
Abstract
A 2020 AARP study reported that 1 in 5 people in the United States provide unpaid family care to an adult (AARP and National Alliance for Caregiving, 2020). With the number of individuals 65 and older anticipated to exceed that of children for the first time in U.S. history in 2035, family caregiving will only become more prevalent (AARP, 2018). While caregiving may provide some benefits to caregivers (Schulz et al., 2020), caregiving for an adult family member is often challenging, filled with uncertainty, stress, and changing family relationships (Gibbons et al., 2014; Moral-Fernández et al., 2018). Family caregiving is associated with high levels of stress and strain (Dahlrup et al., 2015; Roth et al., 2009), as well as negative health outcomes such as depression, insomnia, greater diagnosed comorbidities, and lower participation in preventative health behaviors (Bauer & Sousa-Poza, 2015; Hopps et al., 2017; Schulz et al., 1997; Schulz & Martire, 2004; Trivedi et al., 2014; Zwar et al., 2021). Researchers have called for the development of interventions to support family caregivers (e.g. Sorrell, 2014), but a complicating factor for developing products and services for caregivers is that family caregiving is not homogenous. Caregivers differ in the tasks that they perform, the intensity of their caregiving role, their relationship with their care recipient, their economic resources, their personal background, and the nature of the strain (e.g. physical, emotional, financial) that they experience.
The tasks that caregivers perform for their care recipient represent a significant element of the diversity of caregiver experiences, and further, we will argue, play a key role in determining caregiver strain. Caregiving tasks are typically classified into two key domains: instrumental activities of daily living (IADLs) and activities of daily living (ADL). ADLs are a series of activities necessary for daily living such as toileting, bathing, and feeding, while IADLs are a series of activities that allow for independent living such as managing finances, transportation, and laundry (Guo & Sapra, 2022; Lawton & Brody, 1969). Beyond the typical classifications of ADLs and IADLs, caregivers often also help support care recipients’ mental and emotional well-being, help purchase and setup technology devices, or simply provide company for loved ones (Schulz et al., 2016).
Using diary data from an original survey of family caregivers in the United States, we use latent class analysis (LCA) to examine how caregiving tasks may cluster into activity profiles. In doing so, we aim to complement prior research efforts that focus on care tasks as a means of classifying family caregivers (Ali et al., 2022; Brantner et al., 2024; Huang et al., 2021). However, rather than engaging in classification per se, we aim to understand how different clusters of care tasks may be predictive of different kinds of caregiving strain., expanding our understanding of the diversity of caregiver experiences.
To gain a more comprehensive view of how caregiving tasks influence perceived caregiver strain, we conducted an original online survey that includes an expansive array of care-related tasks that go beyond those usually included under the headings of ADLs and IADLs. For example, we include tasks such as keeping a care recipient company, helping with technology issues, and assisting with care for care recipients’ pets in our list of tasks used in the classification process.
Additionally, our survey instrument operationalized caregiving strain across three dimensions: physical, financial, and emotional strain. While other measures of caregiving strain or burden capture these elements, such as the Zarit Caregiver Burden Interview Scale, these measures primarily aim to provide an overall assessment of burden rather than identifying distinct areas of strain (Zarit et al., 1980). In assessing how care task profiles independently relate to these three strain dimensions, product and service providers, as well as policymakers, can better conceptualize the diversity of caregiving situations to more precisely target areas of intervention for the growing number of caregivers in the United States.
Literature Review
What defines a caregiver’s experience? Several prior studies have prominently included sociodemographic characteristics such as gender, age, education status, employment status, and the relationship between caregiver and care recipient in their attempts to classify groups of caregivers (Graven et al., 2021; Janssen et al., 2017; Wiegelmann et al., 2021). For example, to explain differences in quality of life among caregivers of persons with dementia, Janssen et al. (2017) used caregiver demographics (such as age, gender, and education), care recipient condition variables, and caregiving-related stress to identify five types of dementia caregivers. More recently, Graven et al. (2021) included demographic variables (such as age, gender, and geographic location), relationship to care recipient, and social support (among other variables) as indicators for a latent class analysis of caregiver profiles, which were intended to predict caregiver self-care behavior.
Other studies have focused on the intensity of caregiving and the subjective experience of caregivers in understanding critical differences among caregivers (Brantner et al., 2024; Pristavec, 2019). However, these elements fail to highlight how the specific types of tasks caregivers perform fit into the picture. For example, while classifying caregiving using LCA, Brantner et al. (2024) focused primarily on the care experience, specifically using care intensity and strain as group indicators. While focusing on care intensity is key to understanding the caregiving experience, the authors used aggregated measures of intensity, including the number of activities performed and hours of care provided, obscuring the importance of any individual activity in defining the caregiving experience. In another study, Pristavec (2019) uses perceived elements of caregiving burden and benefits to construct latent classes. However, subjective measures of the caregiver experience reveal little about which specific care activities contribute to burden and strain. In the present study, we shift to identifying individual tasks rather than composite measures of care task engagement or subjective experiences to better understand the contributions of different care tasks to strain.
Other studies, including Ali et al. (2022), use activities performed in combination with individual attributes to classify caregivers. Ali et al. used care activities, care intensity, and care regularity to uniquely group caregivers into “care types.” Huang et al. (2021) also used engagement-based classification among a sample of caregivers in Hong Kong, utilizing measures including ADLs and IADLs, financial and emotional support, and decision making. Huang et al. found statistically significant differences in caregiver burden for each class that emerged. Our study follows Ali and Huang’s efforts to classify caregivers in terms of the tasks they perform but with two key differences: first, we expand the range of caregiving tasks, and second, we aim to predict how different clusters of tasks might contribute to physical, emotional, and financial strain.
Further, the present study treats caregiver strain as an outcome, not as a predictor, to examine how strain correlates with specific activity profiles. We do so in contrast with other studies of U.S. caregivers such as Brantner et al. (2024), which use perceived strain, in addition to care tasks, to classify caregivers. Were we to include both subjective experiences (such as strain) and objective care tasks as predictors, we would be unable to distinguish the unique contributions of engagement in care tasks, or combinations of care tasks, to caregivers’ perceptions of strain.
Following Huang et al.’s (2021) caregiver classification study, we use care-task profiles to predict caregiver strain. However, where Huang et al.’s study used a more general measure of caregiver burden (Zarit Caregiver Burden Interview -Short Form), the present study examines how care tasks specifically contribute to three related but distinct elements of caregiver burden: physical, financial, and emotional strain. Prior empirical and theoretical research on caregiver strain and burden suggests that caregiver strain is multi-dimensional, consisting of emotional, physical, and financial aspects (Mui, 1995; Pristavec, 2019; Riffin et al., 2019). Prior studies focus on emotional strain (such as Brantner et al. (2024)) or combine different dimensions of strain into an overall assessment of caregiver burden (Huang et al., 2021; Sung & Chan, 2022). For the purposes of our analysis, we hold physical, emotional, and financial caregiving strain as distinct outcomes, to better understand how different sets of care tasks caregivers perform contribute to different dimensions of strain. In doing so, we offer additional insight into how care tasks influence a caregiver’s subjective experience.
Research Design
Data Collection
Data were collected via the Qualtrics online survey platform. The survey was sent via Qualtrics email distribution to 1,484 individuals who were members of a longitudinal research panel of current and former caregivers maintained by the Massachussetts Institute of Technology AgeLab Since 2018 [Blinded for review], has maintained a sample of U.S.-based unpaid caregivers of adult family members (i.e., anyone in the U.S. who provides unpaid care to a family member over the age of 18) who participate in ongoing caregiving research. The panel is not representative of the population of caregivers in the U.S., as its members have higher educational attainment and less racial variation than the general population. We discuss implications of panel demographics in the Limitations section. While not nationally representative, the panel does allow for longitudinal data collection to track caregiver experiences over time. For the present study, an online questionnaire was sent to panel members to track their daily caregiving activities, serving as a baseline for future longitudinal caregiver activity data collection efforts.
Our survey instrument expressly asks respondents which tasks they perform that they associate with their caregiving role. While other large-scale surveys such as the American Time Use Survey (ATUS) collect similar detailed data, their focus on activities and time use in general may cause them to undercount caregiving activities. For example, one of the most prevalent caregiving tasks respondents reported in our sample was “keeping a care recipient company.” This task may be undercounted in instruments that measure general time use, as respondents may not indicate that a general activity such as watching TV is a caregiving activity, unless they think to go on to specify that this general activity was conducted in addition to or for the purpose of keeping a care recipient company. By focusing specially on caregiving activities, our survey, while not nationally representative, explicitly and directly asks caregivers to consider a considerably wide array of activities they perform that are related to caregiving, including relatively amorphous or indirect activities. Relevant survey instrument items are presented in Supplemental Material.
404 individuals consented into the questionnaire (27% response rate), 296 of whom were current caregivers (exact survey question wording for caregiver classification is displayed in Supplemental Material). For current caregivers, the survey consisted of questions about how they navigate, manage, and perceive various family, work, and caregiving responsibilities and tasks, and how they think about social interactions and any leisure or self-care time they have. Some questions asked about their experiences generally, while others focused on specific time blocks throughout their day “yesterday”. Participants were compensated with a $10 Amazon.com gift card.
Of the 296 current caregivers who began the survey, 244 completed it. 31 caregivers were removed from the sample due to missing data on key classification variables, strain, or sociodemographic information. The final analytic sample consisted of 213 current caregivers to adult family members.
Measures
Caregiving Activities
Current caregivers were asked to think about the previous day and report the care related activities they performed. Caregivers were asked to indicate whether they had performed any of the 36 provided caregiving activities, including help with finances or technology, home or medication management, help with ADLs, or a series of other daily activities. The complete list of activities is presented in Supplemental Table S1. Caregivers were then asked to report which of the reported caregiving activities were performed within each of eight 3-h time blocks spanning an entire day (e.g., 3pm–6pm). Caregivers were considered as performing a care-related task if they reported they had performed that activity the previous day and assigned that activity to one or more of the 3-h time blocks.
Strain
Caregiving strain was conceptualized as a three-dimensional variable. The survey asked respondents, “Overall, how much of a strain is it for you to take care of your care recipient(s)?” Caregivers answered this question for three strain types: physical strain, financial strain, and emotional strain. Responses options were on a 5-point Likert scale from 1 = Not at all a strain to 5 = Very much a strain.
Sociodemographic Characteristics
Caregiver respondents were asked a series of questions to determine their sociodemographic background and caregiving situation. Employment status was operationalized as two dummy variables indicating whether a caregiver was retired (0 = not retired, 1 = retired) and whether the respondent was employed in some capacity (0 = not employed, 1 = employed). We also include a dummy variable for whether a respondent is currently a parent to a child under the age of 18. Residential environment was operationalized as a 3-category variable including urban, suburban, and rural. Total household income before taxes was included as a 3-category variable including less than $75,000, $75,000-$149,999, and greater than or equal to $150,000. Respondents also reported on gender (female, male), whether they lived with their care recipient (0 = live apart, 1 = live together), and their relationship to their current care recipient (spouse or partner, parent or parent-in-law, or other family member). Respondents also indicated how long they had served as a caregiver to their current recipient and responses were coded into 5 categories: 2 years or less, 3-6 years, 7-10 years, 11-15 years, or 16 or more years.
Analysis
Our analysis proceeds in four parts. First, we used latent class analysis (LCA) to classify co-occurring care-related tasks into activity profiles based on the combination of daily caregiving activities they report in the diary study. Thirty-six caregiving activities, spanning four activity groups (finance and technology, management, ADLs, and other daily activities) were used to determine the optimal number of activity profiles. Activity profiles including 2-6 latent classes were tested and compared. While there is no gold-standard measure to determine the optimal number of classes in LCA analysis (Nylund et al., 2007; Weller et al., 2020), we compared a variety of fit statistics and used knowledge about family caregivers to select a statistically sound and operationally meaningful number of caregiving activity classes (Goodman, 2002).
All models demonstrated statistically significant likelihood ratios, or goodness of fit (G2), indicating that all were potential statistically appropriate models compared to a one-class solution. To further compare model fit, AIC (Akaike Information Criteria) and BIC (Bayes Information Criteria) were calculated for each model, with lower numbers indicating better fitting models (Weller et al., 2020). When comparing information criteria, BIC was given more weight as it has been suggested as superior to AIC regarding determining the optimal number of classes (Muthén & Muthén, 2000; Nylund et al., 2007; Weller et al., 2020). Additionally, the magnitude of the likelihood ratios was estimated and compared across models. To determine the optimal number of classes, we examine likelihood ratios, AIC, and BIC, as well as interpretability of class solutions (Muthén & Muthén, 2000; Porcu & Giambona, 2017).
Once the optimal number of activity profiles was selected, we analyzed descriptive statistics for each of the profiles as well as the full sample of caregivers. Here we examined sociodemographic characteristics such as age, household income, gender, and marital status, as well as information about respondents’ caregiving situation, including their relationship with their care recipient, whether they live with their care recipient, and approximately how long they have been providing care to the current care recipient. For each characteristic, we conducted a one-way ANOVA or a chi-squared test to determine if characteristics varied significantly across activity profiles.
Third, we examined potential predictors of profile membership by estimating a multinominal logistics regression model with sociodemographic and caregiving situation variables as predictors and activity profile membership as a categorical outcome variable. Finally, we examined differences in strain across activity profiles by estimating a series of OLS regression models predicting levels of either physical, financial, or emotional strain using profile membership as the primary predictor variable. We also include controls for sociodemographic variables that have demonstrated empirical relationships with caregiver strain including, retirement status, employment status (Brady et al., 2024; Rubin & White-Means, 2009), parent status (Lei et al., 2023), residential environment (Henning-Smith & Lahr, 2019), household income (Willert & Minnotte, 2021) and gender (Sharma et al., 2016; Willert & Minnotte, 2021), as well as variables indicating a respondent’s caregiving situation (whether or not respondent lives with care recipient, relationship to care recipients, and approximately how long they have been providing care to the current care recipient). Predicted physical, financial, and emotional strain were estimated and compared for each activity profile. All analysis was performed in STATA Version 17.
Results
Latent Class Selection
Model Fit Statistics.
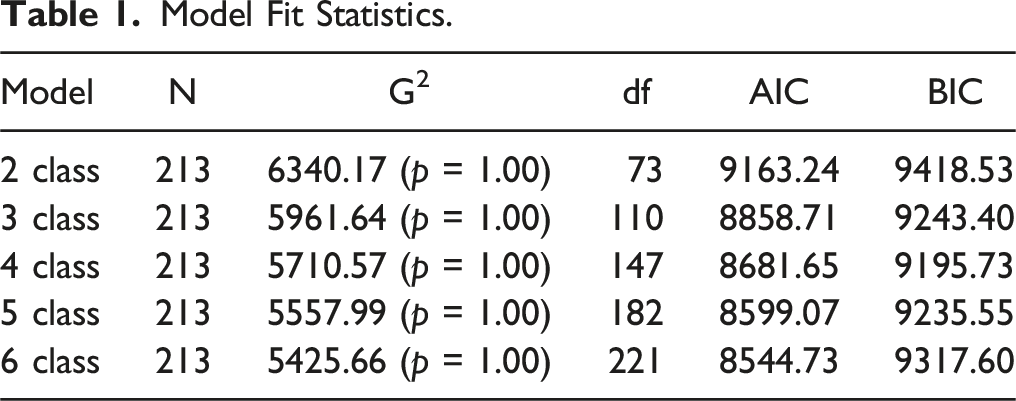
Figure 1 provides illustrations for the specific care-related activities that comprise each activity profiles. The 36 caregiving activities are grouped into four categories. Latent Class Profiles. Note. Numerical results displayed in Supplemental Table S1. Profile 1 = “Little bit of everything”, Profile 2 = “Hands-on”, Profile 3 = “Low demand”, Profile 4 = “The managers”.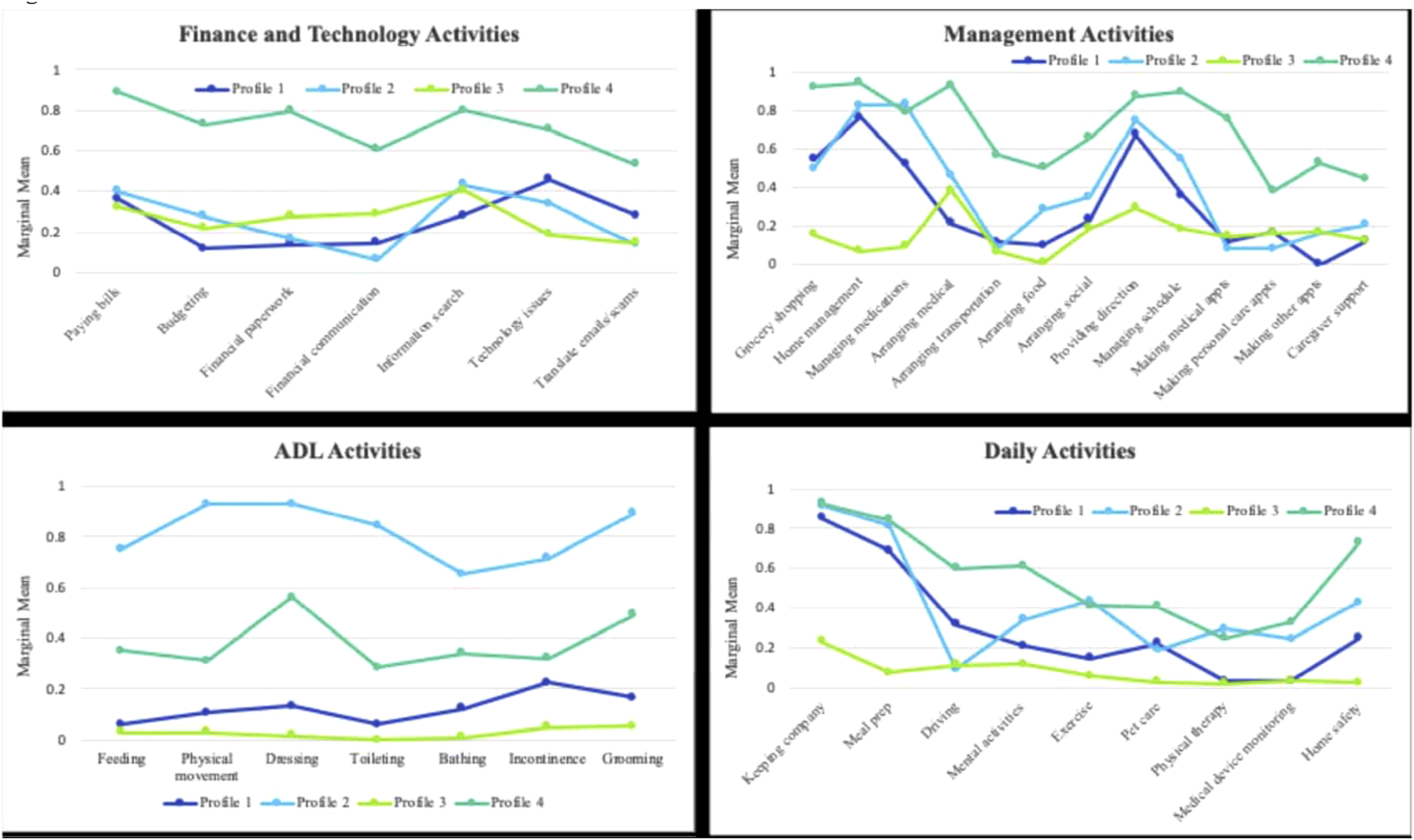
Profile 1 comprises caregivers who perform a variety of caregiving tasks but at lower frequencies than other classes for many activities. Caregivers in profile 1 assist with finance and technology activities and ADLs at a relatively low rate, and they more frequently assist with home management and providing direction to their care recipients. Additionally, caregivers in profile 1 frequently provide company and assist with meal preparation for care recipients. We label this profile “little bit of everything”.
Caregivers in profile 2 engage in a similar number of distinct caregiving activities as caregivers in profile 1, but profile 2 is the most heavily involved in ADLs, with the majority of caregivers performing the majority of tasks in the ADL category. We label profile 2 caregivers “hands-on”.
Caregivers in profile 3 perform the lowest frequency of care tasks across most caregiving activities. Profile 3 caregivers primarily assist with management and financial tasks, especially information search and arranging medical appointments, and perform very few hands-on tasks. We label this profile “low demand.”
Caregivers in profile 4 perform many caregiving tasks as a higher frequency than other activity profiles. Profile 4 caregivers are the most likely to assist with finance and technology and management activities, while also providing support with ADLs and daily activities. We label profile 4 caregivers “the managers”. Marginal means for each of the 36 examined caregiving tasks by activity profile are displayed in Supplemental Table S1.
Latent Class Profile Characteristics
Descriptive Variables for the Total Sample and Each Activity Profile.
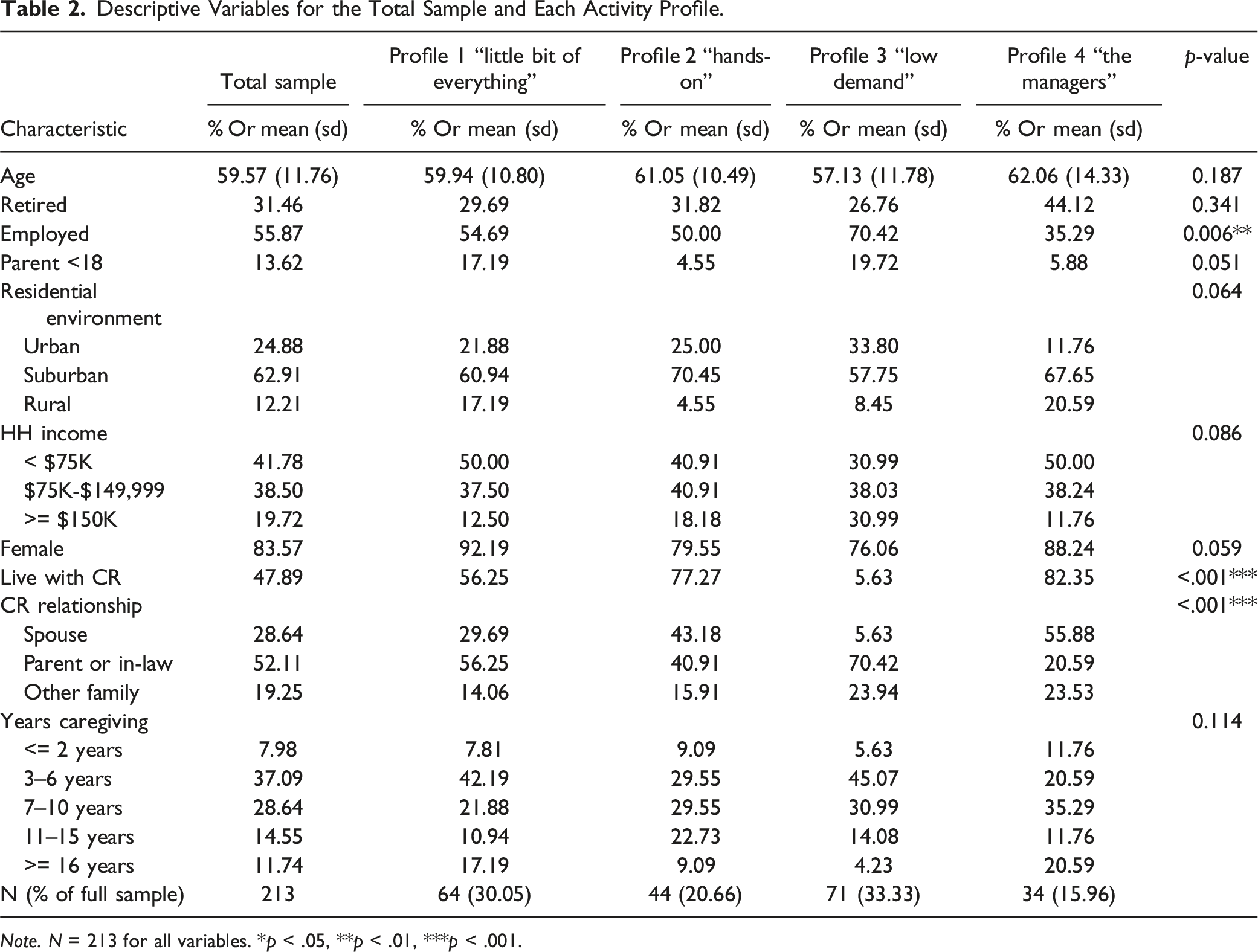
Note. N = 213 for all variables. *p < .05, **p < .01, ***p < .001.
Table 2 also displays descriptive statistics for each activity profile with the last column presenting p-values from one-way ANOVA or chi-squared tests. Employment status varies significantly (p = .006), with the majority (70%) of “low demand” caregivers being employed, while around half of the “little bit of everything” and “hands-on” caregivers reported being employed, and only 35% caregivers in “the manager” profile. A one-way ANOVA of the percent of respondents with children under 18 was marginally significant (p = .051), with “little bit of everything” and “low demand” caregivers containing a higher percent of caregivers with children under age 18 compared to “the managers” and “hands-on” caregivers. A chi-squared test of residential environment across activity profiles was marginally significant (p = .064), with “low demand” caregivers the most likely to live in an urban environment, and “the managers” least likely to compared to other profiles. “Hands-on” caregivers were most likely to live in a suburban environment while “low demand” caregivers were least likely to, compared to the other classes. While the fewest number of caregivers reported living in a rural environment, “the managers” had the highest percent of respondents living in this environment, while “hands-on” caregivers had the lowest percent, compared to other activity profiles. A chi-squared test of household income across profiles was also marginally significant (p = .086). Notably, “low demand” caregivers had the highest percent of respondents in the highest income category (31%) and the lowest percent of respondents in the lowest income category (31%), likely due in part to the high percent of “low demand” caregivers who were employed.
A one-way ANOVA of the percent female was also marginally significant across activity profiles (p = .059), with “little bit of everything” caregivers having the highest percent of females (92%) and “low demand” caregivers having the lowest percent (76%). Living arrangement with a care recipient also showed differences across profiles (p < .001), with under 6% of “low demand” caregivers, 56% of “little bit of everything” caregivers, and approximately 80% of “the managers” and “hands-on” caregivers living with their care recipient. Finally, caregivers’ relationships to their care recipients varied significantly across profiles (chi-squared p < .001), with the majority (56%) of “little bit of everything” and “low demand” caregivers caring for a parent or parent-in-law, a majority (56%) of “the managers” caring for a spouse, and an approximately equal percent of “hands-on” caregivers caring for a spouse (43%) or a parent or parent-in-law (41%).
Predictors of Activity Profile Membership
Multinominal Logistic Regression Model Displaying Predictors of Activity Membership Versus Being in Profile 3 “Low Demand” Caregivers.
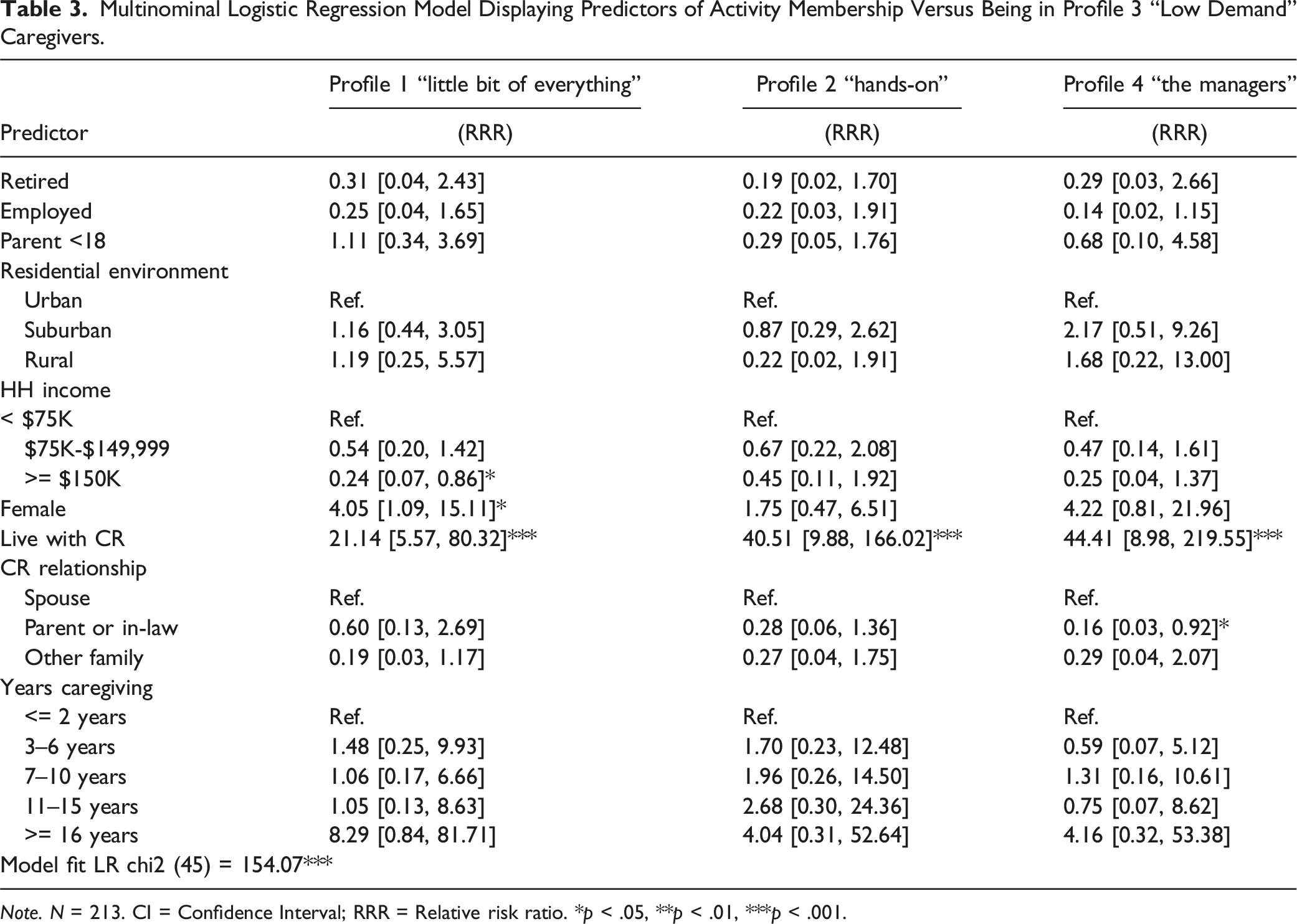
Note. N = 213. CI = Confidence Interval; RRR = Relative risk ratio. *p < .05, **p < .01, ***p < .001.
Strain Differences Accross Activity Profiles
Supplemental Table S2 displays full results for a series of OLS models predicting physical strain, financial strain, and emotional strain among family caregivers by activity profile. From these models, Figure 2 presents predicted physical, financial, and emotional strain by activity class membership. Additional multiple comparison tests using the Bonferroni method (StataCorp, 2023) (not shown) were performed to identify statistically significant predicted strain differences across activity profiles. The “little bit of everything” caregivers (2.46) and the “low demand” caregivers (2.21) displayed the lowest average physical strain, while “hands-on” (3.04) and “manager” caregivers (3.38) had the highest predicted physical strain. “The managers” had the highest predicted financial strain (3.83), which was significantly higher than strain for the “little bit of everything” caregivers (2.32) [p < .001] and the “low demand” caregivers (2.44) [p = .003]. Predicted emotional strain was also significantly higher for “the managers” (4.54) [p < .01 for all comparisons], though all classes displayed relatively high levels of emotional strain (ranging from 3.87 – 4.01). Overall, while the degree of reported physical and financial strain related to caregiving varied by activity profile, all caregivers experienced high levels of emotional strain. “The managers” consistently displayed the highest levels of predicted strain across all three stain types. Predicted Physical, Financial, and Emotional Strain by Activity Profile Membership. Note: N = 213 caregivers. Error bars indicate 95% confidence interval of predicted strain. Full results of physical, financial, and emotional strain OLS regression models are displayed in Supplemental Table S2. Profile 1 = “Little bit of everything”, Profile 2 = “Hands-on”, Profile 3 = “Low demand”, Profile 4 = “The managers”.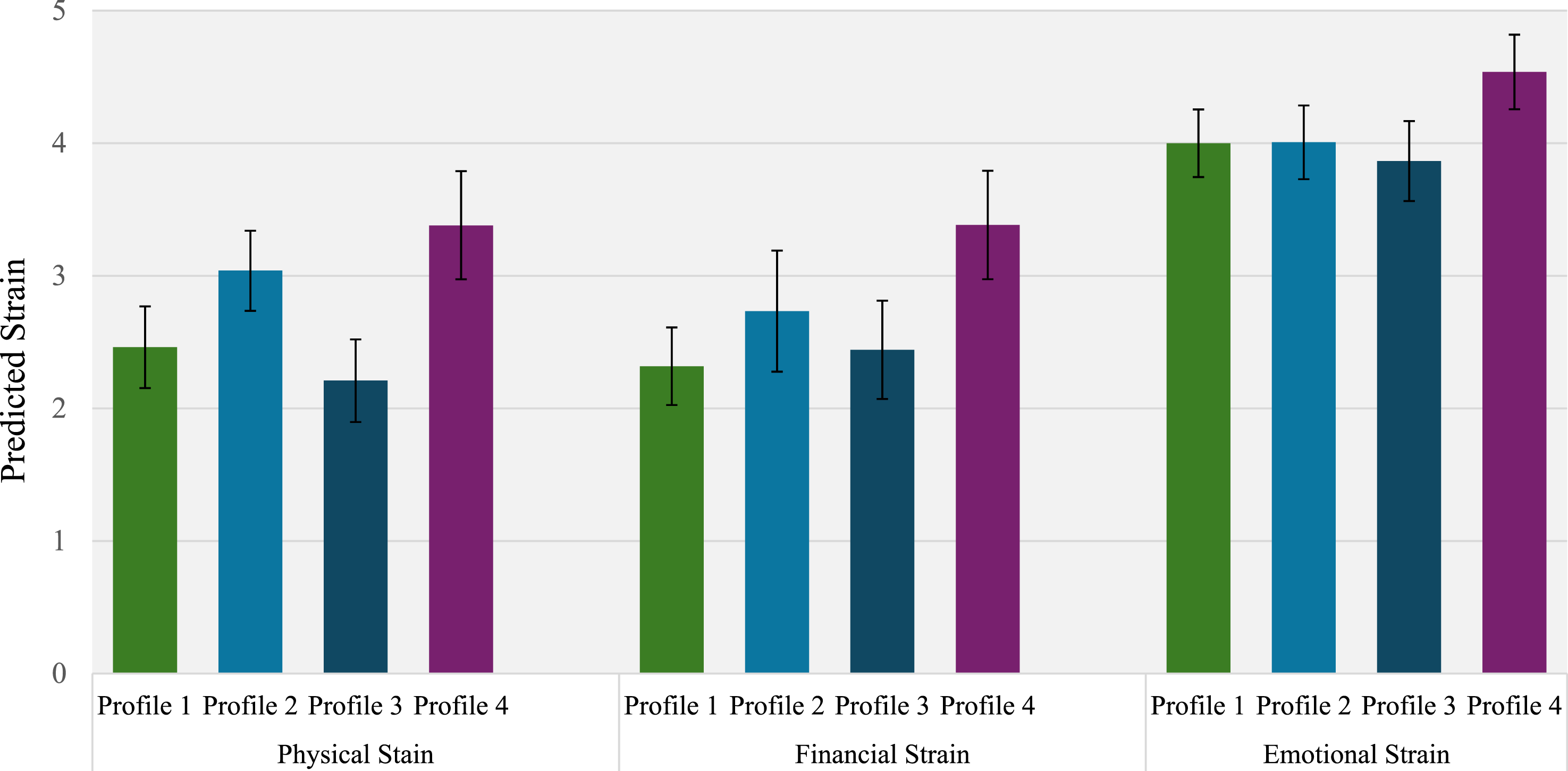
Discussion
The present analysis used original survey data from a diary study of family caregivers to identify caregiver activity profiles based on 36 caregiving tasks performed in a typical day. Diary data allow us to extend prior studies by focusing on a large and comprehensive set of caregiving tasks beyond traditional conceptions of ADLs and IADLs and beyond aggregated measures of activities aimed at capturing the caregiving experience (Brantner et al., 2024). Our study includes caregiving tasks in four primary categories: finance and technology (e.g., paying bills, managing technology issues); management activities (e.g., arranging home and medical services); ADLs (e.g., dressing, bathing); and daily activities (e.g., mental activities, exercising, pet care).
LCA analysis yielded four distinct activity profiles based on caregiving activities performed throughout a day. While the resulting four profiles can be partially distinguished by the number of care tasks performed (i.e., intensity), classes also vary based on the types of care activities caregivers typically perform.
Caregivers across all activity profiles looked relatively similar in terms of sociodemographic characteristics and caregiving situations (i.e., years spent caregiving, relationship with care recipient, and whether caregiver lives with care recipient). In other words, caregivers of similar backgrounds or in caregiving situations did not necessarily perform the same set of care tasks. In our sample, “low demand” caregivers were the most distinctive demographically, as they were likely to be currently employed (likely resulting in higher reports of household income), not living with their care recipient, and likely to be caring for a parent. Not surprisingly, these “low demand” working caregivers were performing the fewest in-person care activities, while primarily assisting with management and financial tasks. However, it was more difficult to distinguish between caregivers in the other three activity profiles using a purely demographic lens. “The managers” were the least likely to be employed (and therefore in the lowest income category), but they were indistinguishable from “little bit of everything” and “hands-on” caregivers across all other characteristics including age, gender, residential environment, and caregiving situation.
The present study also illustrates that caregiver activity profiles are predictive of caregivers’ strain perceptions and experiences. Across all three strain types examined (physical, financial, and emotional), “the managers” reported the highest levels of strain across all categories, while the “hand-on” caregivers reported the second highest physical and financial strain levels. While physical and financial strain levels for the “little bit of everything” caregivers and the “low demand” caregivers were lower than the “hand-on” caregivers and “the managers,” all activity profiles reported relatively high levels of emotional strain associated with their caregiving role. Across strain types, all activity profiles experienced higher levels of emotional strain relative to physical and financial strain. While the “little bit of everything” caregivers and the “low demand” caregivers may have appeared to experience similar levels of strain if it was operationalized as a unidimensional construct, “little bit of everything” caregivers reported higher levels of physical strain, while “low demand” caregivers reported slightly higher levels of financial strain, indicating that different solutions may benefit caregivers comprising this activity profile.
Our findings align with activity-based approaches to understanding the caregiving experience, highlighting that the types of tasks caregivers perform are just as important as the volume of tasks in predicting caregiving strain (Brantner et al., 2024; Huang et al., 2021). For example, Brantner et al. (2024) classified caregivers based on intensity (i.e., the amount of time spent caregiving) and strain, finding that while 13% of caregivers were classified as both high intensity and high strain, nearly a quarter of their sample experienced high caregiving intensity but reported low perceived strain. This suggests that types of caregiving activities play a critical role in shaping strain experiences and perceptions.
An activity-based perspective also implies that strain is driven by the full constellation of activities caregivers engage in, regardless of whether they are related to caregiving. Therefore, when examining caregiver strain, it is also important to consider additional activities caregivers may be involved in that interact with caregiving tasks to influence perceptions of strain. For instance, caregivers who provide care for both an older family member and a child tend to report lower psychological well-being than those caring for a single individual (Hodgdon et al., 2023; Lei et al., 2022). Since no caregivers in our sample were simultaneously caring for a child, we were unable to examine how childcare responsibilities interact with caregiving for an older adult to influence strain. Future research should explore how various activities—including childcare and work—may interact with caregiving tasks to predict strain.
Study results examining caregiver strain highlight the nuanced ways in which strain is perceived and experienced. Our findings suggest that different profiles of caregiving activities contribute in different ways to physical, financial, and emotional strain, emphasizing, that these dimensions of strain are related but distinct. Future research should assess whether interventions such as cash transfers, peer support groups, or respite care more effectively target specific domains of caregiver strain or whether they provide broader benefits across all strain domains. Understanding how interventions impact different aspects of strain can help tailor support strategies to caregivers who would benefit most based on their activity profiles. For instance, while cash transfer programs may effectively alleviate financial strain, they may be less effective in reducing the emotional strain associated with caregiving (Foster et al., 2007; Grootegoed et al., 2010).
Furthermore, our analysis indicates that different kinds of caregiving strain arise to varying degrees depending on the activities that a caregiver performs. Activity profiles may provide a deeper understanding of the causes of different kinds of strain – and so better inform the design of interventions to alleviate strain. If the sorts of activities that caregivers perform are a root cause of different sorts of strain, then interventions may benefit from being designed with the aim of facilitating different sorts of caregiving activities, and, by this mechanism, alleviate strain. Identifying how interventions affect caregivers with specific activity profiles can inform the development of targeted support strategies that align with caregivers' current responsibilities and care activities.
Limitations
While the present study provides insight into task-based care activity classification and how profile membership correlates with various dimensions of strain, it has several limitations. The sample of family caregivers used in the study was relatively limited (N = 213). While caregivers in the sample reported involvement in all 36 caregiving activities used in task-based profile creation, the sample is likely limited in how closely it resembles activity profiles of the population of caregivers in the U.S. In a larger, more representative sample, additional classes of caregiver activity profiles may emerge beyond the four identified in this study. A benefit of our sample, however, is that we were able to directly ask respondents to think about and report care-related activities, which may yield higher reports of care-related tasks than a more general time use survey (e.g., ATUS). Additionally, we were able to capture multiple dimensions of strain directly attributed to caregiving.
Given the modest sample size, we also were not able to explore possible variation by certain caregiver characteristics. Most notably, we were not able to explore how racial identity may correlate with activity profiles given that our sample predominately identified as White (85%). While we found that the majority of demographic characteristics included in our study did not predict activity profile membership, research suggests that caregiving experiences differ by racial identity (Cohen et al., 2019). Future research should examine the extent to which racial identity predicts task-based caregiver activity profiles to gain a deeper understanding of the relationship between racial identity and caregiver strain (Willert & Minnotte, 2021). Additionally, while we included income and employment status in our analyses, we were not able to examine variation by education, as our sample displayed little variation in educational attainment (84% college degree). While income and employment status capture elements of socioeconomic status, our highly educated and less racially diverse sample limits generalizability of our findings. Future research can seek to validate findings of the present study with a more representative sample of caregivers.
While the diary method allowed for comprehensive reporting of caregiving activities, we were only able to collect data for each caregiver over one 24-h period due to resource constraints. It is possible that the day caregivers completed the diary study was not a “typical” caregiving day and may have consisted of greater or fewer care tasks than usual. We attempted to minimize this possibility by fielding the survey on three separate weekdays. Additionally, asking caregivers about the previous day relies on respondent’s recall, which may be less accurate than reporting activities in real-time. Future research may replicate the diary study over a longer period (e.g., a week) and in real-time to develop a more consistent view of family caregiving.
Finally, while the present study found that the task-based caregiver profiles displayed meaningful variation across the three strain dimensions, these profiles may also vary for other caregiver outcomes. Specifically, the strain measures used in the present study capture the subjective experiences of caregivers. However, it is also important to examine more objective measures of caregiving well-being. For example, Brantner et al. (2024) used LCA to classify caregivers based on intensity and strain, finding that the transition into a caregiving role was associated with different magnitudes of change in depressive symptoms as well as physical and cognitive health across caregiver classes. Future research can build on Brantner et al. (2024) as well as the present study to examine how a wider set of caregiver well-being outcomes vary by the comprehensive task-based profiles identified in this study.
Conclusion
The present study employed LCA on data from a sample of unpaid family caregivers in the U.S. to determine unique care-related activity profiles based on reports of 36 care-related activities. Using this approach, we identified 4 distinct activity profiles. Profiles varied minimally by sociodemographic characteristics and caregivers’ care situations; however, profile membership did meaningfully correlate with physical, financial, and emotional strain. Taking a task-based approach allows for a direct identification of what caregivers are doing on a daily basis, and how tasks typically co-occur, providing more direction for product and service providers aiming to support the growing population of family caregivers in the U.S.
We can suggest how the relationship between the activity profiles we identified, and caregiver strain may help point to caregiver unmet needs and potential solutions. For example, the “hands-on” caregivers, who provide high levels of ADL assistance to care recipients, experience high levels of physical strain. Solutions targeted toward caregivers representing this activity profile may focus on helping caregivers physically complete their care tasks. Solutions for “low demand” caregivers, who are most likely to perform finance and management related tasks and report significant financial strain, may focus on helping employed caregivers balance the cost of caregiving with other financial obligations. Overall, this study offers researchers a deeper understanding of the relationships between caregiver activities and their experiences of burden and strain.
Supplemental Material
Supplemental Material - Mapping the Caregiver Experience: Predicting Dimensions of Caregiver Strain Through Task-Based Profiles
Supplemental Material for Mapping the Caregiver Experience: Predicting Dimensions of Caregiver Strain Through Task-Based Profiles by Samantha Brady, Sophia Ashebir, Lisa D’Ambrosio, Alexa Balmuth, Adam Felts, and Chaiwoo Lee in Research on Aging
Footnotes
Author’s Note
This study was approved by Massachusetts’s Institute of Technology’s Committee on the Use of Humans as Experimental Subjects (COUHES) #E-4277.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received financial support from United Church Homes and Transamerica.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.