
Abstract
Personality disorders are an often-misunderstood phenomenon. Many of the persistent misconceptions are related to the fact that personality and personality disorder are understood as a simple collection of a person’s trait characteristics. In this paper, we demystify the meaning of personality and personality disorder by drawing on decades of research on personality development and more recent research on the development of personality disorders. We show that while temperament and personality traits play an important role in setting the stage for the potential development of personality disorder (and other disorders), the onset of personality disorder depends on the interruption of the developmental task of creating a coherent and stable sense of self and identity in adolescents. In this view of personality functioning, psychological processes are identified that go beyond traits to identify malleable prevention and treatment targets that serve to support healthy personality development in young people.
Keywords
Development of Personality
According to McAdams’ (2015) personality theory, personality is formed through three processes (levels) that go through different stages of development, are integrated into the individual, and are referred to as the binding of personality. The first level is the development of
Making sense of the marked individual differences among individuals has been of interest for centuries, and various authors have come to similar conclusions when studying infants and young children that certain temperamental traits can be identified in children and form the basis for later personality traits. While authors have differed in the number and naming of temperamental dimensions that account for individual differences, with some temperamental traits being more widely accepted than others (Shiner et al., 2012), most theories converge with the position of Rothbart (2011) that a person’s behavior is the result of an interaction between their reactivity and self-regulation. She proposed that the most important dimensions of temperament are Surgency, Negative Affectivity, Effortful Control, and Affiliation. These dimensions were identified using self and other reports across the lifespan and in different cultures and validated with factor structures, and were consistent with other temperament observational studies (Vroman et al., 2014) and personality inventories (Evans & Rothbart, 2007). These temperamental dimensions are also related to symptoms of emotional and behavioral disorders, suggesting that temperamental traits can also be explained by an underlying two-factor model of internalizing and externalizing behavior that subserve psychopathology (Kotov et al., 2021; Oldehinkel et al., 2004; Sharp, 2020; Shiner et al., 2012; Tackett, 2006).
With increasing maturity and experience, a child develops their personality further. For decades, the most powerful personality theory, the Big Five Factor (BFF) model, developed from factor analysis of lexical studies of people’s natural language descriptors and self-reports of personality traits and observer ratings (McCrae & Costa, 1997), has been the subject of numerous research studies and has been validated in many cultures around the world (McCrae, 2009). The BFF defines interpersonal differences in terms of five dimensions (extraversion, agreeableness, conscientiousness, neuroticism, and openness to experience) that are closely related to temperamental traits, and some authors view them as earlier and later developmental manifestations of the same basic traits (Sharp, 2020; Shiner, 2015). Personality traits are generally considered to be moderately stable across the lifespan, but they also undergo systematic changes, particularly in early life stages. Meta-analytic findings show that individual differences in personality exhibit modest rank-order stability during early childhood, which increases substantially during adolescence and peaks in young and middle adulthood (Bleidorn et al., 2022). Contrary to older assumptions, stability does not continue to rise markedly beyond the age of 30, and some studies even suggest slight declines in later life. Moreover, personality traits continue to develop through interactions with the environment, social roles, and life experiences. On average, individuals show increases in traits that reflect psychological maturity, such as emotional stability, conscientiousness, and agreeableness, especially during young adulthood (Bleidorn et al., 2022; Roberts et al., 2006). Thus, while individuals tend to maintain their relative position within a group over time (rank-order stability), their absolute trait levels (mean-level change) remain open to developmental influences across the lifespan. Despite considerable variability in personality traits and environmental influences, the majority of individuals follow normative developmental trajectories and achieve healthy personality functioning over time.
In the first stage of personality development, McAdams (2015) emphasizes the importance of the interaction between the characteristics of the child and the environment and compares it with
However, people are not just a collection of traits, and descriptive information about a person’s level of traits may have limited clinical value. Characteristic adaptations play an important role in shaping personality and emphasize the individual as a goal-oriented being. The second level of personality development is referred to as the motivated actor, according to McAdams (2015), and refers to a person’s motivation, goals, and values, their translation into plans and strategies, and taking responsibility. Toddlers begin to express their desires in an egocentric way (“I want!”), more sophisticated adaptations develop at ages 5–7, closer to puberty, more individualized goals develop, and children begin to pursue them more thoughtfully (McAdams & Olson, 2010). In response, self-esteem increases as an important marker of successful development. Later, this level is reflected in personal and professional long-term goals and in overcoming challenges. The emerging mentalization processes help the child in this process, for example, through social referencing, when the child learns to manage his or her behavior and emotional reactions in unfamiliar situations by observing the emotional responses of his or her caregivers (Vandivier & Hertenstein, 2013). Next, the ability to temporarily imagine an alternative reality—pretend play—helps the child to learn the difference between reality and fantasy, improve social skills and emotional regulation, and give the child the opportunity to test out different identities (Weisberg, 2015). Also, the development of “Theory of Mind” allows the child to become aware that they and other people have beliefs and desires that influence the behavior displayed, and that the content of their mind may be different from the content of another’s mind (Apperly, 2012).
The third level of personality development, according to McAdams (2015) (the autobiographical author), is the development of identity through the construction of a narrative life story. Narrative identity, internalized, evolving life story that provides a sense of unity, purpose, and temporal coherence, emerges from early autobiographical memory in preschool years, shaped by caregivers (McAdams, 2015; McAdams & McLean, 2013). However, a self-authored, coherent “story of the self” typically develops in adolescence, alongside advances in metacognition, formal-operation thinking and mentalizing abilities (McAdams & Olson, 2010; Sharp & Wall, 2021; Sharp et al., 2025).
To summarize, optimal personality development depends, first, on the fundamental dispositions and experiences of the individual. These factors then interact to determine how the personality is organized over time and whether the individual will be able to accomplish all developmental tasks, that is, learning to regulate one’s emotions, developing a stable and realistic self-image with a sense of intrinsic worth, integrating values into internalized goals to guide behavior, and building lasting and fulfilling interpersonal relationships. Ultimately, it is about whether he or she will be able to integrate this into a final identity that leads to further self-actualization, or in other words, whether he or she will reach an optimal level of personality functioning. Elsewhere, we have used McAdams’ (2015) concept of “binding of personality” to describe this process of bringing together all aspects of personality functioning as a significant milestone of adolescent development (Sharp & Wall, 2021).
From Maladaptive Personality Development to Adolescent Personality Disorder
Unfavorable interactions between the characteristics of an individual and the environment can contribute to the unfavorable development of a child’s personality right from the start. For example, a young child with a difficult temperament (high neuroticism and impulsivity) and neurodevelopmental problems such as ADHD is more likely to elicit negative reactions from their parents than a sibling with other traits (high surgency and high effort control), thus increasing their risk of developing a maladaptive personality (Kiff et al., 2011). Important interacting factors influencing the formation of personality are the characteristics of the social environment, including caregivers, the types of messages and interactions the child receives from parents and others, and whether these influences are providing enough scaffolding for the binding of young adult personality, or whether the personality will develop in a dysfunctional way. Some of the greatest risk factors for maladaptive development are a suboptimal family environment that does not meet the child’s basic emotional needs, such as the need for secure attachment, love, autonomy, competence, clear and realistic boundaries, early traumatic experiences (such as abuse, neglect, or loss), and a chronically dysfunctional environment (such as poverty). These risk factors can impair the development of mentalization and prevent the development of stable personality structures and interpersonal skills (Fonagy et al., 2002; Stepp et al., 2016). It is important to note that while certain early personality traits or unfinished developmental tasks have been identified as risk factors for later personality pathology, this does not imply a deterministic developmental trajectory per se. In the development of psychopathology, we speak of the principle of multifinality, which means that individuals with similar characteristics and experiences can have different end results (Cicchetti & Rogosch, 1996). For example, even high levels of the traits themselves do not lead to a personality disorder (PD), nor do traumatic events or poverty have the same impact on all children. The outcome depends primarily on resilience and the complex interplay of risk and protective factors over time.
Although research on borderline personality disorder (BPD) in adolescents shows that the disorder is usually preceded by negative affectivity, impulsivity, and internalizing and externalizing psychopathology, PD is not simply a conflation of personality traits, but an interruption of developmental milestones. These include the formation of a coherent and stable self-concept, constructing the identity, building the capacity for affect regulation, the development of empathy, and the emergence of reflective functioning (mentalization) and enchasing interpersonal development (Sharp & Wall, 2018; Stepp et al., 2016). This task becomes particularly salient during adolescence, when metacognitive and mentalizing capacities allow for the integration of experiences into a unified self-concept. Failure to achieve this integration may result in fragmented identity, impaired self-regulation, and difficulties in interpersonal functioning, all leading to potential derailment into pathology.
For example, “theory of mind” develops in 4- to 5-year-old children, and at the age of 5–7 years, we already observe some normative interpersonal behaviors that are made possible by the acceleration of mentalizing abilities. The lack of mentalization skills at this age (which means that the child is unable to consider other perspectives or that he or she follows his or her own desires without considering the desires or needs of others) means an increased risk of later maladaptive personality development. However, a diagnosis of PD can only be made later, after puberty, when metacognition allows adolescents to integrate their experiences into a coherent self-narrative. At this age, we can observe insufficient development of mentalization, weak reflexive capacity and emotional regulation, weak identity, and an incoherent sense of self in some individuals (Sharp, 2020; Sharp & Wall, 2021). With difficulties in managing the self, an individual is also then unable to establish stable and warm interpersonal relationships, either due to difficulties in seeing or integrating the perspectives of others or a lack of trust (Sharp, 2020).
According to the DSM-5 (American Psychiatric Association, 2022), a PD is an enduring pattern of internal experience and behavior that deviates markedly from the expectations of the individual’s culture, is pervasive and inflexible, begins in adolescence or early adulthood, is stable over time, and results in distress or impairment. For many years, the categorical model (DSM Section II) was used as the basis for decisions about the treatment of PDs. However, it has been shown that among the ten identified categories of PDs, there is a high degree of heterogeneity, a lack of discriminant validity, high comorbidity, and co-occurrence of different PDs, which means that the model cannot be methodologically supported by factor analyses (Krueger et al., 2018; Sheets & Craighead, 2007). Moreover, individuals within the same group can differ greatly from each other, and at the same time, the thresholds for diagnosis are arbitrary (Krueger et al., 2018). Despite these concerns, the categorical system is still used by many clinicians and forms the basis for some therapeutic interventions. In practice, however, it appears that clinicians do not differentiate between the different PDs, but mainly make a broader diagnosis (PD-NOS) (Verheul et al., 2007). As a result, the practice of providing patients with manualized treatments is discontinued, and patients receive eclectic treatments that lack evidence-based support and cannot be systematically evaluated (Krueger et al., 2018).
As a result, the dimensional approach to personality pathology has gotten significant traction over the last 10 years (Sharp & Miller, 2022). The dimensional approach to the diagnosis of PD has evolved since the 1950s and is now included in the most recent versions of classification systems, like DSM-5-TR (Section III—Alternative Model for Personality Disorders [AMPD]; American Psychiatric Association, 2022) and ICD-11 (World Health Organization, 2019). The ICD-11 marks a paradigmatic shift from categorical prototypes to a dimensional model of PDs with emphasizing impairments in self and interpersonal functioning and classifies personality pathology according to severity (mild, moderate, or severe), with optional trait domain specifiers (e.g., negative affectivity, detachment, dissociality, disinhibition, anankastia) to describe the individual’s maladaptive personality patterns. Similar in DSM-5-TR, Section III, the AMPD refers to this factor as “Level of Personality Functioning” (LPF) represented in Criterion A (the entry criterion) of the PD diagnosis. The assessment of LPF focuses on mental representations of the self (identity and self-direction) and others (empathy and intimacy) and is central to establishing a PD diagnosis. Both systems allow for a developmentally informed understanding of personality pathology, emphasizing the role of disrupted development of self and relationships in adolescence (Sharp, 2020; Sharp & Wall, 2021). In particular, provide a clinically useful, flexible framework that bridges normative personality development and psychopathology without relying on rigid categories. Moreover, the inclusion of maladaptive self and interpersonal functioning allows us to see personality in dimensions ranging from healthy personality to pathology (Bender et al., 2011; Sharp et al., 2022). The AMPD Criterion B in DSM-5-TR (similar to optional trait domain specifiers in ICD-11), on the other hand, refers to the assessment of maladaptive trait (Negative Affectivity, Psychoticism, Disinhibition, Antagonism, Detachment), that are based on early dispositional traits and largely reflect the BFF structure (Negative Affectivity—neuroticism, Detachment—opposite of extraversion, Antagonism—disagreeableness, Disinhibition—opposite of conscientiousness, Psychoticism—openness). Criterion B therefore provides a useful description of aspects of personality functioning over time and, in children, an early, albeit non-specific, risk marker for maladaptive personality development. There are currently no guidelines as to when a trait should be considered severe enough to require clinical intervention, meaning that traits are not of sufficient diagnostic value at this point. A diagnosis therefore requires consideration of individual functioning: identity, self-direction, empathy and intimacy—developmental tasks that are central to adolescence (Sharp, 2020). These developmental tasks are summarized in a unidimensional continuum of personality functioning severity (LPF), which allows for the assessment of differences in personality functioning when comparing an individual to others, as well as tracking an individual over time.
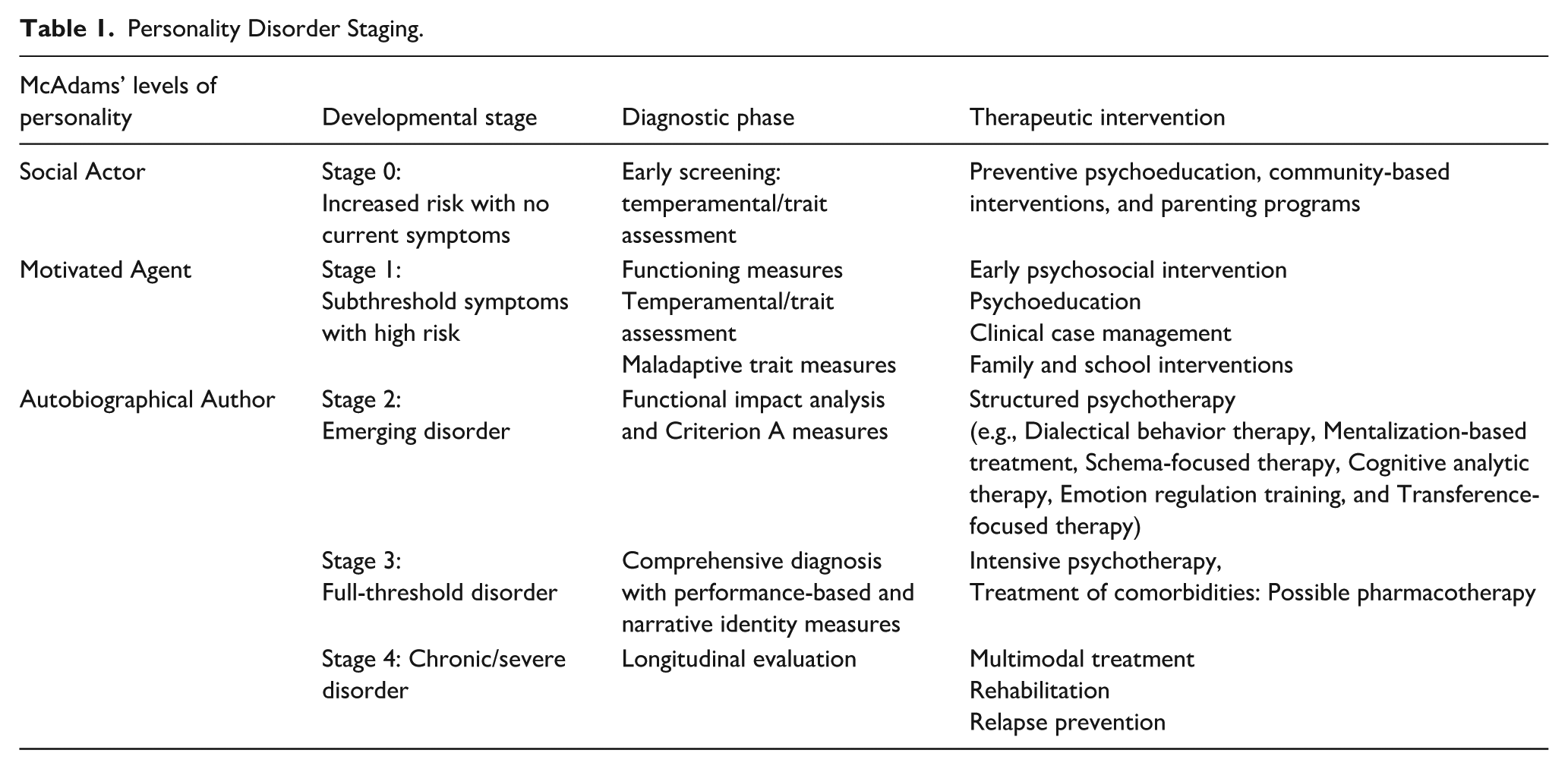
In terms of clinical application of the developmental model for the emergence of PD proposed here, we have argued that it carries a major advantage given its natural convergence with thinking about intervention in clinical staging terms (Chanen et al., 2016; Sharp et al., 2021, 2022, 2025). Clinical staging describes a progression of disorders from
Personality Disorder Staging.
Assessment of Maladaptive Personality and Personality Disorder in Children and Adolescents
The clinical psychological assessment of PD requires a comprehensive approach that incorporates various data sources and adheres to established diagnostic criteria. It usually aims to assess a person’s behavioral patterns, cognition, emotional regulation, and inner experience (Waugh et al., 2017). This process has changed significantly over the past 100 years, from a categorical to a dimensional approach with a focus on LPF (Criterion A), which is now considered the genus of personality pathology (Rucker et al., 2024). Refocusing PD assessment away from the assessment of 10 categorical disorders, to the core of the personality pathology (LPF), the assessment focuses on the evaluation of difficulties in differentiating self from others, the dynamics of self-esteem regulation, and problems in interpersonal relationships. Once this foundation is established, the clinician is interested in the specific maladaptive personality tendencies of Criterion B (maladaptive traits) to better understand how PD manifests. However, the clinician's goal is not only to assess whether the patient meets PD criteria, but rather to integrate all data about his or her functioning with his or her history, taking into account personal, contextual, predisposing, maintaining, protective, and precipitating factors to formulate a comprehensive conceptualization of the patient’s situation and a treatment proposal (Carr, 2006).
To achieve this goal, the assessment utilizes a combination of psychodiagnostic measures (clinical interviews, observer ratings, self-report, and other psychodiagnostic tools). While the classification criteria are already helpful for many clinicians (Waugh et al., 2017), in this paper, we present a developmental approach to diagnostics that not only refers to the overall development but also to the different stages of PD development.
At each stage of development, the
A widely used method in clinical psychological assessment that combines the flexibility of an unstructured interview with the consistency of structured interviews is the
Some of the characteristics of Criterion A can be observed before adolescence (e.g., empathy, theory of mind, self-concept, self-esteem, and self-directedness), but these components are not thought to “bind together” until adolescence (McAdams, 2015; McAdams & Olson, 2010). Prepubescent and preschool children are assessed with significantly higher reliability for temperamental traits, which are considered relatively stable and manifest in extreme forms as internalizing or externalizing problems (Criterion B) (Sharp et al., 2022). For this purpose, the clinical interview and observations can be supplemented by
In adolescence, the components of Criterion A merge into a unidimensional severity criterion, and this developmental time provides an opportunity to assess whether the personality is adequately “bound” (Sharp & Wall, 2021). While high levels of maladaptive traits alone are not sufficient to diagnose PD in preadolescence, assessment of the components of Criterion A provides the opportunity to determine whether personality can occur (Sharp et al., 2022). There are a variety of psychodiagnostic instruments for assessing Criteria A and B, which have been systematically organized and presented to date (Sharp & Wall, 2018). Among the most useful for the assessment of LPF in adolescents and young adults are Assessment of Identity Development in Adolescence (AIDA; Sharp et al., 2023), ICD-11 Personality Disorder Severity Scale (PDS-ICD-11; Clark et al., 2021), The Levels of Personality Functioning Questionnaire (LOPF-Q 12-18; Goth et al., 2018), Level of Personality Functioning Scale—Brief Form 2.0 (LPFS-BF 2.0; Wu et al., 2024), and the aforementioned SCID-5-AMPD (Bender et al., 2018).
In addition to the developmental age, the choice of assessment battery also depends on the clinical severity of the personality dysfunction. Based on the AMPD and the ICD-11, Sharp and colleagues (2022) have developed a battery for the assessment of PD in children and adolescents. In
Because assessment can also be complicated by the fact that the characteristics that define a PD are often ego-syntonic and may not be seen as problematic by patients (American Psychiatric Association, 2022), the use of
In addition, the assessment of PD can be supplemented by the use of
Psychodiagnostic tools for the assessment of personality disorders vary in terms of reliability and validity. For example, the SCID-5-AMPD, a structured interview for assessing Criteria A and B, demonstrates excellent interrater and test–retest reliability (Ohse et al., 2023). Self-report inventories like the AIDA showed strong internal consistency and suitable correlations with other self-report measures of personality pathology; moreover, it could successfully discriminate between adolescents with and without BPD (Sharp et al., 2023). Similarly, LoPF-Q 12–18 revealed good internal consistency and construct validity and provided clinical cut-offs (Kerr et al., 2022). Even the briefest measure of level of personality functioning, LPFS-BF 2.0, with only 12 items, has proven to be a unidimensional factor structure, high internal consistency (α = .93), good convergent validity with similar longer measures, and significant incremental prediction psychometrically sound instrument for youth and adolescents, demonstrating a of borderline features, as well as internalizing and externalizing pathology (Wu et al., 2024). In children and adolescents, direct behavioral observation procedures—such as the Direct Observation Form from the ASEBA system—have shown internal consistency with mean alpha .74, interrater reliabilities from .71 to .97. Similarly, the empirically based scales from CBCL, YSR and TRF demonstrate high internal consistency (α = .71–.97), good test–retest reliability from .87 to .95 and strongly supported content, criterion and construct validity (Achenbach & Rescorla, 2001). Nonetheless, even with well-established psychometric properties, assessment outcomes in PD diagnostics may be affected by interpersonal dynamics, such as self-presentation tendencies of patients and variability in clinicians’ interviewing approaches (Hopwood et al., 2008; Swales, 2022). For this reason, final decisions regarding the presence of a PD should rely on the clinician’s integrative judgment, combining interview data, psychometric results, behavioral observations, and developmental history. This underlines the essential role of clinical experience and training in ensuring accurate diagnosis.
Decision for Diagnosis and Disclosure
As the detection rate is much lower than the clinical-epidemiologic data suggest, a considerable number of professionals still encounter difficulties in the diagnosis and disclosure of PD in minors (Chanen et al., 2022; Laurenssen et al., 2013). This is often attributed to the perception of PD as a lifelong disease, when patients are categorized as difficult and outside the scope of therapeutic intervention (Sharp, 2017). In addition, some phenomena typical of PD also occur in adolescence, and family and clinicians may mistakenly assume that patients outgrow them (APA, 2022; de Clercq et al., 2009; Wright et al., 2011). Some clinicians also adhere to the notion that people with PD are unable to accept or understand their diagnosis.
However, early detection and treatment of PD is critical as the estimated prevalence increases from 1% to 3% in the general population to 11%–22% in the outpatient and 33%–49% in the inpatient psychiatric population (Chanen & McCutcheon, 2013), while the cumulative prevalence in the population aged 14–22 years is more than 25% (Johnson et al., 2008). It is the fourth leading cause of disease burden among all mental disorders and is associated with high levels of stress, increased rates of current psychopathology including psychoactive substance use, self-harm and attempted suicide, low quality of life, poor physical health, poor functional and academic outcomes, increased risk of psychotic and hypomanic symptoms, interpersonal and domestic violence, and premature mortality (Chanen et al., 2022; Wertz et al., 2020). These problems persist for at least two decades (Winograd et al., 2008), while people with PD are stigmatized (Sheehan et al., 2016).
Given the impact of PD on young people (risk of developing psychotic and hypomanic symptoms, self-harm, risk of premature death, and poorer academic and functional life outcomes) (Winsper et al., 2020), facilitating early diagnosis and early intervention programs is critical. Accurate diagnosis and disclosure to patients, accompanied by comprehensive information sharing and psychoeducation, is a critical first step in the management and treatment of PD, is beneficial to patients, and should be provided in a timely manner (Chanen et al., 2017, 2022; Chanen & McCutcheon, 2013). Many patients report that they experience relief when they receive appropriate psychoeducation and clarification of the possible reasons for their interpersonal difficulties. Young patients in particular may have already self-diagnosed via the internet or social media.
The practice of early diagnosis of PD, from the age of 12, is useful (Wertz et al., 2020). It is particularly important to diagnose and disclose information in adolescence, as the personality is still developing at this stage, their brain and mental schemata are still malleable, and there are therefore more opportunities for successful interventions. In addition, certain interventions can target the adolescent’s environment, including parents, teachers, and other significant others who can support processes that are critical to a more favorable outcome in personality development, such as mentalization, identity formation, and support in achieving personal goals and lasting interpersonal relationships.
Disclosing this diagnosis to patients and families requires a higher level of sensitivity than simply telling them that they have, for example, a bacterial ear infection. It is important to adhere to the fundamental principles of disclosure, which, as in clinical medicine, are subject to the rules for communicating serious news (Cleary et al., 2009). This means that sufficient time should be allowed to enable effective communication. The information should be communicated in person, not just through a written report, in an appropriate setting, with only those relatives whom the patient trusts (and to whom they allow disclosure) present. Disclosure is likely to elicit an emotional response from the person, which should be responded to with empathy and an appropriate pace of follow-up information (Cleary et al., 2009). It is advisable to provide basic psychoeducation that allows the patient to gain insight into the diagnosis and better understand the associated symptoms, behaviors, and emotional issues, allowing for a more coherent understanding of their experience (Gunderson, 2014). Disclosure of the diagnosis, if performed appropriately, can serve as an initial therapeutic intervention that facilitates the patient to understand their problems, alleviate feelings of guilt, develop compassion for themselves, and construct a more insightful account of their life. Furthermore, it can prevent additional diagnostic procedures and thus the additional burden on the patient, the family, and the health care system. The patient’s understanding of the diagnosis also helps to reduce stigma, increase motivation and commitment to treatment, and strengthen psychological autonomy and the therapeutic relationship (Fonagy & Allison, 2014; Gunderson, 2014). We have argued that the disclosure of PD in young people is destigmatized when using LPF language to describe a young person’s problems (Sharp & Bevington, 2022). For instance, we have assessed your personality functioning and our assessment shows that you struggle to make sense of yourself and your relationships, and this causes problems for you because it gets you into trouble with others, and makes you feel sad and lonely.
This way of talking about personality functioning as devoid of unfixable traits (“you are a very emotional person who shows strong reactivity to interpersonal situations”) focuses on malleable treatment targets and in our view is a more destigmatizing way to disclose a PD diagnosis to young people and their families: “You have come for help at exactly the right time; you are still putting together the pieces of who you are as person and things and I’m so happy that I can help you in this journey.” Instilling hope with young people and families who have been in and out of psychiatric services for years, we consider to be a critical part of disclosing the diagnosis.
Recommendations for the treatment of the problem, details of possible therapeutic measures and other relevant information should then be given. It is important that the patient feels supported on their road to recovery. This may mean giving them information about further credible treatments or referrals to an appropriate specialist, or giving them sufficient information to manage their condition themselves in the future. It is also crucial to set realistic expectations for treatment and emphasize that the focus is on improving quality of life, reducing self-destructive behaviors, and promoting positive interpersonal relationships, rather than expecting a complete cure (Gunderson, 2014).
Prevention and Treatment
The diagnosis of PD in adolescents and the identification of at-risk children provide an opportunity for prevention and the development of evidence-based interventions, both of which lead to healthy personality development, reduced impairment, and improved functioning. According to the clinical staging model, interventions should be adapted to the level of personality dysfunction and be proportionate to the presenting clinical picture.
It is important to start prevention early, address parenting skills, and focus on mitigating the adverse effects of interactions between children with difficult temperamental traits and their parents. It makes sense to introduce these interventions as early as possible, that is, at
In
In
Early identification and interventions should be encouraged through developmental strategies and awareness raising, involving family and friends as collaborators. Educational and skill development programs should be available for families of youth with PD and should be a top priority for treatment research. Early interventions should also focus on identifying risk factors for the continuation or exacerbation of problems, rather than waiting for the »onset« of PD. As adolescence is a crucial developmental period for personality development, preventive measures should improve mentalization skills during adolescence and focus on slowing down thinking and feeling in relation to oneself and others. This provides guidance in making important decisions on the journey from adolescence to adulthood and enables the development of an adaptive and integrated sense of self (Sharp, 2020).
In the higher stages (
Despite the remaining dilemmas, it is clear that interventions to treat PD should be prevention-oriented, used early, based on different approaches, and, most importantly, feasible with skills that are widely available in mental health services and can be easily scaled up across the health system (Chanen et al., 2022).
Various presented manualized treatments have some common critical therapeutic elements for successful outcomes. These include a strong therapeutic alliance, empathy, goal consensus and collaboration, positive regard and affirmation, mastery, congruence/genuineness, mentalization, a developmentally sensitive approach, and emotional experience as shown in meta-analyses (Nahum et al., 2019). Different approaches also share common features, such as psychoeducation and a focus on psychosocial recovery (Chanen, 2015; Clarkin et al., 2007; Farrell et al., 2009). Evidence suggests that no single approach is universally superior; rather, effectiveness depends on how well the treatment is delivered and how well it matches the adolescent’s developmental stage, understanding the severity of dysfunction and clinical needs. This is why the clinical staging model is particularly useful—it allows clinicians to tailor interventions to the individual’s needs, from early prevention to intensive psychotherapy. Furthermore, incorporating a socioecological approach that actively engages the adolescent’s broader environment (family, school, and social networks) can significantly enhance treatment effectiveness and long-term outcomes (Bo et al., 2022).
Conclusions
After many years, the concept of PD in adolescence is finally being understood through a developmental lens with the availability of the LPF assessment. Maladaptive personality development is now widely researched and proven to be at the core of personality pathology, which is well described by the prominent symptoms of BPD. Using a developmental perspective, staging of clinical severity and considering various risk and protective factors offers virtually unlimited possibilities for general and targeted prevention in the population and treatment of at-risk youth. By applying the dimensional model, there is an opportunity to change the developmental trajectory and significantly reduce the overall burden of adult PD in the future.
Footnotes
Acknowledgements
A more condensed version of the same article was published in ISSBD Bulletin in 2024 (Drobnič Radobuljac & Sharp, 2024).
Ethical Approval
Ethical approval was not required for this work.
Author Contributions
CS and MDR conceived the work, SK drafted the article, CS and MDR revised it critically for important intellectual content, all authors read and approved the version to be published and agree to be responsible for all aspects of the work and to ensure that issues related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Maja Drobnič Radobuljac is the recipient of funding from the Slovenian Research Agency (grant numbers P3-0343 and J3-4534). Simona Klemenčič is the recipient of funding from the Slovenian Research Agency (grant number P3-0343).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
No original data was used for this manuscript.