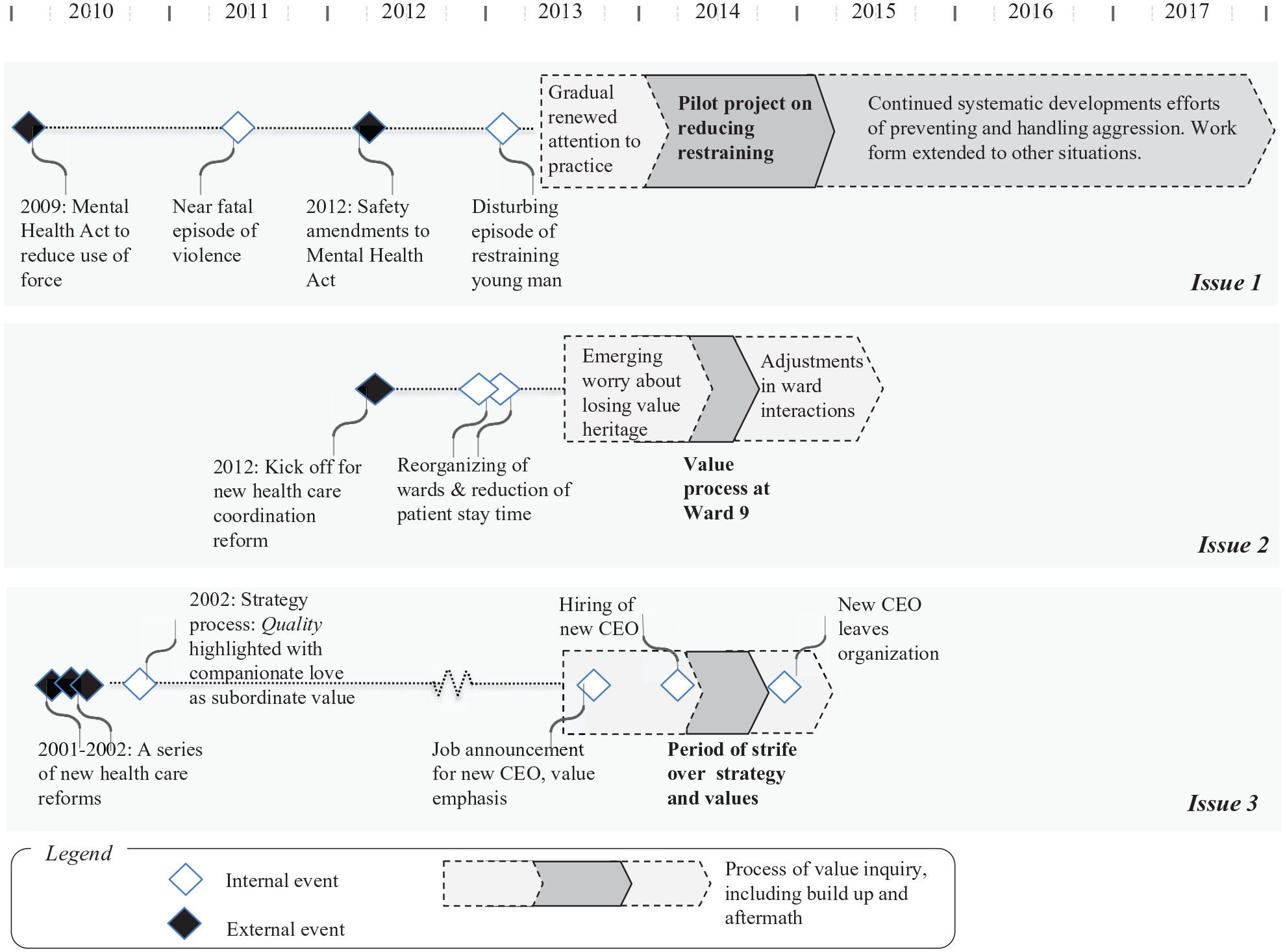
Timeline and key events for the three issues.
Findings: Three processes of value inquiry in comparison
Our empirical investigation of the three value-related issues at the hospital shows intense and recurrent attention to questions of the common good when responding to new institutional demands, as well as producing instances of the good as part of the everyday practice of providing patient care. Still, the handling of the three issues varied considerably in terms of how they were considered ethically fruitful for the set of situations dealt with in the organization. We next describe the key events and the sequence of actions in handling each issue. Table 2 presents an analytical comparison where we use the analytical framework that we have charted.
Handling of the three issues in comparison.
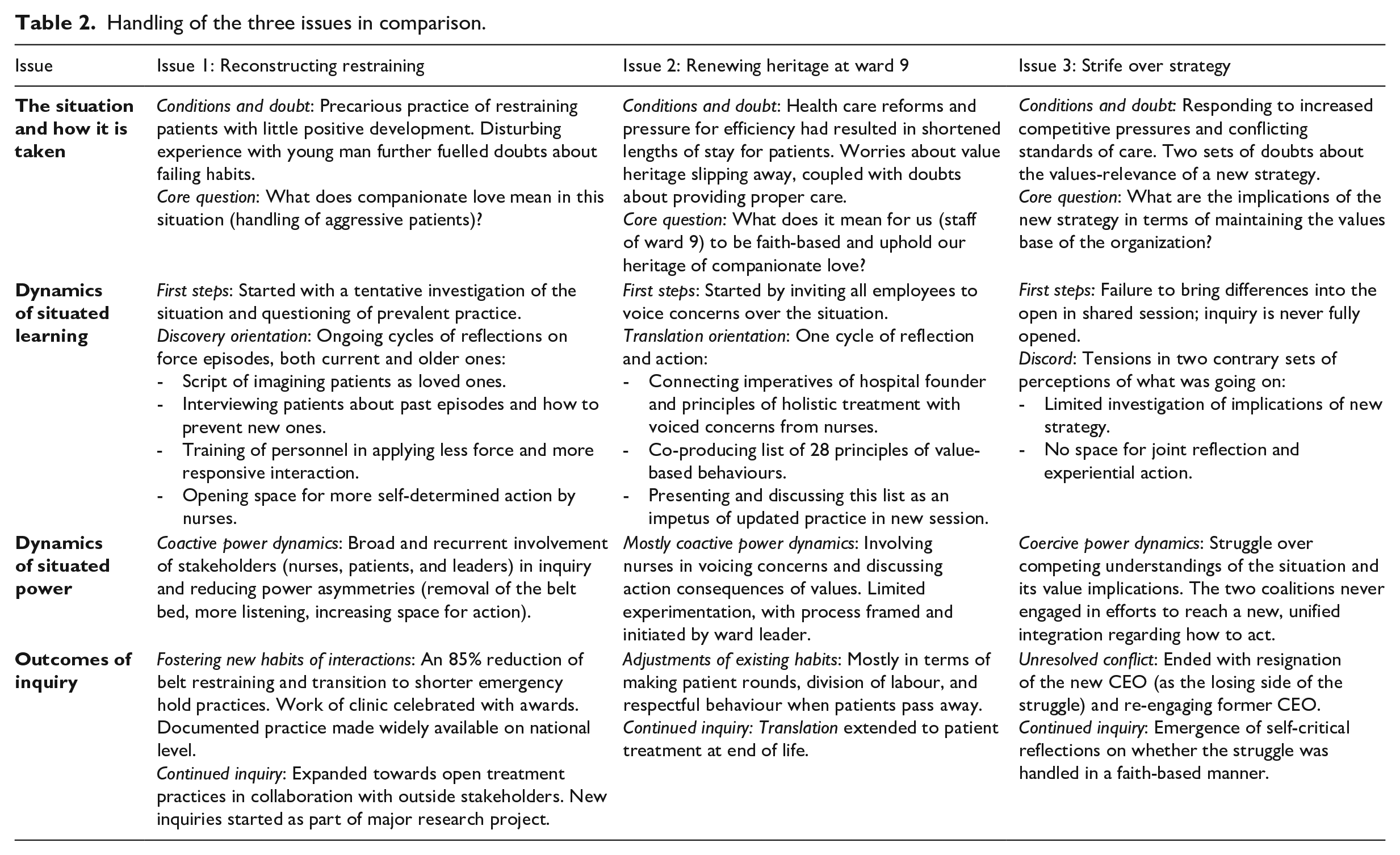
Issue 1: Reconstructing restraining
The situation and how it was taken
The context for the first issue was a sustained period of both organizational and public attention to the use of force in the handling of psychiatric patients. This attention dated back to a Mental Health Care Act in 1999, which imposed stricter regulation regarding the use of force, whether through seclusion, belt restraining, or pharmacological substances. However, according to several of the clinic leaders, as well as research reports and media articles, little had changed. In 2011, a nurse at the hospital was almost killed by a patient. As a result of this and other episodes, the Mental Health Care Act was extended with safety amendments in 2012.
This was the context in early 2013 when Tord began working as a new department nurse at the acute psychiatric clinic, before later becoming the clinic leader. Tord tried to get into his job by taking part in daily operations. A key activity of frontline workers in the acute psychiatric clinic is to receive and screen new patients, often in situations where they are brought in by the police, sometimes handcuffed and in conditions of deep despair and aggression. Within the course of a few minutes, medical personnel need to assess the circumstances and determine whether further restraining is called for or if other courses of action are possible. It can be a precarious situation. Belt restraining can be deeply traumatic. Medical personnel can be wounded, even fatally. During one such situation, as told by Tord (and corroborated by others), an aggressive young man is brought in. He breaks a table, pulls apart one of the legs, and starts waving it against the people in the room. Three of the caretakers throw a blanket at him for diversion and manage to pin him to the ground. Said Tord: At that very moment, he breaks down and cries uncontrollably. There is no more aggression. But by then, it is too late. The standard procedures kick in with injection and belt restraining. I can just feel we are wounding him, that this will stay with him. I cannot help thinking – what if this had been my father or brother? There must be some other way.
To the new manager, the episode was deeply upsetting and it haunted him. He initiated a series of discussions: ‘We simply realized that we had not examined our practice critically enough. How can we meet our patients in a more respectful way? What exactly does companionate love mean in this situation?’
Dynamics of situated learning and power
The first steps of inquiry started with staff looking at records of previous cases in which force was used and consulting the statutory objectives of the law from 1999. As emphasized by Paul, a psychologist and one of the staff members who became central in the processes that followed: The law text is completely unambiguous here. It states that [the use of belt restraints] should be the last way out (. . .). So, when you then start reflecting on those situations where we had used belts, there were several episodes where we concluded that we had in fact, not tried everything. (. . .) We started to thematize that before commencing the project itself (. . .) [we were] trying to have a critical look at our own practice instead of relying on automatic behaviours and doing what we always have done. That’s the easiest way. Doing something over a very long time period establishes the illusion that we have the expertise and are done learning.
The ensuing discussions eventually led to a prolonged effort to reduce the use of belt restraints in the clinic, one that emphasized the involvement of all personnel at the clinic in the learning process. A project initiative gradually took shape, starting with simply placing green or red stickers on the shift plan on the wall to signal episodes of escalating aggressions that had led to belt restraining (red sticker) or had been handled otherwise (green sticker). According to an apprentice nurse, who expressed surprise to be fully involved in the efforts, this action ensured at least a minimum of collective attention to episodes of aggression in the preceding shifts. Later, this activity was extended to more systematic joint reflections on all episodes of force, both current and previous. The belt bed in the hall was removed to ‘defuse the setting’ (nurse, informal interview) and belts were stored in a box, symbolizing less coercive use of power (research article from the project, 2014) and generating a pause for greater deliberation before restraining.
Clinic leaders and employees initiated a formal pilot project at the start of 2014. It involved training personnel on how to practise short manual holding and preventive communication. Many of these activities emphasized more collaboration with patients, such as ‘listening with an attitude of wonder’, ‘trying to remain open and non-judgmental towards the patient’ and emphasizing ‘care over authority’. Said Paul: ‘We calmly tell [the patients] that we want to take care of them (. . .) and find other solutions (. . .) and try to guide them step by step through what is happening.’ The patients were also directly involved through formalized processes, including interviewing them about violence. The purpose was to initiate a learning dialogue with the patients’ history of aggression to prevent further episodes (research article from the project, 2016).
Two features of the power dynamics in the handling of this issue stand out. One is the repeated attempts to reduce asymmetries of power in patient interactions (removal of the belt bed, turning to an attitude of wonder and listening, imagining others as loved ones). Another is the opening for interactive influence between staff and with patients in tackling episodes of aggression. These are joint efforts of reflection and experimentation that engage people in inquiry and function to grow power of a coactive nature. It is an agentic power of emergent nature, manifest as a shared desire and capacity to transform the situation.
Outcomes for situation and organization
The pilot project led to a drastic change in the practice of handling aggressive patients, with an 85% reduction in restraining with belt use, for an average of 5 to 6 hours, in favour of much shorter hand-restraining by nurses, lasting from 9 to 16 minutes. Of 839 admissions during the first project year, only 3 were addressed with belt restraining (research article, 2016). Afterwards, the unit and its leader were honoured for the change in practices, receiving the Acute Psychiatric Prize (2017) and the Health Care Leader Prize (2017). Commenting on the project, the CEO of the hospital, Anders, emphasized how this was a bottom-up initiative of ‘letting values steer priorities’ that he would highlight as a source of inspiration elsewhere in the organization.
In 2018, the new practice was documented in a report to other hospitals in the country. However, as Tord emphasized, ‘This cannot be the end of the process, only the start. We need to continue challenging ourselves and involving people.’ In these continued efforts, patients’ primary health care contacts, along with next of kin, were at the time of data collection increasingly involved in trying new open treatment practices, later to become the subject of clinical trials. Finally, in 2020, the hospital was the only one in the country to join a larger European research project on systematic development work in patient treatment, safety and healthy workplaces. Habits of value inquiry had begun to take hold elsewhere in the organization.
Issue 2: Renewing heritage at ward 9
The situation and how it was taken
In October 2014, Hilde, the leader of ward 9 at the hospital, started a two-month process of discussing the value-based heritage of the institution with her employees. The focus was on consequences for nursing practice. The wards at the clinic had recently witnessed changes because of the new Health Care Coordination Reform (report no 47, 2008–2009) following in the wake of new hospital ownership reform (report no 66, 2001–2002). To reach new targets of increased efficiency while maintaining professional standards and patient interests, management responded by merging three wards into two and reducing the number of patient beds. The length of patient stay decreased from 7 to 2 days. To the staff at ward 9, these demands and changes were increasingly experienced as conflicting with patients’ needs for care. In interviews and observations, nurses spoke of feeling stressed and worrying about what was now involved in proper care (observations and interviews). As Gudny (nurse) voiced, ‘There was no place for arguing for sitting at the bedside of a patient, but that’s what I’ll do now.’
Others saw the reforms as threatening the organization’s heritage (Siv, clinic leader). This was particularly heartfelt by Hilde, a nurse at the hospital for 38 years who had been trained by the last of the caretakers holding the deaconess title. Hilde knew the history of the organization particularly well and worried whether she could pass on the heritage from the founder, for whom she repeatedly expressed a deep sense of pride in the interviews. To her, part of this heritage was to show respect for patients and to treat each person with dignity: ‘What do I see in a patient? Do I only see the fragile old lady, or do I see the beautiful young bride?’ A picture of the founder hung in Hilde’s office, along with friendly imperatives from the deaconesses’ nursing philosophy such as ‘always greet patients when entering rooms’, ‘use the polite personal form to patients’, ‘always bid them farewell or good night’, and ‘no shouting of messages’.
Dynamics of situated learning and power
On this basis, Hilde initiated a process to discuss the situation, with the lingering question being: ‘What does it mean for us at [ward 9] to be faith-based now, in this situation?’ (Hilde, interview). The first step of inquiry started with an invitation for all to submit their concerns about daily tasks in the wake of the recent changes. Next, 13 of the nurses (out of 30) participated in an evening meeting to discuss how to generate better care for patients and improve the work environment for professionals. At this meeting, Hilde highlighted the founding deaconess’s work as a forerunner of holistic treatment that emphasized the totality of patients’ situations, seeing them as whole persons, and the norms for respectful behaviour in nursing (see above). The discussion led to 28 suggestions of succinctly formulated principles of values-based behaviours that Hilde subsequently presented and further discussed at a personnel meeting for all 30 employees of the ward. Compared to how issue 1 was handled, this process also involved employees, though it began more from the concern of losing heritage than from a critical examination of the facts of the situation. Fewer openings for critique, experimentation and interactive influences lead to, we suggest, less potential for creative action and building coactive power.
Outcomes for situation and organization
The process was said ‘to heighten awareness’ (Nina, nurse) by translating and aligning the meaning of the heritage to desired adjustments in work practices. One area of particular emphasis was the need to uphold a quiet, calm and compassionate atmosphere in the ward. In later observations on the ward, this emphasis reverberated as several patients experienced the atmosphere as different from other hospitals: ‘Other places are much noisier. Here, it is so quiet’ (Ann, patient). Overall, one of the nurses experienced the new practice as ‘[a] completely different calm (. . .) I’m not feeling the same stress as I did before’ (Thea, nurse). Another emphasis was changing routines during patient visits, with primary nurses joining physicians in ward rounds to establish better communication and information exchange.
An additional adjustment was a new ritual to make professionals aware that a patient had passed away. When a candle with a black band was lit in the reception area, it signalled that professionals should walk quietly, even when in a hurry, to show respect for the mourning family members. Later, these practices were adopted by others of the hospital’s wards; for example, in the care of patients with rare medical conditions (Hanne, ward leader). Finally, the process led to a similar discussion focusing on the respectful holistic treatment of patients during the last stages of life.
Issue 3: Strife over strategy
The situation and how it was taken
The third issue we investigated started with the hiring of a new CEO, Bjarne, in 2014. This situation also had deeper historical roots and handling it entailed an inquiry that failed in many ways. It was the least fruitful of the three. Bjarne came from a background in business, politics and public administration. He was hired based on discussions related to a series of health care reforms dating back to 2001–2002. Both Anders, the CEO since 2002, and the board realized that the organization would inevitably face increased competitive pressure from business-like health care initiatives in the larger institutional environment (interview with head of the board). The new CEO was meant to be a response to these demands. The board and management were looking for a proactive person with a broad background, a person who could approach the organization with fresh eyes but still nurture its values orientation (as also emphasized in the job announcement).
Only one month after his arrival in May 2014, Bjarne initiated changes that many saw as provocative. He strengthened staff by hiring consultants with little knowledge of health care and cut direct lines of communication from chief physicians and other personnel to upper management. More contested was the launch of a new strategy for the hospital to be a more effective developer of local health care services. At the heart of the dispute were plans to re-open a unit of acute surgery for patients in the city boroughs served by the hospital, a service that had previously been abandoned when choosing to cultivate specializations at the highly successful (in productivity and national esteem) surgical department. According to Geir, the clinic leader of the surgical department, Bjarne ‘had started a war against those who are working here’.
Dynamics of situated learning and power
The set of arguments for and against this new strategy were explicitly values-based, with both sides referring to companionate love and quality in in relation to the suggested plan. The new CEO saw the potential of being able to offer acute surgery as an extension of the mission of the hospital and expanding the enactment of companionate love through services offered in the local community (Bjarne, interview). Others, like the clinic leader of the surgical department, Geir, emphasized how the value of quality was manifest in high demand and economies of scale for specialized services. That demand in turn provided margins that indirectly enabled companionate love for the marginalized in yet other services. Said Geir: He makes the impression that he has no understanding of what we are doing (. . .) Everyone who has worked there [acute surgery] knows it is a completely different workplace [from specialized surgery] (. . .) because then you need to take those who come in with the blue lights, the ones with a broken leg or who are about to lose their leg. You’ve got to take it on before anything else. [Now] it goes to [another hospital in the same city]. They do this best, right? (. . .) But if you mix those cards, you ruin things completely.
The situation gradually emerged as conflicting with these contrary perceptions of what was going on. The new CEO interpreted the resistance as coming from ‘surgeons who are not used to being exposed to leadership’ and who ‘have been allowed to decide what to do’ (Bjarne, interview). He perceived being hired ‘with a mission to be proactive (. . .) What I experienced was that the employees were faith-based only when necessary [for their own purposes]’. To others, the president’s new suggestions were experienced as devaluing what the employees had been building up, not ‘taking into account that we have a history’ and ‘underestimating the competence of medical personnel’.
Geir framed the dispute as a power struggle: ‘This was all [a power strife] about the identity of the hospital.’ Yet other voices were more balanced when highlighting that the new CEO had been disadvantaged when ‘coming in with a different language’, and that learning how to navigate in the established values-based discourse was a taller order than people had expected (interviews).
The two competing interpretations of the value implications remained separate provinces of thought that were variously attacked and defended but never openly shared. Previously, the value implications of acute versus specialized surgery had undergone scrutiny during and after the health care reforms of 2000–2001. Yet the history of handling this situation was not brought up fully in 2014. The discussion was divisive with little space for joint reflection. Opposing views were regarded as threats, and coercive power reigned. A neutral bystander described the lack of early involvement of medical personnel in the new plans as a cardinal relational blunder, like ‘brewing scallop soup without involving the assistant chefs’ (Arne, section leader). Several attempts were made to resolve the situation. A letter from clinic leaders was sent to the board, highlighting the need for further enhancing companionate love and quality as core values of the hospital.
Outcomes for situation and organization
In November 2014, Bjarne resigned after four months of turmoil, concluding: ‘The board wanted calm.’ Afterwards, reactions were mixed. Some were content with what they saw as an inevitable outcome. Others took a more self-critical stance: ‘Did we do the right thing? (. . .) it was not very faith-based what happened, no forgiveness’ (Siv, clinic leader). One impression that persisted was that the conflict need not have escalated. The organization had failed to engage in an open process of inquiry about what the suggestions from the new CEO would entail. The previous CEO was subsequently re-engaged, committing himself to be more transparent and rebuild a shared sense of community, expressing upon return that ‘I left one team and came back to two’ (Anders, reinstated CEO).
Spaces of value inquiry
An analytical summary of the findings is due before we turn to a deeper theoretical discussion. Figure 2 depicts how the three processes of issue handling exemplify types of value inquiry characterized as discovery (issue 1), translation (issue 2) and discord (issue 3).
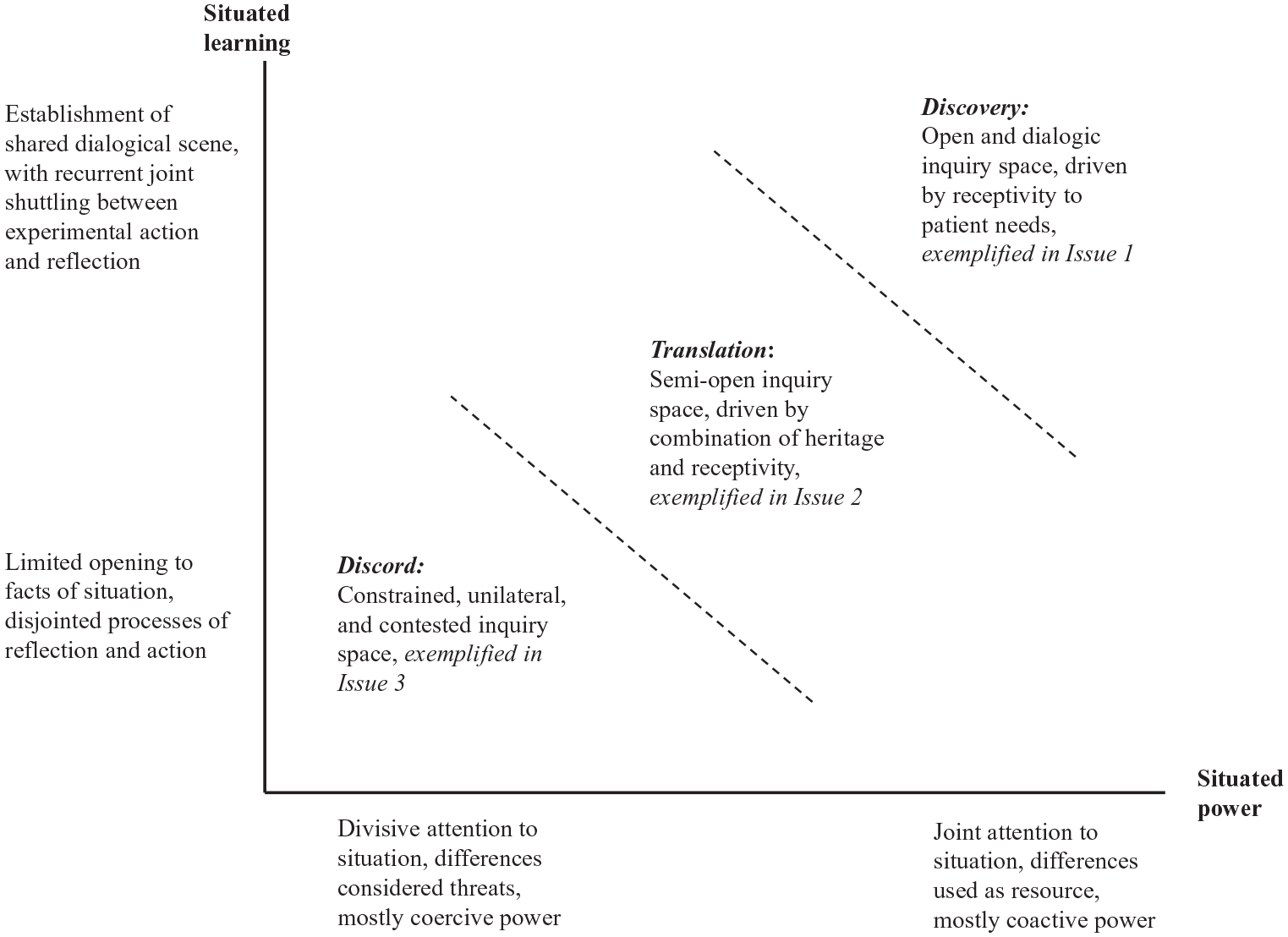
Spaces for value inquiry as situated learning and power.
Our findings suggest that fruitful value inquiry involves the opening of troublesome situations in a way that questions previous practice, enlists people in co-defining what is needed to meet the needs and desires of transformation, and engages in recurrent joint attention to problematic episodes through a sequence of sustained reflection and experimental action. This is the pattern for handling issue 1, the reduction of the use of belt restraints for patients in acute psychiatry. The handling of this issue, which we label discovery, constitutes a dialogic and experimental space for inquiry driven by receptivity to patient needs and shared desires for transforming the clinic’s practice. Of the three processes, the handling of this issue had the most beneficial outcomes for the situation and the organization at large. At its core was the establishment of a shared dialogical scene with joint attention to the situation. That in turn seeded the emergence of agency and coactive power as relational capacities to purposively transform the situation for the better. People were not merely enacting established standards but enlisted into a process of co-discovery, with patients.
Conversely, our data also suggests that the handling of values-related issues that did not involve key elements of inquiry (opening the situation, engaging people in joint experimentation and reflection) – such as the handling of issue 2 and issue 3 – showed more modest or negative outcomes. This was true even when people operated with the very same emphasis on the superordinate values of companionate love and quality of services. The handling of issue 3 offered limited opening or joint attention to the situation in terms of discussing the proposed strategy’s value implications. It appears a disjointed process in which differences in views and assumptions about the strategy’s potential consequences are used in a struggle for coercive power. Here, the value inquiry takes the form of discord between opposing provinces of reasoning.
Issue 2 can be understood as occupying a middle ground between these two outliers. Here, we see a more bounded form of value inquiry taking the form of a translation of the heritage of the organization and its founder into present concerns, less so a full opening of the situation and a critical examination. Indeed, one can see this as typifying values work that starts more from desires to uphold preconceived ideals than from opening an inquiry into the particulars of what was absent.
Our mapping of spaces for value inquiry in the handling of the three issues is as much a characterization of the processes of inquiry as their outcomes. The situation is the trigger, the site and the outcome of inquiry (Lorino, 2018, pp. 103–104). Thus, further moves in terms of reopening the inquiry (issue 2 and issue 3) or closing it down (issue 1) could work to transform the situation and create a new dynamic. For example, making the renewed practice from the handling of issue 1 mandatory and stopping further experimentation, reflection and surfacing of precarious experiences would likely diminish attention given to the uniqueness of each situation and reduce the potential for agency and coactive power to emerge. Conversely, making issue 2 a generator of agency and coactive power could require a deepened examination of the situation and more involvement of employees in continued experimentation.
Discussion: Towards a Theory of Value Inquiry
This paper’s primary contribution is a first theorizing of the notion of value inquiry as it emerged from our abductive coupling of empirical analysis with an underappreciated aspect of Dewey’s theory of valuation. Despite considerable research on values work in organization studies, knowledge about its critical, creative and open-ended nature remains partial.
We have addressed this void by foregrounding the discovery-oriented and transformative constructing of the good, thereby also answering calls for more research on the bottom-up, emergent nature of values work (Gehman et al., 2013; Vaccaro & Palazzo, 2015). Our agenda has not been to deny structural resources in values work, but to provide a shift in emphasis towards processes that bring new values-based repertoires of action into being.
Broadly, the conception of value inquiry suggests that researchers and practitioners devote less attention to processes of maintaining or using values considered ends-in-themselves and more attention to troublesome situations where values are at stake and the relational processes of inquiring together. Along with such a shift comes potentials for understanding work on values in organizations as a distributed and emergent phenomenon rather than forming toolkits of top management.
Further highlighting what we believe to be the uniqueness of our contribution, we will now dwell on two features of value inquiry that are particularly salient from the analysis – each with its own implications for further research. First, by theorizing value inquiry, we relocate ethical agency and the associated coactive power in an evolving issue field. The field of the indeterminate situation is the cradle of desires in value inquiry, with agency and power emerging as a relational capacity from what is ethically absent. We explain below how this emergence depends on how the situation is opened for co-discovery and how people are invited as actors.
Second, our study suggests that value inquiry is most powerful when it is an ongoing, as opposed to a one-time affair, that is, when it grows habits of inquiry. This involves the building of habituated repertoires of action for dealing with specific situations as well as engaging people in organizations in a more open-ended and continual ethical search.
Relocating ethical agency in an evolving issues field
Value inquiry is ethically fruitful and enriches organizational capacities for constructing the good when it sustains the emergence of ethical agency. This insight from our study relocates ethical agency, and the associated coactive power, away from taken-for-granted value conceptions or organizational authorities to emergence in a social field of inquiry. This is a conception of agency that involves an analytical focus on the evolving issue field (Carlsen & Kvalnes, 2023; Dewey & Bentley, 1949 [1991], pp. 107–112; Follett, 1924 [1951], pp. 206–207). In such a field (as exemplified in issue 1), agency cannot be attributed to preformed subjectivities but is a quality of the evolving whole of persons (nurses, patients, managers), their interaction events (stories of prior episodes of patient handling), invocations of past and present voices, as well as co-created resources and symbols (early research articles, stickers on a shift plan, the removal of the belt bed, leadership awards). This is important because it highlights the distributed and collaborative nature of ethical agency, shifting the focus from individual actors to the interactions and resources within evolving situations.
The contrasts between our three cases show that there is nothing automatic or determinate in having agency and coactive power emerge from troublesome situations. Rather, depending on how the situation is taken and how people are involved, agency may emerge in the larger field. One condition for emergence involves how a situation is examined and questioned in order to prepare the ground for joint learning – as a Deweyan approach would imply (Dewey, 1938 [1991], pp. 109–112). This serves to open the situation for further scrutiny to clarify what is lacking and challenge prevailing practice.
A second set of conditions is the need to bring potentially conflicting views and differences into the open – as Follett’s (1940) insights would suggest – thus establishing a dialogical scene in which a multiplicity of voices can be heard (Cooren, 2020). The agentic power with, as illustrated in the handling of issue 1, emerges as a relational capacity from inquiry. It is manifest not only in how people are given an opportunity to participate and give voice, but also in how they challenge (through critical attention to prior practice), experiment (with new ways of handling aggression), and are receptive to the concerns of the human other (patients and colleagues).
These findings point to a potential for unpacking the micro-relational foundations of work on values in organizations. Of particular interest for further research are the conditions and relational processes by which desire in value inquiry is seeded and how the agentic powers of inquiry may emerge from receptivity to the needs of others (Carlsen & Kvalnes, 2023). We have described a case underlining the importance of perspective taking (Bolino & Grant, 2016) and continued inquiry when awakening compassion towards others (Worline & Dutton, 2017). Broader questions remain: What kinds of opening of situations best stimulate perspective taking of employees and beneficiaries? How do people activate shared sentiments that something is at stake in value inquiry?
Our findings also suggest reconsidering the role of agency and power in a responsive ethics (Rhodes, 2023). Agency emerging from value inquiry is neither a form of coercive power nor a property of heroic individuals who obey or resist authoritatively prescribed beliefs. Instead, the co-emergence of agency and power as a joint capacity marks a receptive and responsive form of ethical agency, one premised on distributed interactions (Munro & Thanem, 2018) in continued discovery.
This implication points to a latent tension between an organized ethics and one that continues to be responsive (Rhodes, 2023). We have suggested that ending value inquiry after having built a more ethically responsive practice (as in a national standard for handling aggression in psychiatric clinics) may function to diminish attention to the idiosyncrasies of situations and reduce perspective-taking. Simply sanctioning a repertoire of actions resulting from value inquiry and rolling it out as a canonized standard could weaken the basis for agentic power of an emergent nature. Yet, situations are likely to differ in terms of the vulnerabilities of the persons involved and the need to maintain receptive openness. In which types of situations is it likely that desires for inquiry co-evolve with, or stand against, desires to uphold values-based repertoires of action?
Recognizing the importance of fostering habits of inquiry
When value inquiry is at its most fruitful, as evidenced in the handling of issue 1, our study suggests that the discoveries people make during inquiry will reorient (Golden-Biddle, 2020) and renew prevailing habits of action. This takes two forms. One is through building a habituated repertoire for responding to a type of situation (e.g. screening and receiving aggressive patients). Fostering such intelligent habits (Dewey, 1922, pp. 40–44) of a collective nature means a gradual development of thought–action repertoires that may be flexibly drawn upon and extended to deal with new situations. The narrative script of imagining others as loved ones, and the weight placed on attending to patients with an attitude of listening and wonder, can be seen as an attempt to embed elements of continued inquiry into habits of action, thus seeding in them a self-renewing capacity. This role of inquiry complements other understandings of how to build collective repertoires, such as the role of contestation in reworking value practices (Gehman et al., 2013) or joint reflection on localized versus generalized situations (Cunliffe & Ivaldi, 2021).
It is important to recognize here that fostering habituated repertoires of actions does not stop at formulating abstract rules of what to do. Value inquiry renews habits when continuously connecting and reconnecting challenging situations over time. Our research suggests that the action-guiding potential of a value commitment (such as companionate love) is not unleashed until it is connected backwards to previous episodes (of patient handling or strategy discussions) as a source of reflection and building of repertoire – and connected forward through future episodes when engaging in experimental action. ‘What have we experienced in the past that may enable us to cope with this situation?’ To recognize the salience of this process is to recognize the inherent temporality and potentiality for agency (Emirbayer & Mische, 1998) in values work. When cut off from their moorings in troublesome situations (such as in the handling of issue 3), one risks values being taken for granted and becoming empty labels without action consequences.
This insight from our study is understated in the larger literature on values work but is incipient in two studies on anchoring as a way of reconnecting values to situations (Chatterjee et al., 2021; Vaccaro & Palazzo, 2015). For example, in their study of values work in social entrepreneurship, Chatterjee et al. (2021, pp. 11–12) showed that anchoring took the form of listening to stories about experiences associated with traditional rural values (connecting back), followed by initiating developmental efforts that signified oneness with those values (connecting forward). By continually renewing the situational moorings where values are at stake, people may move beyond prescriptive and reified value conceptions into creative action.
Another form of habituation concerns fostering habits of inquiry in the organization more broadly. Our study has provided tentative evidence that successful inquiry at one site in the organization (handling issue 1) can be carried over to other sites (expansion to open treatment practices, participation in research projects). One could see such proliferation as not necessarily reproducing distinct work forms but rather as strengthening people’s heeding of the possibilities of discovery (Stark, 2009) and emphasizing values less as end states and more as a continued questioning about what is right and true (Alexander, 2013).
Continuing from this, our study suggests further exploring how value inquiry can help individuals be capable ethical actors across types of situations, activity systems and competing orders of worth (Stark, 2009). How does inquiry trigger individuals to reflect on, assess and alter their value orientations more broadly (Bednarek-Gilland, 2016)? How can value inquiry help people navigate, challenge (Cunha, Simpson, Clegg, & Rego, 2019) and contribute to sustaining moral orders (Kraatz et al., 2020) in large and complex organizations?
Conclusion
One of the founders of process philosophy, William James, once remarked, ‘My experience is what I agree to attend to. Only those items which I notice shape my mind – without selective interest, experience is an utter chaos’ (James, 1890 [1950], p. 402, emphasis in original). Value inquiry involves a shift in what people selectively agree to attend to in their ethical reasoning at work and how they do so. It is a shift away from attending to value conceptions as ends in themselves and towards what is ethically difficult and troublesome within organizational activities. Paradoxically, our study suggests that attending to value conceptions abstracted away from their situational moorings may be counterproductive. Rather, the attending we have noticed as particularly fruitful acknowledges that inquiry is driven by the specifics of what is ethically challenging in situations and the absence of a proper response (Giovannoni & Quattrone, 2018). Recognizing trouble and absence pushes people’s attending towards greater receptivity to the particulars and the possibilities of a situation, thereby inviting discovery that in turn may grow agency and coactive power. And the values that matter the most, such as companionate love, might reside in continued discovery of transcendent mystery, whether we choose to locate that in divinity (Bento da Silva, Quattrone, & Llewellyn, 2022) or our wonder in our meeting with the other (Carlsen & Sandelands, 2015).
Values come to life when one attends to the specifics of troublesome situations with the needs of others in their unique infinitude, the corresponding desire for transformation in these situations, and the opening for creative action that may follow. Value inquiry is less about maintaining, complying with and following and more about receiving, critiquing, responding and creating. In the end, constructing the good is a recursive loop. When at its most fruitful, value inquiry – that is, the whats and hows of the ways people in organizations agree to attend to ethical questions – feeds ethical agency, which in turn may feed further value inquiry. Ultimately, by attending to the evolving demands of situations, organizations can nurture a collective capacity for addressing ethical issues with responsiveness and creativity, thereby shifting focus from merely upholding values to continuously searching for and actively constructing the good.
Footnotes
Acknowledgements
We are most grateful to the people in the case organization, including patients, for their participation in this research. We thank Senior Editor Martin Kornberger and three anonymous reviewers for their deep engagement with our paper and very helpful comments. An earlier version of this paper was presented at the 12th International Process Symposium, organized online in 2021. For their support in discussions or readings, our gratitude also goes to Harald Askeland, Jane Dutton, Elena Giovannoni, Saku Mantere and Bjørn Erik Mørk.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.