
Abstract
Loneliness in later life is a significant global public health issue that negatively impacts well-being, life satisfaction, and mental health. This study investigates how material, health, and social vulnerabilities contribute to loneliness among older adults using a welfare regime framework. It examines the link between vulnerability and loneliness in the United States, Korea, Sweden, Spain, and Germany using the Health and Retirement Study (HRS) alongside its international sister studies, encompassing both Western and East Asian welfare states. Findings indicate that older adults in less generous welfare regimes experience higher levels of loneliness and material vulnerability. A multidimensional approach reveals that the most urgently vulnerable population is the multiply vulnerable group. Vulnerable groups are more likely to experience loneliness, with divergent associations emerging across countries. Cross-national variations demonstrate how institutional arrangements can either mitigate or exacerbate the relationship between vulnerability and loneliness.
Loneliness in later life is a major global social and public health issue (Beutel et al., 2017) that affects 25.9% of older adults across countries, including almost 8% who experience severe loneliness (Chawla et al., 2021). Research shows that loneliness has negative impacts on various well-being outcomes, including life satisfaction and depression (Beutel et al., 2017; Cacioppo & Cacioppo, 2018; Galea and Abdalla, 2020). In response to this issue, some countries such as the United Kingdom and Japan have appointed a “loneliness minister” to address loneliness at the national level (World Health Organization, 2021).
Our aim is to contribute to the literature on loneliness by focusing on two aspects that have not been studied enough. Firstly, we highlight the multiple vulnerabilities that increase the risk of loneliness among older adults and examine how they are associated with loneliness. Older adults face challenging circumstances such as reduced income, declining health, and social network, in old age when they have a reduced capacity to respond and adapt to them (Dahlberg et al., 2022; Golaz & Rutaremwa, 2011; Grundy, 2006). These individual risk factors are connected with each other and do not manifest or develop in isolation. Understanding the patterns of multidimensional later life vulnerability is crucial to understand how they are associated with loneliness.
Secondly, we use the welfare regime framework to extend the existing cross-national comparative study on loneliness to include both Western and East Asian welfare states. Previous studies on loneliness have mainly focused on Western countries, especially the comparison between continental/Nordic countries and Southern Europe. East Asian welfare states are characterized by state-led economic growth, a high level of familiarization, and rapid aging. Our study will shed light on loneliness among older adults in East Asian “productivist” welfare states (Holliday, 2000) and whether the patterns of association between loneliness and vulnerability vary across different countries.
This study explores the potential link between vulnerability and loneliness among older adults in the United States, Korea, Sweden, Spain, and Germany. Drawing upon the multidimensional approach to late life vulnerability and existing literature on welfare regimes, the research analyzes the associations between vulnerability patterns and loneliness in these countries. The study aims to shed light on the diversity of older adults’ experiences and the role of institutional factors in shaping the association between vulnerability and loneliness. This knowledge can inform the development of effective programs and policies to address loneliness in later life.
Loneliness and Vulnerability Among Older Adults
Loneliness is a complex and multifaceted experience, often characterized by feelings of aloneness, depression, and a sense of isolation from others (Huang et al., 2010). Loneliness is not just a subjective experience but also a distressing one, often arising from a deficiency in an individual’s social relations stemming from a perceived discrepancy between desired and actual social relationships (Perlman & Peplau. 1981). It is a universal human experience that can lead to depression and low self-esteem (Bekhet et al., 2008). The importance of loneliness in promoting older populations’ well-being is increasingly recognized by researchers and policymakers internationally (Cattan et al., 2005). As a critical social determinant of health, loneliness should be studied as a social and cultural phenomenon (Lykes & Kemmelmeier, 2014; Weldrick & Grenier, 2018) beyond just an individual or psychological level. According to Ong’s study (2016), approximately 25% to 29% of older adults in the United States aged 70 and older report experiencing loneliness based on estimates. Recent studies have shown that loneliness among the older population is associated with various negative health outcomes, including depression (Cacioppo et al., 2006), mental health problems (Coyle & Dugan, 2012), and even increased mortality risk (Holt-Lunstad et al., 2015).
We highlight the concept of vulnerability as a factor for loneliness among older people. The vulnerability concept has recently received much attention in academic research and social practice to understand the disadvantages of aging (Brown et al., 2017; Virokannas et al., 2020). As consequential status derived from complex interactions among discrete risks, a vulnerability in old age is characterized by unpreparedness to deal with difficulties or challenges in various key life domains such as social life, health status or economic status (Kirby, 2006; Schroeder-Butterfill & Marianti, 2006; Virokannas et al., 2020). Studies found that vulnerability includes reduced individual relationships, such as not being married/partnered and partner loss, a limited social network, a low level of social activity, to poor self-perceived health (for reviews, see Dahlberg et al., 2022) and material conditions of income and wealth (Kourouklis et al., 2020).
For a comprehensive examination of late life vulnerability, we draw on the literature on vulnerability in later years in four major life domains: material, physical health, social, vulnerability. Understanding multidomain vulnerability is crucial, as risks across various life domains often interact and compound, amplifying challenges and leading to more significant disadvantages. Examining these vulnerabilities simultaneously provides valuable insights into their combined impact on well-being, particularly in later life (Schröder-butterfill & Marianti, 2006). This approach highlights the interconnected nature of vulnerabilities and underscores the importance of addressing them holistically to improve outcomes for older adults. The material vulnerability relates to economic hardship, such as unmet needs for health care, food, and housing (Alley et al., 2009). Material vulnerability encompasses concepts such as poverty, housing insecurity, and unmet healthcare needs, all of which are linked to poorer health outcomes and increased mortality risk (Bassuk et al., 2002; Bossé; Park & Seo, 2022). Physical vulnerability in later life refers to an increased susceptibility to adverse health outcomes, encompassing chronic illnesses as well as functional impairments such as reduced mobility, weakness, and challenges in performing activities of daily living (ADLs) (Fried et al., 2001). This vulnerability is often intensified by frailty, a condition marked by diminished strength, endurance, and physiological resilience. Frailty places older adults at heightened risk for falls, disability, and mortality (Clegg et al., 2013), making it a critical factor in understanding and addressing physical vulnerability in aging populations. Social vulnerability is defined as the deficits in social factors such as frequency of contact with others and social engagements (Moor et al., 2013; Wallace et al., 2015). Reduced social engagement has been associated with higher levels of loneliness and increased health risks, particularly when older adults lack strong familial ties or friendships (Cornwell & Waite, 2009; Litwin & Stoeckel, 2013). Also, social participation, such as involvement in community activities or volunteering, plays a protective role in mitigating loneliness and promoting better health outcomes (Fakoya et al., 2020).
Despite growing attention to vulnerabilities, further research is needed to understand how different vulnerabilities interconnect and form various patterns of multiple vulnerabilities. Such studies are essential to explore how these patterns relate to late-life loneliness, an area still underexplored in the current literature. Given that vulnerabilities among older adults are closely linked to policy dimensions such as income security and health insurance, it is imperative to investigate how different welfare regimes influence these vulnerabilities.
Welfare Regimes and Loneliness
Despite the discrepancy in empirical typologies, Esping Andersen’s three types of welfare capitalism (1999), Anglo-Saxon, social democratic, and continental welfare states have long been accepted in the literature. Nordic (social democratic) welfare states provide the most generous social welfare policy based on high reliance on the role of the government, resulting in the lowest level of poverty and inequality. In Anglo-Saxon welfare states, relatively limited government support is provided, and the role of the market in relation to government and family is highlighted. Continental welfare states also have lower poverty and inequality compared to Anglo-Saxon welfare states but provide insider-centered generous social programs that often exclude outsiders of the labor market, women or irregular workers, manifesting stratification (Esping-Andersen, 1999; Häusermann & Schwander, 2012). In addition to this original categorization centered around Western European countries, Southern European and East Asian welfare regimes have emerged as important welfare regimes. In the Southern European welfare regime, the role of family is more imminent than the state, and welfare provision is fragmented (Eikemo et al., 2008; Ferrera, 1996). East Asian welfare regimes, known as “productivist welfare states” (Holliday, 2000) offer their citizens relatively less generous social benefits and have a high level of familiarization as they have a high reliance on family in providing benefits.
Different types of welfare regimes have been significantly associated with economic, social, and political vulnerabilities in old age (Whelan & Maître, 2010). Research suggests that welfare states are linked to lower levels of poverty (Fouarge & Layte, 2005), particularly when supported by generous pension systems (Kuitto et al., 2023), and reduced social exclusion (Lee, 2021; Ogg, 2005). For instance, Ogg (2005) demonstrated that Nordic countries exhibit the lowest risk of social exclusion—measured through factors such as social relations, physical health, income, neighborhood cohesion, and social activities—among older adults. Conversely, Eastern and Southern European countries displayed higher levels of social exclusion. Lee (2021) also found that older adults in Nordic societies had better resources, social relations, and health outcomes compared to those in Central and Eastern Europe. However, public pension generosity is negatively associated with poverty rates in the United States, which continues to experience higher poverty rates among older adults (Kuitto et al., 2023). Similarly, Korea’s pension system is less effective in reducing elderly poverty compared to more universal models (Byun, 2024).
Welfare regimes influence not only individual vulnerabilities among older adults but also various well-being measures, including quality of life (Moor et al., 2013), life satisfaction (Lee, 2021), and health (Wallace et al., 2015). Older adults in Nordic nations generally reported higher levels of satisfaction and better health outcomes than their counterparts in other European regions (Lee, 2021). Furthermore, the effects of social vulnerability on mortality and disability were evident in Mediterranean and Continental countries but not in Nordic countries (Wallace et al., 2015). Van der Linden and Colleagues (2020) found that welfare regimes affect the impact of childhood conditions on late-life frailty; for example, economic difficulties during childhood were not significantly associated with higher odds of frailty in Southern and Eastern European welfare regimes. However, the relationship between family resources and life satisfaction does not appear to be moderated by welfare state arrangements (Moor et al., 2013). In both generous and less generous welfare states, family resources remain equally critical to the well-being of older adults.
Similarly, developed welfare states, such as the Nordic, and Continental regimes, are known for their effectiveness in preventing loneliness among older adults compared to Southern and Eastern European regimes (Fokkema et al., 2012; Nyqvist et al., 2019). Nordic welfare states, in particular, foster social integration through significant state involvement, which reduces the reliance on family and other social ties to combat loneliness (Nyqvist et al., 2019). Unlike other regimes, the Nordic model places less emphasis on social contacts, frequency of interactions, and the number of confidants (Nyqvist et al., 2019) and is less influenced by civic participation (Lee, 2021). In contrast, financial difficulties are strongly associated with high levels of loneliness among older adults in Southern and Eastern European countries (Fokkema et al., 2012). A recent study examining the association between higher income inequality and greater loneliness found that the United States reported the highest levels of loneliness compared to 16 European countries (Tapia-Muñoz, Staudinger, Allel, Steptoe, Miranda-Castillo, & Medina, 2024). Even within Nordic regimes, variations in the relationship between material vulnerability and loneliness exist. For instance, income concerns were significantly linked to loneliness in Sweden and Finland but not in Denmark and Norway (Dahlberg et al., 2022).
However, many of these studies provide limited insights into how different dimensions of vulnerability are interconnected and exacerbate overall risks. By focusing primarily on individual indicators of vulnerability, these studies fail to capture how resources across different domains interact to shape the quality of life in later years. A multidimensional perspective on vulnerability suggests that the patterns of vulnerability may vary significantly by welfare regime. For example, in states with high involvement in social welfare, generous pensions, and universal public services, older adults may experience lower levels of inequality and poverty, fostering greater social capital and participation. Additionally, there is a scarcity of research exploring the relationship between vulnerabilities and loneliness across different welfare regimes. Most studies have predominantly examined Western countries, with limited perspectives on regions such as East Asia, leaving a gap in understanding how these dynamics manifest in diverse contexts.
Present Study
This study explores two key research questions. First, it examines the patterns of multiple vulnerabilities among older adults across different welfare regimes, focusing on five representative countries: the U.S. (liberal), Korea (East Asian), Sweden (social democratic), Spain (Southern European), and Germany (continental European). The study hypothesizes that older adults in less generous welfare regimes, such as the liberal, East Asian, and Southern European models, are more likely to face higher levels of material vulnerability. Furthermore, it is hypothesized that interconnected vulnerabilities spanning multiple dimensions—material, health, and social—are more prevalent in Korea and Spain compared to Sweden, Germany, and the U.S.
Second, the study investigates the relationship between vulnerability patterns and loneliness across these countries. It identifies the prevalence of loneliness in each country and examines how different patterns of vulnerabilities are associated with loneliness. The study hypothesizes that vulnerabilities are positively associated with loneliness, but that the strength and nature of this association vary by welfare regime. Specifically, older adults in Nordic and continental European welfare regimes are expected to exhibit weaker associations between vulnerabilities and loneliness due to lower dependency on individual resources and stronger welfare support systems. Conversely, in liberal, East Asian, and Southern European welfare regimes, where welfare systems are less comprehensive, vulnerabilities are expected to have a stronger impact on loneliness among older adults.
Methods
Data Source
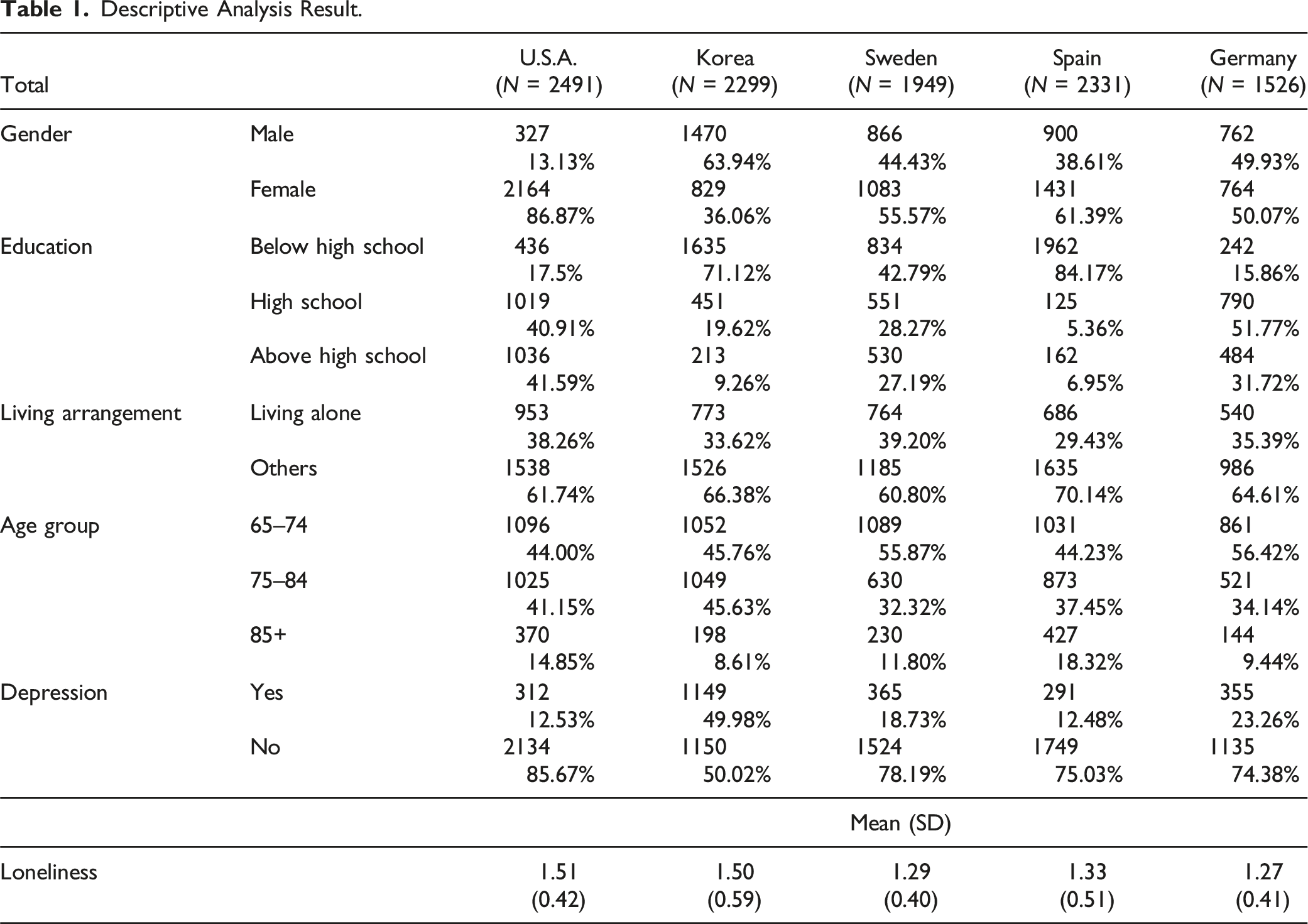
This study used three national data sets that were created to conduct international health and aging comparisons and analyses: the 2014 Health and Retirement Study (HRS) for the United States, the 2014 Korean Longitudinal Study of Ageing (KLoSA), and the 2015 Survey of Health, Ageing and Retirement in Europe (SHARE) for Sweden, Spain, and Germany. The 2014 and 2015 data were the most recent available data when we conducted the data analysis. HRS has been used as a model for other studies of countries, such as KloSA and SHARE which is also called the ‘HRS-family’ studies (Health and Retirement Study, n.d.). All three survey datasets are biannual longitudinal panel data of nationally representative samples of middle-aged and older individuals living in the community. These surveys have comparable variables of socioeconomic factors, family structure, and health conditions. We restricted our analysis sample to individuals aged 65 and older who were the heads of their households. The final sample comprised 10,596 participants from the following countries: the United States (n = 2491), Korea (n = 2299), Sweden (n = 1949), Spain (n = 2331), and Germany (n = 1526). For the final regression analysis, the sample sizes were: the United States (n = 2410), Korea (n = 2297), Sweden (n = 1850), Spain (n = 1946), and Germany (n = 1479). The percentages of missing data for each country were 3.3% for the United States, 0.1% for Korea, 5.1% for Sweden, 16.5% for Spain, and 3.1% for Germany. The age range of the sample was between 65 and 105 years.
Measures
Drawing from theoretical and empirical studies on multi-dimensional old age vulnerability and comparable variable availability of the three data, we used four vulnerability constructs using a total of nine binary indicators: material vulnerability (poverty, high out-of-pocket (OOP) expenditures for health care, unaffordability for housing), physical health vulnerability (ADLs, IADLs, multiple chronic conditions), and social vulnerability (having close children and friends, social participation).
Material Vulnerability
(1) Poverty: Poverty was defined if a family size-adjusted household’s disposable income was less than one-half of the median annual income following the OECD guideline (Balestra & Tonkin, 2018). (2) High OOP: High OOP was measured by assessing the out-of-pocket health expenditure to income ratio. If OOP expenditures exceeded 5% of household income for individuals with household incomes of less than 200% of the poverty line, which was half of the median annual income, it was defined as having a high OOP burden; for higher-income participants, the high OOP burden threshold was 10%. Out-of-pocket healthcare expenditures were computed based on respondents’ usage of non-covered healthcare services, such as hospitals, nursing homes, doctor visits, dental visits, outpatient surgery, monthly prescription drug costs, home health care, and special facility charges (Alley et al., 2009). (3) Housing unaffordability: Housing unaffordability was assessed if a housing cost (rent or mortgage) was 30% or more of monthly household income (Mason et al., 2013; Newman, 2003). For Korea data, housing unaffordability was assessed if a housing-related expenditure (rent, mortgage, maintenance fee) was 30% or more of monthly household income (Park et al., 2015).
Health Vulnerability
(1) Activities of Daily Living (ADLs) Limitations: Individuals were classified as having ADL difficulty (coded as 1 for yes and 0 for no) if they reported challenges with any basic self-care activities, such as dressing, walking across a room, bathing, eating, getting in or out of bed, or using the toilet. (2) Instrumental Activities of Daily Living (IADLs) Limitations: Individuals were classified as having IADL difficulty (coded as 1 for yes and 0 for no) if they experienced challenges with tasks requiring more complex functioning, such as preparing meals, shopping for groceries, managing medications, handling finances, making telephone calls, or using transportation. (3) Multiple Chronic Conditions (MCC) were used to define individuals who have two or more chronic health conditions that had ever been diagnosed by a doctor.
Social Vulnerability
(1) Having close children: Having close children was assessed with the number of close children in the social network. In Korea, having children meet at least once a week was coded as having close children since this question was the most similar questionnaire in other countries. (2) Having close friends: Having close friends was assessed with the number of close friends in the social network. In Korea, having a friend meet at least once a week was coded as having a close friend. (3) Social participation: Social participation was assessed by asking if participants were involved in social activities, including volunteer activities, education, sports/social clubs, and political community. The measures were coded as not being involved in any of the activities or being involved in any activity.
Loneliness
In HRS, loneliness was assessed using the updated UCLA Loneliness Scale, which included 11 questions (Russell, 1996). We created a summary score ranging from 1 to 3. (Smith et al., 2013). In SHARE, loneliness was assessed using the revised UCLA included three questions from 1 to 3 (Hughes et al., 2004). In Korea, loneliness was asked with a question ranging from 1 to 3. We revised the code in all variables, and a higher value indicates a higher sense of loneliness. Previous research has found that these measurements of older adult loneliness were reliable and consistent to compare (Newmyer et al., 2021).
Covariates
Gender was coded male or female (0/1). Age cohorts were coded into three groups: 65-74, 75-84, and aged 85 years and above. Education was coded into three groups: Less than high school, high school, college, and above. The living alone variable was coded as others and living alone (0/1).
Statistical Analyses
For Research Question 1, which identifies different levels and patterns of multiple vulnerability among older adults, we used Latent Class Analysis (LCA) in each of five countries to identify types of multi-dimensional old age vulnerability. LCA empirically categorizes individuals into groups where the individuals within a group are similar to one another and different from individuals in other groups (McCutcheon, 2002). We used three model fit statistics to determine the ideal number of classes: the Lo–Mendell–Rubin (LMR) test, the Bayesian information criterion (BIC), and entropy. Bivariate analyses were then conducted between socio-demographic variables and the identified vulnerability types.
To answer Research Question 2, which examines to what extent types of vulnerability are associated with loneliness in each country, we conducted ordinary least squares (OLS) regression analyses with individual national data.
Results
Descriptive Statistics
Descriptive Analysis Result.
Types of Multi-Dimensional Vulnerability
Based on fit statistics (AIC, BIC, p-value of LMR, and entropy) and the proportions of different numbers of class models, we defined five country-specific models (Figure 1, Appendix Table 1). Class Profiles of Multi-Dimensional Vulnerability Types. *Abbreviations note: MCC-Multiple Chronic Conditions.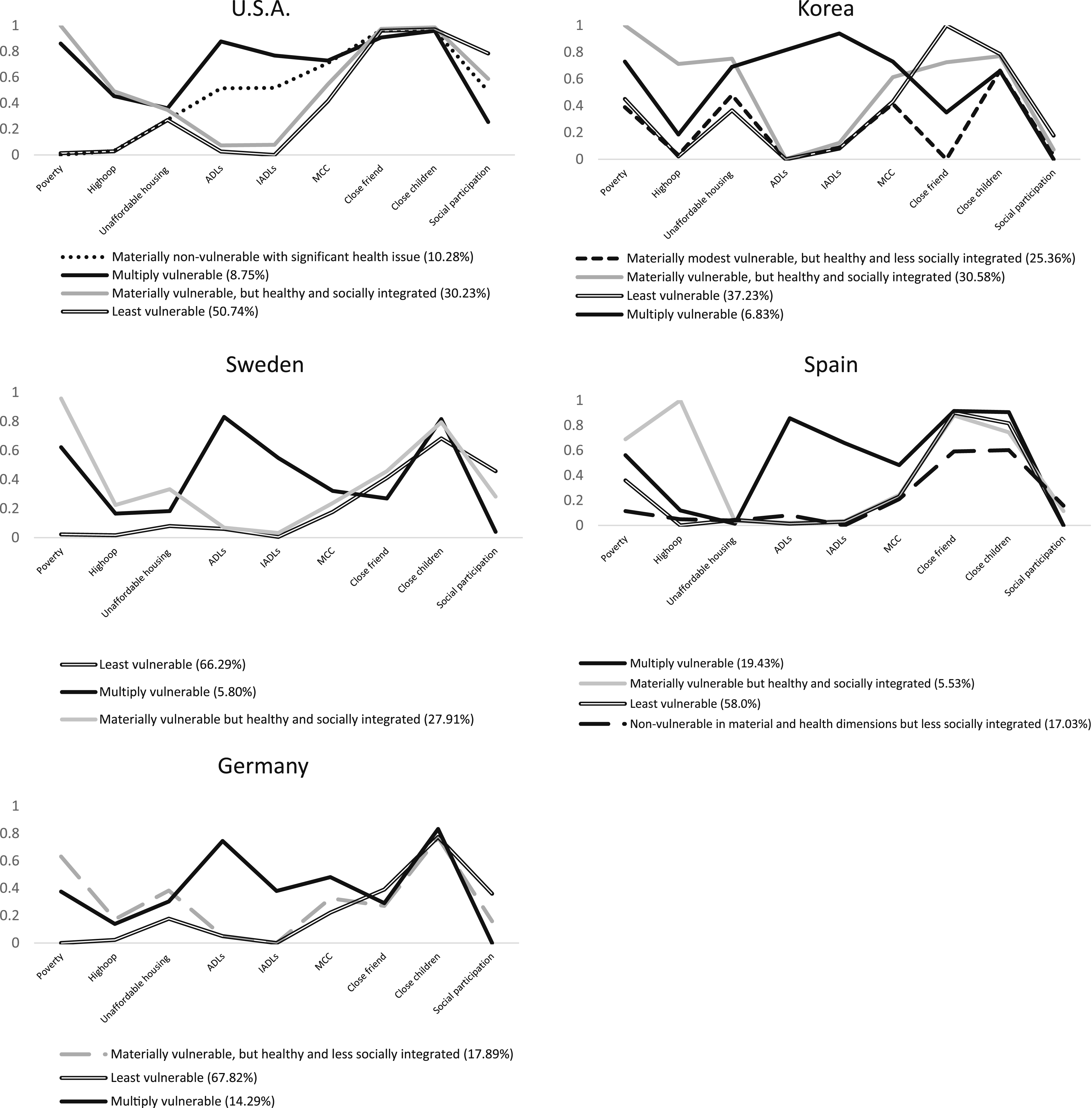
In the United States, four vulnerability patterns were identified: materially non-vulnerable with significant health issues (10.28%), facing moderate ADL/IADL difficulties and chronic conditions; multiply vulnerable (8.75%), experiencing poverty, ADL risks, and limited social engagement but strong child and friend support; materially vulnerable but healthy and socially integrated (30.23%), dealing with poverty and housing challenges without severe health or social issues; and the least vulnerable (50.74%), with low risks and high social participation.
In Korea, four types were observed: materially modest vulnerable but healthy and less socially integrated (25.36%), with modest poverty and limited social ties beyond child support; materially vulnerable but healthy and socially integrated (30.58%), with high material risks but strong support from children and friends; least vulnerable (37.23%), reporting low risks but slightly higher material challenges than non-vulnerable groups in other countries; and multiply vulnerable (6.83%), with high poverty, ADL/IADL risks, and reliance on child support.
In Sweden, three classes emerged: least vulnerable (66.29%), with low risks and strong child support; multiply vulnerable (5.80%), facing poverty, ADL challenges, limited social ties, and low social participation; and materially vulnerable but healthy and socially integrated (27.91%), with higher poverty but better support from friends and children.
In Spain, four types were identified: multiply vulnerable (19.43%), facing poverty, ADL/IADL risks, and strong social integration; materially vulnerable but healthy and socially integrated (5.53%), with high healthcare costs but robust support from family and friends; least vulnerable (58.0%), with low risks and strong social ties; and non-vulnerable in material and health dimensions but less socially integrated (17.03%), with low risks but limited social networks.
In Germany, three types were identified: materially vulnerable but healthy and less socially integrated (17.89%), with high poverty and strong child but limited friend support; least vulnerable (67.82%), with low risks and high social participation; and multiply vulnerable (14.29%), with moderate material vulnerabilities, significant health risks, and low social engagement.
In each country, two common groups emerged: the least vulnerable group and the multiply vulnerable group. Sweden and Germany stand out with the highest proportions of least vulnerable individuals (66.29% and 67.82%, respectively), demonstrating the strength of their comprehensive welfare systems in ensuring material, health, and social security. In contrast, Korea (37.23%) and Spain (58%) have lower proportions in this category, highlighting the limitations of productivist East Asian and family-centered Southern European welfare models. The USA, while maintaining a sizable least vulnerable group (50.74%), shows a high proportion of materially vulnerable with significant health issue (30.23%), reflecting material challenges despite relatively low functional impairments.
Multiply vulnerable groups are most prominent in Spain (19.43%) and Germany (14.29%), indicating overlapping vulnerabilities in these welfare contexts. This points to weaker public welfare systems in Spain that rely heavily on family networks, leading to significant vulnerabilities across dimensions. In Germany, while the proportion of the most well-off, least vulnerable group is high, it also has high level of the disadvantaged group, multiply vulnerable. Conversely, Sweden has the lowest proportion of multiply vulnerable individuals (5.80%), underscoring the role of its universal welfare model in mitigating multi-dimensional risks. This supports our hypothesis that less generous welfare systems may struggle to alleviate material and multiple vulnerability.
Unique country-specific patterns further enrich the analysis. Korea has a significant Materially modest vulnerable but healthy and less socially integrated group (25.36%), reflecting the reliance on family-centered support systems, as they present high level of children supports. This family-centered support can reduce material vulnerability but often fail to foster broader social integration. Similarly, Spain exhibits a notable Non-vulnerable in material and health dimensions but less socially integrated group (17.03%), highlighting social isolation as a persistent issue despite material and health security. Social vulnerability was more prevalent in countries with less generous welfare regimes, including those following East Asian and Southern European models. This finding confirms the hypothesis that limited welfare provisions are insufficient to mitigate social vulnerabilities. In Germany, a distinct Materially vulnerable but healthy and less socially integrated group (17.89%) points to material and social challenges that remain despite strong health support.
Social Demographic Characteristics Across the Vulnerability Types
Across countries, distinct sociodemographic patterns emerge within different vulnerability groups, highlighting shared factors that contribute to risk (Appendix Table 2). The Multiply vulnerable group consistently exhibits the highest levels of vulnerability, with a majority being 75+ older adults such as 43.36% in Sweden and 50.96% in Korea, predominantly female (e.g., 61.95% in Sweden and 88.99% in the USA), with low educational attainment, and significant loneliness. This is often compounded by a large proportion living alone, such as 66.37% in Sweden and 54.59% in Germany. The Conversely, the Least vulnerable group demonstrates a younger age profile (65-74), with 65.94% in Sweden and 52.77% in the USA, higher educational levels, strong social connections, and the lowest rates of loneliness. Materially vulnerable but healthy and socially integrated group shows moderate vulnerability, characterized by lower education but better social and health profiles, and with more individuals living with others compared to the multiply vulnerable.
Regression Analysis
Regression Analysis Results (Ref: Least vulnerable).
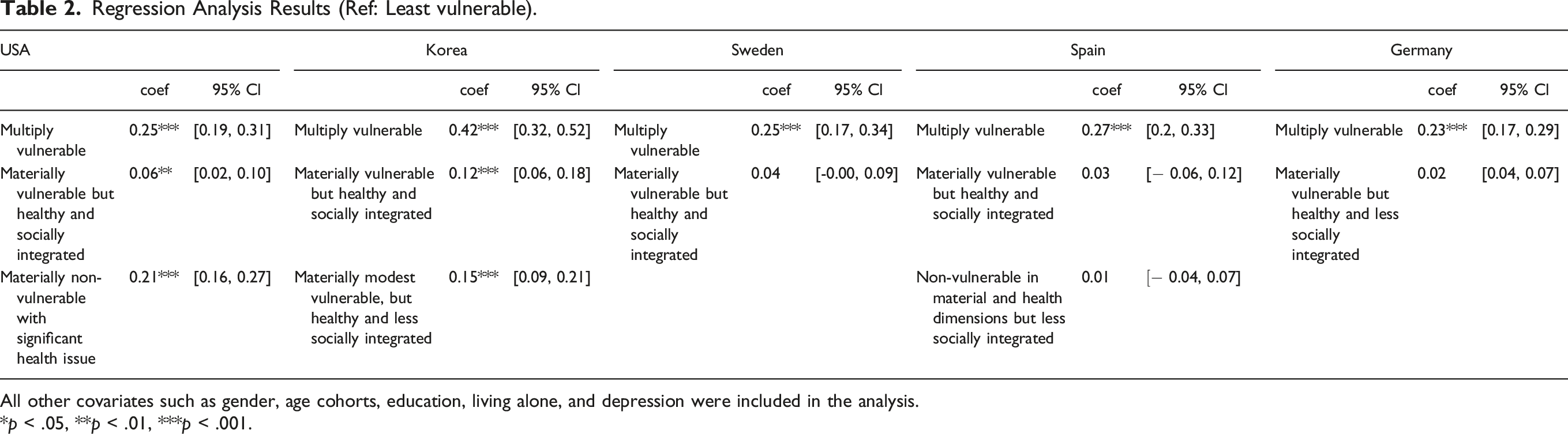
All other covariates such as gender, age cohorts, education, living alone, and depression were included in the analysis.
*p < .05, **p < .01, ***p < .001.
Discussion
Multidimensional approach to vulnerability provides insights on older adult’s life experiences with a holistic view in various life domains. The typology of welfare regimes is an important tool in understanding the complex processes and distribution of resources. This study explores how material, physical health and social vulnerability interact and combine with others across different welfare regimes. In addition, different domains of vulnerability, such as material or social (Diener & Fujita, 1995), and health (Högberg et al., 2018), are conditioned by the institutional contexts of welfare regimes. This study has revealed cross-national variations in vulnerability and how institutional arrangements attenuate or strengthen the association between vulnerability and loneliness.
Welfare regimes significantly influence patterns of vulnerability among older adults. Our findings confirm the hypothesis that less generous welfare systems struggle to alleviate material and multidimensional vulnerabilities, underscoring the crucial role of welfare regimes in redistributing resources. The cumulative effects of social provisions on inequality often become more pronounced in old age. Countries with comprehensive welfare systems, such as Sweden (66.29%) and Germany (67.82%), excel in reducing vulnerabilities across all dimensions, resulting in the largest proportions of least vulnerable individuals. In contrast, Korea (37.23%) has the lowest proportion of least vulnerable individuals, reflecting the limitations of its family-centered welfare model. Spain, meanwhile, has the highest proportion of individuals experiencing overlapping vulnerabilities (19.43%), followed by Germany (14.29%). Sweden has the lowest proportion of multidimensional vulnerabilities (5.8%), demonstrating the effectiveness of its universal welfare policies in addressing such challenges. These findings support the hypothesis that older adults in less generous welfare regimes are more likely to experience higher levels of material vulnerability.
Korea’s welfare system, characterized by modest support, reveals significant material hardships among older adults, with 6.83% identified as multiply vulnerable and 30.58% as materially vulnerable but socially integrated. Including those categorized as modestly materially vulnerable and less socially integrated (25.36%), over 62% of Korea’s older adults face material hardships. Even Korea’s least vulnerable group shows greater vulnerability compared to similar groups in other countries, with a high likelihood of experiencing poverty. This reflects Korea’s old-age poverty rate of 40.4%, the highest among OECD countries, which is over twice that of the USA (22.8%) and more than three times higher than Germany (11.0%) and Sweden (11.1%) (OECD, 2023). This high poverty rate stems from rapid changes in family structures and an underdeveloped social security system requiring more than 20 years of contributions to qualify for pension benefits—a threshold many older adults fail to meet.
In the USA, the welfare system highlights the interplay of material and health vulnerabilities, reflecting significant gaps in public safety nets and heavy reliance on private market solutions. Even materially secure groups often experience health vulnerabilities, illustrating limitations in healthcare access and affordability. These patterns emphasize the critical role of welfare policies in shaping vulnerability profiles across countries and the necessity of robust systems to mitigate material and health risks in later life.
In addition, the comparison of social dimensions across countries reveals notable patterns shaped by their welfare regimes. Limited welfare provisions are insufficient to mitigate social vulnerabilities and older adults in generous welfare states are more likely to be associated with lower social vulnerabilities. Social vulnerability was more prevalent in countries with less generous welfare regimes, including those following East Asian and Southern European models. Sweden stands out with the highest levels of friendships and social participation, reflecting the inclusiveness of its social democratic welfare system. Germany shows a more balanced approach with moderate levels across all social dimensions, though less pronounced than Sweden. The USA also shows strong personal relationships with friends and children but falls behind in fostering broader community engagement. In contrast, Korea and Spain rely heavily on family networks, particularly strong relationships with children, but exhibit significant gaps in social participation, indicating the limitations of their family-centered welfare models. These findings emphasize the role of welfare systems in shaping social connections. Social democratic regimes like Sweden foster both personal and community-based relationships, while family-centered systems like Korea and Spain prioritize familial ties at the expense of broader social integration.
Regardless of welfare regimes, vulnerable groups are more susceptible to experiencing loneliness. The multiply vulnerable group has higher loneliness level relative to the least vulnerable group in all countries. A multidimensional approach has identified this group as the most urgent and at-risk population. However, the findings do not support the hypothesis that the impact of material and social vulnerabilities on loneliness is lessened in generous welfare regimes. While welfare regimes influence the levels and types of vulnerabilities, the strong and consistent association between vulnerabilities and loneliness across different systems suggests that vulnerabilities remain a key driver of loneliness regardless of welfare support. This underscores the pervasive impact of vulnerabilities on well-being, highlighting the need for comprehensive policies to address multidimensional risks and reduce loneliness among older adults.
The United States and Korea present a unique case where all vulnerability types—multiply vulnerable, materially vulnerable but healthy and socially integrated, and materially non-vulnerable with significant health issues (only in the U.S.) and Materially modest vulnerable, but healthy and less socially integrated (only in Korea) —are associated with higher levels of loneliness compared to the least vulnerable group. This pattern is not observed in other countries. In particular, in the U.S., materially non-vulnerable individuals with significant health issues experience loneliness levels comparable to those of the multiply vulnerable group. This highlights the critical role of health issues in contributing to loneliness within the U.S. context. Material vulnerability but healthy and socially integrated is also significantly associated with higher loneliness, although its impact is smaller compared to that of materially non-vulnerable individuals with significant health issues. These findings suggest that while material vulnerability remains an important factor in limited welfare states like the U.S., health issues play a more pronounced role in exacerbating loneliness. On the contrary, in Korea, materially modest vulnerable, but healthy and less socially integrated is more strongly associated with loneliness than materially vulnerable but healthy and socially integrated, suggesting that social vulnerability is a crucial factor. These underscore the need for comprehensive welfare policies that address material, health and social-related vulnerabilities to mitigate loneliness effectively.
Spain emerged as an interesting case its levels of vulnerability and loneliness align more closely with those observed in other European countries rather than being more similar to liberal or East Asian countries. Even though Spain has the large proportion of multiply vulnerable compared to other countries, their loneliness level is lower than those in USA and Korea, slightly higher than Sweden and Germany. This goes against our initial hypothesis that vulnerability and loneliness in Spain would be similar to that in the USA and Korea, where older adults tend to experience higher levels of loneliness. Contrarily, Sweden, Germany, and Spain have lower levels of loneliness. This can be speculated in two ways. First, in Spain, familial interdependence and support are highly valued compared to Northern Europe, where independence-related values are more common (Fernández–Ballesteros, 2002; Rodrigues et al., 2014). Their family-centered approach might produce balanced and beneficial outcomes to older adults. Secondly, this could be because including Korea and the USA, which have less generous and liberal welfare systems, might have blurred the differences among European welfare regimes. Therefore, it’s possible that welfare regime theories alone may not be enough to understand loneliness and vulnerability, and culture may also play a role. Country differences may not be fully explained by welfare regimes, but rather other factors such as culture. The meaning of loneliness may also be complex and culturally grounded. People’s resource requirements to feel satisfied are subjective and likely to vary by culture and country (Barreto et al., 2021).
The vulnerability types identified in our study may be influenced by differences in welfare state configurations and cultural norms. Although the welfare typologies we used helped us understand representative cases of welfare states, we may have overlooked variations within a welfare regime. We used latent class analysis in our study to identify different patterns of vulnerability, including those experienced by multiply vulnerable groups. However, this method has limitations in determining the individual impact of each vulnerability indicator, as each indicator does not have the same influence on forming patterns of vulnerabilities. The clusters identified in our study were mainly based on material and social vulnerabilities, but not physical health. This could be problematic if indicators that influence forming clusters do not have much impact on loneliness or vice versa. For example, we could not examine the role of health on loneliness in our analysis of the association between vulnerability clusters and loneliness. While this study focuses on identifying associations between vulnerabilities and loneliness, it does not establish causal relationships or address potential endogeneity issues. Future research could utilize longitudinal datasets to examine how vulnerabilities evolve over time and influence loneliness, while accounting for institutional contexts and addressing causality.
Despite these limitations, our study highlights the cross-national variations in vulnerabilities faced by older adults and the most vulnerable groups who experience multiple vulnerabilities and suffer the highest level of loneliness. We have also expanded our understanding of the association between vulnerabilities and loneliness in East Asian countries, which have been overlooked in the welfare regime literature.
Supplemental Material
Supplemental Material - Material, Health, and Social Vulnerability and Loneliness Among Older Adults: From the Welfare Regime Perspective
Supplemental Material for Material, Health, and Social Vulnerability and Loneliness Among Older Adults: From the Welfare Regime Perspective by Ji Young Kang, Oejin Shin, Sojung Park, Jihye Baek, and Minyoung Kwak in Research on Aging
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Chungnam National University.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.