
Abstract
Accessing information through eHealth technologies is typically suggested to be empowering. This study challenges this idea and explores individuals’ perceptions of patient portals and how the variation in these perceptions can be explained in terms of different orders of empowerment. The study extends conceptual understanding of (dis)empowerment as an outcome of patient portal use. It takes an information perspective and draws from an analysis of data from a population-level survey study of older adults (55–70 years) in Finland (N = 251). The questionnaire included questions on health information seeking and management, health behaviour as well as the use and views of current and future eHealth technologies available through patient portals. The data was analysed using exploratory factor analysis. The findings show how individuals can get empowered and disempowered in multiple ways by eHealth technologies. Four forms or orders of (dis)empowerment were identified: disempowerment, knowledge empowerment, emotional empowerment, and information and communication empowerment. Rather than assuming that empowerment is a monolithic outcome of technology use, this study underlines the importance of acknowledging the presence of different orders of (dis)empowerment as means to the diverse ends that individuals have in their lives.
Keywords
1. Introduction
eHealth technologies, that is, digital healthcare technologies such as health information exchange platforms, are commonly expected to empower individuals, typically referred to as patient empowerment [1,2], by improving access to services, informing people, and supporting them in taking an active stance in their own healthcare [3]. Consequently, this is expected to lead to positive health care outcomes [4]. The positive impact of increased empowerment of individuals on both individual and healthcare system level has been highlighted especially among older adults (51–66 years old) – in comparison with the elderly (>66 years) and younger (<51 years) individuals – who are living in a stage of life where healthcare needs often increase [5].
Patient empowerment lacks a concise definition [6,7], but it is typically viewed to be both about individuals taking control or responsibility over their own health, illness, and care [8], and their ability to participate in the consultation and decision-making process [9]. eHealth technologies that enable access to personal health information have been expected to not only have a positive impact on individuals’ ability to effectively manage and make informed decisions on their health and illness, but even to be a prerequisite for it [1,2,10].
The literature acknowledges the multifaceted nature of the concept of patient empowerment; individuals can be empowered and disempowered in multiple ways. For example, distinctions have been made between individual and collective empowerment [11], isolated and ‘complete’ patient empowerment [12], individualistic, instrumental, democratic, and emancipatory patient empowerment [13], and discretionary, psychological, and leadership empowerment [14]. Moreover, empowerment literature outside of the health domain points to other, more specific, mundane, and situational forms of empowerment and their underlying facets [15–17].
Against this background, by acknowledging empowerment as a multifaceted rather than a monolithic concept, we explore variations in people’s perceptions of eHealth technologies and the outcomes of their use and how those perceptions can be explained in terms of different forms of empowerment. Considering the earlier empirical research pointing to links between empowerment and perceived usefulness of systems and services [18,19], we find it plausible to hypothesise that the diverse perceptions people have on the outcomes of the use of eHealth and technologies in a broader sense can be conceptualised in terms of and are indicative of different orders of (dis)empowerment of individuals.
The aim of this study is to provide new knowledge on the ways older adults’ aged 55 to 70 perceptions of the usefulness of technologies, with a particular focus on eHealth and patient portals, can be conceptualised in terms of their varying experiences of how the technologies are empowering and disempowering. The research questions addressed are:
While the research questions address empowerment in general, we specifically focus on the ways information and people’s interaction with it are connected to the experiences of being empowered. On the basis of extensive earlier research in the field of (health) information behaviour research [3,20–22], meaningful differences in this respect include the tendencies of active or passive information seeking, varying levels of health information literacy, and beliefs of having control over one’s own health (i.e. locus of control). The studied age group 55 to 70 years is termed older adults (as e.g. in [5,23]) contrasting to younger individuals and elderly acknowledging the lack of established terminology and multiple categorisations, some with slightly different intervals and others using the term of everyone older than middle-aged (see e.g. [24–26]).
The study is based on the analysis of data collected in a nation-wide self-reported postal survey (N = 251) in Finland, targeted to older adults aged 55 to 70. The study does not seek generalisation but is exploratory in nature.
2. Literature review
2.1. Older adults as users of digital health services
Earlier research points to individuals having largely positive views of patient-centred eHealth technologies, as well as their anticipated and experienced usefulness [20,27]. However, unsurprisingly, not all users share the positive views [28]. In previous research, differences in the interest in and use of eHealth has been found between people based on health condition [29], experiences of eHealth use [30], self-efficacy [28], and age [31].
This study focuses on older adults, who, as a group, have been identified as a key target group for promoting eHealth use [32]. Especially the period of younger old adulthood, in many countries close to the typical retirement age, stands out as a transitory period in people’s relationship to their health and healthcare ([5], also e.g. technology use during the same period [33]). Older adults are frequently singled out as a group with a potential to benefit from digital health services [34]. In parallel, older age has been associated with perceptions of barriers to technology use and readiness to use eHealth [35], and less actual use of patient portals and eHealth in general [36,37] as well as not managing personal health information online [38].
Studies have examined the reasons for eHealth use and non-use among older adults in connection to perceptions of usefulness, user support, and especially usability [20]. A systematic review of factors related to electronic personal health records use by Abd-alrazaq et al. [29] showed the influence of personal and socioeconomic factors, perceived usefulness and ease of use, and the organisational factor of facilitating conditions on eHealth use. Moreover, Wilson et al.’s [28] literature review on why older adults engage with eHealth found that intrinsic individual barriers to use eHealth were often related to physical ageing and loss of cognitive or motoric abilities (cf. [39]) as well as self-efficacy related to technology use (cf. [40]), whereas facilitators included willingness to learn or being motivated to change one’s lifestyle. Extrinsic barriers related either to a lack of experience or awareness of eHealth or negative experiences of such technologies (cf. [39]), as well as perceptions of excessive efforts to learn how to use them. Facilitators, instead, covered perceptions of benefits of use, of independence and self-management of care, and positive previous experiences (cf. [28,41]). Experienced difficulties with using technology and lack of technology skills [31,39] are barriers to use eHealth. The ICT use in general can, on the other hand, be linked to eHealth technology acceptance [35].
2.2. Empowering eHealth technologies?
eHealth technologies are often viewed to promote patient empowerment by facilitating individuals’ control and providing tools for self-management [1,2,10], which can support the shift away from the ‘paternalistic’ model of healthcare, where experts makes decisions on behalf of individuals, towards a patient-centred approach [42]. Online access to personal health records, in particular, has been suggested to empower patients [43]. Reportedly, access to personal health records and information exchange between patients and medical professionals can result in increased patient involvement in their own care [44] and self-management [45], better attendance to self-care and informed decision-making, and improved trust between patients and medical professionals [46].
However, evidence of eHealth’s impact on patient empowerment, engagement, and activation remains inconclusive [2], partly due to varied definitions and the multifaceted nature of empowerment also reflected in the different operationalisations of the concept [16,47,48]. Patient empowerment can be viewed both as a personal disposition, referring to individuals’ taking control over their health or illness, and as a relational concept, referring to the patient–professional relationship [49] and the possibilities of the individuals to participate [10]. Moreover, it is possible to deduce from the literature [50] that empowerment can be understood either as a process or as an outcome.
Zimmerman [51] viewed different levels of empowerment (individual, community-level, organisational) as interlinked. At the individual level, he used the concept of psychological empowerment to refer to ‘perceptions of personal control, a proactive approach to life, and a critical understanding of the sociopolitical environment’ (p. 581) and viewed it to both influence and be influenced by other levels of empowerment. However, Zimmerman [51] noted further that measuring psychological empowerment can be difficult as it can change over time and its manifestations and underpinnings might vary across individuals and settings. A focus on individual level empowerment should neither lead to overlooking social or contextual factors. In empirical research, individuals’ beliefs that they have control over their own health (internal locus of control [52]) and their beliefs in their own abilities (self-efficacy [53]) have been associated with empowerment at an individual level [54]. At a relational level, a collaborative and negotiated relationship between the patient and a healthcare professional, for example, is shown to foster empowerment [55].
Castro et al. [11] distinguished four key antecedents for patient empowerment in the literature: a dialogue between health care providers and patients; a patient-centred approach; enhancement of individuals’ competences (necessary knowledge, skills, and attitudes); and active participation. However, Petrič et al. [56] noted that patient empowerment does not necessarily lead to better outcomes from the perspective of the patient–professional relationship or differentiate between functional and dysfunctional empowerment, which can manifest in the different empowerment dimensions.
Critics argue that assumptions underlying patient empowerment – including the ideas that all individuals want to and benefit of choice and control, that health care providers support patients’ efforts to gain control, that providing information to patients ‘empowers’ them, and that ‘informed’ and ‘empowered’ patients take better care of their health – are unsubstantiated [48]. Moreover, according to Fumagalli et al. [57] there is confusion between patient empowerment and related concepts such as patient engagement and patient participation. They view the relationships of these concepts as a process where engagement and enablement can lead to empowerment which, in turn, can lead to participation and involvement [57].
In this study, we ask in what ways eHealth technologies can be empowering or disempowering from the patients’ perspective. This question directs focus on different ways people may experience the empowering potential of such technologies. Moreover, instead of trying to understand empowerment in a broad sense, we focus on the ways increased access to health information, enabled by eHealth, may be experienced as (dis)empowering.
To approach empowerment from this perspective, we have consulted empowerment literature beyond the health domain with a more nuanced understanding of forms of empowerment and their underlying facets, especially in connection to information [15–17]. In the management field, Wilkinson [17] distinguished five forms of empowerment: (1) information sharing referring to horizontal communication between people at lower and higher levels in hierarchy; (2) upward problem-solving suggesting that individuals on the lower levels of hierarchy are tasked on suggesting improvements and solve problems; (3) task autonomy referring to having autonomy in performing tasks; (4) attitudinal shaping suggesting empowerment as a psychological process of feeling empowered; and (5) self-management which, ideally, would involve eroding divisions between people in different positions and making decisions together. An interesting aspect of Wilkinson’s [17] categories is that they highlight the role of information in empowerment. Moreover, he points out that not only ‘varying types of empowerment carry different meanings, but also techniques with the same name, structure and processes may be experienced in very different fashions’ (p. 50).
An understanding of empowerment as a multifaceted concept, also connected to people’s interaction with health information, may help in understanding the standpoint of the users of eHealth technologies from their point of view, instead of that of healthcare.
2.3. Role of information interactions in patient empowerment
We view information and people’s interaction with it as central in their feelings and experiences of being empowered. Even though the common premise of developing eHealth technologies is to support patient empowerment through providing access to health information, people’s propensity to approach and utilise health information varies, and therefore, also the outcomes differ.
People seek and use health information for diverse reasons, including to increase awareness, to make sense of a situation or health-related decisions, and to cope with serious illness [22]. An eHealth service is only one among (the) many information resources people can use to manage their health and wellbeing and make informed health-related decisions. Reviews on health information seeking suggest empowerment-related outcomes of interacting with health information, including enhanced ability to engage in shared decision-making regarding medical treatments, increase in self-efficacy and self-care, or increased ability to maintain independence [21,58]. Empirical research indicates that active health information seeking is linked to patient adherence [59], health promoting behaviours, and better self-reported health [60].
Individuals may also avoid information, that is, to prevent or delay ‘the acquisition of available but potentially unwanted information’ [61]. According to Sweeny et al. [61] people may avoid information when anticipating that receiving information would (1) necessitate an undesired action such as behaviour change or (2) result in negative emotions. In crises, negative emotions such as increased stress or fear, or increased frustration or confusion might lead to avoidance [62,63]. Furthermore, a person might feel overexposed by a topic if habitual activities are interfered [64], if the information does not suit one’s needs [63], or if information is anticipated to create dissonance [65]. In other words, information sometimes rather increases than reduces anxiety [66]. Therefore, people may not want to be exposed to some types of information independent of their beneficiality or usability ‘due to issues related to coping with oneself and one’s psychosocial and sociocultural environment’ [67]. Moreover, external locus of control – believing you cannot control your own health – has been linked to increased information avoidance behaviour [68].
Information seeking behaviours are associated with both personal competences, also known as (health information) literacies, internal beliefs in one’s abilities such as locus of control [69, cf. 70], and the empowerment level and form of individuals (e.g. [7,71]). The findings are not consistent, however, as the health empowerment model claims that health literacy and empowerment do not correlate, although they determine certain health outcomes together [54], whereas Papp-Zipernovsky et al. [70] contradicted this assumption by showing a correlation.
Health information literacy (HIL) refers to abilities to recognise a need for health information, to know how and where to find information about health, and how to evaluate and use this information in everyday life to make good health decisions [72]. Related concepts include eHealth literacy [73] and digital health literacy [74]. A systematic review shows that eHealth literacy better predicts the willingness to adopt a computerised personal health record than socioeconomic variables do [75]. In addition, significant moderate correlations were found between eHealth literacy scores and empowerment in a Hungarian population [70], whereas Schulz et al. [71] found that higher levels of eHealth literacy increased online health information seeking, which led to increased empowerment especially in the oldest studied group of baby boomers. In Jiang et al. [7], those with high health literacy level demanded more health empowerment as per perceived benefits, both informational (being more informed by seeking information) and concerning decision-making (increased knowledge and skills gained by seeking information).
3. Methods and materials
3.1. Data and instrument
3.1.1. Target population and data collection
The study is based on the analysis of data collected in a nation-wide postal survey in Finland, targeted at older adults aged 55 to 70 representing the earlier identified transitory group [5] in younger older adulthood. A postal survey was mailed in 2019 to a population of 1500 individuals aged 55 to 70, drawn using random sampling from the national Population Information System of Finland. The sampling criteria were that the participants should be aged 55 to 70 by the end of 2018, have a permanent address in Finland, and be registered as speakers of the national languages, Finnish or Swedish.
3.1.2. Sample characteristics
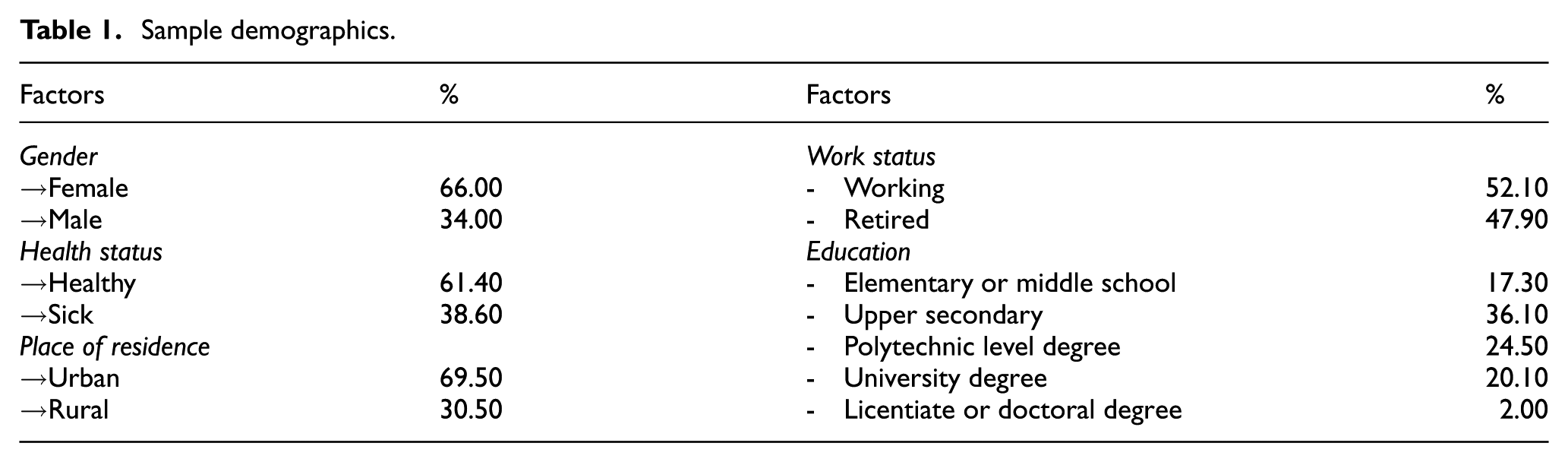
A total of 251 usable responses were received out of 1500 surveys distributed, yielding a response rate of 16.7%. Although this response rate is relatively low, it is considered acceptable given that substantial non-response is typically observed in postal surveys of the general population [76]. The average age of the respondents was 63.2 years. The majority of the respondents were female (66%) and most considered themselves healthy (61.40%). Approximately 30% of the respondents lived in rural areas and 70% in urban areas. One-half were still in some form of employment (52.10%) and none had no education at all. Overall, the sample is largely representative of the Finnish population in terms of educational level and rural–urban distribution. However, the gender distribution is skewed. Women are overrepresented in the sample, whereas national demographic figures show that men and women each constitute approximately 50% of the Finnish population. A detailed demographic overview is provided in Table 1.
Sample demographics.
3.1.3. Variables and their measurement
The questionnaire included questions on health information management, use and views of current and future eHealth technologies available through patient portals, health information seeking and health behaviour. The present study focuses on analysing questions concerning the perceived usefulness of eHealth technologies and their different features (Appendix 1), and a series of information-related contextual factors, including health information seeking and non-seeking measured on a 5-point Likert-type-like scale, information technology use, everyday health information literacy, and health-related locus of control. The selection of these factors was informed by previous literature indicating their potential association with perceptions of the usefulness of eHealth and the possible role of information in empowerment [60,77–79].
The measures were partly adapted from earlier surveys. (Dis)empowerment was explored using an inventory of 18 statements designed to probe conceptually distinct facets of empowerment identified in the literature [11,17,57] and aimed to explore different aspects of empowerment. Drawing on Wilkinson’s [17] forms of empowerment, particularly information sharing, attitudinal shaping, and self-management, as well as the distinction between empowerment as a personal disposition and as a relational concept [49], the items were developed to capture a range of conceptual domains, including concerns about the quality and consequences of eHealth information, emotional and psychological responses to eHealth use, knowledge and decision-making related aspects of engaging with health information and the communicative dimension of interacting with healthcare professionals through eHealth technologies. While these conceptual starting points guided item development, no fixed factor structure was imposed a priori. Rather, exploratory factor analysis was used to allow the empirical structure to emerge from the data.
We adapted an everyday health information literacy (EHIL) scale meant to reflect people’s confidence in their abilities in relation to health information. A modified instrument was developed on the basis of the three-factor EHIL model [80] to indicate Access (ability to understand health terminology, recognise authoritative sources, and deal with conflicting information), Assessment (ability to assess the reliability of health information in print and online, and to determine whether it is accurate), and Awareness (recognition of the importance of health information, interest in applying it and acquiring it from multiple sources). Internal and external loci of control were measured using 7-item scales adapted from Ross et al. [81]. Perception of the patient-portal-like eHealth technologies was measured using a 6-item scale developed following Sun and Belkin [82]. Respondents were also asked about their frequency of internet use, their confidence in using information technology, and their exposure to information technology, that is, their use of various technological devices such as computers, smart TVs, and smart watches. Although these three technology related variables could be combined into a single construct to capture overall technological capability, we opted to retain them as distinct constructs. Each represents a distinct theoretical dimension, and combining them would obscure their distinct influence on (dis)empowerment.
4. Results
Descriptive statistics of the responses to the questions relating to the implications of using eHealth technologies and the contextual factors are reported in Table 2.
Contextual factors.
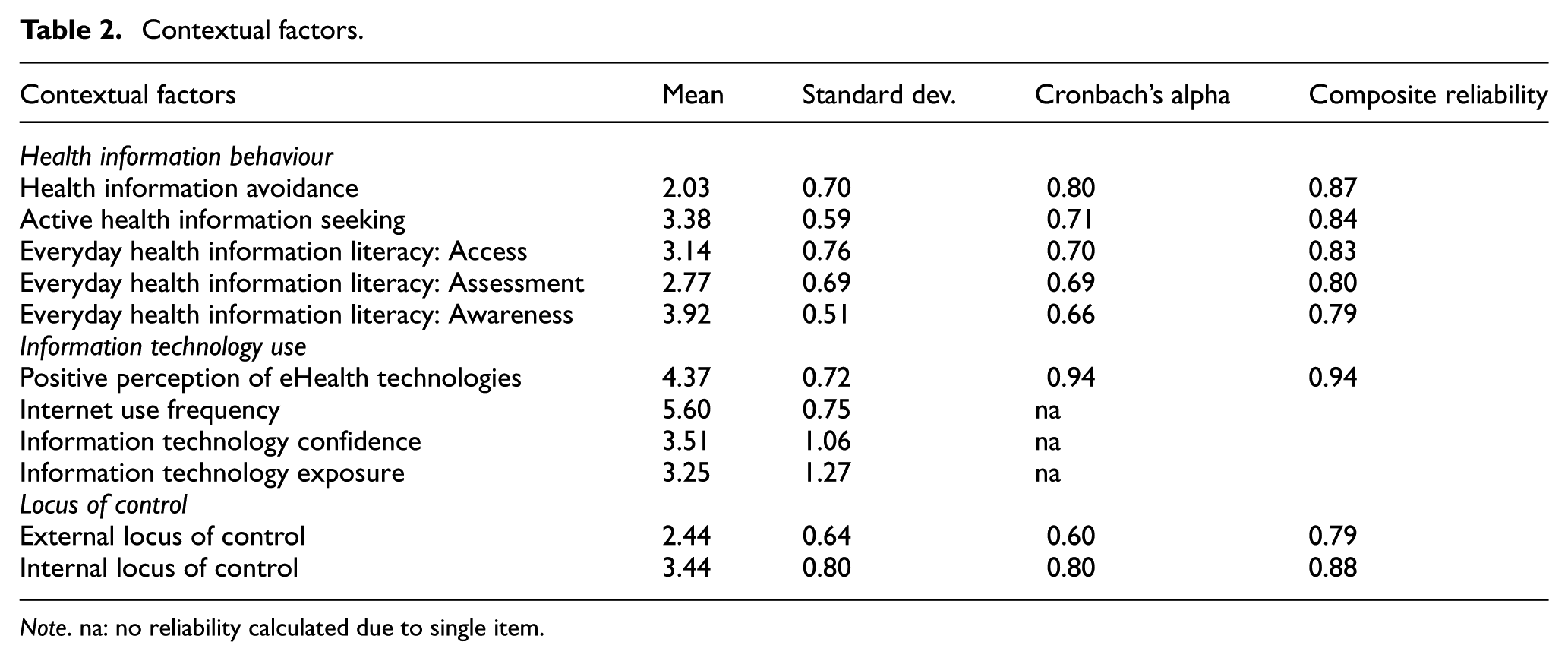
Note. na: no reliability calculated due to single item.
4.1. Factor analysis results
An exploratory factor analysis using principal components analysis was conducted in SPSS 28.0 on the individual items indicating the respondents’ views of eHealth technologies they had used to explore how the respondents had experienced these as (dis)empowering.
The suitability of the data for factor analysis (FA) was assessed using the Bartlett’s test of sphericity and the Kaiser–Meyer–Olkin (KMO) measure of sampling adequacy. The KMO value of 0.88, the significance of Bartlett’s test, and a subject to item ratio greater than 5:1 [83,84] indicate that the data meet the requirements for factor analysis.
Determining the number of factors to retain is usually based on the Kaiser criterion and Cattell’s scree plot, which is a visual representation of factors and eigenvalues [83]. Four factors were retained based on the eigenvalue of one and the inflection point in the scree plot (Figure 1). These factors were viewed to indicate views on eHealth technologies and were labelled as disempowerment (NEG), knowledge empowerment (KNO), emotional empowerment (EMO), and information and communication empowerment (INF).
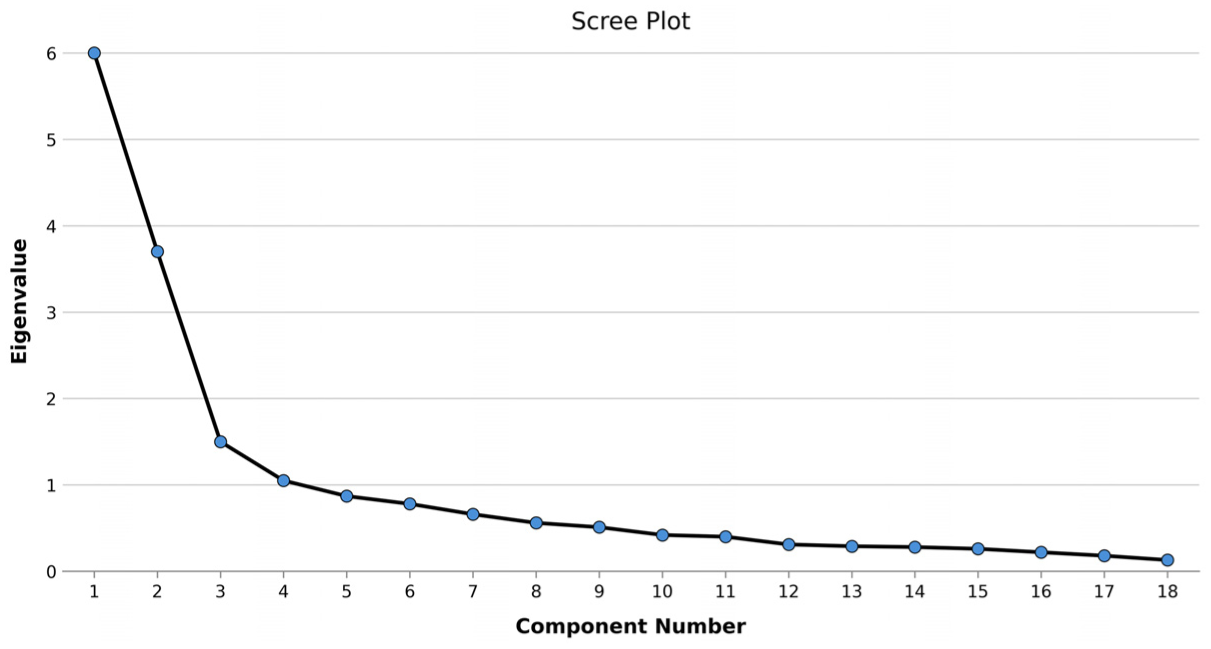
Scree plot of factor analysis.
The results of the factor analysis are presented in Table 3. Most statements have high loadings on their respective factors. The only exception is S18, which has a high cross-loading on INF and EMO. This is theoretically interpretable, as getting in contact with health professionals is simultaneously a communicative act and a source of emotional reassurance. We retain S18 within INF as it is about contacting health professionals which aligns more closely with the communicative factor than with emotional empowerment. A communality value of 0.40 is usually accepted as the minimum cut-off, with 0.70 being the ideal value. In our analysis, most of the communalities are above 0.70 and none below 0.40. Overall, we retained all statements.
Results of the factor analysis.
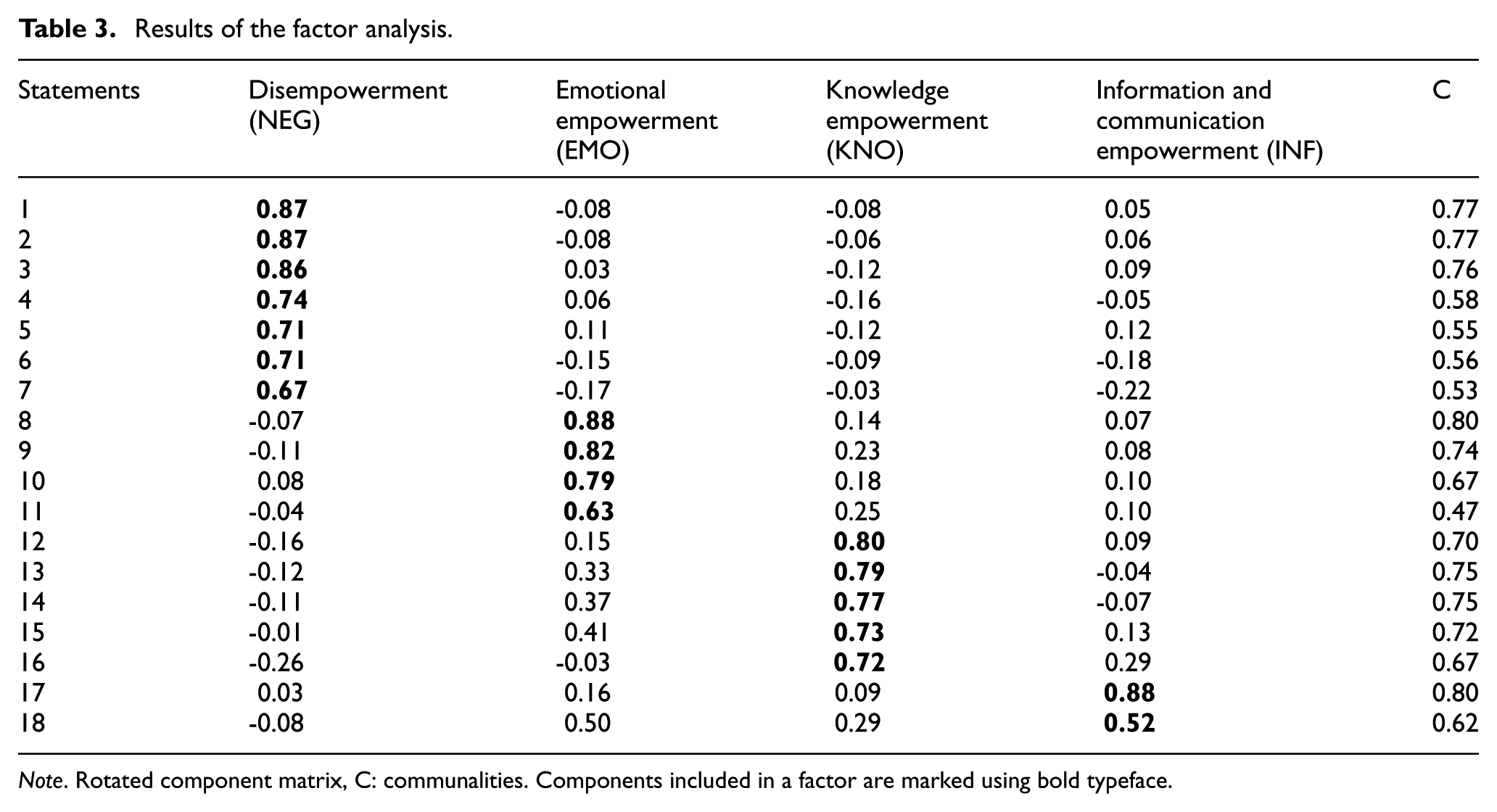
Note. Rotated component matrix, C: communalities. Components included in a factor are marked using bold typeface.
To ensure the stability of the identified four-factor structure, we performed robustness checks. First, we alternated extraction and rotation methods. A principal component analysis with Promax rotation yielded identical item assignments, confirming the structure is robust to different variance-modelling assumptions. Moreover, we conducted a sensitivity analysis by randomly excluding multiple items. The four-factor solution remained stable, indicating the constructs are not dependent on specific individual statements.
4.2. Regression analysis results
The next step was to analyse how the four forms of (dis)empowerment are related to information-related contextual factors. First, the quality of the measurement scales was assessed by examining the internal reliability of the multi-item constructs using Cronbach’s alpha and composite reliability. As shown in Table 2, three constructs had Cronbach’s alpha values below the conventional threshold of 0.70, but none fell below 0.60 which is acceptable for exploratory research [85], which is the case in this study. Nevertheless, to further ensure the reliability of the constructs, we also calculated composite reliability. All constructs demonstrated composite reliability values above the recommended threshold of 0.70.
Regression analysis was then used to assess the relationship between (dis)empowerment and the contextual variables. The results of the regression analysis are shown in Table 4. All predictors were entered simultaneously. The coefficients reported in the table are standardised beta coefficients (β), which allow comparison of the relative strength of the associations between variables.
Results of regression analysis for associations between empowerment (NEG, EMO, KNO, INF) and contextual factors.
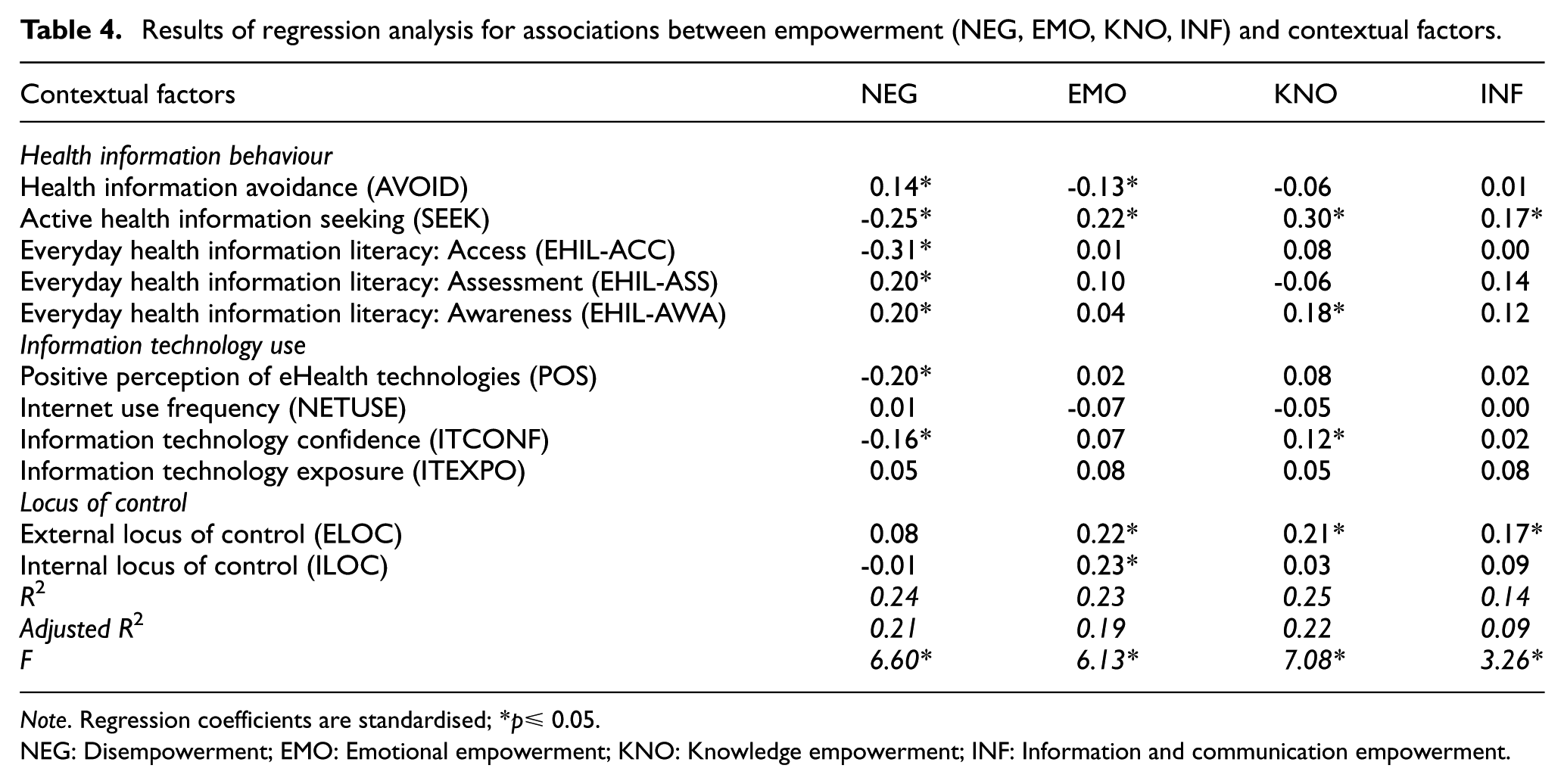
Note. Regression coefficients are standardised; *p≤ 0.05.
NEG: Disempowerment; EMO: Emotional empowerment; KNO: Knowledge empowerment; INF: Information and communication empowerment.
The four extracted factors (Table 3) represent different forms of empowerment – NEG, KNO, EMO, and INF. The first and strongest factor without major cross-loadings with other factors is NEG that represents a general negative view of eHealth technologies, their content, trustworthiness, and outcomes of use. The second factor KNO represents a view that eHealth technologies have positive implications to improving one’s own knowledge and awareness on health issues, helping to make better health-related decisions. The third factor EMO refers to emotional support, positive emotions, and expectations of behavioural change and sense of control. Finally, the fourth factor INF points to views on eHealth technologies as having potential to improve communication with healthcare professionals.
The regression analyses (see Table 4) of the four factors and contextual factors show several significant associations. The NEG was found to be associated with a lack of confidence in information technology use (ITCONF) (β = −0.16, p < 0.05), and, unsurprisingly, with negative views of eHealth technologies (POS) (β = −0.20, p < 0.05). Moreover, as can be expected, it was linked to information avoidance (AVOID) (β = 0.13, p = 0.05) and negatively associated with active health information seeking (SEEK) (β = −0.25, p < 0.05) and the perceived ability to understand health information and recognise authoritative sources (EHIL-ACC) (β = −0.31, p < 0.05). Yet, interestingly, it was positively associated with appreciating health information and one’s own competence to assess it (EHIL-AWA; EHIL-ASS) (β = 0.20, p < 0.05, β = 0.20, p < 0.05).
According to the results, experiencing KNO in using eHealth was associated with high information technology confidence (ITCONF) (β = 0.12, p = 0.05), relying on health professionals’ help to stay healthy (ELOC) (β = 0.21, p < 0.05), being active in health information seeking (SEEK) (β = 0.30, p < 0.05), and appreciating health information (EHIL-AWA) (β = 0.18, p < 0.05).
In contrast, EMO is more associated with having a high external (ELOC) (β = 0.22, p < 0.05) and internal (ILOC) (β = 0.23, p < 0.05) locus of control and being active in health information seeking (SEEK) (β = 0.22, p < 0.05).
Finally, INF was found to be higher among those who believed in health professionals’ help in staying healthy (ELOC) (β = 0.17, p < 0.05) and were active in health information seeking (SEEK) (β = 0.17, p < 0.05).
5. Discussion
As a whole, the results align with earlier findings of the predominantly positive experiences of eHealth technologies in patient portals among older adults aged 55 to 70; according to the participants of this study, eHealth can improve knowledge and awareness on health issues and facilitate making better health-related decisions [20], provide emotional support (as e.g. in Budrionis et al. [86] and Slev et al. [87]), positive emotions (e.g. [88]), and expectations of behavioural change [89], as well as sense of control [90], knowledge and capacity to deal with health information (as e.g. in Budrionis et al., [86] and Slev et al. [87]), and improve communication with healthcare professionals [91].
A key contribution of this study in contrast to earlier research is the identification of different forms of (dis)empowerment experienced by individuals in terms of the four identified orders: knowledge empowerment (KNO, own knowledge and awareness on health issues that help in making better health-related decisions), emotional empowerment (EMO, emotional support, positive emotions and expectations of behavioural change and sense of control), information and communication empowerment (INF, improvement of communication with healthcare professionals), and disempowerment (NEG, the negative experiences of eHealth technologies, their content, trustworthiness and outcomes of use). The findings also highlight the role of information seeking in empowerment. Active information seeking is linked to all identified forms of empowerment with eHealth, whereas the lack of it and information avoidance are associated with disempowerment. Also Schulz et al. [71] found a link between more active health information seeking and gains in empowerment.
Furthermore, prior reviews point to empowerment-related outcomes of health information behaviours, including that seeking health information contributes and functions as means to empowerment [58,21]. Similarly to older Swedes studied by Wiklund Axelson and Melander Wikman [92], in our study, most respondents were ready to use eHealth technologies and considered these to have a positive impact on their life. The findings also align with earlier findings from Finland underlining the perceived importance of accessing information and supporting self-management [93,94]. However, even if the experiences on average were positive, the presence of negative views point to the same direction as earlier studies reporting negative reactions (e.g. [86]) and the presence of positive (feeling confident about treatment decisions, being informed, and having a sense of control and connectedness) and negative (feeling scared, depressed, lonely, and anxious/stressed) emotions [36].
5.1. How can eHealth technologies be found (dis)empowering?
The first main finding of this study answering RQ1, the results of the factor analysis, provides new insights into how the experienced benefits and disadvantages cluster. We interpret the four factors derived from the factor analysis tentatively as representing three forms or orders (cf. e.g. orders of worth [95], and orders of discourse [96]) of empowerment and one of disempowerment. While drawn from statements relating to perceptions of eHealth technologies, we interpret the factors as indicative of distinct empowerment configurations rather than mere descriptive dimensions or indications of general evaluative valence. Even if the survey participants were given examples of eHealth technologies to consider, the statements were not specific to perceived usability of one specific tool only or concerning mere user satisfaction but probing into broader societal and emotional experiences.
Orders of (dis)empowerment are the forms and arrangements of how an individual can experience being empowered or disempowered in terms of (eHealth) technology use. As factors in exploratory factor analysis, these arrangements can overlap with each other. An individual can be simultaneously empowered in different ways and even empowered and disempowered at the same time. In contrast to conceptualising empowerment through its direct outcomes to, for example health, as an inclination to take control and responsibility [8], or an ability to participate in decision-making processes [9], framing empowerment according to different orders of how and in what terms a person is empowered, directs attention to what empowerment is and how it functions instead of its anticipated impacts. The tendency to focus on impact and its contexts applies to many earlier categorisations of different types of empowerment including individual and collective empowerment [11], situational and ‘complete’ patient empowerment [12], individualistic, instrumental, democratic, and emancipatory patient empowerment [13], and discretionary (i.e. discretionary authority on action), psychological (perception of self-control and motivational aspect of self-efficacy), and leadership (engaging experienced patients in intermediary and leadership roles in patient communities) empowerment [14].
Simultaneously, however, the four orders of (dis)empowerment identified in the present study show affinities with Wilkinson’s [17] empowerment categories. Information sharing (vs. downward communication) has similarities with information and communication empowerment, attitudinal shaping (empowerment as psychological process of feeling empowered) with emotional empowerment and self-management (by individuals or groups) with knowledge empowerment. The orders of informational (INF), knowledge (KNO), and emotional (EMO) empowerment also come close to the three types of support identified by Mathijssen et al. [97] about medication use that patients needed: informational, practical, and emotional. The order of disempowerment (NEG) can be described as a form of discretionary empowerment (cf. [14]), which is, however, channelled as opposite from the healthcare perspective to resist the use of eHealth technologies experienced as lacking positive implications. A major risk with the dominance of the order of disempowerment is that disempowerment can turn to a form of autonomous upward problem-solving [17]. Feeling strongly disempowered by eHealth can lead to preferring alternative information sources that provide ‘disnormative’ information [98], that is, either consciously willful disinformation or flawed misinformation [99] that goes against the best available evidence.
The strength of the disempowerment factor suggests that eHealth can be a major source of negative experiences of lacking power and influence. As suggested earlier [28, cf. 39], the negative experiences can, for their part, act as barriers to continued use of eHealth technologies. In contrast, the more moderate loadings of factor scores relating to the three positive orders of empowerment could suggest that when a person experiences empowerment, eHealth stands out as a complement, not replacement to other sources of empowerment. This can be linked to earlier findings of how previous positive experiences, in addition to perceived benefits of use, and perceptions of independence and self-management of care play a major role, as they may facilitate the continuation of engagement with eHealth technologies [28, cf. 41].
Similarly to how disempowerment can be compared with discretionary empowerment, knowledge and emotional empowerment can be framed as two parallel cognitive (KNO) and emotional (EMO) forms of – from a healthcare perspective positive, and pluralistic – participatory facets of attitudinal shaping [17], personal control, self-efficacy, and psychological empowerment (cf. [14]). Self-efficacy [28,40] together with perceptions of independence and self-management [28], in other words control, are important for engagement with eHealth. Information and communication empowerment does for its part emerge as a low-stake variant of leadership empowerment (cf. [14]) with characteristics of self-management [17], associable with individuals’ perceived ability to act in relation to health care professionals. Previous research shows that knowledge – or rather lack of it [100] – or familiarity with eHealth [101] are connected to willingness to consult such services.
5.2. Variation of the experiences of empowerment and disempowerment among older adults aged 55 to 70
As per the RQ2, the findings provide insights into the variation of experiences of empowerment and disempowerment among older adults aged 55 to 70 when using eHealth. The order of disempowerment was found to be associated with the largest number of contextual constructs tested in the study. Apart from being the most pronounced experience, it had a negative association with information technology confidence (ITCONF), positive experiences of eHealth technologies (POS), active information seeking (SEEK), and the perceived ability to understand health information and recognise authoritative sources (EHIL-ACC). Previously, self-efficacy in technology use has been related to use of eHealth [28] and positive experiences are facilitators for use [41,28]. In contrast, in this study, it was positively associated with both information avoidance (AVOID) and the awareness and assessment dimensions of everyday health information literacy (EHIL-AWA; EHIL-ASS). Schultz et al. [71] on the other hand, found that higher levels of eHealth literacy were associated with seeking health information online. This all points to the fact that disempowerment reflects a general negative experience of digital services. However, the disempowered individuals still feel that they are competent in dealing with health information, as interestingly, disempowerment is associated with all three dimensions of EHIL and unrelated to both external (ELOC) and internal (ILOC) locus of control, that is, the degree to which people believe they have control over their health. This is contradictory to previous studies showing that higher levels of eHealth literacy are connected with more empowerment [70], and suggests that disempowerment constitutes a particular form of autonomous informational (dis)empowerment unrelated to an experience of lacking control over health. In previous research, people with a higher internal locus of control have been found with a greater preference for shared decision-making and receiving more comprehensive information, in contrast to people with a more external locus of control [102,103]. Ek and Heinström [60] found that people with an internal locus of control seem to be ‘driven by a strong monitoring “need to know” ethos to obtain information themselves’; they are more interested in health information, seek it actively, and are less likely to avoid information.
The association of emotional empowerment (EMO) with both internal (ILOC) and external (ELOC) locus of control suggests that an eHealth technology can provide emotional support for both those taking responsibility for their own health (ILOC) and those relying on others to do it (ELOC). This is an interesting finding, as studies generally show that having either internal or external locus of control distinguishes groups from each other [60].
In the earlier literature, Zhou and Wang [104] distinguished informational (seeking and provision of health knowledge) and emotional support (perception that others in the group provide understanding or empathy) as two types of social support available in online health communities that remind of KNO and EMO respectively. However, while in their study, both informational and emotional support were positively associated with eHealth literacy on Norman and Skinner’s [73] scale, the current results do not show a corresponding association with EHIL. A possible explanation is that the eHealth technologies are considered straightforward enough to use to an extent that becoming empowered does not require specific information skills and competences.
Earlier studies show that personal and socioeconomic factors influence people’s engagement with eHealth [29], as do familiarity with ICT in general [35]. In the present study, the contextual factors did not correlate heavily with any of the identified orders. Similarly, the lack of association of technology related issues (ITCONF, NETUSE, ITEXPO) with the factors point to what has been noted in the literature [20], that technology is only one of the many factors contributing to how services are found beneficial and empowering. Even if often overlooked, informational [20] and cognitive factors [39] play a significant role that is not necessarily technology-related.
As a whole, considering the second research question regarding the variation of (dis)empowerment, the findings suggest the presence of four distinct clusters with diverging premises, needs, and projected ends of how (eHealth) technologies should be helpful. Those with lower confidence in their IT skills, who avoid information but still consider themselves competent information users (EHIL), tend to be disempowered (NEG) by eHealth technologies. This differs from results suggesting positive relationships between health literacies and empowerment [7,70]. It can be assumed that this group could benefit from easy-to-use services. However, disempowerment does not necessarily indicate inferior health or health information behaviour. Using non-digital channels and avoiding unnecessary health information can be effective personal health strategies that the healthcare system should support. Forcing individuals to use digital systems and manage information overload can be detrimental.
Research shows relationships between health information seeking behaviour and empowerment [71]. In the current study, among those empowered, active information seekers with either a strong internal or external locus of control and who have retired, are those who are most likely to get emotional support (EMO). For this order of empowerment, the distinctive feature is the confidence that either the individuals themselves or the healthcare system can help them to stay healthy. Maintaining this confidence can be crucial for the order of empowerment to persist. It can also be speculated that the reason for using eHealth technologies is to utilise them as an aid for upkeeping the status quo.
For those who gain KNO, a distinctive feature is awareness of health information’s importance, confidence in using it, and trust in one’s technological competence. For this order of empowerment to last, individuals need usable and useful eHealth technologies and must stay actively involved in their own health matters. This order aligns closely with the ideal of generic empowerment as an outcome of and a rationale for developing eHealth technologies and increasing patient autonomy.
Finally, for those who gain INF, a key issue is health information and communication with health care professionals. The key is that the technology provides a trustworthy channel for communication and accessing high-quality, professionally warranted information. Here, empowerment means being able to use eHealth technologies as a no-nonsense channel to reliable and relevant health information.
5.3. Limitations and future work
When considering the findings, it is necessary to consider certain limitations in the present study. Self-reported data, single source of information, cross-sectional design, and a response rate of 16.7% with unknown bias obviously limits the generalisability of the findings. As the sample is gender-skewed, overrepresentation of women may limit the extent to which the results can be generalised to older men. Experiences of empowerment are contextual and therefore the identified categories of (dis)empowerment might not be directly transferable to other contexts and populations. Future research also needs to assess the relation of perceived usefulness as indicative of empowerment and explicit experiences of empowerment. The study is situated in Finland, which consistently ranks among the highest in Europe in digital literacy, digitalisation, and the adoption of technology in public services [105]. This high baseline level of digital maturity may shape respondents’ perceptions and expectations of (dis)empowerment through digital health services in ways that differ from countries with lower levels of digitalisation. Comparative research across countries with varying levels of digitalisation would help determine the extent to which the identified orders of (dis)empowerment are context-dependent or generalisable. Finally, among the four identified empowerment orders, INF comprises only two items making it relatively less robust and potentially sensitive to data context and analytical choices. Future research should seek to validate and expand this factor with additional items.
6. Conclusion
The findings of this exploratory study show how individuals can become (dis)empowered in different ways by eHealth technologies. Four forms or orders of (dis)empowerment were identified: disempowerment (NEG), knowledge empowerment (KNO), emotional empowerment (EMO), and information and communication empowerment (INF). Of these, the negative order of disempowerment is one of the key findings and requires consideration, as disempowered individuals do not find health information crucial or eHealth technologies useful, whereas emotionally empowered ones trust both the healthcare system and themselves. Knowledge empowered individuals use eHealth technologies for health-related needs and decision-making, while information and communication empowered individuals rely on professional information from patient portals. Comparisons to earlier research suggest the plausibility of the identified orders but we also encourage future research to validate, nuance, and expand the current findings in other information and technology contexts.
Investigating contextual factors related to information behaviour provides insights into variation of (dis)empowerment. Although all forms of empowerment are linked to confidence and competence, higher levels of everyday health information literacy in disempowered individuals suggest informational autonomy. Disempowerment may indicate shortcomings in patient portals, but negative perceptions can also mean that these individuals manage their health by other means and are empowered differently. There should, hence, be caution with attempts to influence users, as promoting autonomy and health information literacy may increase anxiety and encourage disnormative behaviour. Against this background, rather than assuming that empowerment is a monolithic outcome of eHealth use, this study underlines the importance of acknowledging the presence of different orders of (dis)empowerment as means to diverse ends that individuals have in their lives.
Footnotes
Appendix 1
Acknowledgements
The authors would like to thank the anonymous reviewers for constructive comments on the earlier iterations of this paper.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The reported work was supported by the Academy of Finland Grant #287084 for the project Taking Health Information Behaviour into Account: implications of a neglected element for successful implementation of consumer health technologies on older adults (HIBA).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.