
Abstract
This study aimed to evaluate the efficacy of a web-based health information intervention on knowledge, care burden and attitudes of family caregivers of patients with dementia. This study is a unblinded randomised controlled trial. The study population consisted of family caregivers of patients with dementia (n = 50) which were randomly allocated to the intervention group (access to the web-based health information) or control group (access to information as usual). The participants completed knowledge, care burden and attitude questionnaire at baseline and at two months follow-up. A total of 50 caregivers participated in this study. Before the intervention, there was no statistically significant difference between the knowledge, care burden and attitude score between the two groups. In comparison to the control group after the intervention, participants in the intervention group showed significant improvements in all outcomes. These findings provide further evidence that web-based information interventions helped caregivers feel more confident, empathetic and concerned about dementia care with less care burden.
1. Introduction
Dementia is a globally prevalent disease that requires ongoing and increasing levels of care, often provided in the first instance by informal caregivers [1]. In 2021, there are over 55 million people worldwide, and there are nearly 10 million new cases every year; this number is expected to rise to 78 million in 2030 and 139 million in 2050 [2]. There is the same condition in Iran, given the rapid population ageing. The number of people living with dementia in Iran is about 700,000, and every 11.5 min, one person develops the disease [3,4]. Most people with dementia (PWD) live at home and receive care and support from their family members [5]. Most caregivers provide care at home, providing social and emotional support, advanced care planning and financial support [6]. This number is probably higher in Iran due to the culture of Iranian families, their attitude towards their old parents and the lack of appropriate nursing homes [7].
It seems that taking care of PWD is a complex and stressful form of caring [8]. Caregivers may experience many negative consequences in physical and psychological health, such as higher levels of strain and depression and premature mortality in some instances [9]. Family caregivers face common difficulties in caring for PWD, including insufficient knowledge and skill gaps associated with dementia and a lack of practical advice on delivering care to patients [10]. Family caregivers need some skills to monitor patients’ symptom changes, elicit caregiving problems, support tasks, such as assistance with activities of daily living and use available resources properly during the care period to cope with the challenges [11]. Resources must be in place to support family caregivers because they have limited information, resources and support to prepare for their caring role [12].
Professional support at home was widespread to prevent social isolation and offset time shortage among caregivers of PWD. Improving interprofessional dementia-related education is needed to ensure high-quality primary care [13]. Evidence has shown that family caregivers’ educational interventions can reduce depression, stress and feelings of burden and improve family caregivers’ social outcomes [14].
Professional self-management support interventions for PWD family caregivers revealed a significant improvement in the psychological well-being of family caregivers [15]. As a high-functionality tool, the Internet is becoming increasingly popular, and the number of people who receive health information through the web is increasing. The importance of Internet-based educational programmes for preventing and treating chronic or progressive diseases has been well recognised in recent years [16,17].
Furthermore, 80% of Internet users search for health information on the web, and caregivers of people with chronic illnesses often look for information and support for their loved ones through the web [18].
Despite many problems, such as technical, individual, economic and financial barriers [19], the application of e-health can provide high-quality care and health information for patients with complex needs [16].
Some studies provided an overview of the evidence for the effectiveness, feasibility and quality of Internet interventions (mainly websites) for informal caregivers of PWD. Also, these studies showed that Internet interventions for family caregivers could improve various aspects of well-being, such as confidence, depression, anxiety and care burden [20]. The literature suggests that web-based education is a flexible and cost-effective medium; however, to be practical and functional, it must contain features that promote learning and support knowledge translation into practice [21]. Unlike face-to-face interventions, web-based interventions can be delivered to a large number of people without imposing additional costs on each user and making them available all day long [22]. Web-based interventions can provide an efficient, less costly and more accessible way to train and support informal caregivers [23].
Therefore, given the expected increase in the number of PWD and the high level of the physical and mental burden of family caregivers, and the lack of appropriate mechanisms to provide them with accurate health information, this study aimed to determine the beneficial effects of providing health information using the more accessible and affordable approach for family caregivers of PWD. We hypothesised that this web-based intervention could provide health information, skills and training, which reduces family caregivers’ burden and enhances their knowledge and attitudes about the disease.
2. Methods
2.1. Design
We carried out an unblinded randomised controlled trial (RCT) with two parallel groups on family caregivers of PWD who attended neurologist’s offices in Kerman, Iran. Measurement scores were scheduled equally for both groups at baseline and two months after baseline. This study was registered on 26 February 2017 at the Iranian Registry of Clinical Trials by registration ID IRCT2016052828121N1 (http://www.irct.ir/).
2.2. Participants and recruitment
Participants were family caregivers of patients with dementia who were referred to the four neurologist’s offices in Kerman that specialise in dementia diagnosis and treatment. According to the neurologist’s diagnosis, family caregivers of patients diagnosed with moderate and severe dementia were recruited with the assistance of the neurologists in random hours and days during six months. Caregivers were invited to participate in this RCT if they:
Have the ability to read and write in Persian
Have the main responsibility for providing care
Have daily access to the Internet
Have a smartphone, tablet or desktop device
Have the ability to use the Internet and devices mentioned above
and caregivers are excluded if:
Unable to continue participation
Delegate care to another person
A patient dies
Then, researchers contacted eligible caregivers about participation and obtained their consent to participate in this research.
2.3. Sample size
The sample size was calculated according to the data extracted from Canonici et al. [24] in the Comparing Two Means–Sample Size formula. Based on the standard deviation of the care, burden scores after the intervention reported in this study (SD1 = 13.7, SD2 = 8.1). With an assumed mean difference (d = 10) to reach a larger sample size, 20 participants needed to be included to detect this difference in each group with a 90% power (α = 0.05). In this way, with respect to loss to follow- up of 15%; our sample size increased to 25 participants for each group.
2.4. Randomisation
In this study, 50 caregivers were randomly allocated to the intervention group and control group. Randomisation was based on using the Microsoft Office Excel randomisation equation with stratification according to age and the number of hours of care a day. The study flow chart was developed following the CONSORT guideline and is shown in Figure 3.
2.5. Website development
A web-based information intervention was designed as a free, password-protected, fully automated website to be used through any devices, such as a mobile, tablet and desktop, anywhere, by the caregivers. The website has been developed in the Persian language (Figure 1).

Screenshots from different parts of the website. (a and c) Home page and menus. (b) Session content.
The website content was based on the educational topics and it was divided into four main sections: documents, videos, news and events, and forum (Figure 2). The content is generated by reviewing the relevant literature, guidelines and scientific articles. Initially, the first author investigated the contents and then sent the relevant content to expert group, including two neurologists, one psychologist, one general practitioner and one of the experienced caregivers for investigation. After collecting their comments and suggestions, the website’s concepts were examined during two sessions with the first author and the expert group. The modifications were made, and the contents of the website were finalised. Eventually, each session is uploaded on the website (one or two sessions a week). These concepts were presented in texts, slideshows, pictures, useful links and videos. In addition, a chat room was placed on the website to interact with other caregivers, ask questions and advise.
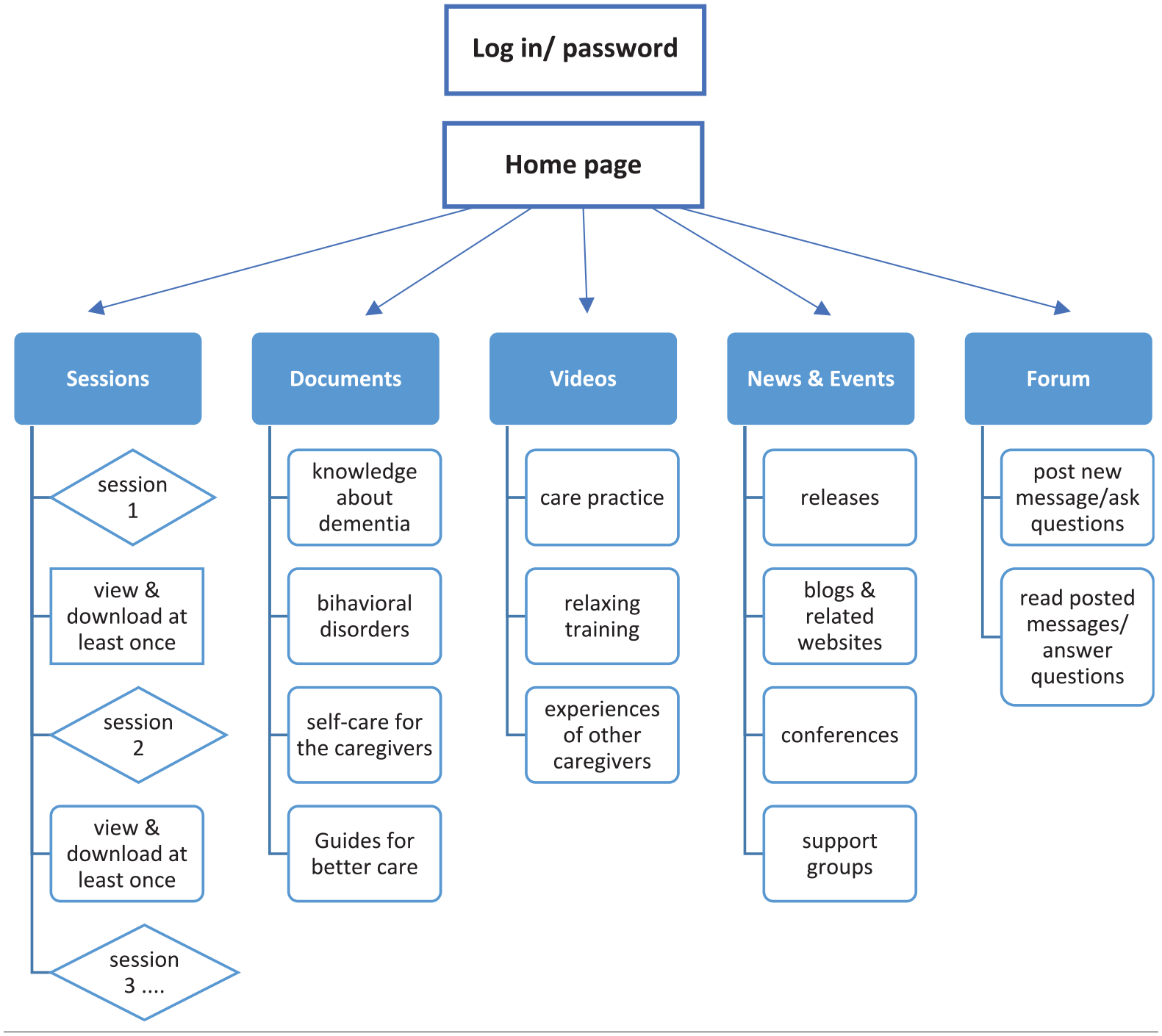
Layout of the website and process for viewing weekly sessions.
2.6. Intervention
The intervention period was two months (eight weeks). Each week contained one or two sessions (lasting 15–30 min).
Each participant had a unique username and password, and their logging information and frequency of visiting the website were saved. The first researcher sent weekly recommendations to participants in the intervention group through email or SMS to communicate with them to ensure they read the session’s concepts.
In total, 12 computer-interactive sessions were designed to be taken. These 12 sessions cover the following sections:
Following areas as a text and images: (a) information about dementia, (b) Behavioural disorders, (c) Self-care for the caregivers and (d) Guides for better care.
Videos about (a) relaxing training, (b) practical care training and (c) experiences of other caregivers.
Important events and news.
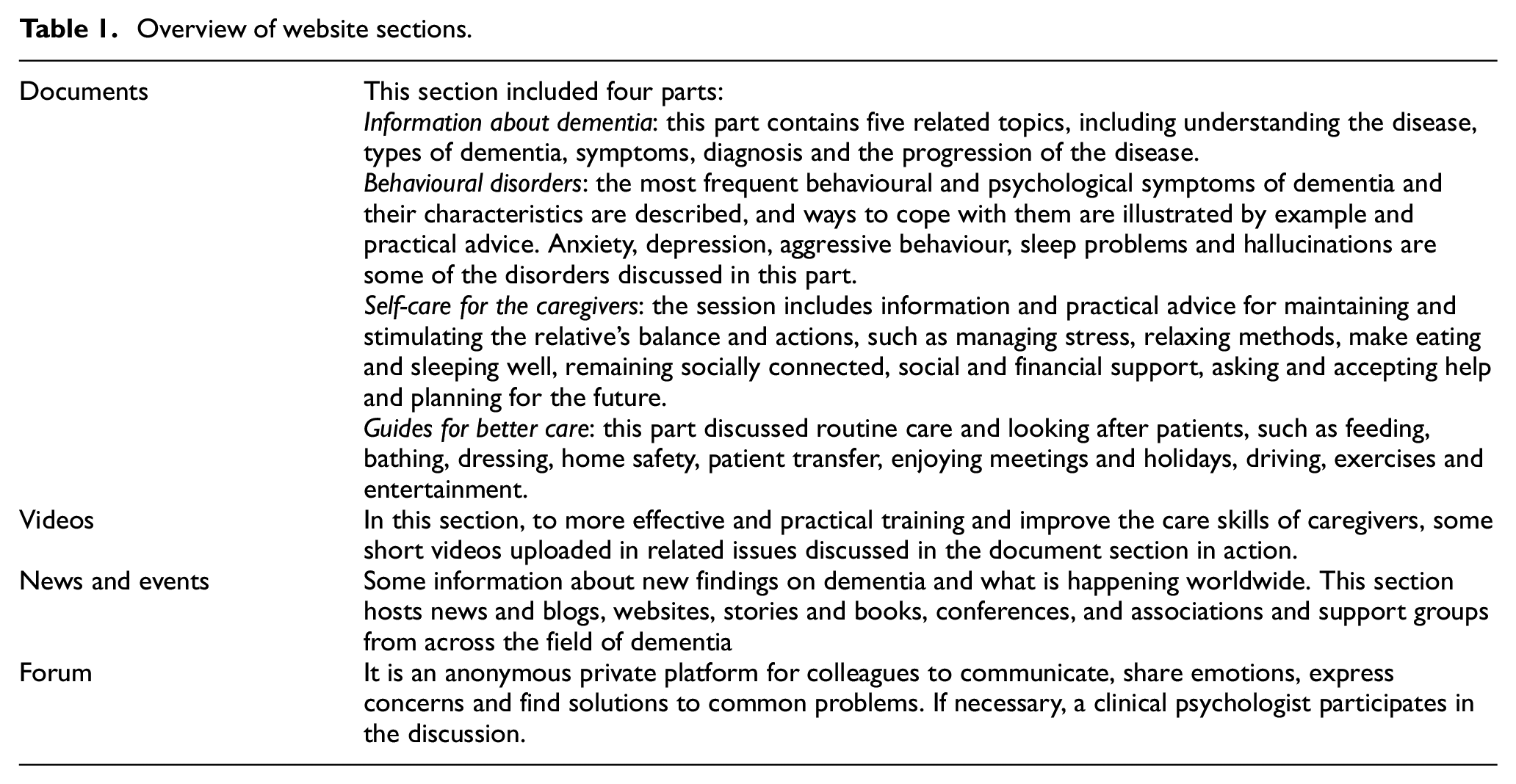
In addition, the website includes a forum to share the information, experience and ask questions with no time limit, and the participants could access these sections as long as they wished at any time. A new session was uploaded after the validation of the previous session. An overview of the sections is shown in Table 1.
Overview of website sections.
Participants in the intervention group had to validate one or two sessions per week for two months.
Participants in the control group receive usual information, such as a neurologist’s semi-annual follow-up appointment, during which the family caregivers obtain illness information from the neurologist.
At first, all intervention and control groups completed three questionnaires described below at baseline and two months after baseline (end assessment).
The intervention group participants received a 20-min training session at baseline on using the website, a username and a password to log in. All participants were advised to look for additional help if necessary and were asked to inform the researcher about it.
2.7. Outcome measures
We used a questionnaire to assess caregivers’ care burden, knowledge and attitudes before and after the intervention. Our measures were divided into four sections:
A questionnaire collected demographic information of the patients and the family caregivers, including age, gender, degree of education, marital status, employment, income, caregiver-receiver relationship, hours of care a day, years of care, and financial status.
The care burden perceived by the caregiver was measured by the Zarit Burden Interview (ZBI) [25]. This scale is a widely used scale that rates the caregiver’s perceived care burden. The validity and reliability of the Persian version of the ZBI have been confirmed in the previous study [26]. This instrument includes 22 items and measures the care burden of caregivers. The score range is from 0 to 88, where the increase in burden score means an increase in caring load. ZBI cuts off as ‘high burden’ with scores > 40/88 and ‘low burden’ with scores ≤ 40/88.
The second questionnaire was the Alzheimer Disease Knowledge Scale (ADKS) [27]. The previous study confirmed the validity and reliability (82%) of the Persian version of this questionnaire [28]. In the analysis, one point was given for each question answered with ‘True’, and ‘False’ and ‘I Don’t Know’ answers gave no point. Thus, the total score ranged from 0 to 30, with higher scores signifying good knowledge about Alzheimer’s disease.
Attitude towards the disease (DAS) was evaluated with 20 items questionnaire designed by Lunsman and Mc Fadden [29], in which five psychologists and neurologists confirmed its content validity. Cronbach’s alpha also determined the reliability of the questionnaire (r = 0.85). This scale was compiled of 20 items that assessed participants’ attitudes towards Alzheimer’s disease and related dementias. The participant was asked to rate each statement’s agreement on a seven-point Likert-type scale where one strongly disagrees and seven strongly agreed. A higher score on the questionnaire means a positive attitude towards Alzheimer’s disease.
2.8. Data analysis
Data were analysed by SPSS version 24 using inferential statistics, including chi-square, Mann–Whitney, Wilcoxon Tests, and linear regression model. The chi-square test compared the qualitative variables between the intervention and control groups. The Chi-squared test was employed to compare the demographic variables between the two groups. Mann Whitney U test was used to compare the change in knowledge, care burden and attitude before and after the intervention between the two groups, and the Wicoxon was used to compare the scores within the groups before and after the intervention. The linear regression model was also used to determine demographic variables associated with knowledge, care burden and attitude.
3. Results
Overall, 94 individuals were assessed for eligibility. However, 36 of them did not meet the inclusion criteria, and eight declined to participate. Therefore, 50 caregivers consented and were randomised to either the intervention group (n = 25) or the control group (n = 25). Ultimately, 47 participants were included in the final data analysis. The patient recruitment and reasons for excluding participants before starting the trial and those who dropped out during the trial are presented in Figure 3.
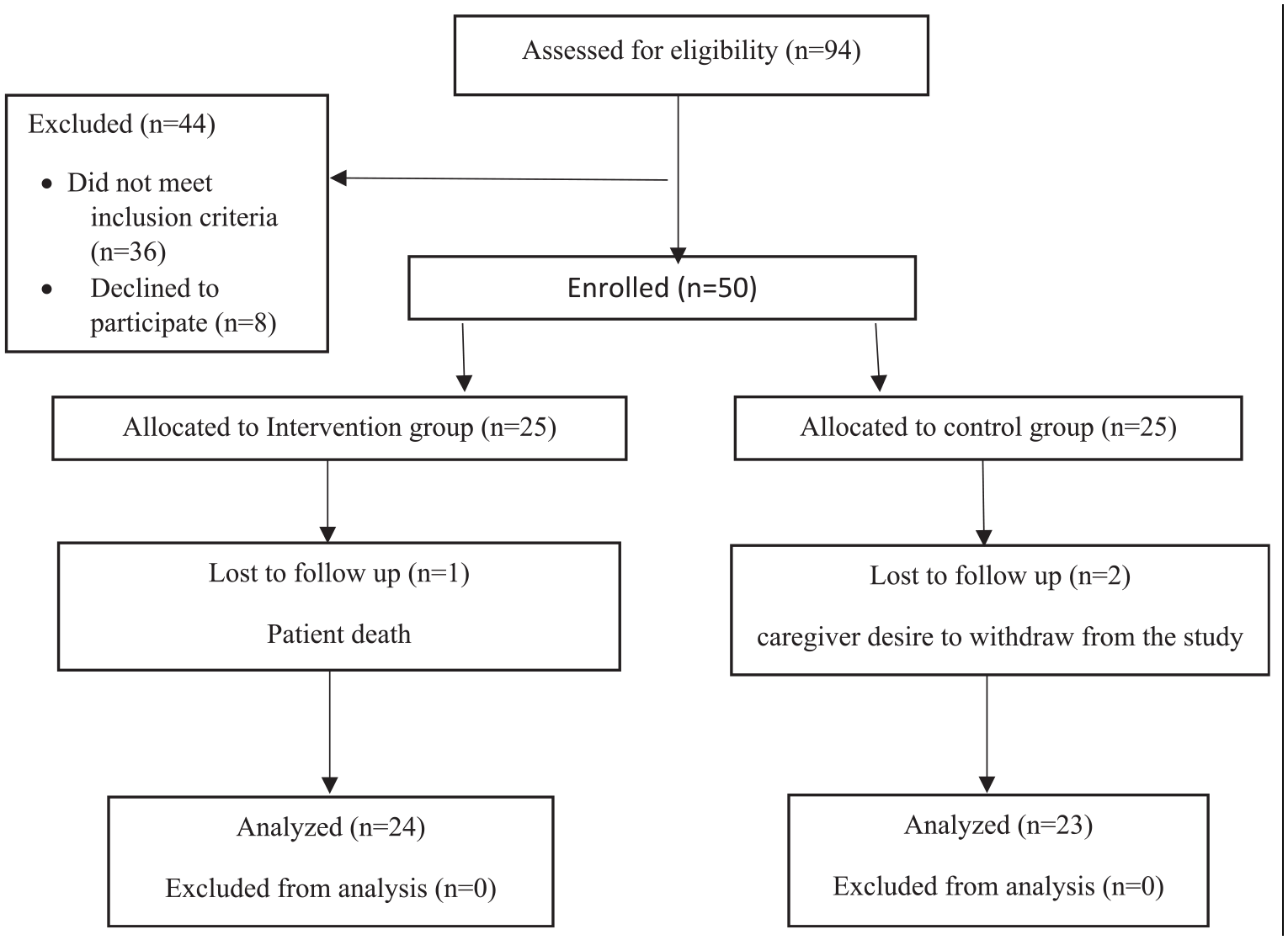
The CONSORT flow diagram of the pilot RCT.
3.1. Demographics information of the participants
Table 2 shows demographic information of the intervention and control groups. Most family caregivers in both groups were female and aged between 41 and 50 years. The highest education level in the two groups was the postgraduate degree belonging to 51% of participants, and the lowest was the primary education degree belonging to 12% of participants. Most caregivers were married and unemployed. More than half of them earn between 10 and 30 million RLS per month (minimum monthly wage was 8,500,000 RLS at the time of recruitment). Overall, 62% of patients needed care almost 24 hours, and 32% were under the support of their families more than three years. Also, only 29% of caregivers had access to the Internet, and 70% connected through mobile phones.
Demographics information of the participants.
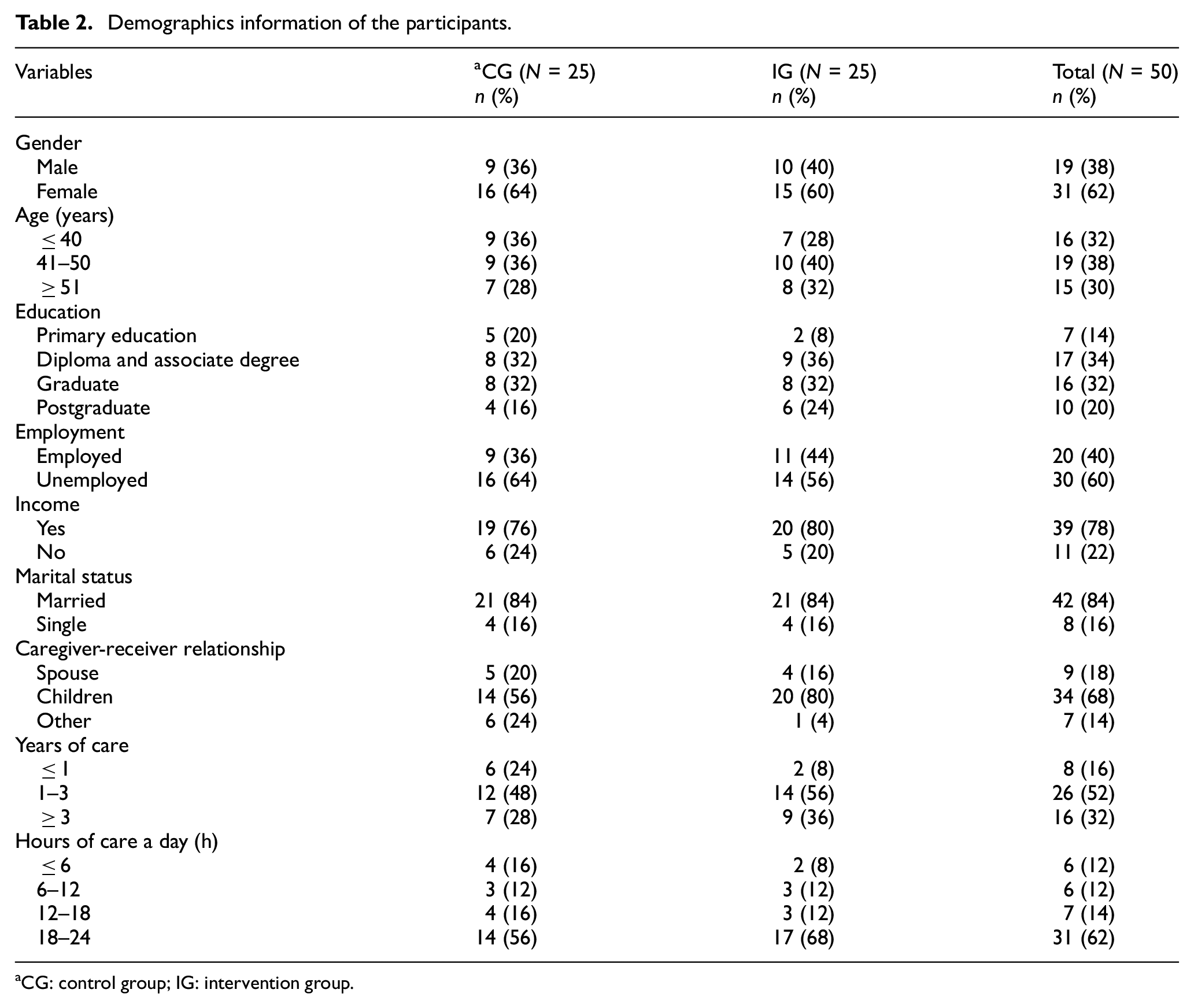
CG: control group; IG: intervention group.
3.2. Compare the knowledge, care burden and attitude scores at baseline and after the intervention
The Mann–Whitney and Wilcoxon Tests (Table 3) showed that the difference between care burden scores before and after in the intervention group was decreased about 14 units, which was significant (p<0.05). In contrast, the difference between care burden scores before and after the intervention in the control group decreased about one unit.
Between-group and within-group effects of the intervention.
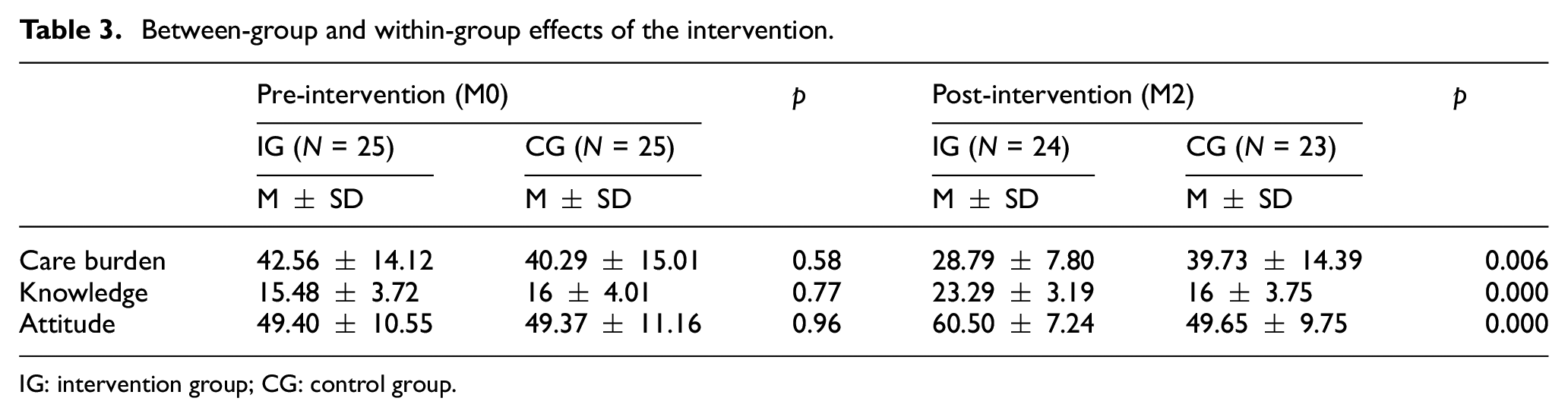
IG: intervention group; CG: control group.
Participants who used the website (IG) showed eight units increase in their knowledge score, and this difference is statistically significant (p<0.05). Caregivers’ knowledge before the intervention in both the control and the intervention groups was not significantly different and was 15.48 in the intervention group and 16 in the control group.
At baseline, there were no statistically significant differences in both groups according to attitude questionnaire results (about 49), but results showed about 11 units improvement in the intervention group after the intervention (p<0.05). Furthermore, no differences were observed in the control group.
It is clear from these results that the intervention group improved from the pre-test to the post-test in all three factors, whereas the control group remained unchanged.
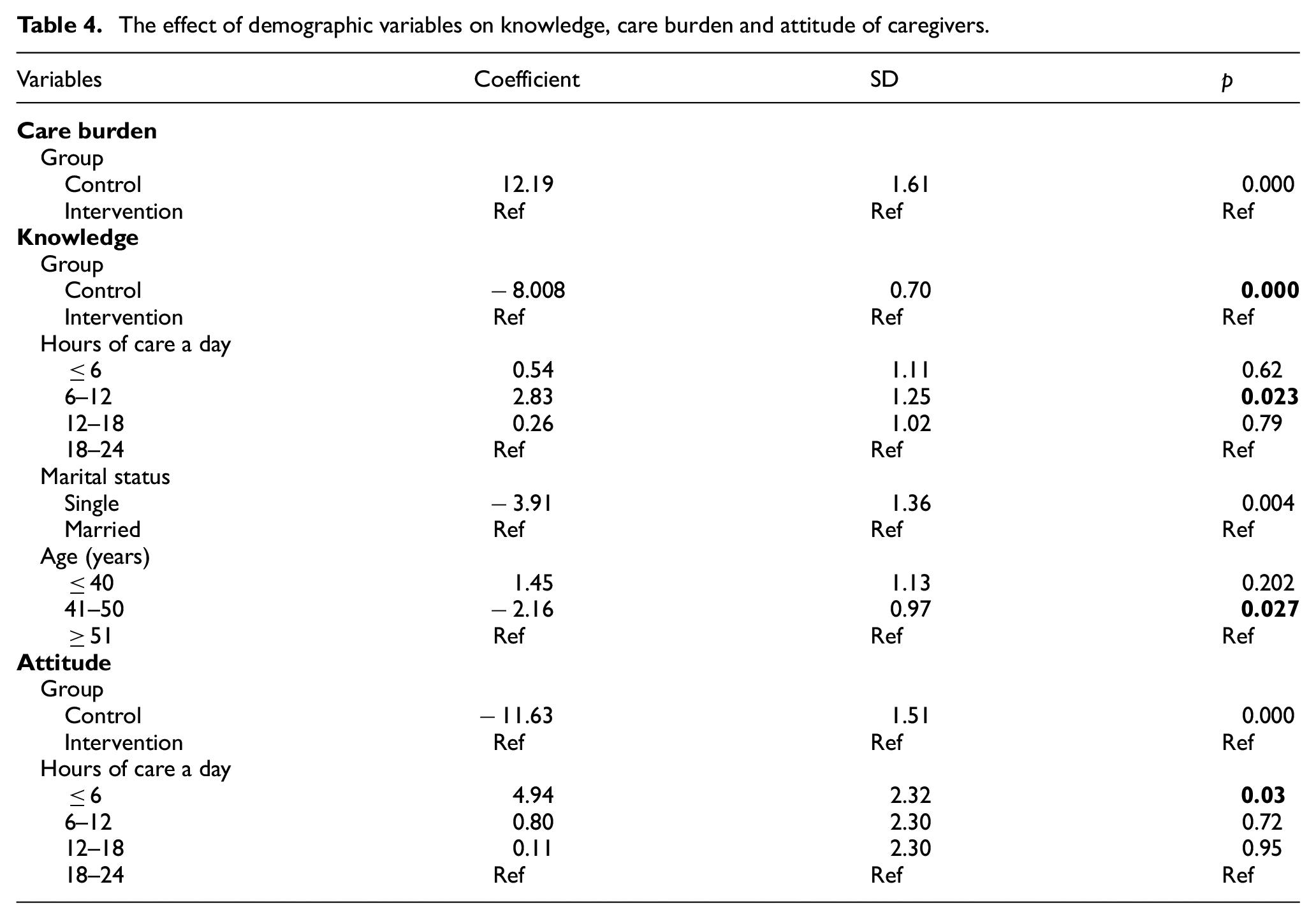
The linear regression model analysis showed that the group variable was a significant variable for all three factors, demonstrating the positive effect of information intervention in improving knowledge, attitude and decreasing care burden (p<0.05).
The knowledge score of the caregivers after the intervention was dependent on the variables of the group, hours of care a day, marital status and age. According to our results, caregivers who provided care 6–12 hours a day have a higher knowledge. Moreover, the age and marital status variables showed that caregivers in the age group of 41–50 years and single caregivers had a lower coefficient and performed their caring tasks worse than other groups.
According to Table 4, the variables of group and hours of care a day affect the attitudes of the patient caregivers, which were statistically significant (p < 0.05). The backward linear regression analysis also showed that the attitude score of the caregivers who provided care at most six hours a day is higher than other groups.
The effect of demographic variables on knowledge, care burden and attitude of caregivers.
4. Discussion
We set up the website to examine the effectiveness of web-based interventions in promoting knowledge, improving attitude and reducing the care burden of family caregivers of patients with dementia.
Lack of knowledge about dementia causes caregivers to overestimate the patient’s abilities, leading to tremendous anger, frustration and depression, and many family caregivers are unaware of their patients’ impairment. These findings highlight safety concerns in dementia and suggest that family caregivers could benefit from education about potential patient losses, such as diverse cognitive, functional and behavioural symptoms that lead to dementia [30]. Unfortunately, caregivers of PWD often have limited knowledge about dementia [31]. Knowing and utilising the long-term supports and services available to the care receiver can improve the quality of their care [32].
The use of our educational website effectively improves family caregivers’ knowledge about dementia. Our findings showed a significant increase in the mean score of knowledge in the intervention group. There is evidence that web-based training could increase staff and caregivers’ confidence, knowledge, skills and attitudes towards PWD and be sustainable over time [21]. A study in 2015, showed the knowledge of informal caregivers of persons with Alzheimer’s disease who were exposed to a web-based psychoeducational programme is increased [33]. In the case of dementia, the importance of demonstrating the improvement of knowledge of a broad group of participants through free and widespread online courses is evident [34].
Moreover, the improvements in caregiver burden resulting from web-based interventions in this study are promising. Family caregivers reported a level of medium burden. Previous research has shown that the level of care burden in the intervention group reduced significantly while there was no change in the control group. These results indicate the effectiveness of interventions related to providing health information and counselling and training in these patients [5]. Other web-based intervention studies for caregivers have confirmed the importance of providing information to reduce stress and anxiety [35]. Due to the widespread use of the Internet, web-based interventions can play an essential role in reducing the stress and distress of caregivers and improving their health [23].
The results of our study showed that the family caregivers have moderately low attitudes towards patients with dementia. After web-based information, their responses indicated an increased desire to provide care to PWD. The web information intervention significantly affected the positive attitudes towards PWD in the intervention group. Our findings also confirm results obtained by Irvine about the positive effects of Internet-based interventions on attitudes and empathy of aggressive residents and caregivers [36].
In another study, over 80% of participants felt that the information and skills they gained from online dementia education programmes were frequently associated with new knowledge, improving their understanding, awareness, attitudes and changes in practice [37]. Evidence of attitude changes after technology-based training was not very convincing. However, improved knowledge can also influence practitioner attitudes [38].
Similar to ours, previous research has found that most participants suggested that the web-based intervention improved their caregiving skills and found the technology to be easy to use [39]. Family caregivers’ confidence in caring for persons with dementia increased after using an Internet-based programme [40].
Numerous studies of web-based programmes for dementia caregivers and chronic caregivers, in general, have shown that caregivers have described using this approach as easy, helpful and practical and have positive results in knowledge, attitude and self-efficacy. In addition, a sense of empathy, a reduction in stress and anxiety in caregivers and caregivers feel more confident about their caregiving skills and communicating with their patients [41–43]. Also, a web-based learning environment is a platform that delivers a platform that is self-directed, individualised, interactive, multimodal, flexible, accessible, consistent and cost-effective [21].
Caring is sometimes considered all the physical, psychological, economic, social and family consequences of caring. Most family caregivers perceived inadequate support from the health care providers in managing dementia-related problems reported strain. They had low confidence in managing caregiving, and the results of this study indicate the high necessity for implementing educational-specific intervention for caregivers of adults. As shown in Table 3, caregivers who spend fewer hours caring for their patients have better knowledge and attitude after the intervention. It may indicate that if other family members or healthcare providers support family caregivers, they can take more time to recover and increase their knowledge, eventually reducing care pressure and improving their mental status. In this way, easy and accessible educational methods, such as web and mobile education, can save time and energy.
Our research has shown that web-based educational programmes positively affect caregivers’ knowledge and attitudes about this disease. Recommendations are made that healthcare professionals should assess family caregiver burden and address their physical and mental health needs. Family caregivers should also be regularly educated on everyday caregiving tasks to ease their burden. Our web-based intervention provides convenient, effective and easy-to-use methods for supporting caregivers and provides evidence-based interventions based on web and mobile health technologies. Caregivers of patients who have dementia deserve the chance to recover, and accessible, evidence-based help and support through a web offers hope and an opportunity to promote their quality of care and quality of life.
There may be some possible limitations in this study. Our sample size was limited. Many family caregivers found themselves in embarrassing situations because they cared for someone with dementia and refused to cooperate with the researchers, even though their information remains confidential.
Another problem was the difficulty in selecting people who met the inclusion criteria. One of the inclusion criteria was Internet access and working with it. Unfortunately, some people do not even have access to the Internet and lack knowledge of using it, especially older caregivers. So, given the ever-expanding use of the Internet and the prevalence of information today through the Internet, it is suggested to provide more people with the necessary communication infrastructure and cheaper and faster Internet access; however, training in the use of communication tools is a prerequisite.
This study was done in one of the large developing cities in Iran, but our result could be different in other cities with various Internet and mobile infrastructure. Also, we evaluated the effect of a web-based information intervention on caregivers during two months, and the long-term effects of this method need to be investigated. We suggest addressing these problems in future studies.
5. Conclusion
The web-based format is a potential platform for delivering interventions to dementia patients’ caregivers for its unique advantage of easy accessibility, no geographic and time barriers. This study found that web-based interventions could significantly improve knowledge and attitudes towards dementia, leading to a better quality of care provided by caregivers with less care burden. Future research will identify whether more extended use of the educational website can significantly affect other behavioural outcomes. Future studies can assess family caregivers’ needs to help health policymaker and developers to design and implement technology-based interventions considering family caregivers’ needs. Moreover, other studies can concentrate on technology use barriers. There are some barriers to using technology-based interventions for family caregivers. It is important to determine these barriers before designing and implementing interventions to increase accessibility and use of these interventions.
Footnotes
Acknowledgements
The authors thank all neurologists and patients who participated in this study. They also thank Mr Mehdi Samadani, one of the experienced and skillful caregivers, for his advice, support and encouragement throughout our study.
Author contributions
S.S., M.A. and K.B. were responsible for the overall design of this study; S.S. addressed ethical considerations and trial registration, designed the website, collected data and set the intervention; K.B. confirms all health information uploaded on the website; M.M. planned statistical analysis; S.S. and N.J. wrote the first draft article. All authors contributed to the final article, and all authors have read and approved the final article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the Vice Chancellor of Research and Technology, Kerman University of Medical Sciences, Kerman, Iran.
Ethics approval and consent to participate
Ethical approval was obtained from the ethics committee of Kerman University of Medical Sciences, Iran (IR.KMU.REC.1395.185), and a written consent was signed by each participant.
Consent for publication
No individual data are contained in this manuscript.
Availability of data and materials
The datasets generated and/or analysed during the current study are not publicly available but are available from the corresponding author on reasonable request.