
Abstract
Evidence on how co-occurrent internalizing difficulties (ID) and aggression in early childhood influence mental health in adolescence is rather limited. Moreover, despite known heterogeneity in symptoms and comorbidities, sex differences in the association between early childhood difficulties and adolescent mental health remain largely unexplored. We investigated these gaps with data from the prospective Norwegian Mother, Father and Child Cohort Study (MoBa). Mothers reported on child ID and aggression at age 5 (n = 11,996; 6,459 girls). Adolescents reported on life satisfaction, prosocial skills, depression, anxiety and conduct disorder symptoms, psychopathy, and psychotic tendencies and psychotic-like experiences at age 14. At age 5, children were classified in one of four profiles based on ID and aggression, that is, low-symptom/normative; primarily internalizing; primarily aggressive; co-occurrent. Adolescents in all three risk profiles reported lower life satisfaction; those in the primarily aggressive profile reported lower prosocial skills. Children in the co-occurrent profile reported higher depressive, anxiety and psychosis-related difficulties in adolescence, whereas primarily aggressive children reported higher depressive, conduct-related and psychosis-related difficulties and psychopathy. Sex did not significantly moderate these associations. Co-occurring internalizing problems and aggression during preschool signal increased risk for lower mental well-being and higher mental ill-being in adolescence, but with no evidence of sex differences. Early identification and preventive interventions, especially targeting aggression and co-occurring problems, may contribute to reducing later risk, including developing psychosis.
Introduction
In early childhood, both internalizing and externalizing problems are uniquely predictive of a host of negative adjustment outcomes over time (e.g., Arslan et al., 2021). However, recent evidence increasingly supports the co-occurrence of internalizing and externalizing difficulties (e.g., Bista et al., 2025; Isdahl-Troye et al., 2022) as early as age 3 years (Tsotsi et al., 2023). For example, subgroups of children with co-occurrent difficulties have emerged from person-centered approaches, in addition to low-symptom/low-risk subgroups, and children with only (i.e., ‘pure’) internalizing or externalizing difficulties (Isdahl-Troye et al., 2022; Tsotsi et al., 2023; Wang et al., 2020). Although shifts between profiles may occur over time, especially in early childhood, child membership in a co-occurrent subgroup exhibits relatively stability across the preschool years (Tsotsi et al., 2023), but also over longer developmental periods, even extending to late adolescence (Brieant et al., 2025). Such stability is observed despite gains in cognitive or emotional domains across development and is suggestive of continuous risk and time-invariant underlying mechanisms, including genes, temperament, and life events with lingering effects (e.g., parents living in separate households; Bista et al., 2025; Wichstrøm et al., 2017).
Evidence for the continuity of risk for co-occurring internalizing and externalizing symptoms also stems from studies of prospective associations between co-occurrent subgroup membership in early/middle childhood and later mental health problems. For example, Tsotsi et al. (2023) reported that children with co-occurrent internalizing and aggression difficulties at ages 3 and 5 years exhibited higher levels of depressive, anxiety, and opposition-defiant symptoms at age 8 years compared to children with only internalizing or externalizing difficulties. Similarly, there is evidence to suggest that children with co-occurrent difficulties are: (1) at higher risk for meeting diagnostic criteria for personality or depressive disorders in pre-adolescence (Winsper et al., 2020); (2) more likely to attempt suicide in young adulthood (Commisso et al., 2023); and (3) score lower on measures of social and economic growth as adults (Vergunst et al., 2023). Notwithstanding, there is still a relative paucity of research examining associations between co-occurrence in early childhood and mental health outcomes in adolescence, especially based on self-reports or interviews (rather than reports by parents or others).
Adolescence is an important and unique developmental period for assessing mental health outcomes, as it is at this age when mental health disorders frequently emerge (World Health Organization, 2025). Although heterogeneity in symptom patterns, comorbidities, and trajectories is well documented, possible sex differences in the association between such difficulties early in childhood and aspects of mental health in adolescence have yet to be specifically explored. Such differences are worth considering given previous evidence of sex differences in youth mental health difficulties, including trajectories of distinct symptom dimensions (Murray et al., 2022). For example, antisocial disorders are more commonly observed in males, whereas symptoms of depressive or eating disorders are more frequent among females (Martin & Hadwin, 2022).
As the idea of how early risk influences later outcomes in children is not new, the primary goal of the present study was to contribute additional knowledge by exploring links between early risk for mental health difficulties at age 5 years and self-reported well-being and mental health outcomes in adolescence, with a particular emphasis on potential sex differences. Our first aim was to investigate whether child membership in different risk profiles identified at age 5 years (i.e., primary internalizing, primarily aggressive, co-occurrent, normative) would differentially associate with self-reported indices of mental health and well-being at age 14 years. We hypothesized that the co-occurrent group would report the highest mental ill-being and the lowest mental well-being scores. Our second aim was to assess the moderating role of child sex in these associations; no a priori hypotheses were formulated regarding the direction of these findings.
Method
Participants and Procedures
The Norwegian Mother, Father and Child Cohort Study (MoBa) is a population-based pregnancy cohort study conducted by the Norwegian Institute of Public Health. Participants were recruited from all over Norway from 1999 to 2008. The women consented to participation in 41% of pregnancies. The cohort includes approximately 113,632 children, 94,834 mothers and 75,229 fathers (Magnus et al., 2016). Out of this initial sample, maternal questionnaire response rates were 54% for the 5-year-old time-point (Schreuder & Alsaker, 2014) and 26% for the 14-year-old time-point, www.fhi.no/en/ch/studies/moba/for-forskere-artikler/moba-research-data-files/). In the present study, mother-child dyads were further excluded if children were twins, had a 5 min Apgar score of ⩽ 7 or had a diagnosis for a genetic syndrome or neurological damage/disorder or autism-spectrum disorders or developmental delay at age 5 or 14 years. Data attrition is outlined in detail in Figure S1 (Supplement). Included participants (n = 11,996; 6,459 girls) had obtained profile membership at age 5 years and provided complete data on at least one of eight outcomes at age 14 years.
A description of attrition in the overall MoBa cohort can be found in Vejrup et al. (2022). With regards to the present study, additional comparisons were conducted between 11% of the original MoBa participants who are included in the present study and the remaining 89% of participants who essentially did not have available data at 14 years of age. Except for birthweight, significant differences were noted in terms of child sex, maternal education, maternal age at birth, marital status of the parents, maternal mental health during pregnancy, number of children in the household and mother tongue as a proxy of ethnicity. The effect sizes for these differences were all very low (Cohen’s d = 0.05 to 0.13). Mothers of included children were older when they gave birth, attained higher education, were more likely to live with the child’s father, reported lower mental health difficulties during pregnancy and had more children. In addition, comparisons were conducted between included children who had available data at both 5 and 14 years of age (33%) and the remaining 67% of children who only had available data at 5 years for aggression and internalizing problems. Despite small effect sizes (Cohen’s d = 0.09 to 0.17), included children manifested lower levels of both aggression and internalizing problems. Thus, in the present study, a disproportionate number of participants with high-risk characteristics is excluded. Still, given the small effect sizes of the observed differences, it is unlikely that the pattern of reported associations would be affected.
The current study is based on version 12 of the quality-assured data files released for research in 2021. The establishment of MoBa and initial data collection was based on a license from the Norwegian Data Protection Agency and approval from the Regional Committees for Medical and Health Research Ethics. The MoBa cohort is currently regulated by the Norwegian Health Registry Act. The study was approved by the Regional Committees for Medical and Health Research Ethics (REK-2009/1899-7; 2013/2061) and the Norwegian Center for Research Data. All participants have provided their informed consent prior to participation.
Measures
Child Profiles at Age 5 Years
Child ID and aggression were assessed using items from the Child Behavior Checklist (Achenbach & Rescorla, 2000). The selection of items used in MoBa was conducted by a team of clinical and developmental psychologists based on theoretical and empirical representativeness. Mothers reported whether they agreed with each item on a three-point Likert-type scale ranging from 0 to 2. Aggression was assessed with four items (raw score range: 0–8) and internalizing difficulties were assessed with ten items (raw score range: 0–2; Tsotsi et al., 2023).
Using these two scores, MoBa children were previously classified into one of four profiles at age 5 years (Tsotsi et al., 2023). The four profiles emerged following a latent profile analysis (LPA) using maximum likelihood with robust standard errors and full information maximum likelihood for missing data estimation. The two scores described above, that is, ID and aggression, were used as the indicators in the LPA models. Models consisting of 1–6 profiles were tested using several fit statistics (Asparouhov & Muthén, 2012), including the Akaike Information Criterion, the Bayesian Information Criterion (BIC), and the sample size-adjusted Bayesian Information Criterion, the bootstrapped likelihood ratio test and the entropy criterion. The decision to retain the four-profile solution was based on the combination of the BIC index (lower BIC value, compared to the two- and three-profile solutions) and entropy (higher entropy compared to the five- and six-profile solutions) values, along with overall model parsimony and interpretability of the profile solution. This four-profile solution was the easiest to interpret (i.e., low-symptom/normative, internalizing difficulties-based, aggression-based, co-occurrent). Profile A was labeled as “low-symptom/normative” and manifested the lowest scores on both ID and aggression. Profile B was labeled as “primarily aggressive” and included children with low levels of ID and moderate levels of aggression. Profile C was labeled as “primarily internalizing” and included children with low levels of aggression and moderate levels of ID. Profile D was labeled as “co-occurrent” and consisted of participants with high levels of ID and moderate levels of aggression. In the present sample, the normative profile included 9,843 children (82% of the sample), the primarily aggressive profile included 1,123 children (9.4% of the sample), the primarily internalizing profile included 860 children (7.2% of the sample), and the co-occurrent profile included 170 children (1.4% of the sample).
Indices of Mental Health and Well-Being at Age 14 Years
Adolescents completed several measures assessing aspects of mental health and well-being. These included: (1) the Satisfaction with Life Scale (Diener et al., 1985), comprised of 5 items rated on a 7-point scale, and with internal consistency in the present sample of α = .92; (2) the prosocial subscale of the Strengths and Difficulties Questionnaires (Goodman, 2001), 5 items rated on a 3-point scale, α = .66; (3) the Short Mood and Feelings Questionnaire (Messer et al., 1995), 13 descriptive phrases assessing symptoms of depression, rated on a 3-point scale, α = .90; (4) the short version of the Screen for Child Anxiety-Related Disorders (Birmaher et al., 1997), 5 items rated on 3-point scale, α = .70; (5) Rating Scale for Disruptive Behavior Disorders (Silva et al., 2005), 8 items assessing symptoms of conduct disorder rated on a 6-point scale, α = .69; (6) the child version of the Young Psychopathic Traits Inventory (van Baardewijk et al., 2008), 11 items describing manipulative, callous, or impulsive behaviors rated on a 5-point scale, α = .76; (7) an adapted version of the Examination of Anomalous Self-Experience Symptom Checklist (Parnas et al., 2005) assessing psychotic tendencies with three items (created by combining items of the original measure) rated on a 3-point scale, α = .80; and (8) the Community Assessment of Psychic Experiences (Capra et al., 2013), assessing persecutory ideation, bizarre experiences, and perceptual abnormalities using the 15-item version of this measure plus one item from the 9-item version (16 items in total) rated on a 4-point scale, α = .83.
Covariates
For all analyses, we controlled for: (1) birth weight adjusted for gestational age; (2) child sex (at birth, obtained from the National Birth Registry of Norway); (3) mother tongue (as a proxy of ethnic background); (4) number of children in the household; (5) maternal education; (6) maternal working status; (7) relationship status of the study child’s biological parents; (8) the child’s school grade; and (9) maternal anxiety/depression at age 5 years (as a means for controlling for reporter bias at that age).
Maternal anxiety and depression were assessed using the eight-item version of the Hopkins Symptoms Checklist (Derrogatis et al., 1973; Tambs & Røysamb, 2014). Mothers were asked to rate anxiety (four items) and depressive mood (four items) during the past 2 weeks on a 4-point scale. Internal reliability in the present sub-sample was α = .75 (anxiety) and α = .81 (depressive mood).
Data Analytic Plan
Statistical analyses were conducted in R (http://www.r-project.org) using the lavaan (Rosseel, 2012) and semhelpinghands (Cheung, 2024) packages. To address our first aim, eight multivariable linear regressions were conducted with the categorical four-profile variable at age 5 years as the main independent variable and each of the eight mental health outcomes as the dependent variable, controlled for the confounders listed above. To address our second aim, we conducted the same eight multivariable regressions, adding interaction terms between child sex and each of the three risk profiles. When an interaction term was significant, we conducted multivariable regressions for that outcome variable, separately for boys and girls, additionally controlling for pubertal maturation. Results were subjected to Bonferroni correction for multiple comparisons based on the number of outcomes, that is, eight; only results at p < .006 will be reported as significant. Missing values (see Table 1) were imputed through multiple imputations.
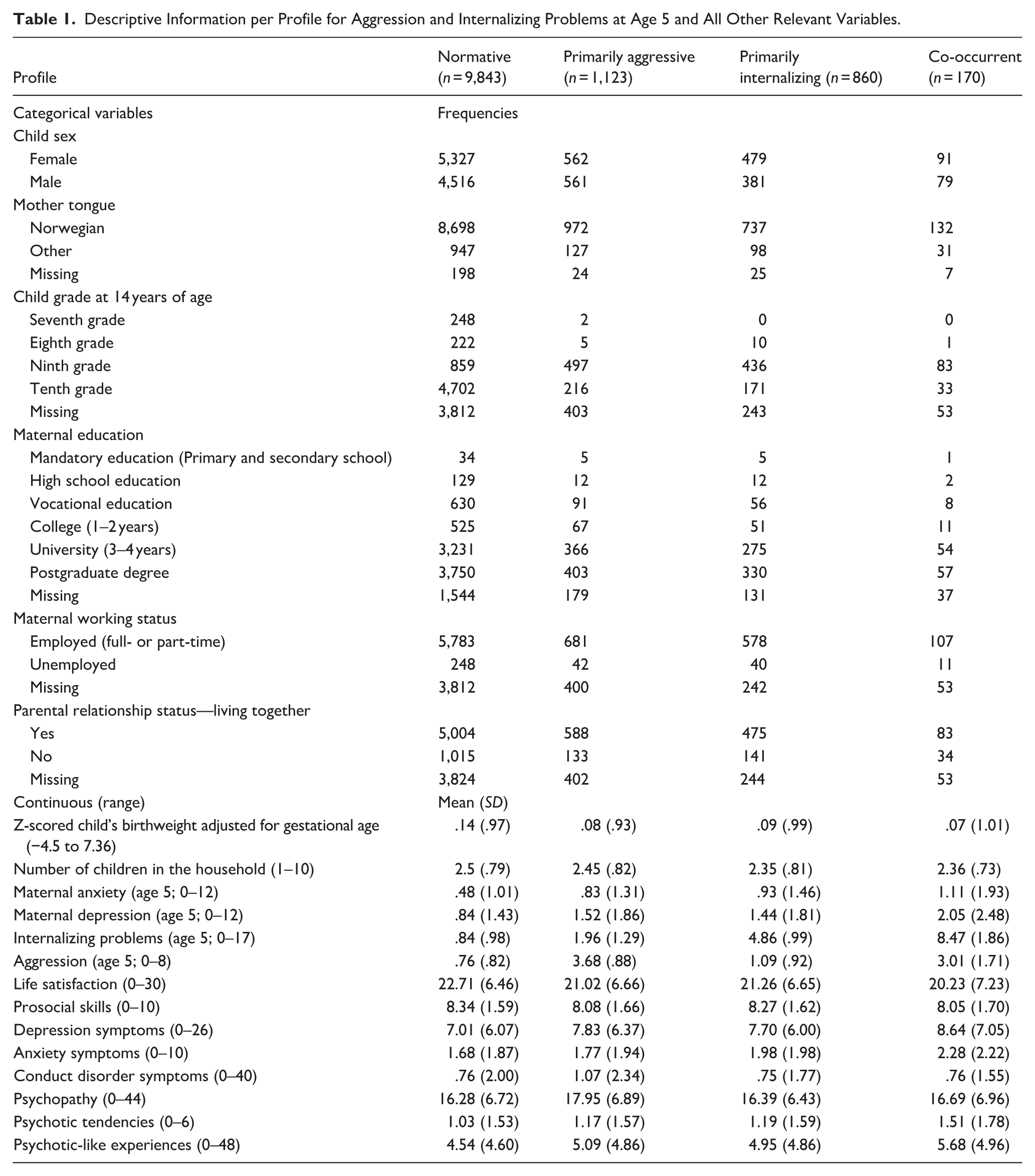
Descriptive Information per Profile for Aggression and Internalizing Problems at Age 5 and All Other Relevant Variables.
Results
Table 1 presents descriptive information per profile. Correlations between variables are presented in the supplement. Of note, males were significantly more likely to be members of the primarily aggressive profile than females.
Results from linear regressions predicting each of the eight outcome variables are displayed in Table 2. For indices of well-being, children belonging to a risk profile reported significantly lower life satisfaction compared to children in the normative profile. As well, children in the primarily aggressive profile reported lower scores compared to those in the normative profile.
Results of Multivariable Linear Regressions Assessing the Association Between Membership in One of the Three Risk Profiles at Age 5 Years and Mental Health Symptoms at Age 14 Years.
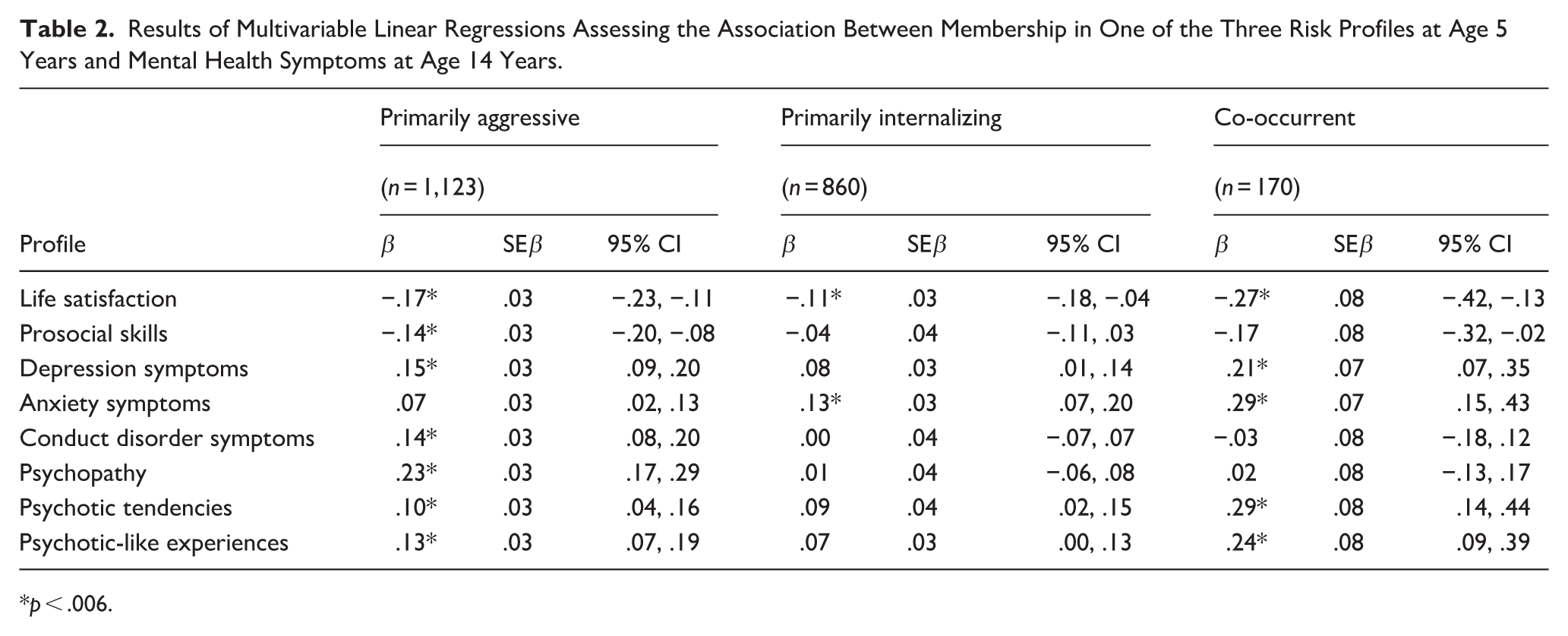
p < .006.
For indices of ill-being, children in the primarily aggressive profile reported higher scores on depressive symptoms, conduct disorder symptoms, psychopathy, psychotic tendencies and psychotic-like experiences compared to children in the normative profile. Children in the primarily internalizing profile reported higher scores on anxiety symptoms compared to those in the normative profile. Children in the co-occurrent profile reported higher scores on depressive symptoms, anxiety, psychotic tendencies, and psychotic-like experiences compared to children in the normative profile (see Table 2).
With regards to our second aim, for indices of well-being although girls reported significantly higher prosocial skills and boys reported significantly higher life satisfaction, no significant interaction effect emerged. For indices of ill-being, girls reported significantly higher depression and anxiety symptoms, psychotic tendencies and psychotic-like experiences, whereas boys reported higher conduct disorder symptoms. No sex differences were noted in the association between the three risk profiles and indices of well-being or ill-being (Table 3).
Results of Multivariable Linear Regressions Assessing the Interactive Effect of Child Sex and Membership in One of the Three Risk Profiles at Age 5 Years on Mental Health Symptoms at Age 14 Years.
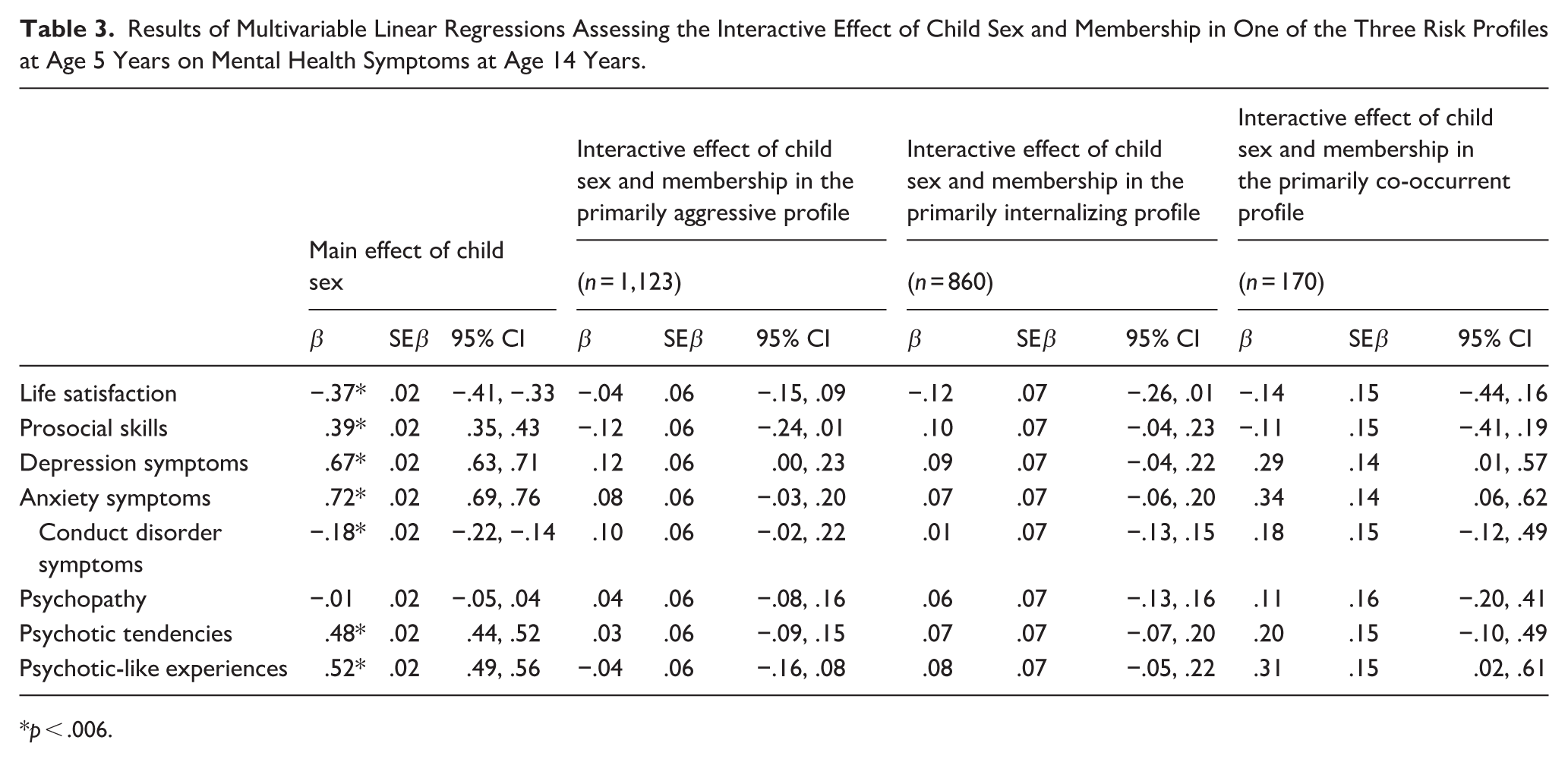
p < .006.
Discussion
The primary goal of this study was to investigate associations between young children’s membership in risk profiles (i.e., primary internalizing, primarily aggressive, co-occurrent, normative) and self-reported indices of well-being and mental health at age 14 years. Our findings indicated lower life satisfaction among all risk profiles and lower prosocial skills in the primarily aggressive profile. Children in the co-occurrent and primarily aggressive profiles reported higher depressive and psychosis-related difficulties in adolescence. In addition, children in the co-occurrent profile reported higher anxiety, whereas children in the primarily aggressive profile reported higher conduct-related difficulties and psychopathy. These findings are consistent with our earlier findings on outcomes at age 8 years (Tsotsi et al., 2023) and other longitudinal investigations (Bista et al., 2025; Isdahl-Troye et al., 2022), suggesting that this early risk continues further into adolescence. Notably, here, our findings are based on adolescent self-reports, extending the robustness of these findings beyond potential concerns of shared-method variance, and implying that adolescents’ experience and perception of their own mental health echoes the risk identified by their parents earlier in childhood.
Regarding the moderating role of sex, although sex differences were observed in relation to well-being and ill-being in adolescence, the role of early risk in the form of mental health difficulties was similar for girls and boys. Adolescent girls and boys may thus differ in the symptom dimensions they manifest in adolescence, notwithstanding their similarity in early risk during the preschool years. These findings echo earlier longitudinal work suggesting that despite similar initial levels in emotional and conduct symptoms in early childhood, their subsequent slope of development differs between girls and boys (Álvarez-Voces et al., 2024). It is also possible that the aggression dimension in girls may proceed in a decreasing manner, as has also been previously observed throughout middle and late childhood (Álvarez-Voces et al., 2024; Brieant et al., 2025). These findings are also in line with earlier work suggesting that despite similarities in comorbid conduct-related and internalizing psychopathology between girls and boys in childhood, girls manifested with higher probabilities for lifetime diagnoses of internalizing nature (e.g., anxiety-related disorders; Konrad et al., 2022).
Our investigation has been the first to assess the association between co-occurrent difficulties and later psychotic-related difficulties. Children in the primarily aggressive and co-occurrent profiles exhibited a higher risk for psychotic-related difficulties. This finding suggests that one’s risk for experiencing psychotic-related difficulties increases when one has struggled with aggression as a child, irrespective of whether it manifested alone or in co-occurrence with other symptoms. Earlier evidence has also pointed toward similar links between antisocial behaviors in childhood and the development of psychotic symptoms (Gin et al., 2021) or psychotic-oriented personality traits (Arslan et al., 2021) in adulthood. Previously specific types of psychotic-like experiences were more prevalent among girls than boys (Wu et al., 2022). In the present study, higher levels of psychotic-related difficulties were also noted in adolescent girls, but the association of such difficulties with early risk was similar for girls and boys. This presents two possibilities for further exploration: refining early childhood symptom and trait constellations and including external factors when examining sex differences in psychosis development in adolescence.
Notwithstanding, results from this study should be considered within the context of some limitations. Data were derived from maternal reports at age 5 years and self-reports at age 14 years. To account for reporter bias at age 5 years, we controlled for maternal anxiety and mood at that time-point in all relevant analyses. Future investigations should aim at replicating the present results using clinical interviews or patient registry data to understand how many adolescents do in fact fulfill criteria for a diagnosis. As only a subset of items was included for some of the MoBa questionnaires, limiting comparability to other studies, replication after using more comprehensive measurements is warranted. Generalizability of the findings may be somewhat limited due to attrition in MoBa cohort which led to a lower number of participants with high-risk characteristics being included in the present study. While the present findings are still meaningful from a population-based standpoint, it is important to ask similar research questions in populations with clearly identified risk, such as children with clinically identified comorbidities or those exposed to specific environmental risk factors.
The present study builds upon earlier evidence on one’s risk for the development of mental symptoms, including psychotic-related difficulties, in adolescence, as this is conveyed by co-occurrent ID and aggression in early childhood. Importantly, the findings highlight the lack of sex differences at large, both in terms of mental well-being and ill-being. Besides the importance of identification and preventive interventions in early childhood, tackling aggressive or co-occurrent difficulties early may hinder later risk for developing psychosis.
Supplemental Material
sj-docx-1-jbd-10.1177_01650254261438685 – Supplemental material for Co-occurrence of internalizing difficulties and aggression in preschoolers and mental health outcomes in adolescence
Supplemental material, sj-docx-1-jbd-10.1177_01650254261438685 for Co-occurrence of internalizing difficulties and aggression in preschoolers and mental health outcomes in adolescence by Stella Tsotsi, Robert J. Coplan, Nikolai O. Czajkowski and Mona Bekkhus in International Journal of Behavioral Development
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Norwegian Mother, Father and Child Cohort Study is supported by the Norwegian Ministry of Health and Care Services and the Ministry of Education and Research. We are grateful to all the participating families in Norway who take part in this ongoing cohort study. This study was also supported by funding from the Research Council of Norway (RCN:301004, RCN: 288083).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data and materials from the Norwegian Mother, Father and Child Cohort Study and the Medical Birth Registry of Norway used in this study are managed by the national health register holders in Norway (Norwegian Institute of Public Health) and can be made available to researchers, provided approval from the Regional Committees for Medical and Health Research Ethics (REC), compliance with the European Union General Data Protection Regulation (GDPR) and approval from the data owners. The consent given by the participants does not allow for the storage of data on an individual level in repositories or journals. Researchers who want access to data sets for replication should apply through ![]() . Access to data sets requires approval from the Regional Committee for Medical and Health Research Ethics in Norway and an agreement with MoBa. The analytic code necessary to reproduce the analyses presented in this paper is not publicly accessible but can be made available upon request to the corresponding author. The analyses presented here were not preregistered.
. Access to data sets requires approval from the Regional Committee for Medical and Health Research Ethics in Norway and an agreement with MoBa. The analytic code necessary to reproduce the analyses presented in this paper is not publicly accessible but can be made available upon request to the corresponding author. The analyses presented here were not preregistered.
Supplemental Material
Supplemental material for this article is available online.