
Abstract
Theorized mechanisms linking views on aging, self-regulation, and well-being have not previously been examined longitudinally. This study considers goal re-engagement as a potential mediator of longitudinal relationships between awareness of age-related change (AARC) and vitality. We expected that more positive perceptions of aging (i.e., higher AARC-gains and lower AARC-losses) at Time 1 (T1) would be associated with increases in goal re-engagement and, in turn, increases in vitality. We also examined possible moderating effects of age on associations of AARC with goal re-engagement and vitality. A sample of 408 middle-aged and older adults (60 years and over) completed three online assessments capturing AARC (gains and losses), goal re-engagement, and vitality over a 12-month period. Parallel process latent growth models were used to test for mediation. Associations among variable intercepts revealed that more positive views of aging were associated with higher levels of goal re-engagement and greater vitality. However, there was no support for the longitudinal mediation hypotheses, with T1 levels of AARC showing negligible associations with rates of change in goal re-engagement and vitality. Moderation analyses revealed a stronger association of T1 AARC-gains with the intercept for goal re-engagement at older, relative to younger ages. Although growing evidence supports cross-sectional links between views on aging, self-regulation and well-being, research with longer measurement intervals and a more comprehensive array of potential mediators is needed to conclusively identify underlying mechanisms.
Introduction
Throughout life, people form beliefs about aging in general, as well as their own experience of aging (Kornadt et al., 2020). While views on aging impact development across the lifespan, they become increasingly self-relevant in middle-age and older adulthood (Diehl & Wahl, 2010; Fry & Keyes, 2010). Relatively recently in the subjective aging literature, Diehl and Wahl (2010) developed the construct of awareness of age-related change (AARC), which refers to ‘a person’s state of awareness that [their] behavior, level of performance, or way of experiencing life has changed as a consequence of having grown older’ (p. 342). In contrast to most previous subjective aging measures (for an exception see Steverink et al., 2001), AARC distinguishes between positive (AARC-gains) and negative (AARC-losses) dimensions of subjective aging. There is now a substantial body of research showing that greater levels of subjective, psychological, and physical well-being are linked to higher AARC-gains and lower AARC-losses (Brothers et al., 2016; Dutt et al., 2018a; Sabatini et al., 2020). However, less is known about the cognitive and behavioral processes through which awareness of aging could exert an influence on well-being. In this study, we examined longitudinal associations among AARC, goal re-engagement (an index of tendencies toward effective self-regulation), and vitality in a sample of adults aged 60 and older who completed three surveys over a 12-month interval.
AARC, Regulation of Goals, and Well-Being
In Diehl and Wahl’s (2010) original model of AARC, self-regulation of behavior is identified as a set of intervening processes through which AARC influences health, engagement, and well-being. As a specific form of self-awareness, AARC is presumed to inform intentions and actions surrounding goals and goal striving (Baltes, 1997). Older adults often effectively adjust personal goals to maximize opportunities for developmental gains and reduce the occurrence of developmental losses (Baltes, 1997; Heckhausen & Schulz, 1995; Rothermund & Brandstadter, 2003; Wrosch et al., 2003). According to Diehl and Wahl (2010), AARC may prompt processes of personal meaning-making and self-regulation, with individuals contrasting their current performance with their past performance or the performance of others, which in turn informs processes of goal adjustment (Wrosch et al., 2007) in efforts to stabilize one’s sense of self (Greve & Wentura, 2003). For example, in older adulthood, one may choose to take a step back from participating in physically demanding activities in response to functional limitations and choose to pursue alternative goals (e.g., participating in less demanding but equally satisfying activities). Detaching from, and devaluing unattainable goals (goal disengagement), and redirecting energy and resources toward achievable goals (goal re-engagement) are both important self-regulatory processes (Wrosch et al., 2003) that increase in their importance in older adulthood, due to the shifting balance of developmental gains and losses (Brandtstadter & Renner, 1990).
Some research evidence provides indirect support for Diehl and Wahl’s (2010) model, demonstrating associations of views on aging with self-regulatory behavior. For example, Wurm et al. (2013) found that older adults who experienced a negative health event were more likely to engage in adaptive self-regulatory strategy use, but that this tendency was weaker among those who perceived aging as characterized by physical loss. Recently, studies have begun to examine associations of self-regulatory tendencies with views on aging using Diehl and Wahl’s (2010) multidimensional AARC framework. More frequent use of adaptive goal regulation strategies has been linked to higher AARC-gains and lower AARC-losses (Dutt et al., 2018b; Wilton-Harding & Windsor, 2022). AARC-gains may foster feelings of self-efficacy (Bandura et al., 1999) and competence (Ryan & Deci, 2000), facilitating ongoing engagement in activities (Windsor et al., 2022). Conversely, AARC-losses may undermine personal agency and reduce motivation (Dutt et al., 2018b).
Just as associations between views on aging and self-regulation have been reported previously, there is also substantial evidence supporting links between self-regulation and well-being. For example, a meta-analytic review found that tendencies toward re-engaging with new goals in the face of unattainable goals was associated with higher positive and lower negative aspects of well-being, whereas the tendency to flexibly disengage from blocked goals was associated with lower negative aspects of well-being (Barlow et al., 2020). More recently, positive longitudinal associations have been reported between positive affect, life satisfaction, and sense of purpose with goal re-engagement (Haase et al., 2020), and a longitudinal study conducted across the early months of the COVID-19 pandemic found a positive within-person association of goal re-engagement with perceived control (Hamm et al., 2023).
Regulation of Goals as a Precursor to Awareness of Aging
As outlined above, in Diehl and Wahl’s (2010) conceptual framework, awareness of aging informs self-regulatory behavior and cognition, which in turn influence well-being. However, it is also plausible that people’s experience of self-regulatory processes could have implications for the ways in which they view their own aging. According to the motivational theory of lifespan development (Haase et al., 2013; Heckhausen & Wrosch, 2016), central to human motivation and adaptation is the capacity to exert control over the environment (primary control) while adjusting the self (e.g., changing self-expectations) in ways that facilitate goal attainment and preserve primary control. One’s experiences in exercising agency translate into mental representations of the self. Consequently, secondary control strategies such as attributing failure to external causes, or downward social comparison, can help to preserve motivation and self-image. Indeed, individual differences in self-regulatory skills mean that those less capable of flexible adaptation in terms of goal regulation are more prone to poor well-being outcomes (Heckhausen & Wrosch, 2016). It follows, that in later life when developmental losses in some domains (e.g., health, cognition) begin to accrue, it may be the most effective self-regulators who are best placed to recognize AARC-gains and avoid AARC-losses. Diehl and Wahl (2010) note that “experiences in everyday life (e.g., age-based stereotyping) create situations in which individuals are reminded of their chronological age” (p. 347). Alternative developmental processes have also been suggested. More specifically, Dutt et al. (2018b) describe how processes of successful goal regulation could promote positive subjective aging experiences, sustaining higher AARC-gains and lower AARC-losses.
Consistent with Diehl and Wahl’s (2010) original framework, and the conceptual orientation of previous studies in the area (Wilton-Harding & Windsor, 2022), we focused on examining AARC as a predictor of changes in goal re-engagement, and in turn, well-being, operationalized as vitality. However, recognizing the plausibility of the alternative causal pathway described above, we also examined whether goal re-engagement predicted subsequent changes in AARC and, in turn, vitality.
The Present Study
We used parallel process latent growth models (PP-LGM; Cheong et al., 2003) to examine temporal associations between AARC, goal re-engagement, and vitality. Although flexible self-regulation combines processes of both goal disengagement and re-engagement (Wrosch et al., 2003), consistent with Hamm et al. (2023), we focused just on goal re-engagement tendencies in this study, as it offers a less-ambiguous marker of self-regulatory potential than goal disengagement (e.g., a tendency to disengage from achievable goals prematurely may reduce developmental potential) and previous studies have reported more consistent associations of goal re-engagement with indices of well-being (Barlow et al., 2020; Haase et al., 2020).
We assessed well-being using vitality, a marker of enthusiasm defined as “one’s conscious experience of possessing energy and aliveness” (Ryan & Frederick, 1997, p. 530). Vitality is regarded as a key marker or organismic wellness and functionality, as opposed to simply the presence and/or absence of ill-being and disease (Lim, 2023). While cultural views of aging often focus on decline and loss, feelings of vitality may reflect tendencies to find fulfillment, flourishing, and personal growth in older adulthood (Laceulle & Baars, 2014). Having energy available to the self for continued development when losses are experienced has been identified as an important resource for adaptative capacity and resilience (Baltes & Smith, 2003; Smith & Ryan, 2016), yet vitality is a relatively understudied component of adaptive aging (American Psychological Association, 1996; Cardini & Freund, 2020; Erikson et al., 1986). Vitality is thought to be an important driver of self-regulatory potential (Cardini & Freund, 2020), and has been found to predict falls in older women independently of physical health (Burns et al., 2012).
We predicted that goal re-engagement would mediate associations between AARC and vitality. Specifically, we predicted that participants reporting higher AARC-gains at Time 1 (T1) would show more positive (or less negative) rates of change in goal re-engagement over the study interval, and that changes in goal re-engagement would be positively associated with changes in vitality. Similarly, we predicted that those with higher AARC-losses at T1 would show relatively more negative longitudinal changes in goal re-engagement over time, and that changes in goal re-engagement would be positively associated with changes in vitality. We also re-specified the parallel mediation models to explore the alternative possibility that goal re-engagement at T1 predicts rates of change in AARC and, in turn, vitality.
Finally, we included moderation analysis to assess whether key associations of interest varied as a function of chronological age. Because aging-related losses become more normative in late life (Baltes & Smith, 2003), it is possible that with increasing age, an associated awareness of losses may be more likely to result in a degree of acceptance and reduced goal re-engagement than is the case in young-old adulthood, when experience of losses is less normative and potentially more threatening to one’s sense of self (Dutt et al., 2018b). In their cross-sectional analysis, Dutt et al. (2018b) did not find evidence of age moderating associations of AARC with self-regulatory tendencies. Our longitudinal data provided the opportunity to further interrogate possible age moderation. We tested the hypothesis that negative associations of AARC-losses with goal re-engagement would be weaker among older, relative to younger participants.
Method
Study Design and Participants
Following approval from the Flinders University Ethics Committee [project ID 1921], an advertisement was placed on CloudResearch, an online crowdsourcing platform (Litman et al., 2017), inviting American workers who met eligibility criteria (aged over 60 years, completed > 100 previous studies, with participation approval ratings greater than 95%) to participate in a 15-min online study focused on coping and well-being across the lifespan in July 2019. Participants (N = 408) were invited to complete follow-up surveys approximately 6 (N = 361; January 2020) and 12 (N = 311) months later (July 2020).
At T1, participants were aged between 60 and 88 years (M = 67.07, SD = 4.57). Just under two-thirds (65.9%) of participants were female (34.1% male, 0% non-binary), and 53.5% were retired. More than half of the participants reported completion of tertiary education (58.3%), 49.6% were partnered, and 90% identified as Caucasian (5% African American, 2% Asian American, 3% other). Simulation data reported by Cheong (2011) indicate that when assuming a substantial proportion of variance (R2 = .8) in measured variables is accounted for by the growth factors and using asymmetric confidence intervals to assess significance of an indirect effect, a sample size of N = 400 is sufficient to detect a mediation effect of medium magnitude with power > 0.8.
Measures
AARC
The AARC-10 SF (Kaspar et al., 2019) was used to assess perceptions of aging across two subscales (AARC-gains and AARC-losses). Participants responded to items regarding how their life may have changed due to growing older (e.g., “‖ I have more experience and knowledge to evaluate things and people”). Scores for each subscale were summed, with higher scores reflecting greater AARC-gains and AARC-losses, respectively. Cronbach’s α ranged between .69 and .74 for AARC-gains, and between .82 and .84 for AARC-losses across the three time points.
Goal Adjustment
Using the six-item goal re-engagement subscale from the Goal Adjustment Scale (Wrosch et al., 2003), participants rated their agreement with statements regarding how they respond when they must stop pursuing an important goal (e.g., “I seek other meaningful goals”). Scores were summed, with higher scores reflecting higher goal re-engagement tendencies (α range = .84–.87).
Vitality
The Subjective Vitality Scales (Boerner, 2004; Brandtstadter & Renner, 1990; Steptoe et al., 2015) were used to assess vitality. Participants indicated their agreement to six statements concerning their levels of energy and enthusiasm (e.g., “I look forward to each new day”) on a scale from 1 (not at all true) to 5 (very true). Scores were summed, with higher scores reflecting greater subjective vitality (α range = .92–.93).
Covariates
Models were adjusted for chronological age, gender (male = 0, female = 1), education (0 = did not complete tertiary education, 1 = did complete tertiary education), and physical functioning, due to previous associations with subjective aging, goal adjustment, and well-being (Boerner, 2004; Brandtstadter & Renner, 1990; Steptoe et al., 2015). Physical functioning was measured with the 10-item physical functioning subscale from the RAND health survey (M = 70.96, SD = 26.55, range: 0–100, with higher scores reflecting better physical functioning; Ware & Sherbourne, 1992). We also controlled for labor force status (0 = not in the labor force; 1 = in the labor force) as a substantial proportion of the sample were employed (see Table 1). When analyzing effects of AARC-gains or AARC-losses, the alternate AARC subscale was included as a covariate to isolate the unique effects of each dimension.
Descriptive Statistics and Correlations Among Study Variables at Baseline.
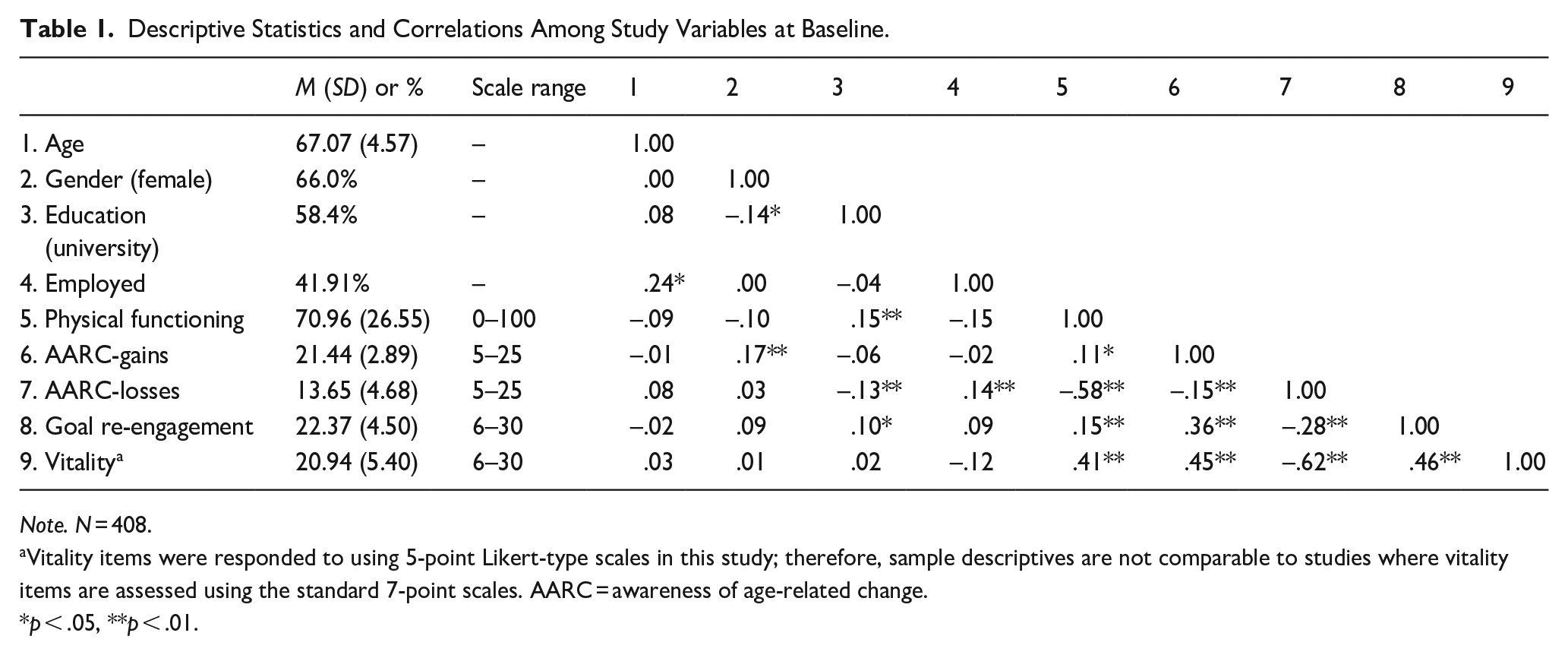
Note. N = 408.
Vitality items were responded to using 5-point Likert-type scales in this study; therefore, sample descriptives are not comparable to studies where vitality items are assessed using the standard 7-point scales. AARC = awareness of age-related change.
p < .05, **p < .01.
Statistical Analysis
Our main analyses were conducted in a Structural Equation Modeling framework using Mplus 8 (Muthén & Muthén, 1998). PP-LGMs (Cheong et al., 2003) were fitted to first examine goal re-engagement as a mediator of associations between (T1) AARC and vitality. The model was then re-specified to examine AARC-gains and AARC-losses as potential mediators of associations between (T1) goal re-engagement and vitality. A diagram of the model used to test the hypothesis that goal re-engagement would mediate the association between AARC-gains and vitality is shown in Figure 1 (equivalent models were fitted with T1 AARC-losses as the independent variable, as well as a T1 goal re-engagement as the independent variable with AARC-gains and AARC-losses as mediators). Here, parallel growth processes are modeled to represent levels (the intercept) and rates of change (the slope) in the mediator (M) and the outcome (Y). The independent variable, X (in this case, AARC-gains) includes the T1 assessment. For testing mediation, the key parameter of interest is the indirect effect of the independent variable on rates of change in Y, via its effect on rates of change in M (a*b). The significance of indirect effects was estimated using bias-corrected 95% bootstrapped (5000 samples) confidence intervals (Zhu et al., 2021). The intercepts and slopes of M and Y were regressed on the covariates (not shown in Figure 1), and latent intercept and slope factors that were not associated via directional regression paths were allowed to correlate. When modeling AARC-gains as the independent variable, AARC-losses was controlled for (and vice versa).
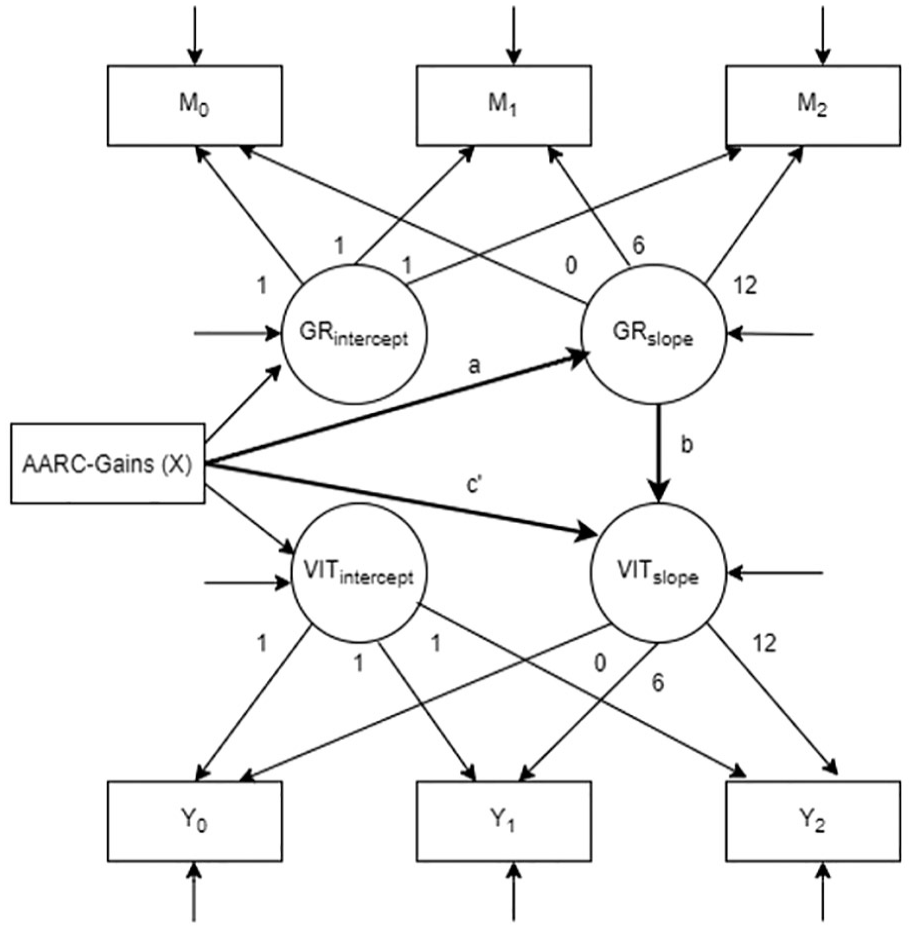
Diagram of PP-LGM Used to Test Goal Re-Engagement as a Mediator of the Association Between AARC-Gains and Vitality.
Following the tests of mediation, cross-product terms (age × independent variable) were included in the models to test whether paths from each specified independent variable to the intercepts and slopes of the corresponding growth factors varied as a function of age. To assess model fit, we considered the root mean square error of approximation (RMSEA; where values lower than 0.06 reflect good fit), the comparative model fit index (CFI; where values greater than 0.95 reflect good fit), and the chi-square test of model fit (where low, non-significant values indicate good fit; Hoyle & Panter, 1995). Missing data (11.8% of the total data set) were handled under full information maximum likelihood estimation.
Results
Results are reported in four steps. First, we describe associations among all study variables at T1, and report intercorrelations among the main study variables over time. Second, we report results of univariate growth models to describe patterns of mean-level stability and change over time. Third, we report results of the PP-LGMs used to test our main mediation hypotheses. Finally, we report tests of age moderation on associations of AARC with levels and rates of change in goal re-engagement and vitality.
Descriptive Statistics and Bivariate Associations
Descriptive statistics and the bivariate associations among the study variables at T1 are shown in Table 1. AARC-gains and AARC-losses were weakly and negatively correlated. Several moderate correlations (rs .3 to .6) were evident, with better physical functioning associated with lower AARC-losses and higher vitality, higher AARC-gains associated with higher vitality and higher goal re-engagement, higher AARC-losses associated with lower vitality, and higher goal re-engagement associated with higher vitality. Table 2 shows intercorrelations among the key study variables over the three measurement occasions. In general, rank-order stability was relatively high for the AARC measures and vitality with test-re-test correlations T1–T2 ranging from .72 to .78, T2–T3 ranging from .73 to .84, and T1–T3 ranging from .72 to .81. Rank-order stability was more moderate for goal re-engagement; T1–T2 r = .54, T2–T3 r = .52, T1–T3, r = .55.
Intercorrelations Among AARC, Goal Re-Engagement and Satisfaction With Life Over Time.
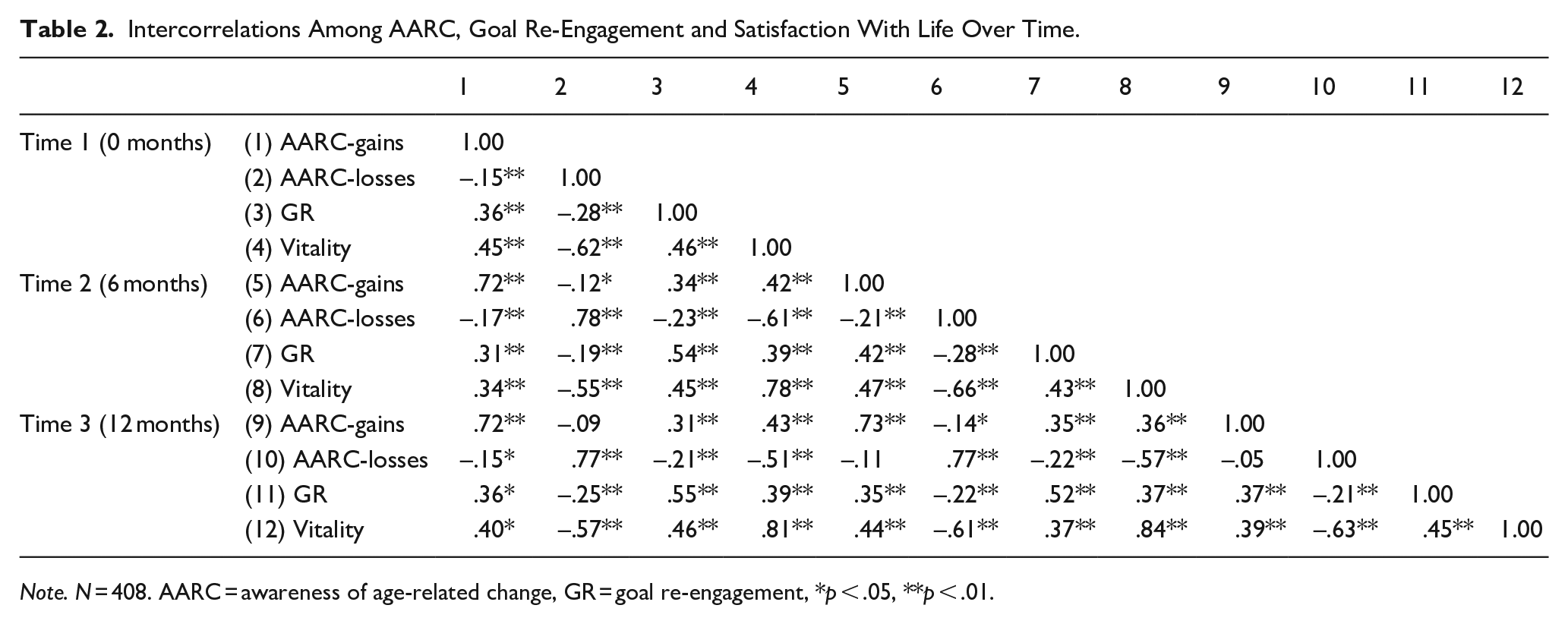
Note. N = 408. AARC = awareness of age-related change, GR = goal re-engagement, *p < .05, **p < .01.
Univariate Growth Curve Models
Results of growth curve models used to describe changes in AARC, goal re-engagement and vitality over the 12-month study period are shown in Table 3. As can be seen, participants showed small average decreases in vitality (around 0.19 SD decrease per year) and goal re-engagement (around 0.18 SD decrease per year) over the study interval. No mean-level changes were observed in AARC-losses or AARC-gains. Although significant inter-individual differences for the intercept were evident for each measure, none of the variance terms associated with the slope parameters were significantly different from zero, pointing to only small or negligible inter-individual differences in rates of change. In the case of AARC-losses, the model produced a small negative value for the slope variance, thus we fixed this parameter to zero to allow model identification.
Univariate Latent Growth Curve Model Results.
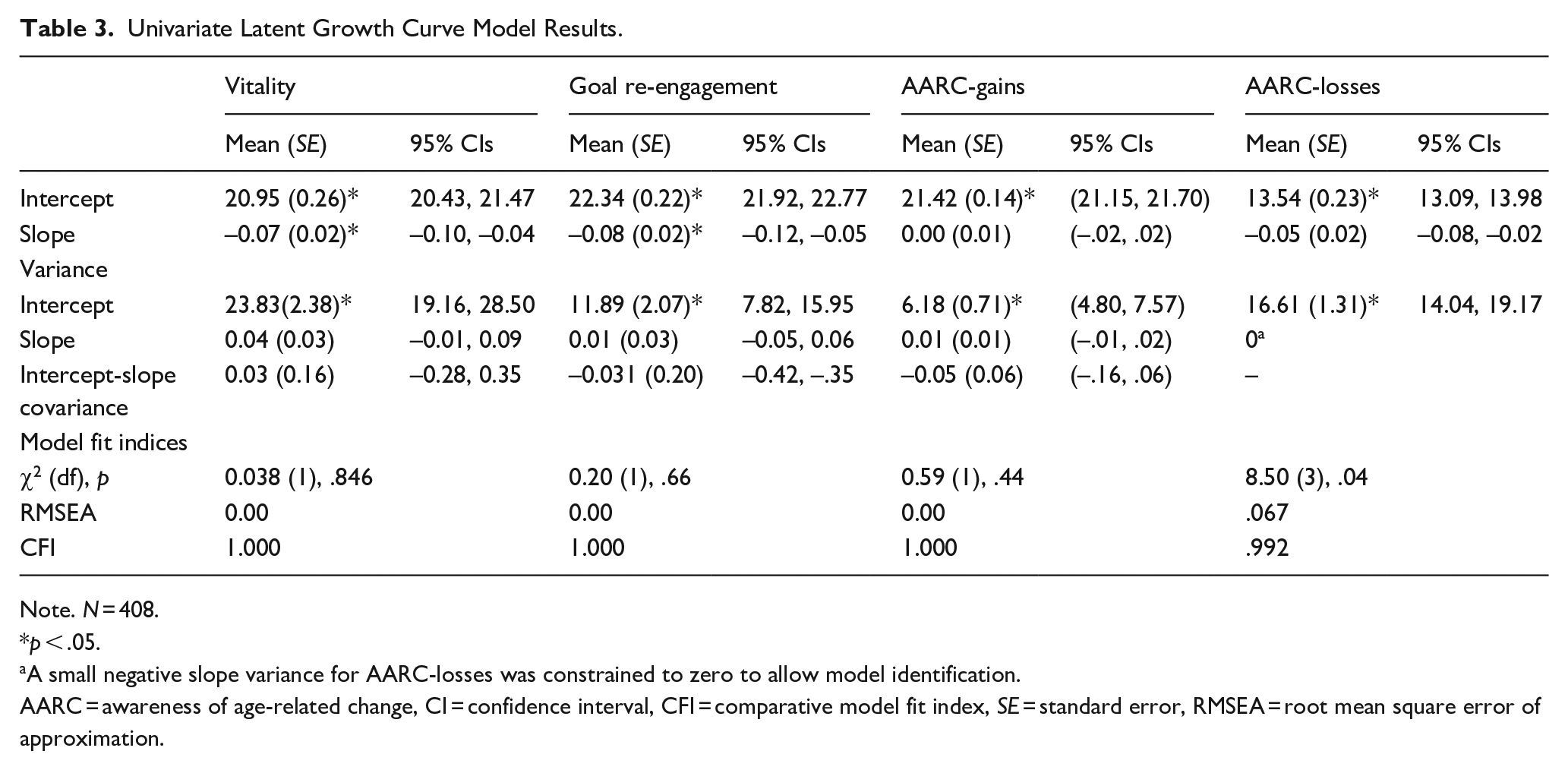
Note. N = 408.
p < .05.
A small negative slope variance for AARC-losses was constrained to zero to allow model identification.
AARC = awareness of age-related change, CI = confidence interval, CFI = comparative model fit index, SE = standard error, RMSEA = root mean square error of approximation.
Longitudinal Mediation Analysis
Results of PP-LGM models used to test our first mediation hypotheses (AARC→goal re-engagement→vitality) are shown in Table 4. As both AARC subscales were included in each model (i.e., as the predictor or as a covariate), estimates between AARC, goal re-engagement, vitality and covariates were consistent across both models. To avoid repetition, both models which include AARC as the independent variable (i.e., gains and losses) are presented in Table 4. The only differences in these two models are the tests of indirect effects (i.e., tests of mediation).
Parallel Process Latent Growth Models Testing Mediation Pathways Linking AARC With Vitality With Goal Re-Engagement as Mediator (Model 1) and Age as a Moderator of Associations of AARC-Gains and AARC-Losses With Goal Re-Engagement and Vitality (Model 2).
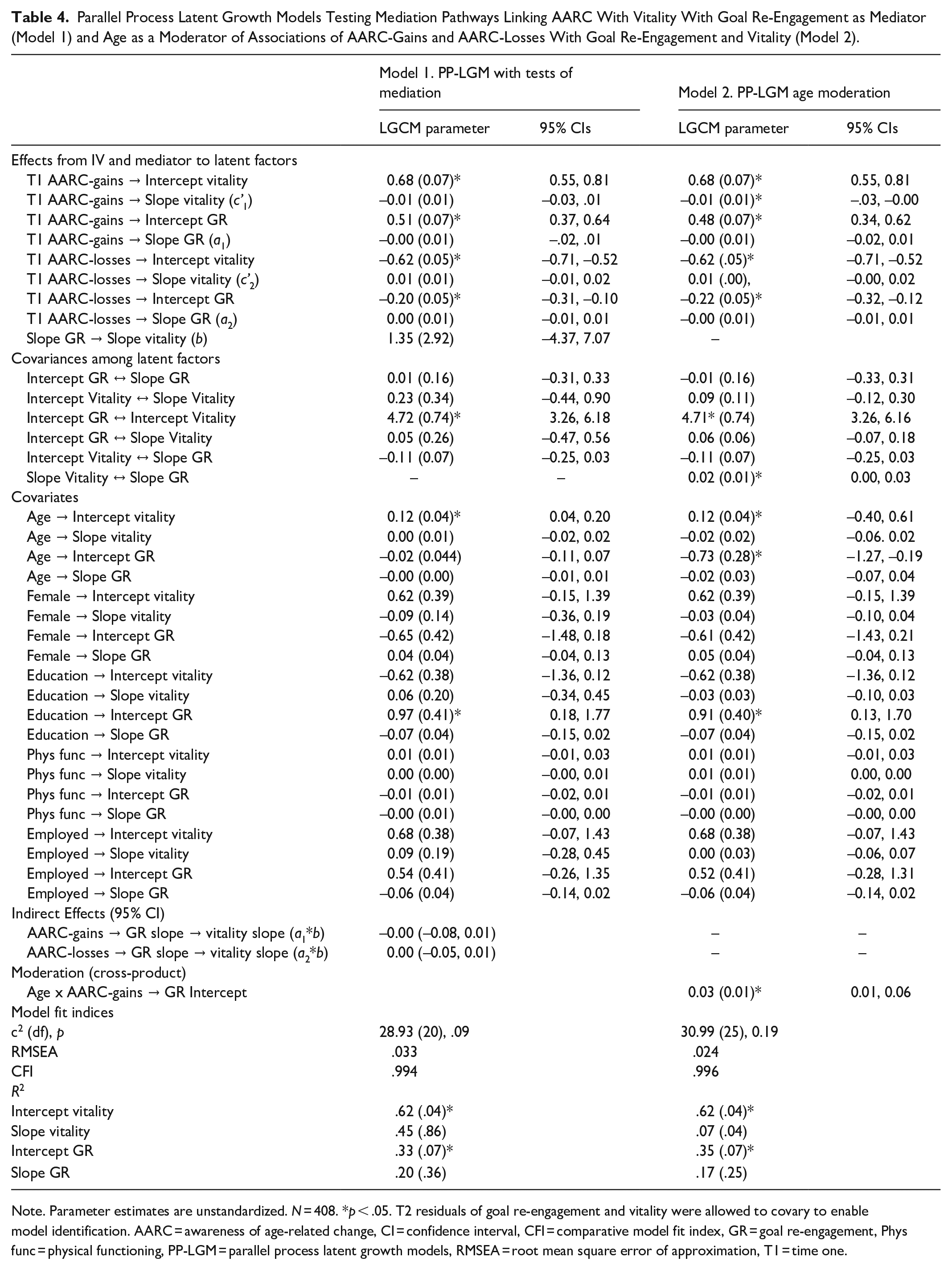
Note. Parameter estimates are unstandardized. N = 408. *p < .05. T2 residuals of goal re-engagement and vitality were allowed to covary to enable model identification. AARC = awareness of age-related change, CI = confidence interval, CFI = comparative model fit index, GR = goal re-engagement, Phys func = physical functioning, PP-LGM = parallel process latent growth models, RMSEA = root mean square error of approximation, T1 = time one.
Focusing first on the model that included AARC-gains as the independent variable and goal re-engagement as the mediator (Table 4, also see Figure 1), positive associations were evident between T1 AARC-gains and the intercepts for both goal re-engagement and vitality. This indicates that participants with higher AARC-gains at T1 also tended to show higher overall levels of goal re-engagement and vitality. The covariance between the intercepts of goal re-engagement and vitality was also positive. Turning attention to predictors of change, the slope for vitality was not associated with either T1 AARC-gains (c’1) or rates of change (the slope) for goal re-engagement (b). AARC-gains also did not predict rates of change in goal re-engagement (a1), and the relevant indirect effect (a1*b) was not significant. Thus, there was no evidence for goal re-engagement mediating an association of T1 levels of AARC-gains with changes in vitality over 1 year. A similar pattern of findings emerged when the model was re-specified to include AARC-losses as the independent variable. AARC-losses was associated with lower levels of goal re-engagement and vitality (as indicated by negative associations with their intercepts). However, T1 AARC-losses did not predict rates of change in vitality or goal re-engagement, and the indirect effect (a2*b) was non-significant, indicating no support for the mediation hypothesis.
In addition to testing our main mediation hypotheses, alternative model specifications were tested allowing for the possibility that goal re-engagement could predict changes in AARC which, in turn, predict changes in vitality. Because the growth model for AARC-losses required the slope variance to be constrained to zero for identification (see above), we only tested longitudinal mediation for the model that included T1 goal re-engagement as the independent variable and AARC-gains as the putative mediator. Results are presented in Table 5. Associations of goal re-engagement with the intercepts showed patterns that mirrored those for the between-person associations reported above in the initial PP-LGMs. Regarding mediation, despite no reliable associations of goal re-engagement with the slopes of AARC-gains or vitality (and no association of the AARC-gains slope with the vitality slope) the 95% confidence intervals did not cross zero, indicating a significant indirect effect. However, the indirect effect was negative on account of a negative association between goal re-engagement and the AARC-gains slope (higher T1 goal re-engagement was weakly associated with a decrease in AARC-gains over the study interval). Therefore, the results did not provide support for the mediation occurring in a way consistent with the alternative postulated causal pathway that goal re-engagement could promote a more positive profile of AARC which in turn would support vitality.
Parallel Process Latent Growth Model Mediation Pathway Linking Goal Re-Engagement With Vitality With AARC-Gains as Mediator.
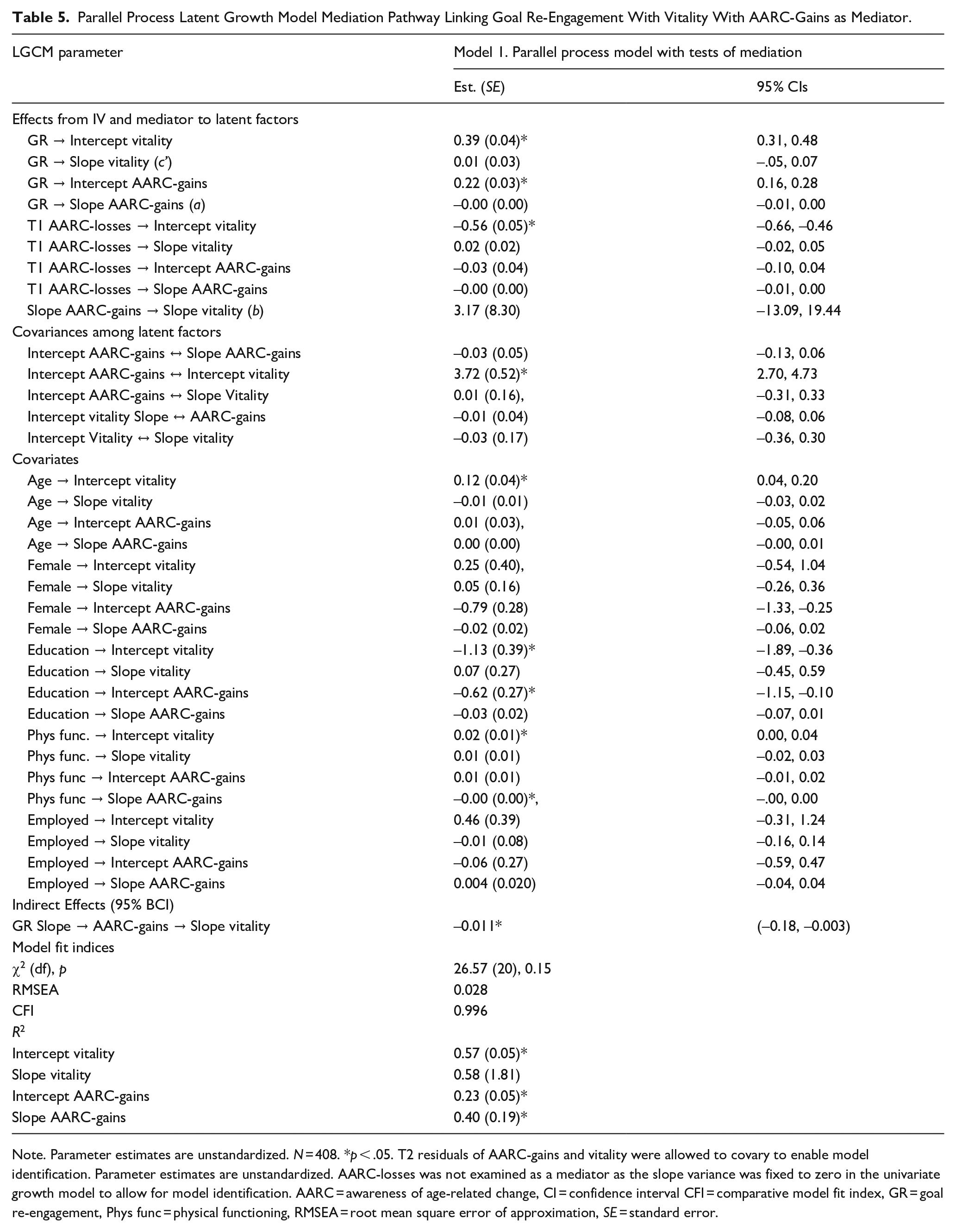
Note. Parameter estimates are unstandardized. N = 408. *p < .05. T2 residuals of AARC-gains and vitality were allowed to covary to enable model identification. Parameter estimates are unstandardized. AARC-losses was not examined as a mediator as the slope variance was fixed to zero in the univariate growth model to allow for model identification. AARC = awareness of age-related change, CI = confidence interval CFI = comparative model fit index, GR = goal re-engagement, Phys func = physical functioning, RMSEA = root mean square error of approximation, SE = standard error.
Cross-Sectional Mediation Analysis
We conducted additional follow-up tests of cross-sectional mediation, to further contextualize the findings by focusing just on between-person associations. An initial attempt to fit a parallel growth model and focus on associations among the model intercepts did not converge, hence we fitted a model that included just baseline AARC-gains and AARC-losses (IVs), goal re-engagement (mediator) and vitality (DV), with 95% bootstrapped (5000 samples) confidence intervals used to assess significance of indirect effects. Results are shown in Supplementary Table 1 and indicated a significant indirect effect of AARC-gains on vitality via goal re-engagement (a*b = 0.14, SE = 0.03) and a significant indirect effect of AARC-losses on vitality via goal re-engagement (a*b = −0.06, SE = 0.02).
Tests of Age Moderation
In our final analyses, models were re-specified with the inclusion of age × AARC interaction terms to assess whether associations of the different independent variables with intercepts and slopes of the mediator and vitality, varied as a function of age. One interaction term emerged as statistically reliable, with Age × AARC-gains predicting the goal re-engagement intercept (Table 4, Model 2). The nature of the moderation is displayed in Figure 2, which shows predicted values of goal re-engagement for older (Mean + 1 SD) and younger (Mean − 1 SD) participants scoring higher (Mean + 1 SD) and lower (Mean − 1 SD) on AARC-gains. As can been seen, participants with higher AARC-gains retained relatively high levels of goal re-engagement irrespective of age; however, among those with relatively lower AARC-gains, older age was associated with lower levels of goal re-engagement.
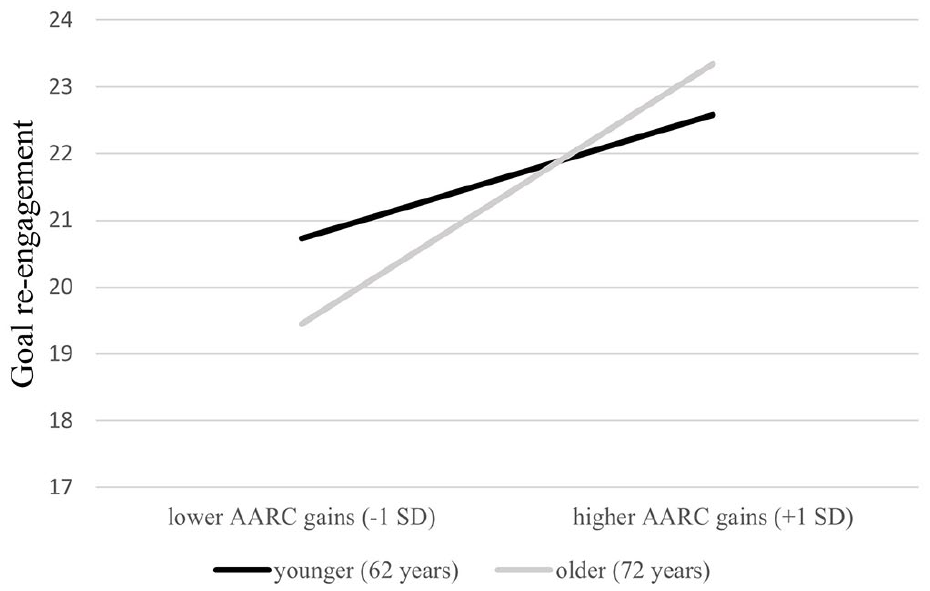
Interaction of AARC-Gains and Age in the Prediction of the Intercept of Goal Re-Engagement.
Discussion
To our knowledge, this is the first study to examine longitudinal associations between AARC, goal re-engagement, and vitality. Overall, we did not find evidence for the hypothesized mediating role of goal re-engagement in longitudinal associations between AARC (gains or losses) and vitality. Consistent with Dutt et al. (2018b) and our previous analysis of the current data set at T1 (Wilton-Harding & Windsor, 2022), associations between growth model intercepts were observed, with these associations aligning with expectations that a more positive profile of AARC (i.e., higher gains and lower losses) would be associated with both greater vitality and greater goal re-engagement. Similarly, follow-up tests of simple cross-sectional mediation using baseline data supported the predicted associations at the between-person level. However, our goal was to extend previous cross-sectional findings by focusing on goal re-engagement as a mediator of longitudinal associations between AARC and vitality. To this end, the incorporation of longitudinal data was key, as there is growing consensus that cross-sectional data are often inadequate for examining hypothesized longitudinal mechanisms (e.g., O’Laughlin et al., 2018).
There are several possible reasons for the absence of evidence for longitudinal mediation. One possibility is that the processes of subjective aging and self-regulatory change that are outlined in Diehl and Wahl’s (2010) model unfold over longer developmental periods, and a 1-year measurement interval was insufficient to observe such changes. In our data, the longitudinal stability of key constructs (especially AARC and vitality) was high. Previous research on well-being in older adults showed that while rank-order stability remained high, well-being was still subject to change in response to changing life circumstances over a relatively short time interval (3–6 months; Chamberlain & Zika, 1992). Moreover, an interval of around 1 year has been suggested as sufficient to detect meaningful changes in goal adjustment (Haase et al., 2020). Although we observed small mean-level declines in vitality and goal re-engagement in our growth models, it was telling that the slope variances for each of the key variables were small and did not differ significantly from zero. This lack of variability in rates of change over 1 year likely hampered our capacity to detect the longitudinal associations that were our focus. Thus, future examinations focusing on theorized mechanisms linking AARC with well-being may benefit from including additional assessments and a longer total study duration (Brandmaier et al., 2018).
Although it seems likely that our investigation was at least partly limited by the methodological issues discussed above, it is also important to acknowledge the possibility that goal re-engagement tendencies do not play a central role in accounting for changes in late-life vitality. For example, a recent study identified several longitudinal predictors of late-life vitality including depressive symptoms, objective and subjective markers of health, and emotional support (de Breij et al., 2021). AARC has previously been found to predict physical and mental health (Sabatini et al., 2022), and it is conceivable that subjective perceptions of aging affect aspects of mood and health which in turn impact vitality. We do, however, note that in our data, T1 physical functioning was not associated with rates of change in vitality. Ultimately, longer-term longitudinal studies that include a series of theoretically plausible mediators that can be tested in parallel may be needed to better understand mechanisms linking perceptions of aging with markers of well-being including vitality.
A significant negative indirect effect was found linking T1 goal re-engagement with changes in vitality via changes in AARC-gains. We are reluctant to place much importance on this finding, given that both the individual “a” and “b” paths whose product comprised the indirect effect were not significantly different from zero. Given that the goal re-engagement and AARC-gains intercepts were positively associated, indicating that those with higher overall goal re-engagement also tended to have higher AARC-gains, we think the negative association of the goal re-engagement intercept with the AARC-gains slope likely represents either a chance finding or the possibility that those who entered the study with higher goal re-engagement (and associated higher AARC-gains) may have had more room to subsequently decline in AARC-gains via regression to the mean.
Tests of Age Moderation
In addition to testing mediation, we also explored whether associations of the key predictor variables with vitality and the putative mediators varied as a function of age. Our hypothesis that a negative association of AARC-losses with goal re-engagement would be weaker at older ages was not supported. These findings were consistent with those of Dutt et al. (2018b) who found no age moderation effects when examining associations of AARC-gains and AARC-losses with assimilation, a measure of active engagement with the environment in the service of goal attainment that is conceptually alike to goal re-engagement, in a sample of adults aged 42 to 100. Although further replication is needed, taken together, our results and those of Dutt et al. (2018b) suggest that—at least cross-sectionally—the implications of subjective aging for the management of goals remains relatively consistent from late midlife into retirement age and beyond.
The one age interaction that emerged from our analysis showed that the positive relationship between AARC-gains and the intercept for goal re-engagement was stronger at older relative to younger ages. While awareness of growing older is present as early as middle adulthood (Kornadt et al., 2018), AARC may show stronger associations with goal adjustment processes later in life when aspects of aging become more salient. In older adulthood, age-related losses may be more expected than at younger ages (Heckhausen et al., 1989). However, AARC-gains may become less common with age (Kite et al., 2005), and therefore particularly valued (Dutt et al., 2018a), possibly highlighting available resources and triggering processes of goal re-engagement. Furthermore, blocked goals in later life (e.g., ages 75+) are more likely to be driven by aging-related changes in, for example, health and cognition, whereas blocked goals in young-old age may be more likely due to work and/or family commitments. These are highly speculative interpretations; however, a greater focus on the possible protective role of AARC-gains (e.g., Windsor et al., 2022) seems warranted. If an appreciation of AARC-gains can help older adults—including those in the fourth age (Baltes & Smith, 2003) to re-engage in response to thwarted goals, the enhancement of AARC-gains, perhaps through efforts to reduce ageism (Levy, 2018), could represent a fruitful avenue for intervention work.
Limitations and Future Directions
Apart from the limited longitudinal timeframe already discussed, it is important to consider the current findings in the context of several additional limitations. First, the current sample under-represented the oldest-old. In addition, participants reported relatively high levels of education and physical functioning; which are both associated with aging well (Boerner, 2004). People with higher educational and physical resources may be more likely to pay attention to personal goals and show greater discernment regarding processes of AARC and goal adjustment. Furthermore, online samples of older adults have been shown to differ from national probability samples in multiple constructs such as verbal fluency, depressive symptoms, and self-rated health/memory (Ogletree & Katz, 2020). Our sample was also predominantly white, consistent with recent work pointing to lower technology access among non-White Americans (Suntai & Beltran, 2023). Thus, our findings cannot be generalized to more racially diverse and potentially more vulnerable older populations.
The final wave of this study was conducted after COVID-19 was declared a global pandemic by the World Health Organization. Greater COVID-related disruption has been found to be associated with higher AARC-gains and higher AARC-losses (Kolovos & Windsor, 2023). However, the extent to which peoples’ awareness of aging shifted from pre-COVID to during COVID is not known. Evidence suggests that attitudes toward own aging may become more negative during the pandemic (Wettstein & Wahl, 2021). However, findings are inconsistent regarding whether subjective age was impacted during COVID-19. Some studies suggest that people may have reported feeling younger than their actual age in the early period of COVID-19, potentially to psychologically distance and protect themselves from ageist narratives (Kornadt et al., 2021) and feeling particularly at risk for COVID-related complications (Terracciano et al., 2021; Wettstein & Wahl, 2022). Furthermore, goal re-engagement may have been particularly important for maintaining well-being during the early stages of the pandemic due to a potentially higher instance of blocked goals (Hamm et al., 2022). While it is not known precisely how COVID may have impacted the pattern of our results, it is important to keep the historical context of the current research in mind when interpreting the broader findings.
There were also some limitations associated with the measures used in this study. Specifically, our focus on goal re-engagement captures a specific aspect of self-regulation (the motivation to re-engage with new goals in response to goal non-attainment) and may not adequately capture other key features of goal regulation such as persistence or tenacity in pursuing existing attainable goals. Furthermore, while vitality correlates with various aspects of positive functioning across the lifespan (Kasser & Ryan, 1999; Ryan & Frederick, 1997), there are limitations to subjective vitality being the sole indicator of well-being in this study. While the amount of energy available to the self may be reflective of psychological well-being, older adulthood is often a time of shifting priorities and the reappraisal of important goals. Older adults show a general tendency to conserve their available resources for pursuits that will be more valuable (Cardini & Freund, 2020). Hence, vitality may not necessarily be an indicator of psychological well-being for all people at all times. Future studies may consider a broader selection of outcome variables, alongside assessment of changes in well-being over longer time periods.
Conclusion
To our knowledge, this study is the first to examine longitudinal inter-relationships among AARC, self-regulation of goals and well-being in middle-aged and older adults, testing theoretical propositions outlined by Diehl and Wahl (2010). Findings at the between-person level based on growth model intercepts (and follow-up cross-sectional analysis) were consistent with previous research suggesting that both a more favorable profile of AARC (lower losses and higher gains) and a greater willingness to engage with new goals were associated with higher vitality. However, we did not find longitudinal evidence in support of goal re-engagement mediating pathways from AARC to vitality, which may reflect methodological limitations (study duration and sample homogeneity) or the operation of alternative untested mechanisms. Studies with more assessments, longer measurement intervals and tests of multiple mediators are needed to provide more conclusive evidence regarding the centrality of self-regulation to processes linking views on aging to late-life well-being, including vitality.
Supplemental Material
sj-docx-1-jbd-10.1177_01650254241298896 – Supplemental material for Examining goal re-engagement as a mediator of longitudinal associations between awareness of age-related change and vitality in midlife and older adulthood
Supplemental material, sj-docx-1-jbd-10.1177_01650254241298896 for Examining goal re-engagement as a mediator of longitudinal associations between awareness of age-related change and vitality in midlife and older adulthood by Tim D. Windsor and Bethany Wilton-Harding in International Journal of Behavioral Development
Footnotes
Data Availability
The raw data supporting the conclusions of this article will be made available by the authors upon request.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: B. Wilton-Harding was supported by The Australian Government Research Training Program Scholarship.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.