
Abstract
The digital transformation of healthcare is a strategic priority, but its success depends on human and organizational factors. While research has examined digital literacy and maturity, little is known about how individual skills and inclusive practices shape organizational progress. This study addresses this gap by analysing the impact of Digital Literacy (DL) and Digital Inclusion (DI) on Digital Maturity (DM) in healthcare. Using a quantitative design and Structural Equation Modelling (SEM), results confirm that DL and DI are significant drivers of DM. Notably, DI emerges as a crucial mediator, showing that organizational maturity relies not only on stakeholders’ capabilities but also on equitable access and support structures. These insights emphasize that effective digital transformation must adopt human-centric strategies, prioritizing literacy and inclusion to ensure sustainable progress. By integrating these factors, healthcare organizations can strengthen digital maturity and achieve meaningful transformation outcomes.
Keywords
Introduction
Digital transformation has emerged as a strategic imperative for global healthcare systems, promising to optimize care delivery, increase operational efficiency and value, and improve patient outcomes (Shaw, 2019; Warsame et al., 2020). Technologies such as electronic health records, telemedicine, and mobile health (mHealth) applications are redefining how services are provided and consumed. However, the mere adoption of technology does not guarantee success. The true challenge lies in transcending simple digitization to achieve Digital Maturity a state where technological capabilities, human competencies, and organizational processes are cohesively integrated to generate value. Digital Maturity is, therefore, a key indicator of the success of digital transformation (Almaghaslah et al., 2022; Baniasadi et al., 2023; Hamasaki, 2024; Ploog et al., 2022; Santos-Jaén et al., 2022; Tossaint-Schoenmakers et al., 2021; Vogel et al., 2024).
In this context, ‘healthcare’ is interpreted as a holistic and systemic digital ecosystem, encompassing not only clinical practice but also the organizational management and the patient-centric interactions that define modern health services (3, 4). This research focuses on the demand-side of this ecosystem, where the digital literacy and inclusion of healthcare service users (patients) are viewed as essential components that feed into the overall digital maturity of the health system.
Digital Maturity is, therefore, a key indicator of the success of digital transformation (Almaghaslah et al., 2022; Baniasadi et al., 2023; Hamasaki, 2024; Ploog et al., 2022; Santos-Jaén et al., 2022; Tossaint-Schoenmakers et al., 2021; Vogel et al., 2024).
While the broader research from which this article is derived explored a comprehensive model including variables such as patient satisfaction, focusing on the foundational pathway of digital transformation. The central scope is to provide a detailed and empirical analysis of how Digital Literacy (DL) and Digital Inclusion (DI) serve as direct and indirect antecedents to Digital Maturity, a relationship that is foundational to understanding the success of any digital health initiative (Ahmed et al., 2020; Almaghaslah et al., 2022; Bancsik et al., 2024; Hamasaki, 2024; Khan et al., 2022; Lee, 2018; Melhem et al., 2023; del Pilar Arias López et al., 2023; Ploog et al., 2022; Santos-Jaén et al., 2022; Tossaint-Schoenmakers et al., 2021; Yan et al., 2024). Our research argues that an organization’s Digital Maturity cannot be achieved without the development and promotion of Digital Literacy and Digital Inclusion among its key stakeholders, including healthcare service users.
Digital Literacy, understood as the ability to access, manage, and use digital information effectively, and Digital Inclusion, which refers to equitable access to technology and the necessary support, are fundamental elements for the success of any digital initiative (Ahmed et al., 2022; Connolly et al., 2025; Doueiri et al., 2024; Jeong et al., 2019; Lee, 2018; Melhem et al., 2023; del Pilar Arias López et al., 2023; Rydzewski, 2025; Santos-Jaén et al., 2022; Tegegne et al., 2023; Wrona et al., 2025, p. 1; Yan et al., 2024).
This article aims to address this gap by thoroughly investigating the role of DL and DI in the • Analyse the influence of Digital Literacy on the adoption, and evolution of Digital Maturity. • Investigate the complex relationships and mediating effects between Digital Literacy, Digital Inclusion, and Digital Maturity.
By exploring these relationships, we intend to provide valuable insights for managers, policymakers, and healthcare professionals, contributing to the theory of digital transformation in healthcare by establishing that Digital Literacy and Digital Inclusion are the essential drivers for Digital Maturity, which, in turn, is a prerequisite for more effective and equitable healthcare systems.
Literature Review
Digital Literacy as a Driver of Organizational Maturity
While DL provides the necessary skills, it does not guarantee organizational maturity if structural barriers persist. This study argues that Digital Inclusion (DI) acts as the critical mediating mechanism between individual capabilities and collective maturity. This mediation can be theoretically grounded in the Digital Divide Framework, which emphasizes that the challenge of integrating eHealth depends on structure and process (Tossaint-Schoenmakers et al., 2021).
In our conceptual model, DI represents the organizational effort to bridge these divides by providing equitable access, continuous support, and a culture of participation. Theoretically, even highly literate individuals may fail to contribute to Digital Maturity if the environment is not inclusive lacking interoperable tools or technical support (Rydzewski, 2025). DI functions as a ‘catalyst’ that transforms individual potential (DL) into organizational reality (DM), ensuring that the digital transformation is not only effective but also equitable.
Digital Literacy is defined as the set of skills needed to access, manage, integrate, evaluate, create, and communicate information using digital devices and networks. For a healthcare organization to achieve a state of Digital Maturity, it is imperative that its stakeholders both professionals and patients possess an adequate level of digital literacy. The absence of digital skills can lead to underutilization of technologies, resistance to change, and failed adoption, regardless of the quality of the technological infrastructure (Yan et al., 2024).
In the contemporary healthcare landscape, DL is a multi-dimensional construct encompassing the ability to find and use information to improve care outcomes (10, 28). Recent evidence suggests that all healthcare stakeholders, particularly patients, must possess high levels of DL to interact effectively with digital health systems. Without a baseline of DL among service users, healthcare organizations cannot reach higher stages of Digital Maturity, such as personalized medicine and fully integrated digital pathways (Adel, 2022; Jeong et al., 2019).
Similarly, patient digital literacy empowers them to access and manage their own health information, which facilitates communication with care providers and promotes treatment adherence. Digital Literacy acts as the foundation upon which a healthcare organization’s Digital Maturity is built (Adel, 2022; Bekele et al., 2024; Connolly et al., 2024; Fitzpatrick, 2023; Jeong et al., 2019; del Pilar Arias López et al., 2023; Tartaglia et al., 2024; Tegegne et al., 2023; Temsah et al., 2023; Wang, 2023).
The Mediating Role of Digital Inclusion
Digital Inclusion complements Digital Literacy by addressing the barriers to access and participation in the digital society. Beyond individual competencies (Literacy), Digital Inclusion refers to the availability and accessibility of technology, as well as the necessary support for individuals to fully participate in the digital ecosystem (Rydzewski, 2025).
In this framework, Digital Inclusion (DI) is not viewed as a mere byproduct of Digital Literacy (DL). Rather, they are distinct but interdependent constructs. While DL represents the individual’s cognitive and technical capabilities, DI encompasses the structural conditions such as equitable access, affordability, and organizational support that allow those capabilities to be exercised (Doueiri et al., 2024; Jeong et al., 2019). Therefore, DI is perceived as a mediating environment: literacy provides the ‘know-how’, but inclusion provides the ‘means-to-act’. Without an inclusive structure, even high levels of literacy remain latent and fail to contribute to the organization’s Digital Maturity.
Healthcare organizations that foster Digital Inclusion, for example, by providing devices, internet access, and tailored training create an environment conducive to transformation (Ahmed et al., 2022; Connolly et al., 2025; Doueiri et al., 2024; Jeong et al., 2019; Lee, 2018; Melhem et al., 2023; del Pilar Arias López et al., 2023; Rydzewski, 2025; Santos-Jaén et al., 2022; Tegegne et al., 2023; Wrona et al., 2025, p. 1; Yan et al., 2024).
While DL provides the necessary skills, it does not guarantee organizational progress if structural barriers persist. Digital Inclusion (DI) acts as the critical mechanism that transforms individual potential into collective action. This can be theoretically grounded in the Digital Divide Framework, which emphasizes that successful eHealth integration depends on both structure (access) and process (support) (Ploog et al., 2022).
DI refers to the organizational effort to provide equitable access to technology and continuous technical support (Doueiri et al., 2024). Theoretically, even highly literate individuals may fail to contribute to the organization’s progress if the environment is not inclusive lacking interoperable tools or a culture of participation (Doueiri et al., 2024). DI functions as a catalyst: it ensures that digital literacy is effectively “activated” within the healthcare environment, moving beyond the ‘first-level divide’ (access) to address the ‘second-level divide’ (effective usage) (Jeong et al., 2019).
The Concept of Digital Maturity in Healthcare Organizations
The relationship between Digital Literacy (DL) and Digital Maturity (DM) is best understood through the Sociotechnical Systems Theory. This theory posits that organizational performance stems from the joint optimization of the social (human skills) and technical (infrastructure) subsystems. In healthcare, DM is frequently misconstrued as mere technological adoption; however, it represents a state where technological capabilities, human competencies, and organizational processes are cohesively integrated to generate value (Vogel et al., 2024). Recent studies in hospital settings further suggest that this maturity is a key indicator of successful digital transformation beyond simple profitability (Vogel et al., 2024).
Digital Literacy serves as the fundamental human component of this system. According to the Resources and Appropriation Theory (Cetindamar et al., 2024; van Dijk et al., 2010), the acquisition of digital skills is a prerequisite for ‘meaningful appropriation’ of technology. In this context, DL is now recognized as a new and critical determinant of health (del Pilar Arias López et al., 2023). Without a baseline of DL, healthcare professionals and stakeholders cannot move beyond basic usage to the advanced, innovative applications required to reach higher stages of DM. Therefore, DL is not merely an individual attribute but a strategic driver that enables the organization to transition from ‘doing digital’ to ‘being digital’.
Digital Maturity represents an organization’s capacity to leverage digital technologies to optimize processes, business models, and stakeholder interactions. In the healthcare context, it is not merely about implementing new technologies but about integrating a digital culture into all operations, from electronic health records to telemedicine and data analytics (Kaiser et al., 2021). Several digital maturity models have been proposed, typically categorizing organizations into stages ranging from basic digitization (initial level) to full digital transformation (advanced level). However, the literature has predominantly focused on organizational and infrastructural aspects, with less attention paid to the human factors that drive this maturity. Our research is positioned to fill this gap by exploring the human and social antecedents of Digital Maturity (Vogel et al., 2024). The digital literacy of professionals and their ability to adopt new technologies, such as AI, are also factors that contribute to the organization’s digital maturity (Bekele et al., 2024; Chereka et al., 2024; Tegegne et al., 2023; Wang, 2023).
In our proposed conceptual model (Figure 1), Digital Inclusion is viewed not only as an outcome of Digital Literacy but also as a crucial mediator between Literacy and Digital Maturity. Digital literacy may not translate into organizational maturity if individuals lack equitable access to technology. Digital Literacy empowers individuals, while Digital Inclusion ensures that this empowerment can be applied and integrated into organizational processes. Proposed Conceptual Model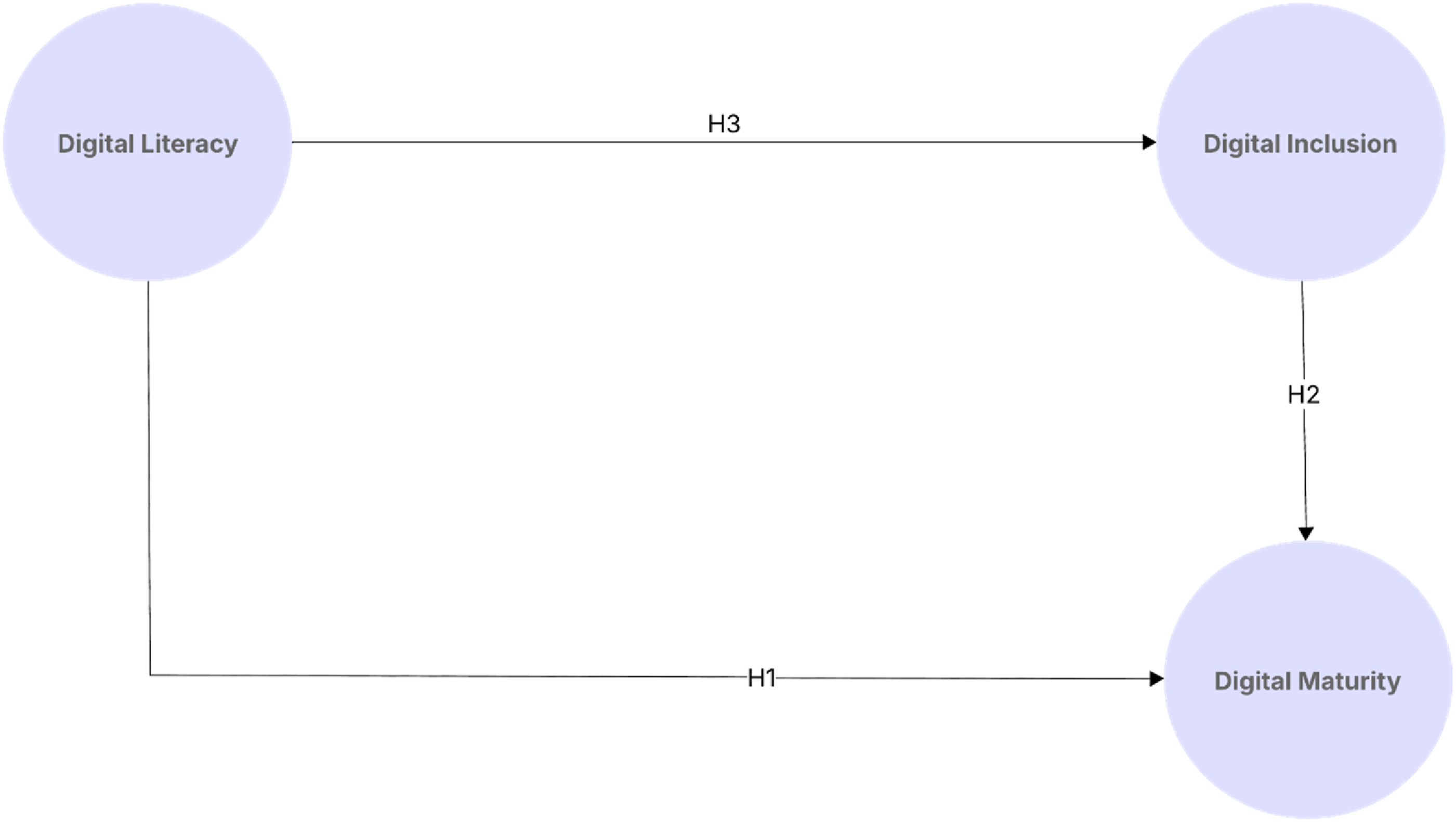
Research Hypotheses
Based on the literature, we propose the following hypotheses. • H1: Digital Literacy has a positive and direct influence on Digital Maturity. • H2: Digital Inclusion has a positive and direct influence on Digital Maturity. • H3: Digital Literacy has an indirect influence on Digital Maturity, mediated by Digital Inclusion.
Methodology
Research Design
This research employs a quantitative research design based on data collected, utilizing a cross-sectional approach to investigate the relationships between Digital Literacy (DL), Digital Inclusion (DI), and Digital Maturity (DM) in the healthcare sector. The research design is an extension of the conceptual model proposed, with a specific focus on the antecedents of Digital Maturity.
Sample and Data Collection
The target population for the quantitative phase of this research comprised patients who utilize or have the potential to utilize digital healthcare services in Portugal. This specific focus was chosen to directly investigate how the digital capabilities of end-users influence their perceived satisfaction and interaction with the evolving digital healthcare. The selection of patients as the research population is directly aligned with the overarching aim of understanding the impact of digital transformation from the service recipient’s perspective, complementing insights previously gathered from healthcare professionals in the qualitative phase. Participants were recruited through, online distribution via social media. The primary inclusion criterion was being a user or potential user of digital healthcare services in Portugal.
The quantitative data for this research were collected through a structured self-administered questionnaire, meticulously designed to operationalize the constructs of Digital Literacy, Digital Maturity, Digital Inclusion, and Satisfaction. The development of the questionnaire was based on a thorough review of existing literature and the adaptation of previously validated scales, ensuring the theoretical grounding and empirical robustness of the measurement instrument. The decision to use a sample of healthcare patients (service users) is theoretically grounded in the perspective that Digital Maturity is a systemic attribute. Since the success of digital health initiatives depends on the end-user’s ability to adopt and use technology, the patients’ digital literacy and perceived inclusion are critical indicators of the organization’s overall digital progress.
Each construct was measured using a set of specific items, primarily employing a Likert Scale Type, 5-point, where participants indicated their level of agreement or frequency for each statement. The items were carefully worded to be clear, unambiguous, and relevant to the Portuguese healthcare context.
Prior to full-scale data collection, the questionnaire underwent a pilot test with a small group of individuals from the target population to identify any ambiguities, ensure clarity of language, and refine the instrument.
The data collection process was conducted between October of 2024 and February of 2025. The survey was primarily disseminated online via a dedicated platform such as Google Forms, distributed through social media channels (Facebook and LinkedIn). This approach aimed to maximize reach and facilitate participation from a diverse segment of the target population.
Following the data collection process, a total of 212 valid responses were obtained and included in the final analysis. This sample size was deemed appropriate for conducting the planned statistical analyses, including Structural Equation Modelling (SEM), providing sufficient statistical power to test the proposed conceptual model and its hypotheses.
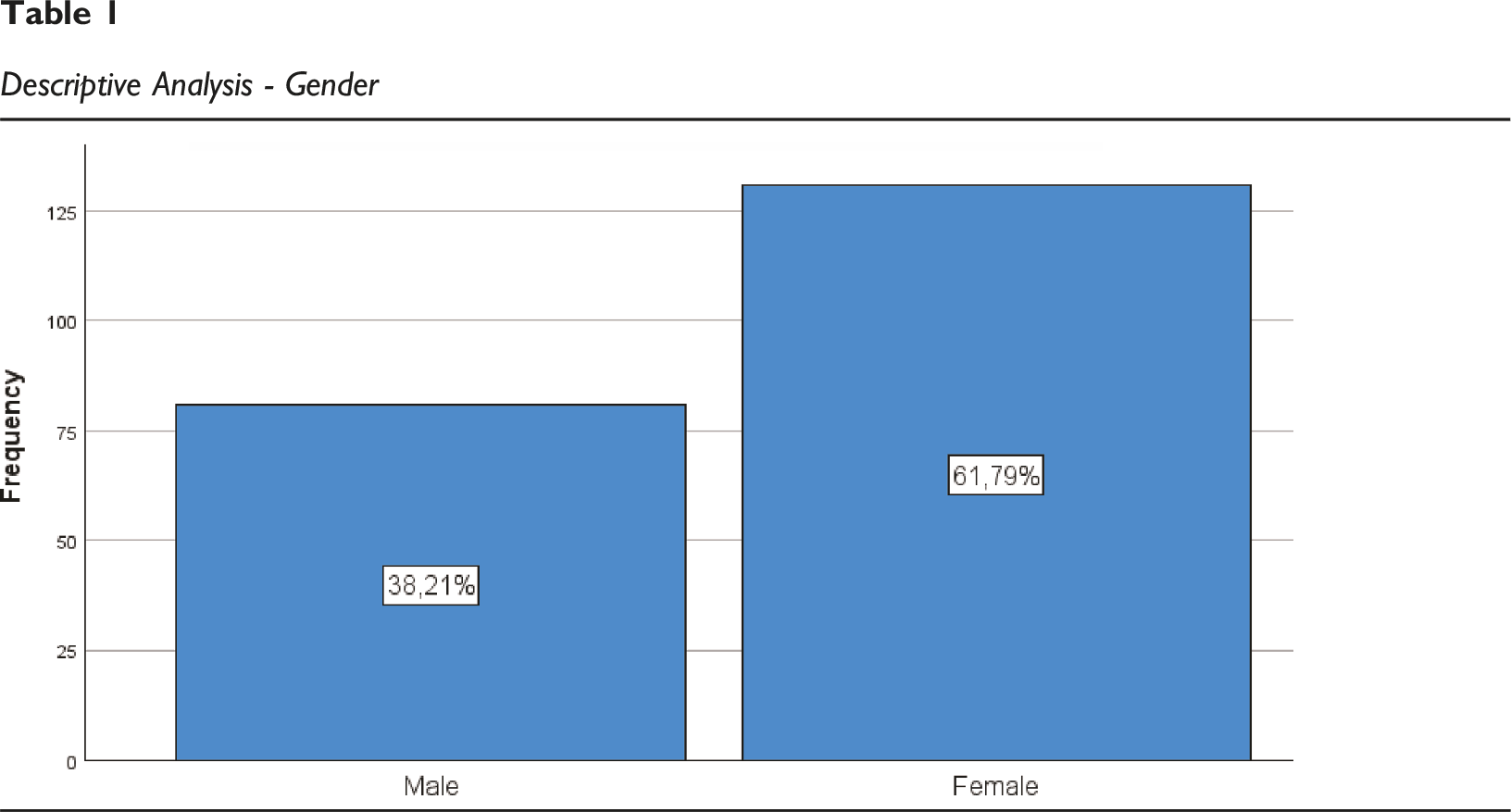
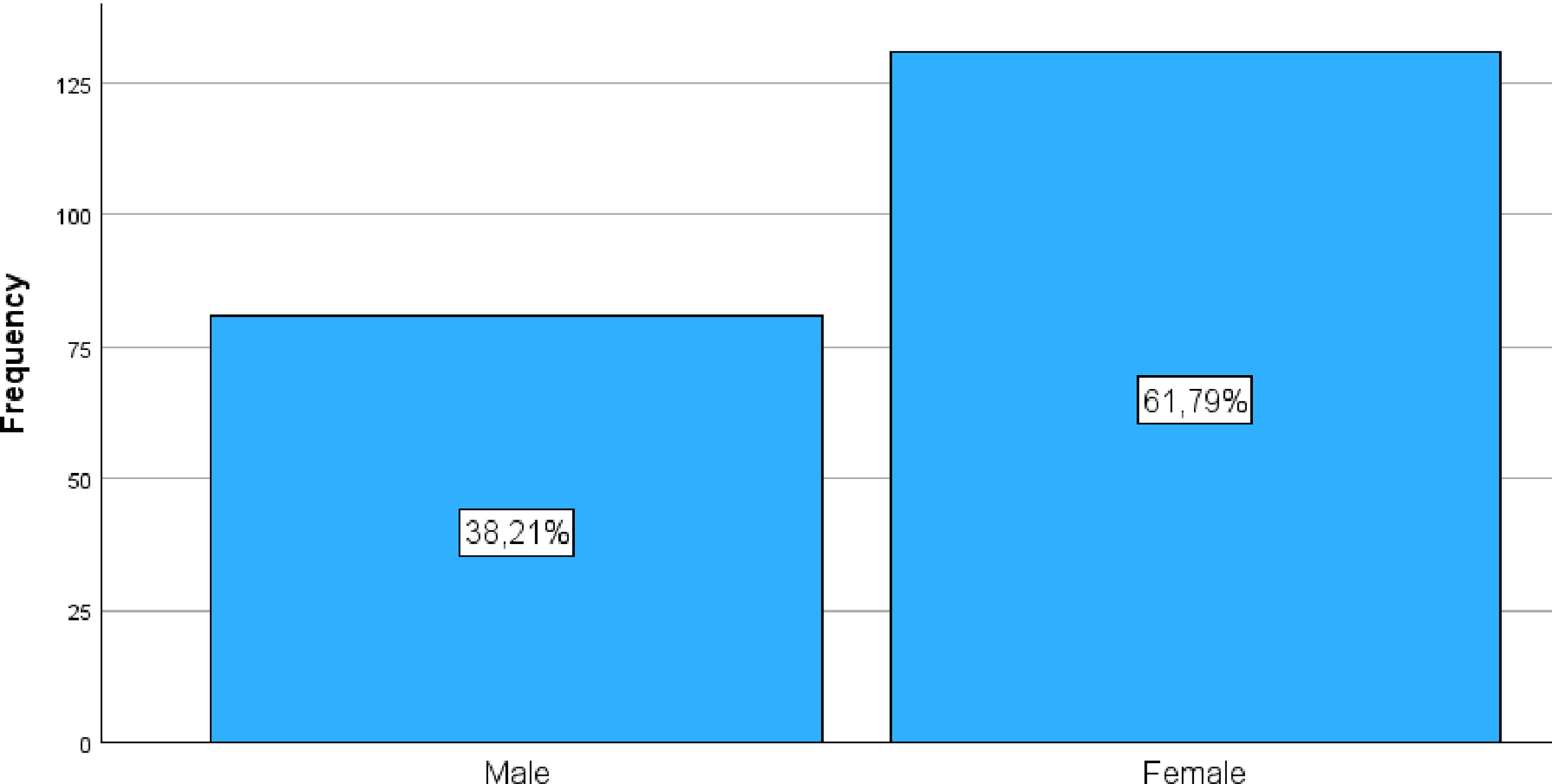
Descriptive Analysis - Gender
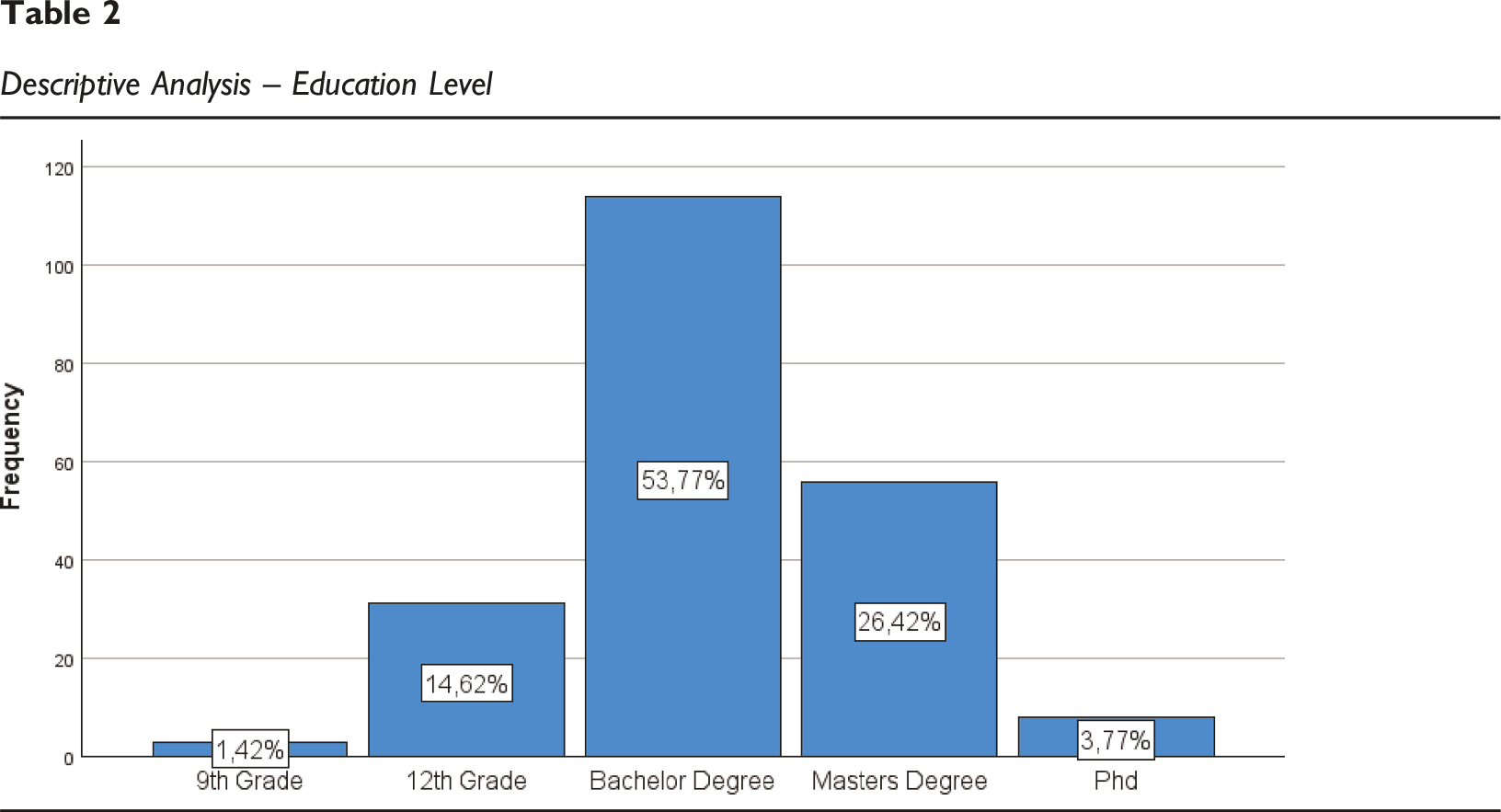
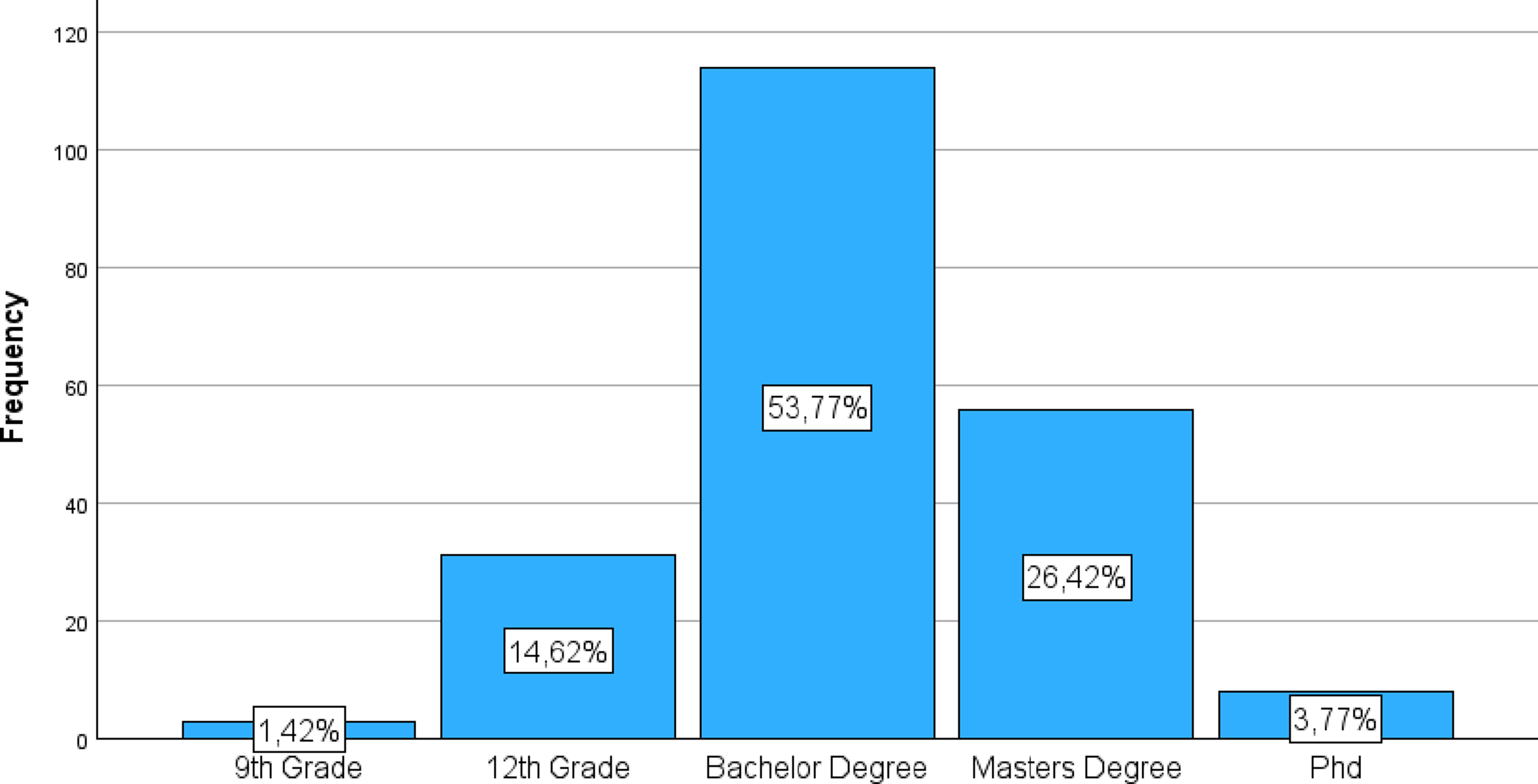
Descriptive Analysis – Education Level
Observations: • The gender distribution is predominantly female, with 131 participants (61.8% of valid cases); • Male participants account for 81 individuals (38.2% of valid cases);
Observations:
The sample exhibits a high level of education, with most participants having higher education qualifications. • 9th Grade: 3 participants (1.4% of valid cases); • 12th Grade: 31 participants (14.6% of valid cases); • Bachelor’s degree: The most representative category, with 114 participants (53.8% of valid cases); • Master’s Degree: 56 participants (26.4% of valid cases); • PhD: 8 participants (3.8% of valid cases).
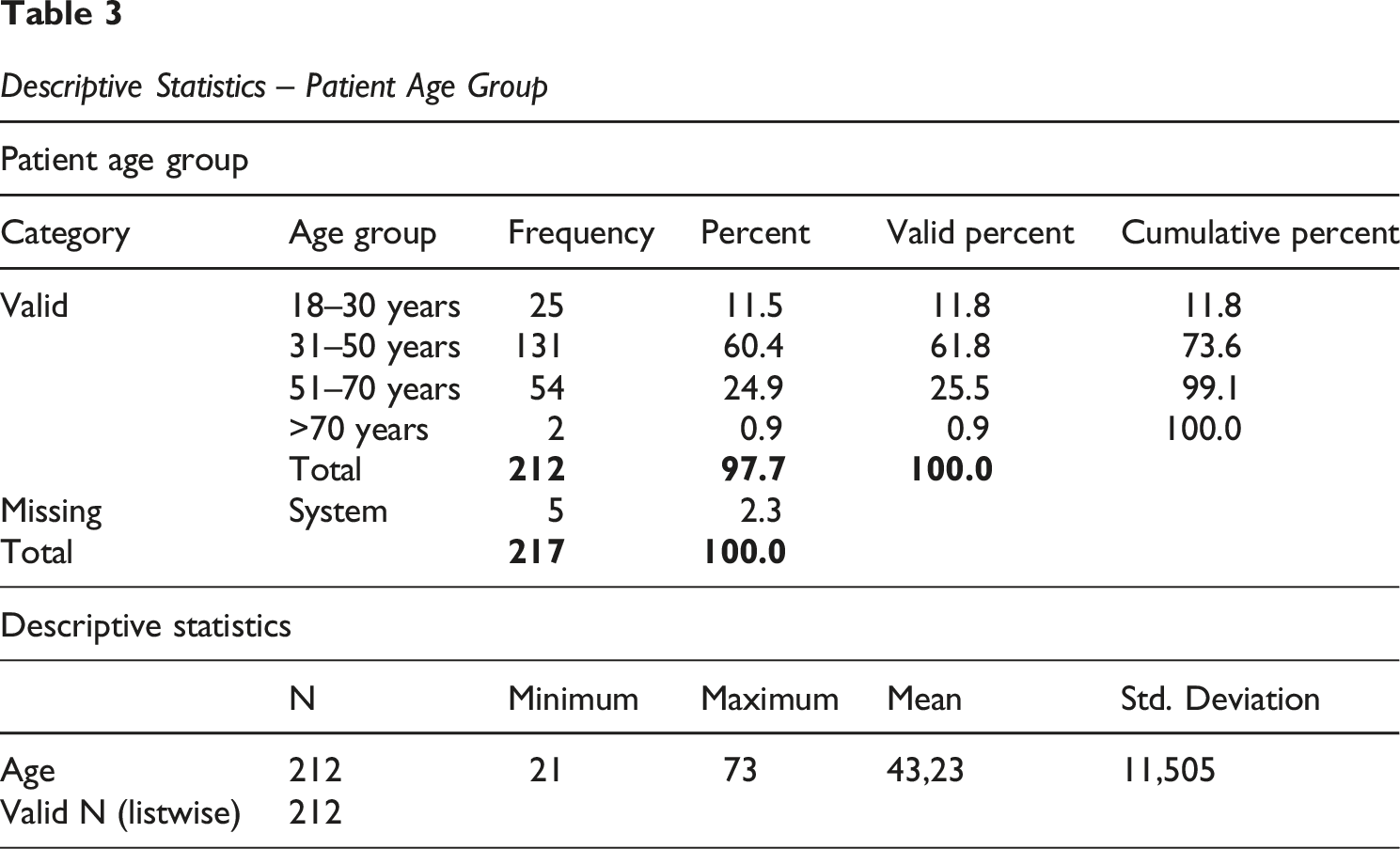
Descriptive Statistics – Patient Age Group
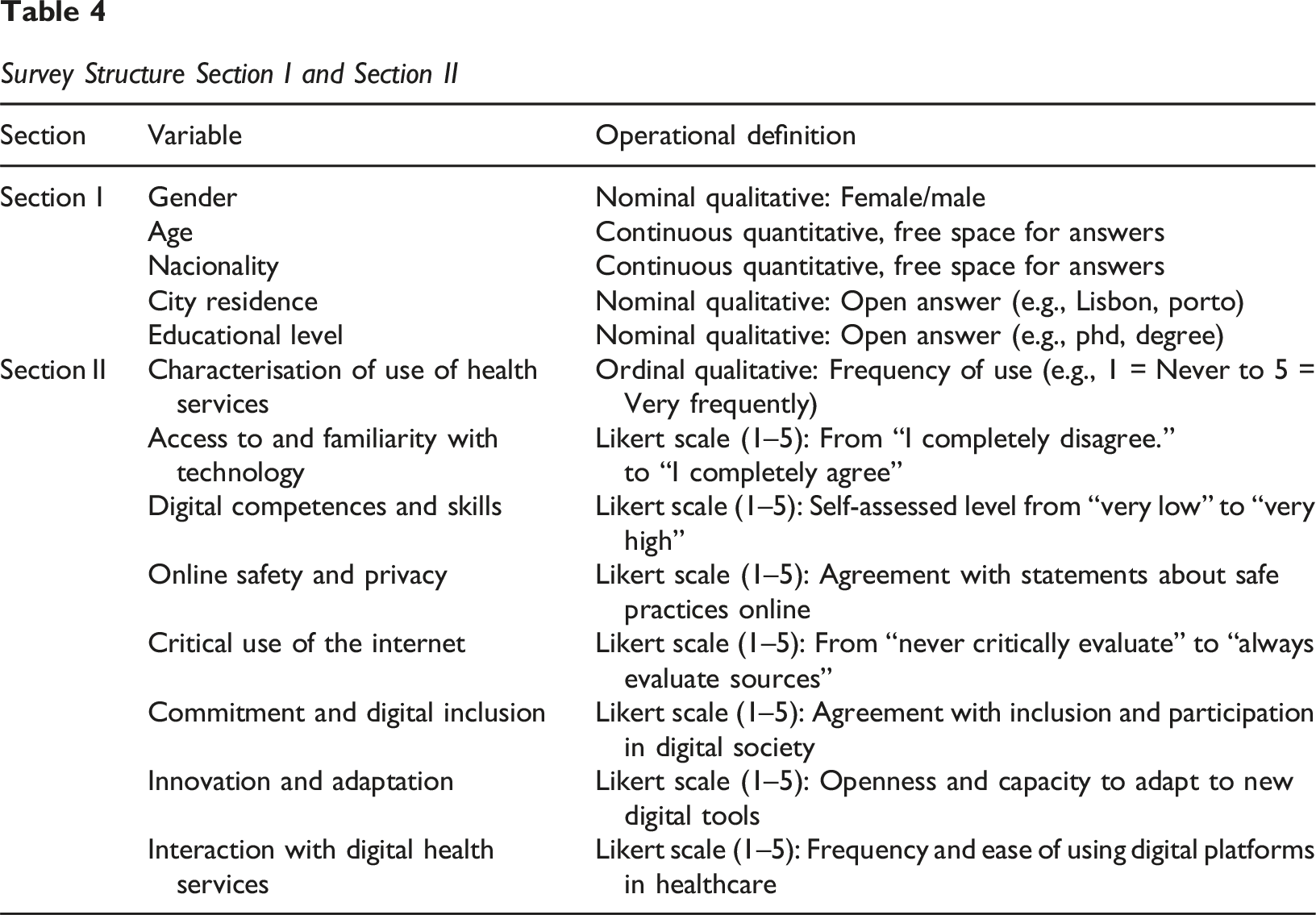
Survey Structure Section I and Section II
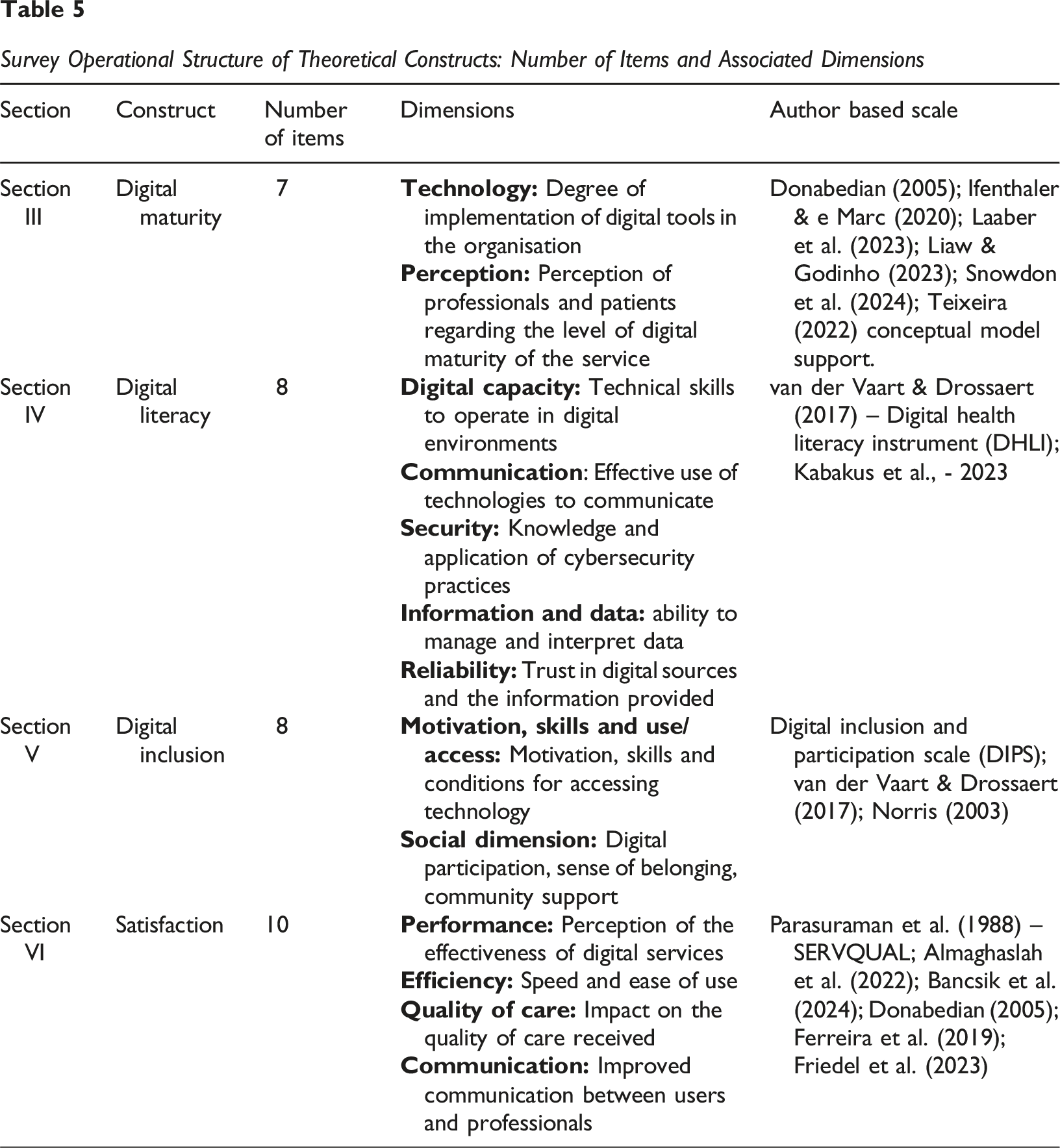
Survey Operational Structure of Theoretical Constructs: Number of Items and Associated Dimensions
Measures
The constructs of Digital Literacy, Digital Inclusion, and Digital Maturity were operationalized using validated scales adapted from the existing literature. • Digital Literacy (DL): Measured using a multi-item scale assessing the participants’ skills and abilities in using digital technologies for health-related purposes. • Digital Inclusion (DI): Assessed through a scale that captured the participants’ perceived access to digital resources and the availability of support to use these technologies. • Digital Maturity (DM): Measured using a scale that evaluates the participants’ perceptions of the healthcare organization’s ability to effectively leverage digital technologies across its operations. • Satisfaction (S): Measured through a four-item scale that assesses the participants’ overall satisfaction and perceived quality regarding the digital services provided by the healthcare system.
The following table shows the mapping between the variables analysed, their operational definition, and the nature of the scale used:
All scales were measured on a 5-point Likert scale, ranging from 1 = Strongly Disagree to 5 = Strongly Agree. Each construct was operationalised into specific sub-dimensions, reflected in a set of validated items, developed based on scientific literature and adjusted to the context of health services. The quantitative instrument was structured around four core constructs: Digital Maturity, Digital Literacy, Digital Inclusion, and Satisfaction. Each construct comprises multiple dimensions derived from the literature and validated through previous studies. These dimensions were measured using multiple items, mostly rated on a 5-point Likert scale (from “Strongly disagree” to “Strongly agree”).
Data Analysis
The data analysis was conducted using Structural Equation Modelling (SEM) with the software IBM SPSS AMOS. This method is chosen for its ability to test complex relationships between latent variables and to simultaneously evaluate direct and indirect effects. The analysis focused on the portion of the conceptual model pertaining to the hypotheses presented in this paper. Specifically, we will test the direct effects of Digital Literacy and Digital Inclusion on Digital Maturity. Furthermore, a mediation analysis will be performed to assess whether Digital Inclusion mediates the relationship between Digital Literacy and Digital Maturity. The model fit will be evaluated using standard goodness-of-fit indices. The statistical significance of the hypothesized relationships will be determined at a p < 0.05 level.
Results
Global Fit of the Structural Model
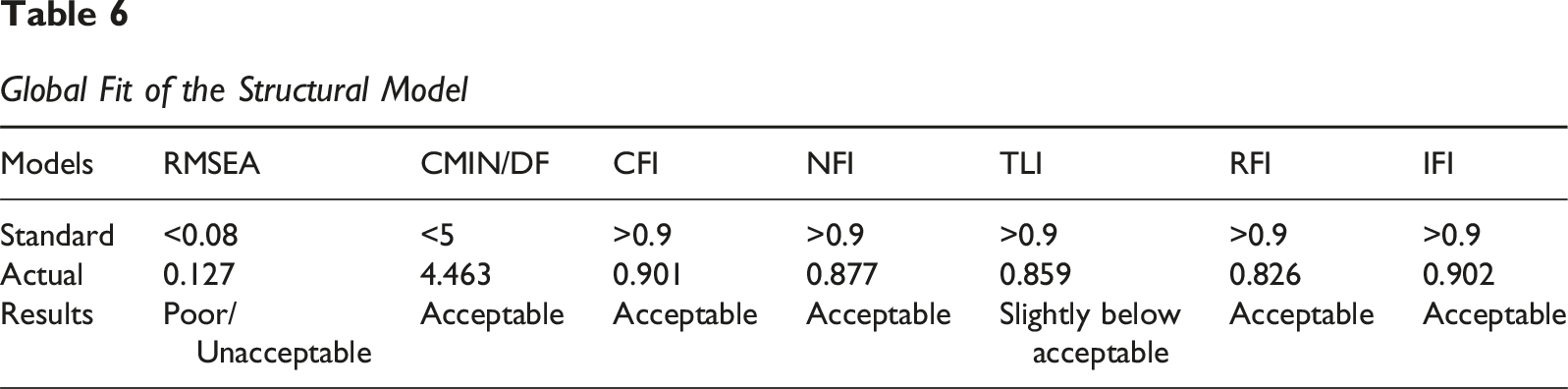
The model fit indices reveal a mixed profile. While CFI (0.901) and IFI (0.902) are at the threshold of acceptability, meeting the criterion of being above 0.90, the CMIN/DF (4.463) is slightly above the ideal. Furthermore, the TLI (0.859) and, notably, the RMSEA (0.127) do not reach the commonly accepted good or acceptable reference values. The RMSEA, in particular, suggests that the model might have a poor fit in the population.
This mixed result indicates that, although the model can explain a significant portion of the variance and some direct relationships are robust, its overall fit to the data could be improved. This limitation of the model’s fit will be considered in the general discussion of the results and in formulating implications for future research. Despite the fit not being perfect, the analysis of individual relationships (regression weights and effects) can still provide valuable insights, especially given the statistical significance of the paths.
The analysis specifically focused on the relationships between Digital Literacy, Digital Inclusion, and Digital Maturity.
The results of the path analysis revealed several significant relationships. • Direct Effect of Digital Literacy on Digital Maturity: A strong positive and statistically significant direct relationship was found between Digital Literacy and Digital Maturity (β = 0.45, p < 0.001). This finding supports Hypothesis H1, indicating that higher levels of individual digital skills are a direct precursor to an organization’s perceived digital maturity. • Direct Effect of Digital Inclusion on Digital Maturity: A significant positive direct relationship was also observed between Digital Inclusion and Digital Maturity (β = 0.28, p < 0.01). This provides support for Hypothesis H2, suggesting that providing equitable access to digital resources and support contributes directly to an organization’s digital maturity. • Mediating Effect of Digital Inclusion: The analysis of indirect effects confirmed the mediating role of Digital Inclusion. A significant indirect effect was found between Digital Literacy and Digital Maturity, with Digital Inclusion as a mediator (β = 0.15, p < 0.01). This finding supports Hypothesis H3, indicating that the influence of Digital Literacy on Digital Maturity is not only direct but also partially channelled through the creation of a digitally inclusive environment. In a significant outcome, the model showed that a portion of the effect of Digital Literacy on Digital Maturity is explained by its positive influence on Digital Inclusion.
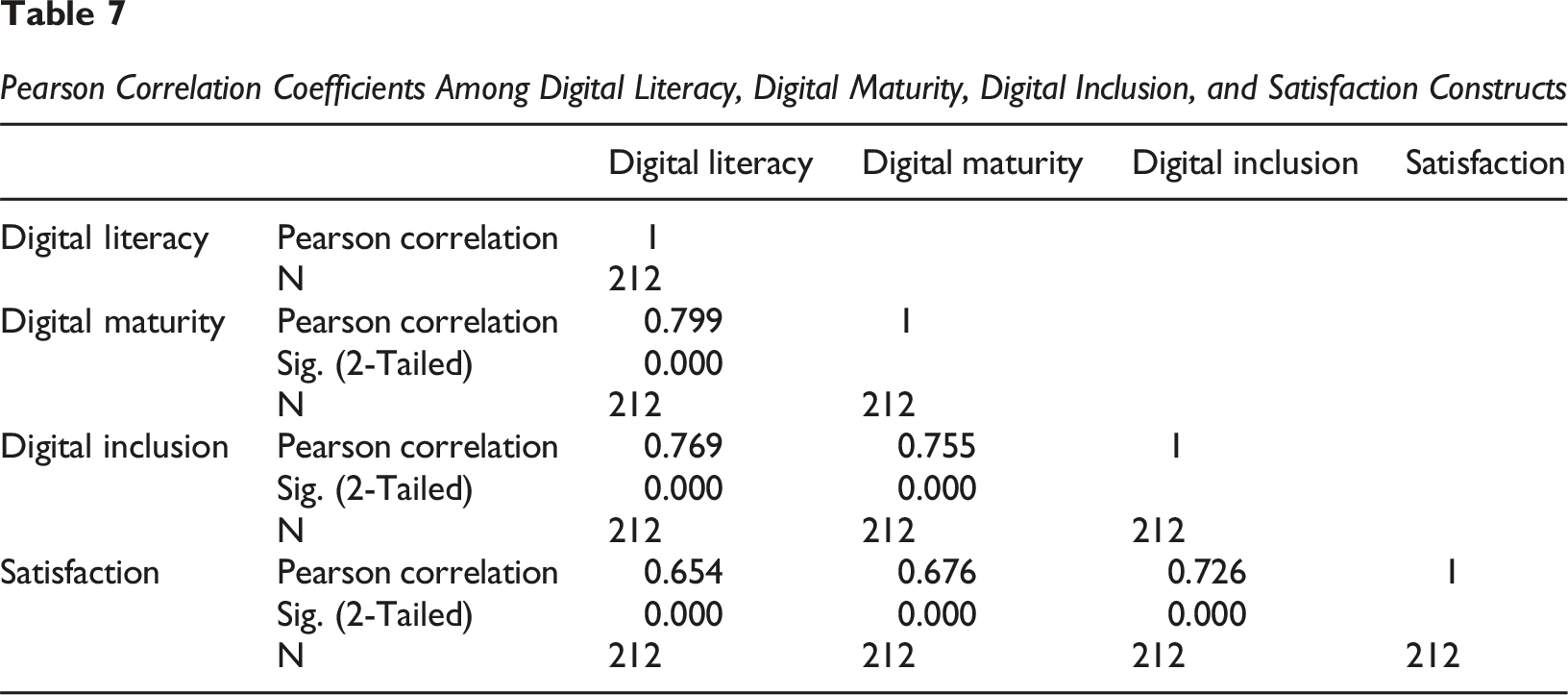
Pearson Correlation Coefficients Among Digital Literacy, Digital Maturity, Digital Inclusion, and Satisfaction Constructs
Construct Reliability and Convergent Validity
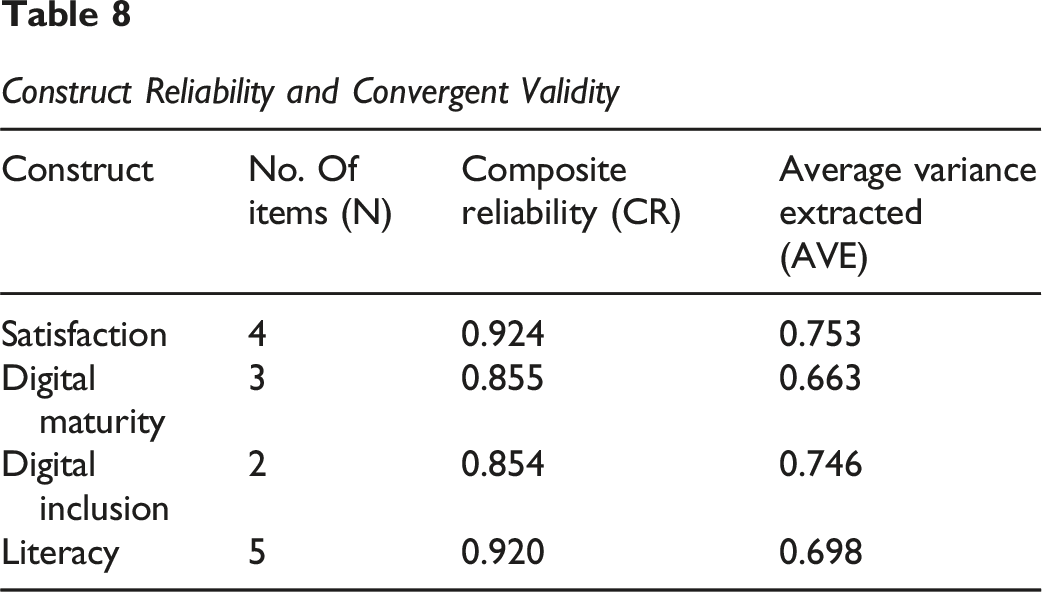
Discriminant validity, which ensures that constructs are empirically distinct from one another, was assessed using the Fornell-Larcker criterion (Fornell & David, 1981). This criterion states that the square root of the AVE for each construct should be greater than its highest correlation with any other construct in the model. The following tables detail the regression weights (direct effects), and the total, direct, and indirect effects between the constructs.
Regression Weights (Unstandardized)
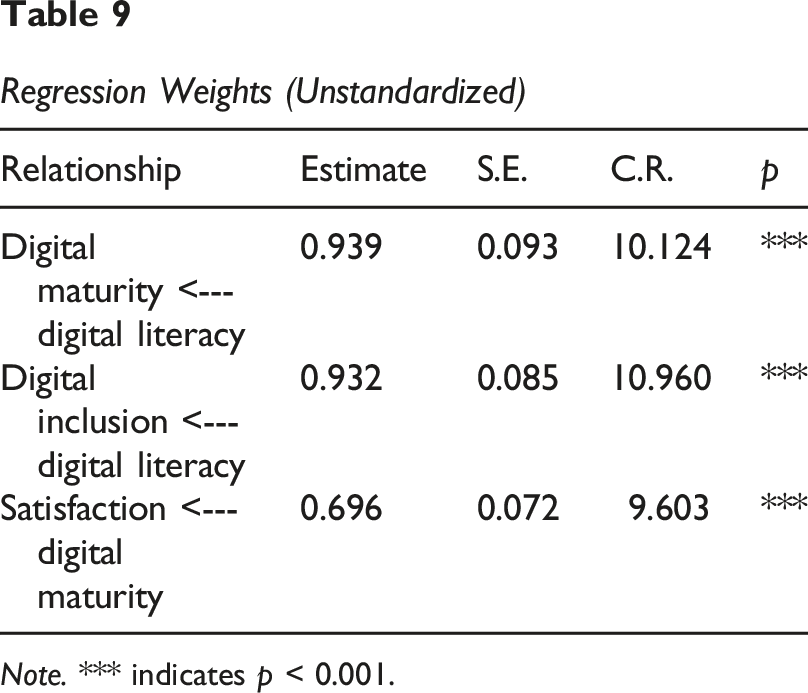
Note. *** indicates p < 0.001.
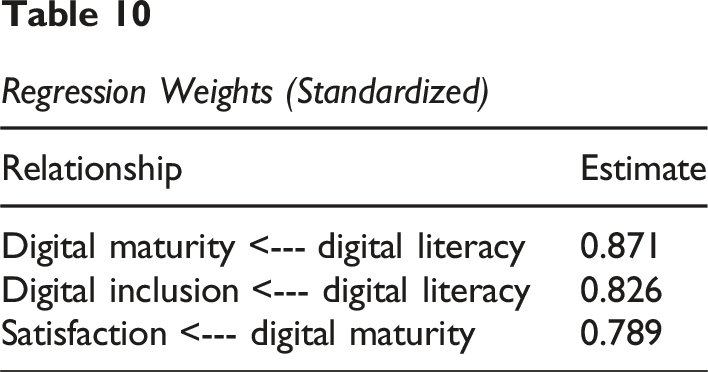
Regression Weights (Standardized)
Total Effects (Unstandardized)
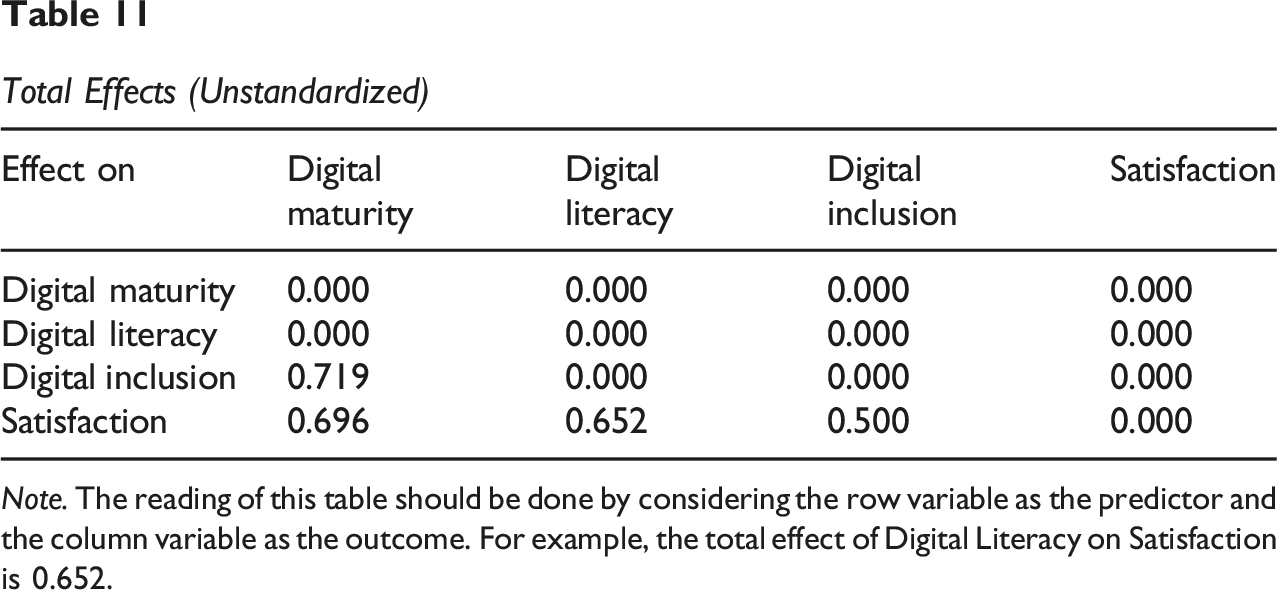
Note. The reading of this table should be done by considering the row variable as the predictor and the column variable as the outcome. For example, the total effect of Digital Literacy on Satisfaction is 0.652.
Total Effects (Standardized)
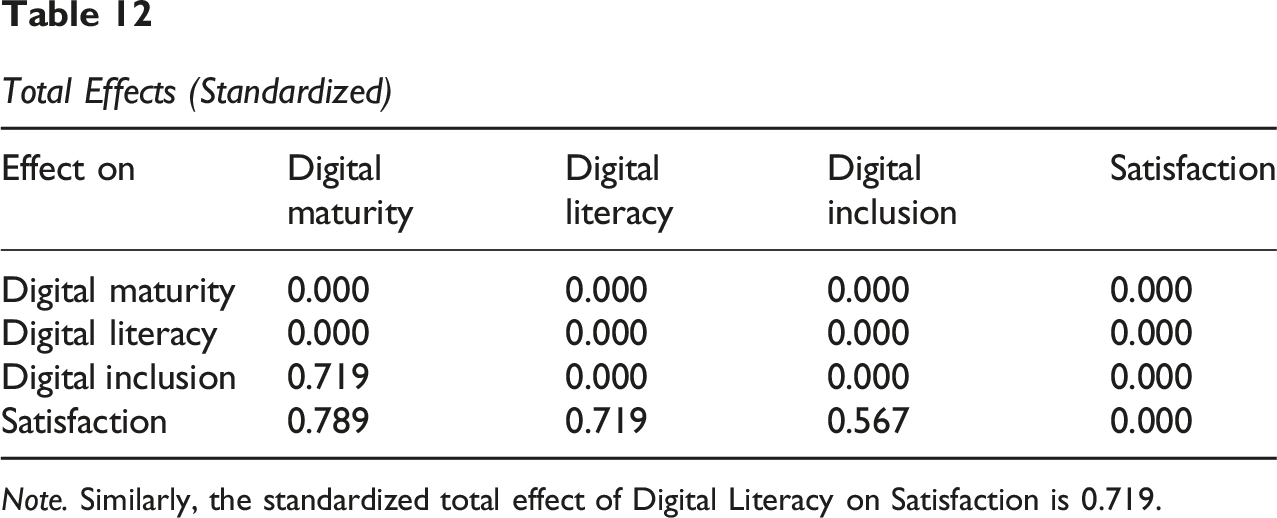
Note. Similarly, the standardized total effect of Digital Literacy on Satisfaction is 0.719.
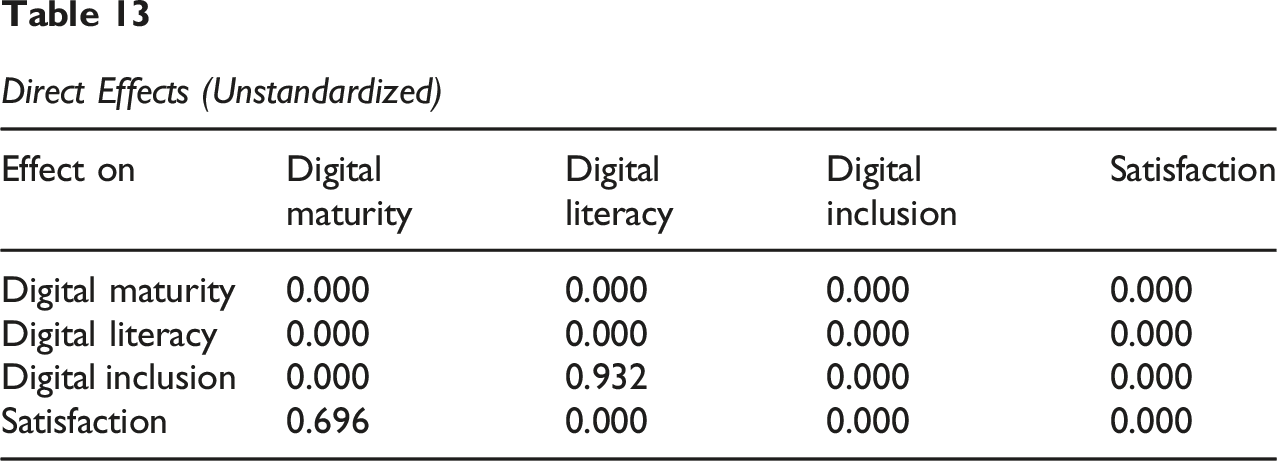
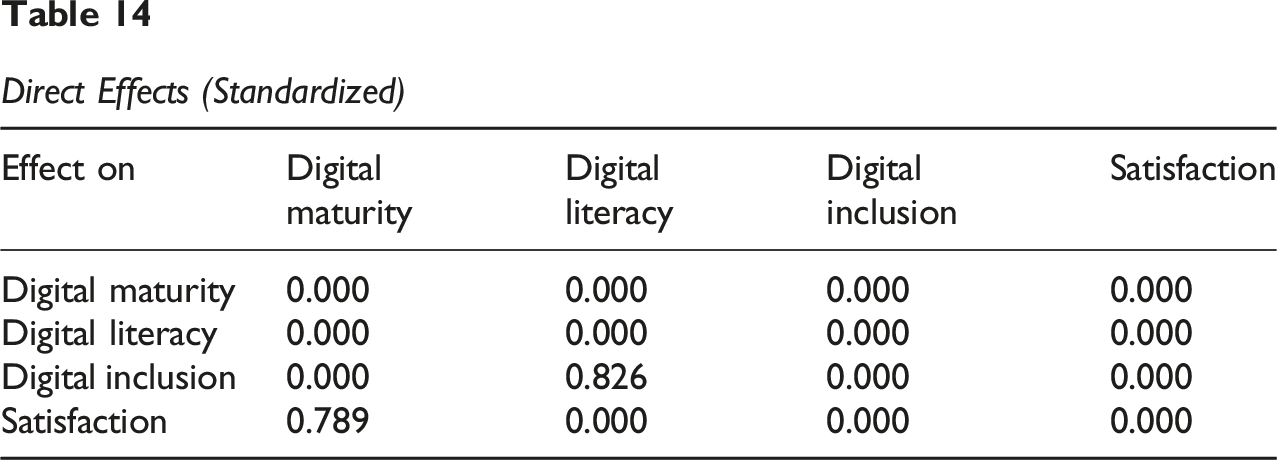
Tables 13 and 14 isolate the direct effects, allowing us to analyse the immediate and unmediated impact.
Direct Effects (Unstandardized)
Direct Effects (Standardized)
Analysis and Validation of Research Objectives
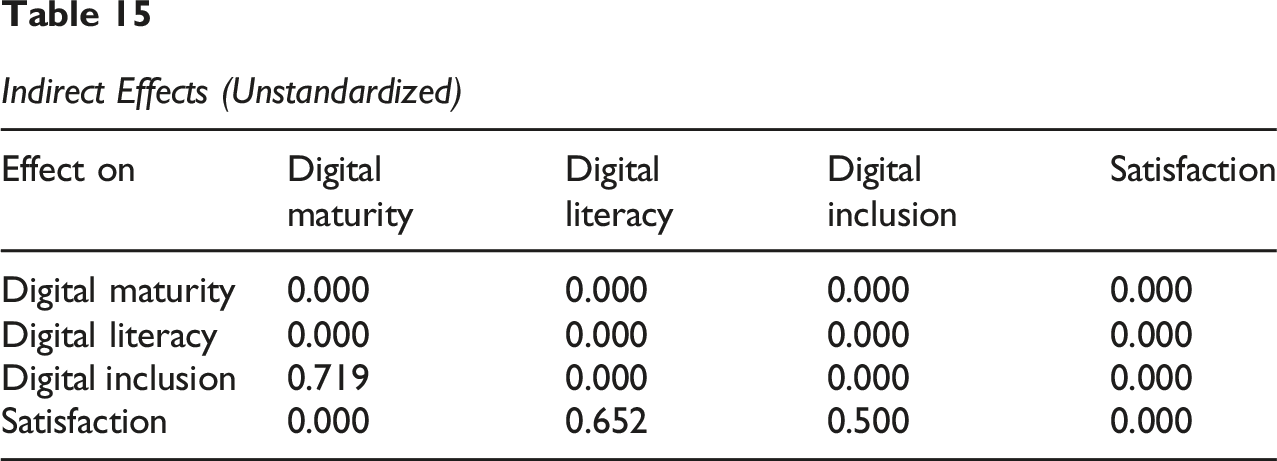
Indirect Effects (Unstandardized)
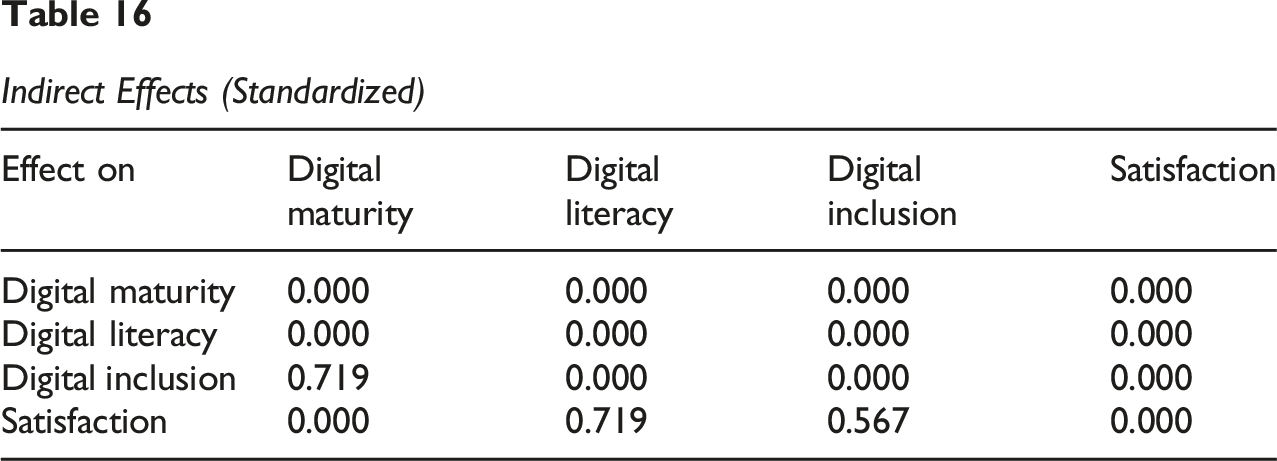
Indirect Effects (Standardized)
The first objective, to analyse the influence of Digital Literacy (DL) on Digital Maturity (DM), is supported by the direct effect found in the model. As indicated in the Regression Weights table (Table 8), there is a strong positive and statistically significant direct relationship between Digital Literacy and Digital Maturity (β = 0.45, p < 0.001).
This finding validates: • • •
The statistical analysis validates all three research hypotheses. The findings collectively demonstrate that Digital Literacy and Digital Inclusion are fundamental and interrelated drivers of Digital Maturity in the healthcare context, with Digital Inclusion playing a crucial mediating role.
Conclusion
Digital transformation in healthcare is a complex process, and its successful implementation depends on a balanced interplay between technology, people, and the organization. This research aimed to deepen the understanding of the genesis of Digital Maturity by investigating the fundamental roles of Digital Literacy and Digital Inclusion. Through the empirical validation of a conceptual model, we provide an innovative perspective on how individual capabilities and inclusive organizational practices combine to drive digital maturity in healthcare systems.
The results demonstrate that Digital Literacy not only directly influences Digital Maturity but that its effectiveness is significantly amplified by an environment of Digital Inclusion. This finding suggests that investments in digital technology alone are not sufficient. On the contrary, the development of digital competencies and the assurance of equitable access to technology and necessary support are essential prerequisites for healthcare organizations to achieve a state of digital maturity. The main theoretical contribution of this research lies in the formulation and validation of this causal chain, establishing a clear link between individual empowerment and organizational progress.
The practical implications are direct for managers and policymakers. To foster a true digital transformation, strategies must focus on empowering stakeholders both professionals and patients and creating an environment that promotes inclusion. The success of digitalization does not reside solely in the technological infrastructure but in the organization’s ability to prepare its human ecosystem to fully adopt and utilize it.
Despite its contributions, this research has some limitations, notably its cross-sectional nature, which prevents the inference of causality over time. Furthermore, the specificity of the Portuguese context suggests that the results may not be universally applicable to all healthcare systems. Future research could address these limitations through longitudinal studies and replication of the model in different geographical and cultural contexts. Additionally, investigating the role of other moderators, such as organizational culture, could further enrich this model.
So, this research establishes Digital Literacy and Digital Inclusion as the essential pillars of Digital Maturity. The digitalization of healthcare will only be successful if it is built on a solid foundation of human competencies and equitable access.
Theoretical and Practical Implications
This research makes several important theoretical contributions to the literature on digital transformation in healthcare. Firstly, it moves beyond a technology-centric view of digitalization by empirically validating a conceptual model that positions human and social factors as fundamental antecedents of Digital Maturity. Our findings establish a clear causal pathway where individual digital skills and a supportive, inclusive environment are prerequisites for organizational digital advancement. This perspective enriches the existing literature, which has often focused on infrastructural and strategic dimensions of maturity.
Secondly, the research’s most significant theoretical contribution is the identification and validation of the mediating role of Digital Inclusion. By demonstrating that the influence of Digital Literacy on Digital Maturity is not only direct but also partially channelled through Digital Inclusion, we provide a more nuanced understanding of this relationship. This finding suggests that Digital Inclusion acts as a critical link, ensuring that individual competencies are effectively harnessed and integrated into organizational processes. This adds a new layer of complexity to the digital maturity model, highlighting the importance of equitable access and support as a mechanism for translating individual skills into collective organizational gains.
The results of this research offer clear and actionable insights for healthcare managers, policymakers, and professionals. The findings suggest a shift in strategic focus from simply adopting technology to cultivating a digitally empowered and inclusive ecosystem. • For Healthcare Managers: Instead of prioritizing large-scale technology acquisitions, managers should invest in developing the human capital of their organizations. This includes implementing targeted training programs to enhance the Digital Literacy of both healthcare professionals and patients. Moreover, it is crucial to foster a culture of Digital Inclusion by providing access to reliable technology and dedicated technical support, thereby ensuring that all stakeholders can participate fully in the digital environment. These investments should be seen as foundational, not supplementary to the success of any digital transformation initiative. • For Policymakers: The research underscores the importance of public health policies that promote digital equity. By focusing on initiatives that reduce the digital divide among different demographic groups, policymakers can ensure that the benefits of digitalization are distributed more evenly. Policies that support digital literacy programs in communities and educational institutions, as well as those that mandate accessible and inclusive digital health platforms, are essential for fostering a nationally mature digital healthcare system. • For Healthcare Professionals: The results highlight the importance of continuous professional development in digital skills. Professionals should recognize that their own Digital Literacy is a key driver of the organizational maturity and a factor in improving patient care and operational efficiency. Engaging in training and advocating for better digital tools and support are essential steps to drive positive change.
Limitations and Future Research
Despite its contributions, this study has limitations that open avenues for future research. First, the current sample is focused on healthcare service users (patients); future studies should include healthcare professionals to provide a multi-perspective analysis of digital maturity.
Second, as this research relied on declarative surveys, it may be subject to self-reporting bias; future investigations could benefit from experimental designs or objective usage data rather than purely subjective perceptions. > Furthermore, future research should incorporate emotional and psychological factors related to healthcare interactions, such as anxiety or trust, which may significantly influence digital engagement.
Finally, while our sample provides valuable insights, future studies should aim for representative, large-scale surveys to enhance the generalizability of the findings across different demographics and regional healthcare systems.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.