
Abstract
The goal of this prospective longitudinal study was to explore whether co-occurrent internalizing difficulties and aggression in early childhood convey increased risk for later mental health problems in middle childhood. Participants were mothers from the Norwegian Mother, Father and Child Cohort Study (MoBa), who provided assessments of child internalizing difficulties and aggression at ages 3 years (n = 54,644; 26,750 girls) and 5 years (n = 38,177; 18,794 girls), as measures of child depressive, anxiety, conduct-related, and oppositional defiant (OD) symptoms at age 8 years. Using latent profile analyses (LPA) of internalizing difficulties and aggression, four profiles were identified: low-symptom/normative; primarily internalizing; primarily aggressive; and co-occurrent. Among the other results, the co-occurrent group exhibited the highest levels of depressive, anxiety, and oppositional defiant symptoms at 8 years. Most children (78%) remained stable in their profile between ages 3 and 5 years. Among the transition patterns that emerged, transitions were observed both from the normative to a risk profile and vice versa. Children who remained stable within the co-occurrent profile or who transitioned from the co-occurrent profile to one of the other two risk profiles also exhibited more depressive, anxiety, and OD symptoms at 8 years of age, when compared with children who transitioned from the co-occurrent to the normative profile. The heterogeneity between early manifestation of internalizing difficulties and aggression, and specific type of later mental health symptoms not only supports a shared etiology between internalizing and externalizing difficulties but also points toward the need for person-centered monitoring in early childhood with further implications for early identification of difficulties and preventive measures.
The manifestation of internalizing or externalizing difficulties in early childhood features as a prominent risk factor in the pursuit of detecting early risk for the development of psychopathology or other adverse outcomes in later life. Elevated but subclinical parent- or teacher-reported internalizing or externalizing difficulties are frequently reported as early as 3 years of age (Rescorla et al., 2012). Historically, internalizing and externalizing dimensions of difficulties were considered to be quite disparate (Campbell, 1995). Contemporary evidence, including commonly reported positive correlations between these dimensions in early childhood, now suggests that the co-occurrence of internalizing and externalizing difficulties surpasses a chance rate (Forbes et al., 2016; Willner et al., 2016). This co-occurrence tends to remain stable from kindergarten to primary school (Nilsen et al., 2013; Willner et al., 2016) and from primary school until late adolescence (Shi et al., 2020), suggesting a continuity of this type of risk across different developmental stages. This is despite expectant developmental gains in relevant cognitive or emotional domains, such as emotion regulation (Cole et al., 2018).
However, to date, there remain gaps in the extant literature related to the implications of co-occurring internalizing and externalizing problems in early childhood. Accordingly, the goal of this prospective longitudinal study was to explore whether co-occurrent internalizing difficulties and aggression in early childhood convey increased risk for later mental health problems in middle childhood.
Conceptualizing the Co-occurrence of Internalizing and Externalizing Difficulties
The co-occurrence of internalizing and externalizing difficulties has been previously conceptualized in different, but somewhat overlapping ways (Caspi et al., 2014). The partial intersection among these different conceptualizations lies in the shared idea of lack of self-regulation, largely reflecting difficulties with executive functions and emotion regulation (Mathiesen et al., 2009). Such difficulties are frequently observed in types of psychopathologies with varying symptomatology. One perspective is variable-oriented, wherein each individual’s position on a latent dimension is evaluated in comparison to the position of other individuals on the same dimension (Bergman et al., 2015). One example of this approach is the p factor, a general psychopathology dimension underlying disorders with different manifestations (e.g., depression, and conduct problems). The p factor reflects a child’s propensity to developing psychopathology, irrespective of the specific symptoms or disorder (Caspi et al., 2014). The p factor has been validated against other known predictors of general psychopathology, such as child temperament (Brandes et al., 2019) and chronic stress (Snyder et al., 2019).
A second perspective considers the Dysregulation Profile, which is derived based on high scores on three scales from the Child Behavior Checklist (Achenbach & Rescorla, 2000): (1) Anxious/Depressed; (2) Aggressive Behavior; and (3) Attention Problems (Althoff et al., 2010). This combination of characteristics is used to identify children who manifest self-regulation difficulties across affect, behavior, and cognition. Similar to the p factor, the Dysregulation Profile is influenced by non-specific predictors of psychopathology, such as temperament and familial psychopathology (Szkody et al., 2021), but also predicts elevated mental health problems in adulthood, including substance abuse and suicidal behavior (Holtmann et al., 2011; Szkody et al., 2021). The Dysregulation Profile originates from a person-centered approach of conceptualizing the co-occurrence of mental health difficulties (Basten et al., 2013; Vaidyanathan et al., 2011). This approach assumes some degree of heterogeneity in the manifestation of mental health difficulties in the population. Using statistical methods such as latent profile analysis, growth mixture modeling, or latent transition analysis (LTA), specific subgroups of children with a shared pattern or trajectory of difficulties can be identified, while also considering severity or duration of the difficulties.
Both the p factor and Dysregulation Profile may contribute to explaining comorbidity and are considered targets of transdiagnostic interventions (Aitken et al., 2019; Smith et al., 2020). At the same time, the clinical utility of these approaches may be limited by the underlying theoretical understanding and corresponding methodology that elevated scores in all included domains are required to score high on either the p factor or the Dysregulation Profile. In addition, although the Dysregulation Profile assumes a person-centered approach, it is still criterion-based (i.e., only children with high scores in all three scales that comprise the profile are classified as members; Basten et al., 2013). Therefore, groups of children who may have a more nuanced profile of difficulties, such as children with moderate levels of different types of problems, or children with rather “pure” internalizing versus externalizing difficulties are overlooked, with concomitant implications for personalized interventions (Levin-Aspenson et al., 2021).
A third possibility also invokes an expanded person-centered approach that does not require pre-determined levels of severity of difficulties as a criterion for inclusion to a profile (as is the case for the Dysregulation profile). Instead, the expanded person-centered approach assumes that individuals vary in the level of internalizing and externalizing difficulties, allowing for more accurate representation of the individuals within the detected profiles. Through this alternative, a multimorbid profile, consisting of both internalizing and externalizing disorders, was detected in adults, accounting to a large extent for the overlap between these two disparate types of disorders (Vaidyanathan et al., 2011). This was in addition of profiles that included individuals exhibiting only internalizing or externalizing disorders. In a similar fashion, besides a low-symptom/low-risk profile, a pure internalizing profile, and a pure externalizing profile, in children a co-occurring internalizing-externalizing profile is consistently detected across different developmental periods (McElroy et al., 2017; Wang et al., 2020; Wiggins et al., 2015; Winsper et al., 2020). This suggests that a unique constellation of difficulties that cannot be accounted for by internalizing or externalizing difficulties alone may already be present in childhood.
Previous investigations of this co-occurrence utilized measurements of externalizing difficulties that included not only aggression- or conduct-related behaviors but also attention problems or difficulties related to attention-deficit hyperactivity disorder (ADHD). However, according to Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013), ADHD-related difficulties are still neurodevelopmental in nature and frequently co-occur with both internalizing and externalizing (i.e., aggression- or conduct-related) difficulties (Gnanavel et al., 2019). Therefore, their inclusion in investigations of co-occurrence of internalizing and externalizing difficulties may shift the focus away from difficulties that are purer manifestations of inefficient emotion reactivity and self-regulation and social information processing (Granic, 2014; Kunimatsu & Marsee, 2012). To date, there is a lack of evidence on the co-occurrence of internalizing and aggression-related difficulties, particularly during the preschool years.
To date, the stability of co-occurrences among internalizing problems and aggression remains understudied. This is particularly important to explore in early childhood, as self-regulatory processes mature during this period (e.g., executive functions, emotion regulation; Willoughby et al., 2012) along with children exhibiting more exploratory behaviors, thus becoming increasingly more independent in their emotion self-regulation (Callaghan et al., 2019). Existent evidence indicates that approximately 80% of children tend to remain stable in their respective initially classified profile, whereas the most frequent transitions appear to be from a low-symptom profile to a pure internalizing profile or vice versa (McElroy et al., 2017; Willner et al., 2016). However, these earlier studies focused on the stability from kindergarten to primary school (Willner et al., 2016) or from middle childhood to adolescence (McElroy et al., 2017). Moreover, although McElroy et al. (2017) utilized data from a normative, population-representative sample, Willner et al. (2016) focused on a sample that largely included participants with identified aggressive or oppositional difficulties.
Related to stability, there is limited evidence to also suggest that membership in a co-occurring profile in childhood increases the risk for more severe forms of psychopathology in pre-adolescence to a higher extent compared to the manifestation of internalizing or externalizing difficulties alone (Winsper et al., 2020). Essentially, children who were classified as exhibiting co-occurrent difficulties were at higher risk for meeting diagnostic criteria for personality or depressive disorders in pre-adolescence (Winsper et al., 2020), suggesting relative stability of heightened risk for mental health problems in this co-occurrent group. Whether such a risk manifests before pre-adolescence or how membership in a co-occurrent profile increases a child’s risk for developing specific difficulties, for example, depression or oppositional defiant disorder, remain unclear. These are important questions in terms of its implications regarding detection of early risk and the implementation of preventive interventions. Moreover, despite the consistency in the identification of the profiles, earlier studies are based in the United Kingdom or the United States, potentially limiting generalizability of the findings in population with a different cultural and social background.
The Current Study
The present study aimed at addressing these gaps by investigating the latent profile structure of internalizing difficulties and aggression at ages 3 and 5 years—and how the identified profiles shape the child’s risk for developing symptoms of mental health difficulties later in childhood. We focused on the latent profile structure of difficulties during the preschool years, as marked improvements in self-regulatory processes are observed during this period (Willoughby et al., 2012), which again may be reflected in child behaviors such as the manifestation of emotional difficulties or aggression (Tsotsi et al., 2021). Furthermore, we were interested in understanding the nature of risk profiles before school start and how they might affect mental health symptoms during the school years.
In the present study, data were drawn from a sample that is culturally and socially different from those in earlier investigations (i.e., a large Norwegian cohort sample). Although children in Norway and the United States do not differ in levels of self-regulation at school entry age, there are differences in socio-economic factors that influence self-regulation in each country (Lenes et al., 2020). In addition, social benefits and quality of group daycare, which vary greatly across countries, may influence children differently depending on social contexts (Bekkhus et al., 2011). For example, most children in Norway start attending organized childcare as soon as they turn 1 year (e.g., 93.4% of 1- to 5-year-olds in 2021, according to Statistics Norway; 2022). In contrast to other countries, in Norway, public childcare is regulated and heavily subsidized by the government. This arrangement could potentially have a protective effect when it comes to the development of socio-emotional difficulties in early childhood.
Our first aim was to investigate the latent profile structure of internalizing difficulties and aggression at 3 and 5 years of age. Based on earlier findings with older children and adolescents (McElroy et al., 2017; Wang et al., 2020), we sought to replicate the previously identified four-profile structure and hypothesized that this four-profile solution would emerge at both ages, reflecting a low-symptom profile, a profile primarily characterized by internalizing difficulties, a profile primarily characterized by aggression, and a profile characterized by co-occurrence of internalizing difficulties and aggression. Our second aim was to explore the stability of individual membership in these profiles from 3 to 5 years of age. Although no a priori hypotheses were formulated related to the direction of potential transitions, it was hypothesized that the majority of participants would remain stable and that this stability would be more pronounced in the low-symptom group.
Our third aim was to investigate whether the four-profile groups would differentially associate with internalizing and externalizing symptoms at 8 years of age. We hypothesized that the co-occurrent profile would associate with higher internalizing (depressive and anxiety symptoms) and externalizing (conduct disorder and oppositional defiant symptoms) difficulties at 8 years of age compared with profiles of children who primarily manifested emotional difficulties or aggression only. Finally, we explored whether children who remained stable in their profiles between ages 3 and 5 years differed from their counterparts who transitioned to a different profile between ages 3 and 5 years.
Method
Participants and Procedures
The Norwegian Mother, Father and Child Cohort Study (MoBa) is a population-based pregnancy cohort study conducted by the Norwegian Institute of Public Health. Participants were recruited from all over Norway from 1999 to 2009. The women consented to participation in 41% of the pregnancies. Approximately 114,500 children, 95,200 mothers, and 75,200 fathers participated in the study initially (Magnus et al., 2016). Out of this initial sample, maternal questionnaire response rates were 61.4% at the 3-year-old time point, 54% for the 5-year-old time point, and 47% for the 8-year-old time point (Schreuder & Alsaker, 2014). Mother–child dyads were further excluded if children were twins, had a 5-min Apgar score of ⩽7, or had a diagnosis for a genetic syndrome or neurological damage/disorder or autism spectrum disorders or developmental delay at age 5. For the analyses including child mental health outcomes at age 8 years, we also further excluded participants if they had received a diagnosis of neurological damage/disorder or autism spectrum disorders or developmental delay at age 8. Data attrition is outlined in detail in Supplemental Figure S1.
The current study is based on version 12 of the quality-assured data files released for research in 2021. The establishment of MoBa and initial data collection was based on a license from the Norwegian Data Protection Agency and approval from The Regional Committees for Medical and Health Research Ethics. The MoBa cohort is currently regulated by the Norwegian Health Registry Act. The study was approved by The Regional Committees for Medical and Health Research Ethics (REK-2009/1899-7; 2013/2061) and the Norwegian Data Inspectorate. All participants have provided their informed consent prior to participation.
Measures
Child Internalizing Difficulties and Aggression at Ages 3 and 5 Years
Child internalizing difficulties and aggression were assessed using items from the Child Behavior Checklist (CBCL; Achenbach & Rescorla, 2000). The selection of items used in MoBa was conducted by a team of clinical and developmental psychologists based on theoretical and empirical representativeness. Mothers reported whether they agreed with each item on a 3-point Likert-type scale ranging from 0 to 2.
Internalizing difficulties were assessed with 9 and 10 items (ages 3 and 5, respectively; raw score range: 0–18 at age 3 and 0–20 at age 5). Item-response-theory-based reliability ranged between 0.60 and 0.71 at age 3 and between 0.62 and 0.86 at age 5 for the range of values in the internalizing difficulties score.
Aggression was assessed with four items at both time points (raw score range: 0–8). It ranged between 0.60 and 0.65 at age 3 and between 0.58 and 0.70 at age 5 for the range of values in the aggression score. The scores were derived based on a series of analyses that are described briefly in the “Method” and “Results” sections (and in more detail in the Supplemental Material).
Symptoms of Mental Health Problems at Age 8 Years
Child depression symptoms. Mothers reported symptoms of child’s depression on the Short Mood and Feelings Questionnaire (SMFQ; Messer et al., 1995). The scale consists of 13 descriptive phrases regarding how the child had been feeling or acting during the last 2 weeks. Mothers rated items for their child on a 3-point scale (0 = not true, 1 = sometimes true, 2 = true). Internal reliability for the SMFQ was α = .79.
Child anxiety symptoms. Mothers reported on their child’s anxiety symptoms on the 5-item short version of the Screen for Child Anxiety Related Disorders (SCARED; Birmaher et al., 1997). Mothers rated the statements describing their children using a 3-point scale (0 = not true, 1 = sometimes true, 2 = true). Internal reliability for the SCARED’s short version in the present MoBa sub-sample was α = .53.
Conduct disorder symptoms. This type of symptoms was measured with 8 items (out of 16) on the Parent/Teacher Rating Scale for Disruptive Behavior Disorders (RS-DBD; Silva et al., 2005). Mothers were asked to rate items describing their child’s behavior during the last 6 months on a 4-point scale (0 = never/seldom, 1 = sometimes, 2 = often, 3 = very often). Internal reliability for conduct disorder (CD) symptoms was α = .68.
Oppositional defiant symptoms. Mothers reported symptoms of oppositional defiant (OD) disorder on the relevant disorder index of RS-DBD (Silva et al., 2005). This index consisted of 8 items describing child behavior during the last 6 months and reflects symptoms of OD disorder from the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association, 2000). Internal reliability for the OD subscale was α = .84.
Covariates
Covariates included child gender, birth weight adjusted for gestational age, number of children in the household, mother tongue (as a proxy of ethnic background), the child’s school grade, maternal education, and maternal anxiety and depressive mood at age 8 years.
Maternal anxiety and depressive mood were assessed through an 8-item version (Tambs & Røysamb, 2014) of the Hopkins Symptoms Checklist (SCL-8; Derrogatis et al., 1973) at ages 3, 5, and 8 years. Mothers were asked to rate anxiety and depression items during the past 2 weeks on a 4-point scale (0 = not at all, 1 = a little, 2 = quite a bit, 3 = extremely). Internal reliability for the SCL-8 in the present MoBa sub-sample was α = .87 at age 3 years, α = .85 at age 5 years, and α = .87 at age 8 years.
Data Analytic Plan
Statistical analyses were conducted in three steps according to our research aims in MPlus (version 8; Muthén & Muthén, 2017).
Preliminary Exploratory and Confirmatory Factor Analyses
Given that a subset of CBCL items was used at each time point, a series of exploratory factor analysis (EFA) and confirmatory factor analysis (CFA) were separately conducted at ages 3 and 5 using structural equation modeling. The available samples at ages 3 and 5 were split randomly to create two datasets of equal size to be used separately in the EFA and CFA (Kline, 2015).
Step 1: Identifying Latent Profile Structures of Internalizing Difficulties and Aggression
To identify groups of children with similar patterns of internalizing difficulties and aggression scores at 3 and 5 years of age, we implemented LPA separately at each time point, using maximum likelihood with robust standard errors and full information maximum likelihood for missing data estimation. Given that the two identified factor scores (internalizing difficulties, aggression) are comprised by a different number of items, Z-scores of the sum of the items of each factor were used as the indicators in the LPA models. Models consisting of 1–6 classes were tested. Model fit was determined by several common fit statistics (Asparouhov & Muthén, 2012), including the Akaike information criterion (AIC), the Bayesian information criterion (BIC), and the sample size-adjusted Bayesian information criterion (ssaBIC), wherein lower values indicate better fit; the bootstrapped likelihood ratio test (BLRT), wherein a significant p value suggests that a model with k number of classes fits the data better than a solution with k − 1 classes; the entropy criterion, wherein values range between 0 and 1 and a higher value indicates clearer delineation of profiles.
Step 2: Investigating Children’s Transition Between Latent Profiles Over Time
To investigate the transition of individual children between latent profiles over time, we implemented an LTA. An LTA consists of three components. The first is a measurement model, like the LPA described in the previous paragraph, yielding the structure of latent profiles at each time point. The second is a test for measurement invariance to assess whether the measurement model remains consistent over the two time points. For this purpose, we estimated two models, one with full measurement invariance (i.e., wherein conditional item probabilities were constrained to be equal across time) and one with full measurement non-invariance (i.e., wherein conditional item probabilities were freely estimated across time). To assess measurement invariance in an LTA, the two models were compared using the log likelihood ratio test, that is, a χ2 difference test based on the log likelihood values of the models. The third LTA component is an autoregressive model which assesses transitions at the individual level between the profiles over time. To ensure that the models converged on global rather than local solutions, 1,000 random sets of starting values and 100 final stage optimizations were used for both LPAs and the LTA. To account for the influence of maternal mental health on the transition probabilities, we used residuals for the internalizing and aggression scores at ages 3 and 5 following a regression analyses wherein maternal mental health at age 3 and 5 years, respectively, was the predictor variable.
Step 3: Associations Between Latent Profiles at Ages 3 and 5 Years and Mental Health Problems at Age 8 Years
We used the identified latent profiles in multivariable linear regression analyses to assess their association with mental health symptoms at age 8 years. Multivariable linear regressions were controlled for child gender, birth weight adjusted for gestational age, number of children in the household, mother tongue (as a proxy of ethnic background), the child’s school grade, maternal education, and maternal anxiety and depressive mood at age 8 years. For the LPA at age 3, we additionally controlled for maternal anxiety and depressive mood at age 3. Similarly, for these analyses at age 5, we controlled for these same variables at the same time point. To investigate whether children who remained stable between 3 and 5 years of age differed from children who shifted to a different profile from ages 3 to 5 years, we conducted four sets of multivariable linear regression analyses based on the groups of stayers within the same profile and movers to a different profile that we would get following the LTA.
Missing Data
In the first two steps of analyses (LPAs and LTA), participants were included at each time point if they had either an internalizing difficulties or aggression score or both at least at one of the two ages. Thus, we focused on 54,644 (26,750 girls) 3-year-olds and 38,177 (18,794 girls) 5-year-olds. Missing values (see Supplemental Table S1 for exact numbers) were imputed using full information maximum likelihood on MPlus.
In the third step of analyses (regressions with distal outcomes), children were included if they had complete data for CBCL profiles at the corresponding time point and all four outcome variables at age 8 years. Thus, we focused on 31,022 (15,410 girls) and 24,921 (12,404 girls) MoBa children at age 3 and 5, respectively. Little’s Missingness Completely At Random test was not significant, (χ2(69) = 76.71, p = .25, indicating missingness-completely-at-random (Little, 1988). We imputed missing values in control variables through expectation maximization.
Results
Descriptive Statistics
Descriptive information of CBCL internalizing difficulties and aggression scores and their correlation based on the larger samples used in the LPAs and LTA are presented in Supplemental Table S2. Descriptive information of control variables and child mental health variables at age 8 are presented in Supplemental Tables S1 (categorical variables) and S3 (continuous variables).
Preliminary Exploratory and Confirmatory Factor Analyses
The results of these analyses are described in detail in the Supplemental Material. Briefly, at both ages 3 and 5 years, following the corresponding EFAs, a four-factor solution yielded the best fit to the data. CFAs corroborated the four factors at both time points. The four factors were labeled: (1) attention and hyperactivity problems; (2) impulsive temperament; (3) aggressive; and (4) internalizing difficulties. Items loading on factors 3 and 4 were each summed to create the aggression and internalizing difficulties scores, respectively.
Step 1: Latent Profile Structures of Internalizing Difficulties and Aggression
Identifying the Number of Profiles
To identify the latent profile structure of internalizing difficulties and aggression among children in our sample, a latent profile analysis was conducted at each age. Supplemental Table S9 presents the fit statistics for the different profile solutions. As shown there, the two- and three-profile solutions at both ages were not optimal given that all fit indices, besides entropy, indicated that more profiles improved the model fit. Entropy values were identical for the four-, five-, and six-profile solutions at age 3 years but yielded better fit for the four-profile solution at age 5 years, indicating good separation of the profiles (Celeux & Soromenho, 1996). The AIC, BIC, and adjusted BIC values kept decreasing at both ages, indicating that adding more classes improved the model fit. However, the decrease in values reached a plateau from the four-profile solution and above, especially at age 3 years, indicating minimal improvements of the five- and six-profile solution over the four-profile one. The BLRT remained significant even for the six-profile solution, indicating that the optimal solution might consist of six or more profiles. However, in large sample sizes (i.e., n > 1,000), the BLRT may occasionally favor solutions with a higher number of profiles (Morin & Marsh, 2015). Our decision to retain the four-profile solution was based on the combination of the performance of BIC and entropy along with overall model parsimony and interpretability of the profile solution at both ages. The four-profile solution was the solution with a combination of lower BIC value, compared to the two- and three-profile solutions, at both ages and the higher entropy, compared to the five- and six-profile solution, at age 5 years. As entropy values were identical for the four-, five-, and six-profile solutions at age 3 years, the four-profile solution was optimal on grounds of overall parsimony. Interpretability-wise the four-factor solution was easy to interpret at both ages (i.e., low-symptom/normative, internalizing difficulties-based, aggression-based, co-occurrent). The five-profile solutions were similar to the four-profile solutions with one additional co-occurrent profile with slightly different mean scores for emotional difficulties and aggression.
Description of the Profiles
As depicted in Supplemental Figure S2, at both ages, Profile A was labeled as “low-symptom/normative” and manifested the lowest scores on both internalizing difficulties and aggression (nage3 = 36,677, 67.1%; nage5 = 29,581, 78.2%). Profile B was labeled as “primarily aggressive” as it comprised participants with low levels of internalizing difficulties and moderate levels of aggression (nage3 = 8,110, 14.8%; nage5 = 3,805, 10.0%). Profile C was labeled as “primarily internalizing” and consisted of participants with low levels of aggression and moderate levels of internalizing difficulties (nage3 = 8,364, 15.3%; nage5 = 3,710, 9.7%). Finally, Profile D was labeled as “co-occurrent” and consisted of participants with high levels of internalizing difficulties and moderate levels of aggression (nage3 = 1,493, 2.7%; nage5 = 811, 2.1%).
Step 2: Latent Transition Analyses From Ages 3 to 5 Years
Testing for Measurement Invariance Across Time
Besides identifying the number and nature of profiles, the LPAs described earlier also comprised the first step of the LTA (i.e., the measurement model yielding the structure of latent profiles at each time point). Fit statistics for two measurement models for the four-profile solution across time are presented in Supplemental Table S10. The two measurement models are the full measurement non-invariance (i.e., wherein conditional item probabilities were freely estimated across time) and full measurement invariance (i.e., conditional item probabilities constrained to be equal at both time points). The log likelihood ratio test, used to compare the two models, did not yield a significant difference when the measurement invariance constraints were added to the model (LRT = −184,746.46, Δdf = 8, p = .99). This suggests that the model fit did not worsen when measurement invariance constraints were imposed and the identified latent structure at age 3 years was equivalent to that at age 5 years. Therefore, full measurement invariance was assumed in the LTA.
Latent Transition Probabilities
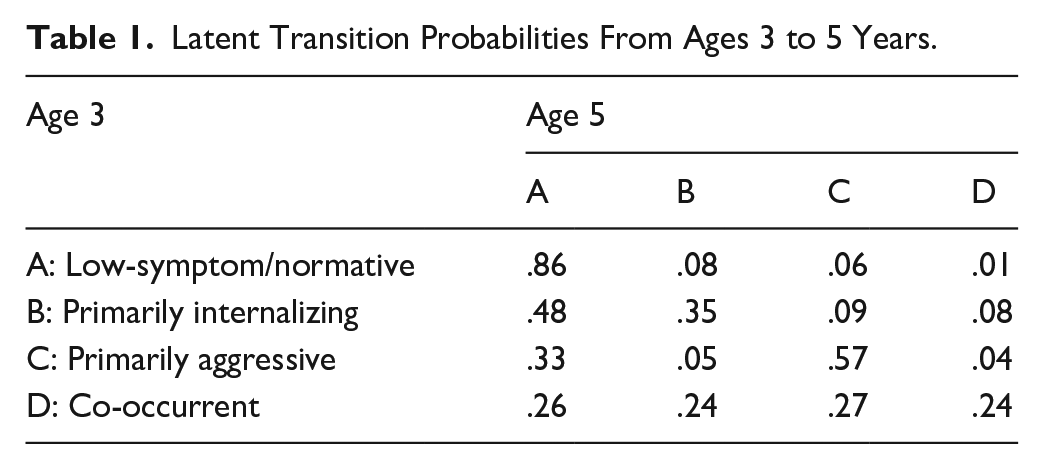
The latent transition probabilities (Table 1) indicated that the majority of children in the low-symptom/normative profile (0.86) and primarily aggressive profile (0.57) remained stable across time. Participants in the primarily aggressive profile had a lower but still substantial probability of transitioning to the low-symptom/normative profile (0.33). Children in the primarily internalizing profile were more likely to transition to the low-symptom/normative profile (0.48) or remain stable (0.35) than to transition to one of the remaining two profiles. Children in the co-occurrent profile were almost equally likely to remain stable (0.24) or transition to one of the other three profiles: primarily internalizing profile (0.27), primarily aggressive profile (0.24), and low-symptom/normative profile (0.24).
Latent Transition Probabilities From Ages 3 to 5 Years.
Identifying Movers and Stayers Across Time
Following these latent transition probabilities, we added one more step in the LTA, specifying a latent mover-stayer variable to identify patterns of mover versus stayer participants. Most children were categorized as stayers (79% of the total sample). Within stayers, low-symptom/normative children comprised 85%, primarily aggressive children comprised 11.7%, primarily internalizing children comprised 3%, and co-occurrent children comprised 0.3%. Taken together with the LTA results, the low symptom/normative and the primarily aggressive profiles were the ones with the highest stability across time. Within movers, four mover types were the most frequent. Movers from the primarily internalizing to the low-symptom/normative profile comprised 38.5% of the total number of movers, those from the primarily aggressive to the low-symptom/normative profile comprised 17.4%, those from the low-symptom/normative profile to the primarily internalizing profile comprised 17.7%, and those from the low-symptom/normative profile to the primarily aggressive profile comprised 9.6%. Although most children in our sample remained stable across time, a subset of children transitioned both ways, not only from normative behavior to some behavior difficulties but also from behavior difficulties to normative behavior.
Step 3: Associations Between Latent Profiles at Age 3 Years and Mental Health Symptoms at Age 8 Years
Besides CD symptoms, children in the co-occurrent profile at age 3 years were at highest risk for developing symptoms of mental health at age 8 years, particularly OD and depression. Children in the primarily aggressive profile were at highest risk for CD symptoms and relative high risk for OD symptoms. These results were based on two sets of analyses. First, a series of multivariable linear regressions was conducted to assess the association between the latent profiles at 3 years and mental health problems at age 8 years (Table 2). The low symptom/normative profile was used as the reference profile. The primarily aggressive, primarily internalizing and co-occurrent profiles differed significantly from the reference profile on all symptom categories. Second, to identify significant differences between the primarily aggressive, primarily internalizing, and co-occurrent profiles, post hoc Bonferroni tests were conducted on each symptom category at age 8 years. These tests were significant at p < .001 for all symptom categories, with one exception: the test between the primarily aggressive and the co-occurrent groups for CD symptoms was significant at p < .05. With regard to depression symptoms, the low symptom/normative profile had the lowest scores and was followed by the primarily internalizing profile and then the primarily aggressive profile; the co-occurrent profile exhibited the highest depression symptoms scores at age 8 years. With regard to anxiety symptoms, the low symptom/normative profile was followed by the primarily aggressive profile and then the primarily internalizing profile; the co-occurrent profile exhibited the highest anxiety symptoms scores at age 8 years. With regard to CD symptoms, the low-symptom/normative profile was followed by the primarily internalizing profile and then the co-occurrent profile; the primarily aggressive profile exhibited the highest CD symptoms. Finally, with regard to OD symptoms, the low symptom/normative profile was followed by the primarily internalizing profile and then the primarily aggressive profile; the co-occurrent profile exhibited the highest OD symptoms.
Results of Multivariable Linear Regressions Assessing the Association Between the Latent Profiles at 3 and 5 Years and Mental Health Symptoms at Age 8 Years.
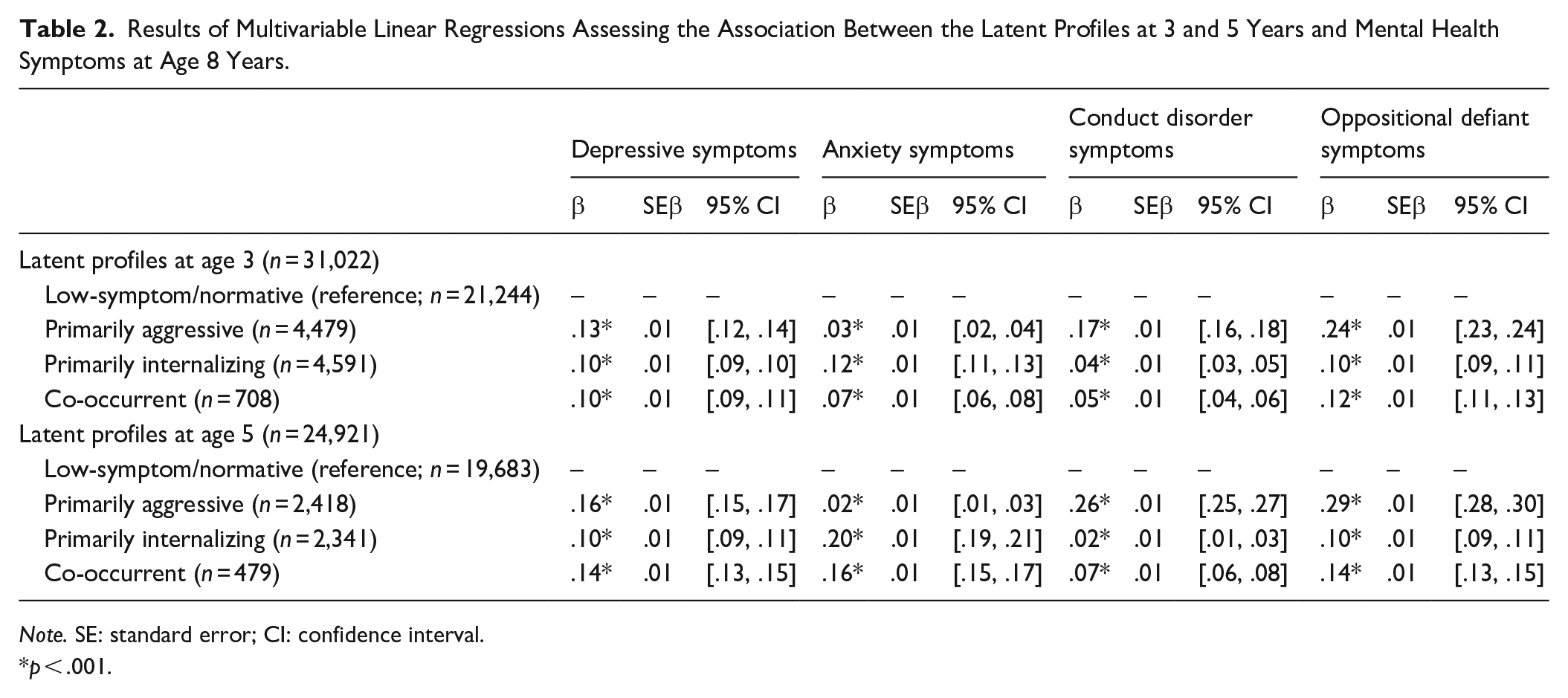
Note. SE: standard error; CI: confidence interval.
p < .001.
Associations Between Latent Profiles at Age 5 Years and Mental Health Symptoms at Age 8 Years
At age 5 years, children in the co-occurrent profile were still at the highest risk for depression, anxiety, and OD symptoms at age 8 years (resembling the findings at age 3 years). Likewise, primarily aggressive children at age 5 years showed the highest risk for CD symptoms at age 8 years.
Similar to 3 years, a series of multivariable linear regressions was conducted to investigate the association between the latent profiles at age 5 years and mental health symptoms at age 8 years wherein the low symptom/normative profile was again the reference profile (Table 2). The primarily aggressive, primarily internalizing, and co-occurrent profiles differed significantly from the reference profile on all symptom categories. To identify significant differences between the primarily aggressive, primarily internalizing, and co-occurrent profiles, post hoc Bonferroni tests were conducted on each symptom category at age 8 years. Post hoc Bonferroni tests, conducted on each symptom category at age 8 years, yielded significant differences for all tests between the profiles for all symptom categories at p < .01, with one exception: the test between the primarily aggressive and co-occurrent profiles on OD symptoms was significant at p < .05. Similar to results at age 3 years, with regard to depression symptoms, the low-symptom/normative profile had the lowest scores, followed by the primarily internalizing profile and then the primarily aggressive profile; the co-occurrent profile exhibited the highest depression symptoms scores at age 8 years. With regard to anxiety symptoms, although the test between the low symptom/normative and primarily aggressive profiles was significant, the mean anxiety scores of these profiles were the lowest and were quite similar. The primarily internalizing profile scored higher on anxiety compared with these two profiles and the co-occurrent profile exhibited the highest anxiety symptoms scores at age 8 years. The low symptom/normative profile exhibited the lowest CD scores, followed by the primarily internalizing profile and then the co-occurrent profile; the primarily aggressive profile exhibited the highest CD symptoms. Finally, with regard to OD symptoms, the low-symptom/normative profile had the lowest scores, followed by the primarily internalizing profile and then the primarily aggressive and co-occurrent profiles; although the test between the primarily aggressive and co-occurrent profiles was significant, the mean OD symptom scores of these profiles were the highest and quite similar.
Associations Between Stayer and Mover Groups and Mental Health Symptoms at Age 8 Years
To examine whether stability versus change in a child’s profile membership between the ages 3 and 5 years would influence their mental health symptoms at age 8 years, four sets of multivariable linear regression analyses were conducted. Significant differences between the groups were identified through post hoc Bonferroni tests on each symptom category at age 8 years.
In the first set, stayers within the normative profile (n = 22,647) were included as the reference group along with movers from the normative profile to a risk profile or from a risk profile to the normative profile (Table 3). Children who transitioned from the normative to the co-occurrent profile exhibited the highest levels of depression, anxiety, and OD symptoms at age 8. Children who transitioned from the normative to the primarily aggressive profile exhibited the highest levels of CD symptoms at age 8.
Results of Multivariable Linear Regressions Assessing the Association Between Stayers and Movers From Ages 3 to 5 Years and Mental Health Symptoms at Age 8 Years.
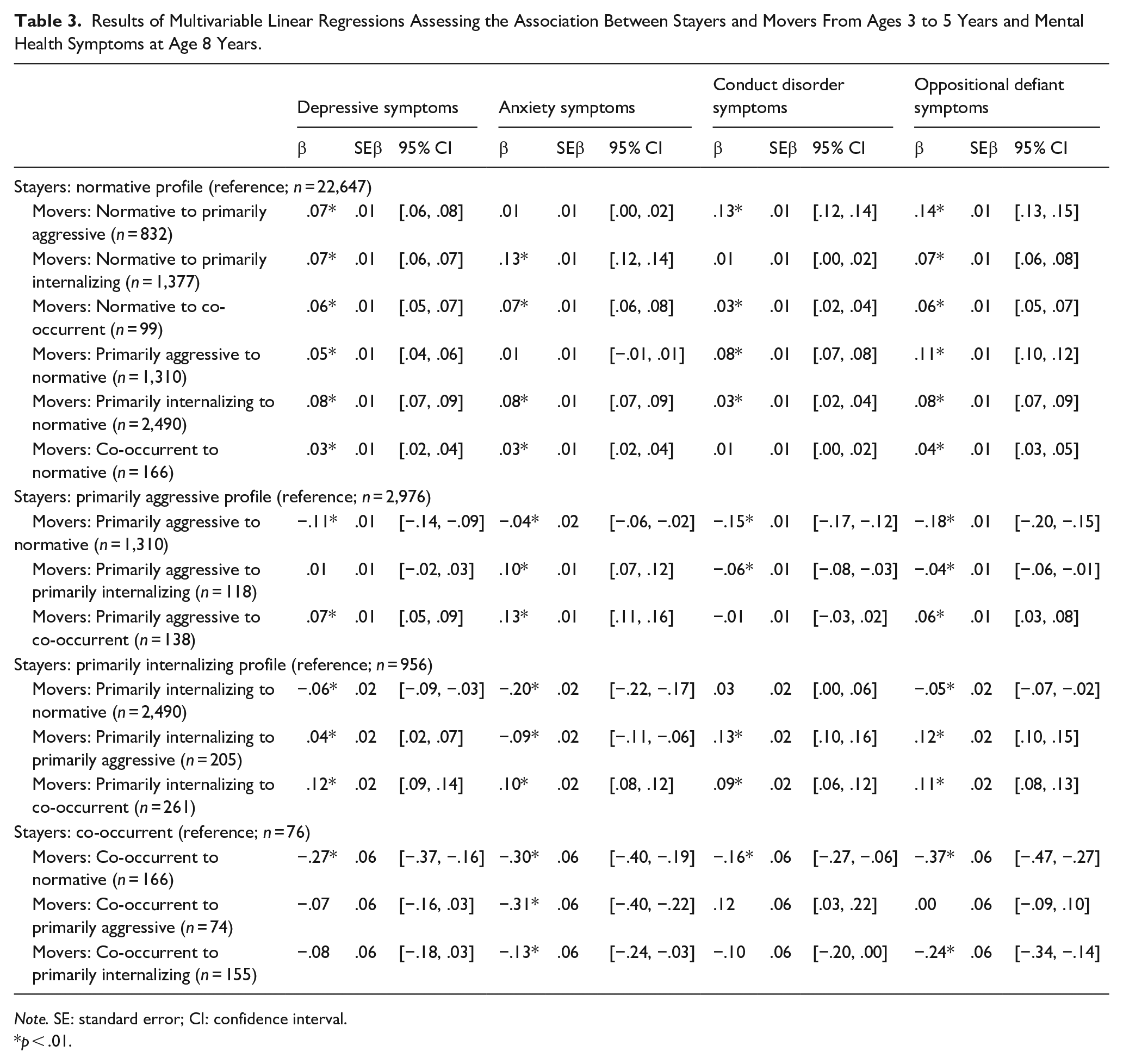
Note. SE: standard error; CI: confidence interval.
p < .01.
For depression symptoms, children who transitioned from a risk profile to the normative profile and children who transitioned from the normative to the primarily internalizing profile did not differ from each other, but they exhibited higher depression symptoms compared with the normative profile stayers and lower depression symptoms compared with the movers from the normative to the primarily aggressive profile. For anxiety symptoms, movers from the normative to the primarily aggressive or vice versa did not differ from the normative profile stayers, followed by the movers from the primarily internalizing or co-occurrent to the normative profile and then by the movers from the normative to the primarily internalizing profile. For CD symptoms, movers from the normative to the primarily internalizing profile and vice versa and movers from the co-occurrent to the normative profile do not differ from the stayers within the normative profile, followed by the primarily aggressive to the normative profile and then by the movers from the normative to the co-occurrent profile. For OD symptoms, children who transitioned from a risk profile to the normative profile and children who transitioned from the normative to the primarily internalizing profile did not differ from each other, but they exhibited higher OD symptoms compared with the normative profile stayers and lower OD symptoms compared with the movers from the normative to the primarily aggressive or co-occurrent profile.
In the second set of analyses, stayers within the primarily aggressive profile (n = 2,976) were included as the reference group along with movers from the primarily aggressive profile to one of the remaining three profiles (Table 3). Movers from the primarily aggressive to the co-occurrent profile exhibited the highest levels of depression, anxiety, and OD symptoms at age 8.
For depression symptoms, movers from the primarily aggressive to the normative profile were followed by the primarily aggressive stayers and movers from the primarily aggressive to the primarily internalizing profile. For anxiety symptoms, primarily aggressive stayers and movers from the primarily aggressive to the normative profile did not differ from each other but exhibited fewer symptoms compared with the movers from the primarily aggressive to the primarily internalizing or the co-occurrent profile. For CD symptoms, stayers within the primarily aggressive profile and movers from the primarily aggressive to the co-occurrent profile exhibited the highest levels of CD symptoms and did not differ from each other, followed by the other two profiles, which also did not differ from each other. For OD symptoms, the primarily aggressive to normative group exhibited the fewest symptoms, followed by the primarily aggressive stayers and the primarily aggressive to primarily internalizing movers who did not differ from each other.
In the third set of analyses, stayers within the primarily internalizing profile (n = 965) were included as the reference group along with movers from the primarily internalizing profile to one of the remaining three profiles (Table 3). For depression symptoms, movers from the primarily internalizing to normative profile exhibited the lowest levels, followed by the primarily internalizing stayers and the primarily internalizing-to-primarily aggressive movers; the primarily internalizing-to-co-occurrent movers exhibited the highest levels. For anxiety symptoms, the primarily internalizing-to-normative and the primarily internalizing-to-primarily aggressive movers exhibited the lowest levels, followed by the primarily internalizing stayers; the primarily internalizing-to-co-occurrent movers exhibited the highest levels. For both CD and OD symptoms, the primarily internalizing stayers and the primarily internalizing-to-normative movers exhibited the lowest levels, followed by the primarily internalizing-to-primarily aggressive and the primarily internalizing-to-co-occurrent movers who exhibited higher levels and did not differ from each other.
Finally, in the fourth set of analyses, stayers within the co-occurrent profile (n = 76) were included as the reference group along with movers from the co-occurrent profile to one of the remaining three profiles (Table 3). For depression symptoms, the co-occurrent-to-normative movers profile exhibited the lowest levels, followed by the other three groups that did not differ from each other. For anxiety, the co-occurrent-to-normative and co-occurrent-to-primarily aggressive movers did not differ from each other and exhibited the fewest symptoms, followed by the co-occurrent-to-primarily internalizing movers or the co-occurrent stayers who also did not differ from each other and exhibited the highest symptoms. For CD symptoms, the co-occurrent-to-normative and co-occurrent-to-primarily internalizing movers exhibited the lowest symptoms, followed by the co-occurrent stayers; the co-occurrent-to-primarily aggressive movers exhibited the highest levels. For ODD symptoms, the co-occurrent-to-normative exhibited the lowest symptoms, followed by the co-occurrent-to-primarily internalizing movers; the co-occurrent stayers and the co-occurrent-to-primarily aggressive movers did not differ from each other and exhibited the highest levels.
Discussion
In the present investigation, we examined the latent profile structure of internalizing difficulties and aggression and its stability at ages 3 and 5 years. In addition, we assessed how membership in the identified latent profiles—as well as the stability versus change in profile membership over 2 years—contributed to child risk for developing mental health problems at age 8 years. Among the results, a four-profile structure was identified for internalizing difficulties and aggression in early childhood (at both time points). Most children also remained stable in their profiles across time. As hypothesized, membership in the co-occurrent profile was more strongly associated with depressive, anxiety, and OD symptoms at 8 years of age, as compared to membership in the primarily aggressive or primarily internalizing profiles. Likewise, children who were stable in their membership in a risk profile (i.e., either within the co-occurrent profile or transitioning from the co-occurrent profile to another risk profile) also exhibited higher numbers of depressive, anxiety, and OD symptoms at 8 years of age, as compared to children who transitioned from the co-occurrent to the normative profile. These findings are discussed in more detail below.
Profile Structure for Internalizing Difficulties and Aggression
A four-profile structure was evaluated at both early childhood time points as best describing the latent structure of the manifestation of internalizing difficulties and aggression. The profile with the highest prevalence included children with low levels of internalizing difficulties and aggression, indicating low probability of manifesting any type of difficulty, labeled as the low symptom/normative profile. Two purer profiles emerged, each representing 10%–15% of the sample, including children with moderate levels of either aggression or internalizing difficulties, and indicating moderate probability of manifesting one type of difficulty only. As such, these were named as the primarily aggressive profile and the primarily internalizing profile, respectively. The least prevalent profile included children with moderate levels of aggression and high levels of internalizing difficulties, indicating high risk for co-occurrent internalizing difficulties and aggression, and was labeled the co-occurrent profile.
This four-profile solution is consistent with earlier investigations in child and adolescent samples in the United Kingdom and the United States (McElroy et al., 2017; Wang et al., 2020; Wiggins et al., 2015; Winsper et al., 2020). This finding further supports a central notion of the internalizing-externalizing comorbidity approach that within the general population there is heterogeneity in the type and severity of manifested difficulties. This is without disregarding the presence of subgroups of individuals with similar patterns of difficulties. Here, a small percentage of children were classified as exhibiting co-occurrent difficulties. To some extent, this may reflect underlying self-regulation difficulties across multiple domains (Winsper et al., 2020), for example, inhibitory control, emotional regulation, and relational security.
Of note, in contrast to the Dysregulation Profile, we implemented a person-centered approach that does not use pre-determined levels of severity of difficulties as a criterion for inclusion to a profile and did not include attention-related problems in our latent structure estimation. Notwithstanding, the percentage of children classified as “co-occurrent” resembled the percentage of children included in the Dysregulation Profile in other investigations (Basten et al., 2013). In this regard, our findings may also be consistent with evidence derived from different implementations of the person-centered approach.
Moreover, our findings are not in essence discordant from evidence derived from variable-centered approaches, such as the p factor (Caspi et al., 2014), especially with regard to psychopathology severity overall. A possible alternative interpretation is that some children (those not in the low symptom/normative profile) may have a biological predisposition toward developing a type of difficulty, but the specific type they develop may depend on other contextual factors. In terms of early risk identification and concomitant preventive measures, however, a person-centered approach, such as the one implemented here, which assumes heterogeneity in the manifestation and severity of different types of symptoms within the same population, allows for a better representation of individuals in a population.
Stability Versus Transitions from Ages 3 to 5 Years
With regard to the stability of the latent profile structure from ages 3 to 5 years, although most children remained stable, some noteworthy transition patterns were also present. For example, the majority of children in the low-symptom/normative profile remained stable across time, suggesting that children who at lower risk at age 3 years rarely go on to develop difficulties later in the preschool period. Whereas most children in the primarily aggressive and primarily internalizing profiles remained stable, the second largest transition probability for these profiles was transiting to the low symptom/normative profile. This finding suggests that among children who start at a moderate risk for a specific type of difficulty, most usually continue to exhibit that risk, but some may revert to a more normative pattern of behavior. Such a reversion may reflect developmental gains between 3 and 5 years of age, as discussed earlier. It may also be attributed to indirect reporter biases, given that internalizing difficulties and aggression were assessed via maternal reports. When children are 3 years old, they are less aware or able to communicate their emotions or properly discuss the situations surrounding them (Pons et al., 2004). Therefore, parents may sometimes speculate about a child’s severity of difficulties, especially in relation to internalizing difficulties. As children mature and their communication skills develop further, parents may increasingly identify whether a behavior is normative or not more accurately.
Finally, children in the co-occurrent profile had a rather equal probability of remaining stable or transitioning to any of the other three profiles, suggesting that most of these children seem to be at highest risk for sustained difficulties across time, irrespective of the specific nature. This may further suggest rather undifferentiated underlying self-regulation difficulties that also tend to be persistent over time. Still, some of the co-occurrent profile children may revert to more normative behavior, which also suggests that besides developmental gains, there may be some other protective factors in place.
Taken together, these findings have a series of implications for further research and clinical practice. Given the variability in the transitions of the at-risk groups and that some participants revert to normative behavior, future investigations should work more thoroughly on identifying sets of risk and protective genetic and environmental factors that when put together in a cumulative fashion may influence the developmental of mental health difficulties in early childhood. Such an identification may be most important for children in the co-occurrent profile who are at highest risk for developing mental health problems later in childhood, as will be discussed thoroughly in the next section. With regard to clinical practice, our findings highlight two points. First, it becomes increasingly more important to keep track of children’s developmental course of behavior, especially when there are some early signs of potential behavior or emotional difficulties. Second, within contexts wherein children spend a substantial amount of time at childcare, early childhood educators also play a crucial role in the early detection and monitoring of such difficulties, even within the first few years of life.
Associations Between Early Childhood Latent Profiles and Mental Health Symptoms at Age 8 Years
The next set of findings was related to the prediction of mental health difficulties at age 8 years based on profile membership at ages 3 and 5 years. Membership in the co-occurrent profile at both ages 3 and 5 years predicted the highest levels of depression and anxiety symptoms at age 8 years, which were higher also when compared to the primarily internalizing profile. This may be due to the co-occurrent group consisting of participants with high internalizing difficulties scores and only moderate aggression scores, but it could also be due to the added impact of aggression as externalizing symptoms are found to be an equally strong predictor as internalizing difficulties on later depression and anxiety symptoms (Nilsen et al., 2013). This finding is consistent with prior evidence in older children and adolescents (Nilsen et al., 2013; Winsper et al., 2020). Membership in the co-occurrent profile also associated with the highest levels of OD symptoms. Interestingly, membership in the primarily aggressive profile also associated with relatively high levels of depression and the highest levels of conduct and OD symptoms.
Taken together, these associations hint to a continuation of the early co-occurrence of internalizing difficulties and aggression later into childhood. This further implies that a co-occurrence of different difficulties as indices of early risk may result in internalizing-externalizing comorbidity at clinical levels in later childhood or adolescence. Such a comorbidity will have concomitant implications about the usefulness of preventive interventions in early childhood in an effort to alleviate the risk. Our findings may also reflect underlying traits at play, such as neuroticism and negative emotionality (Mathiesen et al., 2009). Increasingly, such characteristics have surfaced as common underlying features for both internalizing and externalizing behaviors although traditionally they were associated with depression and anxiety (Karevold et al., 2009; Rhee et al., 2015). It may also be the case that when combined with certain environmental factors, these traits lead to differential manifestations of symptoms. It is also possible, partially due to the presence of maladaptive traits, that these children eventually develop emotion regulation strategies, such as rumination, which have also increasingly been linked with the manifestation of both internalizing and externalizing symptoms (Aldao et al., 2016).
Associations Between Stayer and Mover Groups and Mental Health Symptoms at Age 8 Years
The final set of findings was related to the prediction of mental health difficulties at age 8 years based on stability versus change in a child’s profile membership between ages 3 and 5 years. These findings were complex but can yield two points of particular interest. First, our results highlight relative stability in young children’s experiences of co-occurring internalizing difficulties and aggression appears to yield the highest risk for mental health difficulties in middle childhood. For example, children who transitioned from the primarily internalizing or the primarily aggressive to the co-occurrent profile exhibited high levels of depression and anxiety or CD symptoms, respectively. Children who were stable in the co-occurrent profile exhibited the highest levels of depression, anxiety, and OD symptoms at age 8 years, whereas children who transition from co-occurrent to one of the other risk profiles were comparably at high risk. Consistent with the point made in the previous section, an implication of these findings is the need for close monitoring of the pattern of a child’s difficulties upon detection of early risk as a means of recommending the most suitable preventive measures.
Second, children who transitioned from a risk profile to the normative profile exhibited alleviated risk for mental health symptoms at age 8 years. Although preliminary in nature, this finding might support the idea of a “resilient” transition when it comes to manifestation of early risk and what that suggests for a child’s future risk, compared to transitions that are more resistant. Future research should attempt to extend these findings to more positive outcomes, such as peer relations or one’s sense of mastery. Subsequent investigations should also focus on the reciprocal effects between manifestation of risk and protective factors at play across childhood.
Strengths, Limitations, and Future Directions
The present study has three main strengths. It includes one of the largest samples from a normative birth cohort to date among investigations of the internalizing-externalizing co-occurrence. Also, the available data at each time point and the type of analyses we implemented allowed us to not only replicate the pattern of profiles identified in earlier investigations but also examine individual transitions across time. The longitudinal nature of the MoBa cohort also made it possible to investigate the prospective association between the identified participant profiles and mental health symptoms later in middle childhood and the role that stability versus change in a child’s profile membership across early childhood plays in this regard.
Nonetheless, our study also has some limitations. First, all data were derived from maternal reports. In an effort to account for the influence of maternal mood on their reporting, as previous evidence has suggested in relation to CBCL, we controlled for maternal anxiety and mood in all relevant analyses. However, future investigations should aim at replicating the present results using data from self-reports or other informed reporters, such as teachers, especially in later childhood, when more severe mental health symptoms may start manifesting. Second, only a subset of CBCL items was included in the MoBa questionnaires. Perhaps as a result, the internal consistency coefficients of the two scores were somewhat low, particularly for the aggression score at age 3. However, it should be noted that there have been previous validations of this specific subset of items, including the demonstration of high effect size of correlations between the full internalizing and externalizing CBCL domains and the respective MoBa scores (Helland et al., 2018; Zachrisson et al., 2013).
Notwithstanding, the use of only a subset of CBCL items may also limit comparability of our findings to other studies. This is because we could not use the equivalent CBCL scales of interest or calculate T-scores to establish the percentage of participants that would meet the criteria for a clinical diagnosis. Subsequent investigations should replicate these findings using the full list of CBCL items, given its good diagnostic properties in Norwegian samples (Nøvik, 1999).
Related to this point, the present investigation resulted in interesting and meaningful findings in a normative cohort. However, it is important to ask similar research questions in cohorts wherein clinical data are available and would allow for estimating the number of children that ultimately received a diagnosis, or populations with clearly identified risk, such as children exposed to specific environmental risk factors.
In conclusion, in the present study, we built upon earlier evidence on one’s risk for the development of mental symptoms in middle childhood, conveyed by co-occurrent internalizing difficulties and aggression in early childhood. Most importantly, although this co-occurrence may be somewhat unstable in early childhood, when present, it associates with high levels of depression, anxiety, and OD symptoms later in life. This signifies the potential continuation of this co-occurrence across childhood and further implies that it may associate with clinical levels of internalizing-externalizing comorbidity in later childhood or adolescence. To our knowledge, this is the first study to investigate the stability of this co-occurrence during early childhood and its association with mental health symptoms in middle childhood. The findings lend additional support to the notion that membership in a co-occurring profile may increase one’s risk for more severe forms of psychopathology later in childhood or adolescence.
Supplemental Material
sj-docx-1-jbd-10.1177_01650254231187902 – Supplemental material for Co-occurrence of internalizing difficulties and aggression in early childhood and risk of mental health problems in middle childhood
Supplemental material, sj-docx-1-jbd-10.1177_01650254231187902 for Co-occurrence of internalizing difficulties and aggression in early childhood and risk of mental health problems in middle childhood by Stella Tsotsi, Shaun Goh, Robert J. Coplan, Evalill Bølstad, Nikolai O. Czajkowski, Dinka Smajlagic and Mona Bekkhus in International Journal of Behavioral Development
Footnotes
Acknowledgements
Data and materials from the Norwegian Mother, Father and Child Cohort Study and the Medical Birth Registry of Norway used in this study are managed by the national health register holders in Norway (Norwegian Institute of Public Health) and can be made available to researchers, provided approval from the Regional Committees for Medical and Health Research Ethics (REC), compliance with the European Union General Data Protection Regulation (GDPR) and approval from the data owners. The consent given by the participants does not allow for storage of data on an individual level in repositories or journals. Researchers who want access to data sets for replication should apply through ![]() . Access to data sets requires approval from The Regional Committee for Medical and Health Research Ethics in Norway and an agreement with MoBa. The analytic code necessary to reproduce the analyses presented in this paper is not publicly accessible but can be available upon request to the corresponding author. The analyses presented here were not preregistered.
. Access to data sets requires approval from The Regional Committee for Medical and Health Research Ethics in Norway and an agreement with MoBa. The analytic code necessary to reproduce the analyses presented in this paper is not publicly accessible but can be available upon request to the corresponding author. The analyses presented here were not preregistered.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Norwegian Mother, Father and Child Cohort Study is supported by the Norwegian Ministry of Health and Care Services and the Ministry of Education and Research. We are grateful to all the participating families in Norway who take part in this ongoing cohort study. This study was also supported by funding from the Research Council of Norway (RCN: 301004, RCN: 288083).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.