
Abstract
Family caregivers are essential to the healthcare system, yet many experience significant financial strain. Although financial strain is associated with worse caregiver mental health and well-being, the mechanisms underlying this association remain unclear. This study examines how financial strain relates to caregiver health outcomes within the caregiving stress process and assesses whether psychological resources—sense of purpose and perceived choice in caregiving—mediate these relationships. Using data from N = 1,223 family caregivers from the Caregiving in the U.S. 2020 dataset, hierarchical regression models examined the associations among care-related stressors, financial strain, and the outcomes of physical strain, emotional stress, and caregiving-related health impacts. Subjective financial strain significantly predicted greater physical strain, emotional stress, and negative health impacts. Perceived choice in caregiving was a partial mediator across all three outcomes. Findings underscore the importance of reducing subjective financial strain and strengthening coping resources to mitigate care-related stress.
Family caregivers are a critical pillar of the health and long-term services and supports (LTSS) systems in the United States (U.S.). Approximately 59 million caregivers provide unpaid assistance to adults with varying health, mobility, or cognitive impairments—about 41.8 million of whom care for someone over 50-years-old (AARP & NAC, 2020; AARP & NAC, 2025). Consistent with well-established research and policy literature, a family caregiver is defined as “any relative, partner, friend, or neighbor who has a significant personal relationship with, and who provides a broad range of assistance for, an older person or an adult with a chronic, disabling, or serious health condition” (Reinhard et al., 2023, p. 2). Although there are considerable differences in the terminology recommended to define these unpaid caregivers (e.g., Stall et al., 2020), which include family, friends, and/or neighbors, they will be referred to as ‘family’ caregivers in this paper to be consistent with previous literature. In the U.S., family or ‘informal’ caregivers of adults spend roughly 20 hours per week on care-related tasks – providing approximately 36 billion hours of unpaid care annually, which represents an effort valued at over $600,000,000 (Gruber & McGarry, 2023; Reinhard et al., 2023). This unpaid ‘workforce’ provides wide-ranging assistance with tasks including care coordination, financial management, and medical and nursing tasks—support which accounts for over one-third of the nearly 2% of the U.S. GDP spent on long-term care (Gruber & McGarry, 2023). This magnitude of spending is in line with, and in some cases exceeds, major federal budget functions (for example, international affairs represents roughly 1% of total federal spending), thus underscoring the scale of resources involved in providing assistance to this growing proportion of the population (U.S. Department of Treasury, 2025).
Among their multidimensional responsibilities, roughly 92% of family caregivers for adults provide financial assistance, defined as managing or contributing to their care-recipient’s finances (Lynch & Wave, 2017). In terms of monetary costs, family caregivers who assist an adult with chronic illness spend roughly $6,663 on care-related expenses, with costs increasing to about $8,978 for dementia caregivers (AARP & NAC, 2025). These figures likely underestimate the true financial burden of care, as many expenses (e.g., home modifications, transportation, medical equipment) are not covered by insurance. Recent data show that nearly one in five family caregivers struggle with paying bills, while 14% cannot afford basic necessities such as housing and food (AARP & NAC, 2025). Pragmatically, one study of caregivers assisting care-recipients aged 60+ reported that caregiving compromised short- and long-term savings and the ability to meet both their own and their care-recipients’ needs (Moody et al., 2022). The experiences and impacts of these stressors may be further intensified in the context of dementia, as care demands escalate with advancing impairment (Alzheimer’s Association, 2025), thus representing an important contextual characteristic of the caregiving environment. Irrespective of diagnosis, however, decades of research has consistently documented the economic, physical, and psychosocial consequences of care-related stress and its downstream impact on families, communities, and the broader healthcare system (e.g., Broxson & Feliciano, 2020; Burchardt, 2025).
Correlates of Financial Strain
Financial strain is defined as a state of psychological stress characterized by anxiety, worry, or inadequate coping created by financial or economic circumstances (Lazarus, 1966) and is “synonymous with ‘financial economic hardship,’ ‘financial/economic stress’ or ‘financial difficulties’ or ‘inability to cope financially’” (French & Vigne, 2019, p. 2). Among caregivers of older adults aged 65+, financial strain is linked to poorer mental health, greater emotional stress and depressive symptoms, lower quality of life, more frequent healthcare utilization, and even increases in inflammatory biomarkers (e.g., Hellis & Mukaetova-Ladinska, 2022; Liu et al., 2024; Samuel et al., 2022). More recent work comparing age groups found that younger caregivers face higher risks of depression and anxiety due to greater work-related role conflicts (Fenton et al., 2022; Hellis & Mukaetova-Ladinska, 2022; Koumoutzis et al., 2021). Research also has demonstrated worse mental health outcomes among dementia family caregivers compared to caregivers of other chronic conditions (e.g., cancer) aged 65+ (Karg et al., 2018). However, it is also important to note that the adverse implications of caregiving are the result of a broader combination of factors beyond just patient diagnosis or patient age. For example, research also has documented variation in financial strain by race (Willert & Minnotte, 2021), gender (Liu et al., 2022), and relationship type (e.g., spouses vs. adult children; Kang, 2021; Lee & Zurlo, 2014; Lei, 2023). Although these descriptive patterns highlight who is at risk, they offer less clarity about the mechanisms through which financial strain shapes health and well-being. In line with this perspective, the current study treats care recipient diagnosis (including dementia), caregiver sociodemographic characteristics, and caregiving context as background factors that influence financial strain, rather than as primary stratifiers or moderators of the financial strain–health relationship.
Dimensions of Financial Strain
Prior work identifies financial strain as a key dimension of care-related stress and burden, however the pathways by which specific aspects of strain impact outcomes remain unclear. Existing research is further limited by the differential conceptualization of financial strain across studies. The material-psychosocial-behavioral model of financial hardship (Tucker-Seeley & Thorpe Jr., 2019) informs how the multidimensional nature of financial strain is operationalized—with individual factors such as debt, social resources, and contextual factors (e.g., socioeconomic status) shaping the broader construct of financial hardship (Mage et al., 2024). Notably, the concept of financial strain encompasses both objective economic conditions and subjective perceptions of financial stress. Objective indicators like income or out-of-pocket spending do not necessarily correspond with subjective indicators such as perceived worry about finances. Additionally, subjective financial strain often shows stronger associations with mental health outcomes (Bridges & Disney, 2010; Drentea, 2000; Hamilton et al., 2019; Prawitz et al., 2006). Because objective and subjective indicators capture different aspects of financial hardship, both are needed to understand how caregivers interpret and respond to different dimensions of financial strain (Weissman et al., 2020).
Stress Process Model
Pearlin et al.’s (1990) stress process model offers a theoretical framework for understanding how care-related stressors influence health and well-being. Within this framework, caregiver outcomes reflect not only objective caregiving demands, but also how stressors are perceived and managed over time. The model distinguishes background/context characteristics, primary stressors, and secondary stressors, positing that differential physical and psychosocial outcomes result from the dynamic interplay of these various stress domains. Primary stressors arise from direct care provision and encompass both objective (e.g., level of functional impairment) and subjective (e.g., role overload) indicators of stress. These stressors often spill over into secondary stressors, creating interference between caregiving and other life domains, such as work or family conflict.
The model also highlights the role of mediators, including coping mechanisms and social support, that influence how stressors are appraised, which can subsequently impact caregiving outcomes. Indeed, using data from the Canadian Community Health Survey—Healthy Aging (N = 5,067), Lee and Zurlo (2014) found social support to alleviate financial strain in caregivers of community-dwelling adults. Less explored in the literature, however, is how internal coping resources influence the appraisal of and outcomes associated with financial strain. Psychological resources, such as having a sense of purpose in life and mastery, may foster resilience and enhance positive appraisals of the caregiving role (Drentea & Reynolds, 2015; Fan & Ryu, 2023; Frankham et al., 2020; Polenick et al., 2019), thus leading to more positive outcomes.
Perceived choice in taking on the caregiving role reflects mastery, defined as the belief that one has control over life circumstances (Pearlin & Schooler, 1978). Caregivers with high mastery who perceive having a choice in the caregiving role may differentially appraise or focus on aspects of their financial situation that are amenable to change—approaching financial difficulties with greater problem-focused coping, confidence, and flexibility (Folkman, 1984). Research also has shown that caregivers who feel they had little choice in assuming the role may be especially vulnerable to negative appraisals and poorer outcomes (Schulz et al., 2012). Thus, perceived choice may weaken the link between financial strain and emotional or physical distress by supporting a more adaptive interpretation of financial challenges.
Purpose or meaning in life serves a related, but distinct role. Economic hardship has been shown to undermine key resources and beliefs (e.g., diminished sense of meaning and control), leading to feelings of insecurity, uncertainty, and hopelessness about the future (Drentea, 2000). Conversely, caregivers who perceive a sense of purpose may interpret financial pressures within a broader framework of caregiving-related values or commitment (i.e., familism), which can promote resilience and reduce the impact of stress on health (Drentea & Reynolds, 2015; Fan & Ryu, 2023; Frankham et al., 2020; Polenick et al., 2019). These mechanisms align with the stress process model, which holds that psychological resources shape both the appraisal and outcomes of stress. Given the dynamic interplay of individual, psychosocial, and contextual factors in shaping the experiences and outcomes associated with caregiving, the stress process model provides a useful theoretical framework for examining objective and subjective indicators of financial strain while accounting for caregiving and broader contextual characteristics. Moreover, evaluating positive psychological resources, such as perceived choice in caregiving and perceived sense of purpose/meaning in life will allow for the examination of how psychological processes operate and are influenced by the unique dimension of financial stress within the context of caregiving.
Current Study
As the need for family caregivers continues to grow, it is important to clarify how different forms of financial strain operate within the caregiving stress process. The present study utilizes a modified version of the stress process model (Pearlin et al., 1990) to examine financial strain as a central secondary stressor within the caregiving role. Specifically, financial strain is conceptualized as a multidimensional construct that includes both objective financial impacts and subjective financial strain. These dimensions capture distinct pathways through which financial stress may influence caregiver health and well-being. In addition, we extend the model by examining psychological resources—perceived choice in the caregiving role and sense of purpose or meaning in life—as coping-related mediators that may attenuate the impact of financial strain on physical strain, emotional stress, and caregiving-related health impacts (Figure 1). Caregiver and care-recipient characteristics, including care-recipient diagnosis of Alzheimer’s disease or related dementias (ADRD), are treated as background contextual factors that shape caregiving demands and exposure to stressors rather than as focal analytic stratifiers. We hypothesized that financial strain would be associated with adverse outcomes, specifically greater physical strain, higher emotional stress, and more negative caregiving-related health impacts. Perceived choice and purpose/meaning—two coping-related psychological resources—were examined as mediators of these associations. Conceptual framework with study variables (adapted from Pearlin et al., 1990).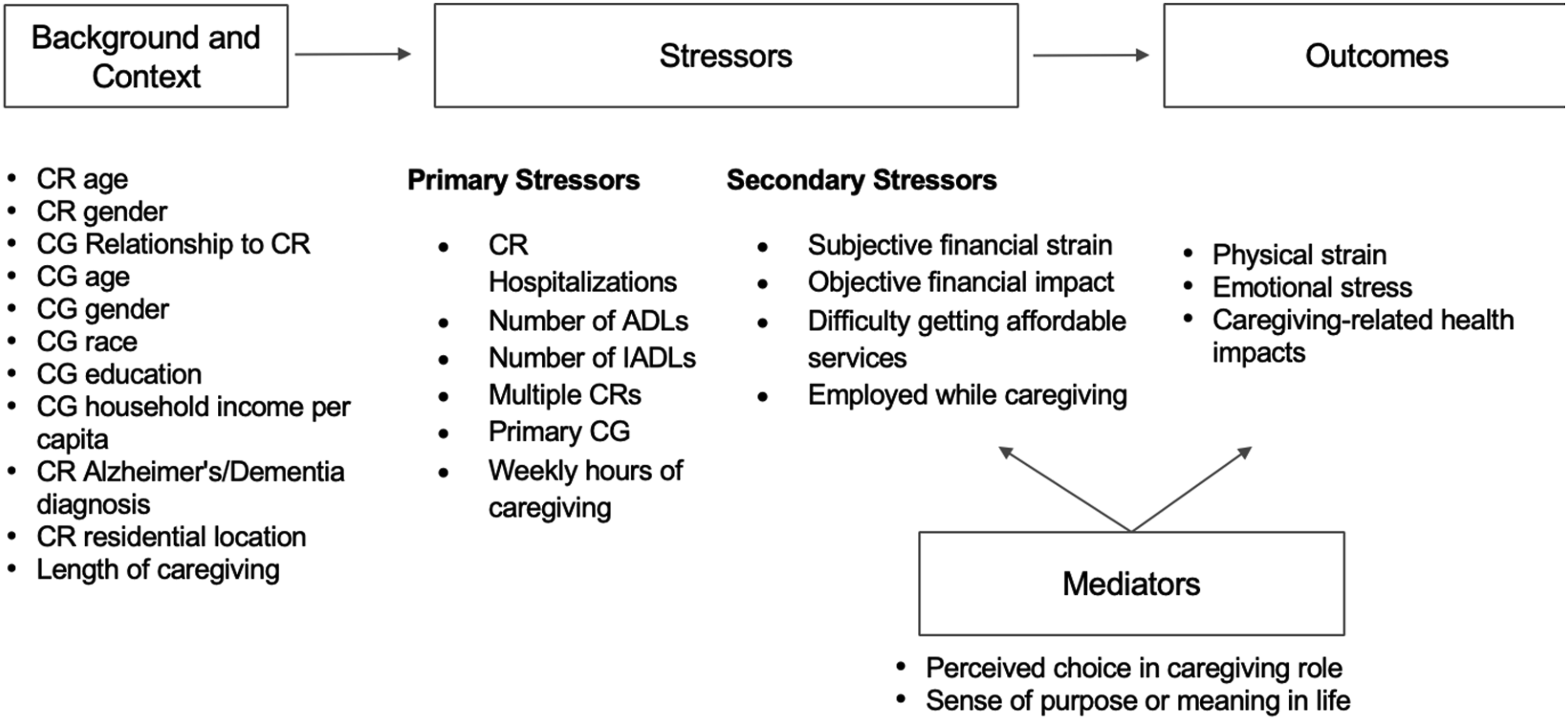
Methods
Data and Sample
We analyzed publicly available, nationally representative data from the “Caregiving in the U.S. 2020” study conducted by the National Alliance for Caregiving (NAC) and American Association of Retired Persons (AARP) (AARP & NAC, 2020). The study employed a rigorous design to ensure accurate data collection and proper validation of caregiver status. Data collection took place in 2019 and was published in 2020, with surveys administered online via Ipsos’ KnowledgePanel®, which is a probability-based sample representative of the U.S. population. This survey included unpaid caregivers of both children and adults and was conducted in both Spanish and English. A total of 1,739 respondents completed the survey. The comprehensive survey methodology is detailed elsewhere (AARP & NAC, 2020). For the purposes of this study, we focused on respondents who self-identified as providing care to an older adult aged 50+ within the past 12 months, resulting in an initial sample of 1,425. We then excluded participants with missing data for key variables (N = 202), yielding a final analytic sample size of 1,223.
Measures
Independent Variables
Guided by our conceptual model (see Figure 1), we included variables on caregiver/care-recipient characteristics and context, potential stressors related to caregiving activities (including financial stress/strain), and mediating variables.
Background and Context Variables
Care-recipients’ demographic characteristics (e.g., age and gender) and relationships to their caregivers, categorized as spouse/partner, parent, or other extended relationships were included. We also included caregivers’ demographic characteristics including age, gender, race/ethnicity, education, household income per capita (calculated as total household income divided by number of household members). Caregiving characteristics including the care recipient’s residential status (e.g., with caregiver, in the care-recipient’s own or someone else’s home, in long-term care, or other), length of caregiving (ranging from < 6 months to over 10 years), and ADRD diagnosis were included as indicators of caregiving history and context. ADRD status was treated as a background/contextual characteristic to capture caregiving demands and complexity, and was examined as a covariate in multivariable models.
Stressors
Assessment of primary stressors included variables related to the care recipient’s level of need for support. Specifically, we included the number of overnight hospitalizations (ranging from 0 to 3+ times) experienced by the care recipient in the last 12 months as an objective, clinically significant event often used in health services research as a proxy for healthcare utilization and care-related support needs (Andersen, 1995; Hurd et al., 2013). Additionally, caring for more than one care-recipient, serving as primary caregiver, and weekly hours of caregiving were included. Number of activities of daily living (ADLs, 6-items: transferring, dressing, toileting, bathing/showering, feeding, dealing with incontinence) and instrumental activities of daily living (IADLs, 7-items: transportation, grocery/other shopping, housework, meal preparation, financial management, medication administration, arranging outside services) the care-recipient required assistance with was included as an indicator of functional dependency.
In terms of secondary stressors, two measures of financial strain/stress were included as the main variables of interest. Caregivers were administered a single item to assess subjective perceptions of financial strain, with response options ranging from 1 (not at all) to 5 (very much). The second variable represents objective financial impacts. Participants were asked whether they had experienced 13 caregiving-related financial impacts across five domains: savings, debt, bills, work, and home arrangements, with binary response options (Yes/No). Total scores were calculated as the sum of yes/no responses across these 5 domains, ranging from 0 to 5. Cronbach’s alpha for the current study is α = .76, indicating acceptable internal consistency.
Additional variables related to caregiver burden included caregiver’s employment status in the past year while providing care (as an indicator of secondary role strain) and difficulty getting affordable care, with response options ranging from 1 (not at all difficult) to 5 (very difficult).
Dependent Variables
We included three key variables related to caregiving health and well-being.
Physical Strain
Caregivers were asked a single-item: “How much of a physical strain would you say that caring for your care recipient is/was for you?” Response options ranged from 1 (no strain at all) to 5 (high strain).
Emotional Stress
Caregivers were asked a single-item question: “How emotionally stressful would you say that caring for your care recipient is/was for you?” Response options ranged from 1 (not at all stressful) to 5 (very stressful).
Caregiving-Related Health Impacts
Caregivers were asked a single-item question: “How would you say taking care of your care-recipient affected your health?” Response options included: “(1) Made it worse”, “(2) Did not affect it”, and “(3) Made it better.” Due to the small frequency of participants (n = 50) selecting the “Made it better” option, the “Did not affect it” and “Made it better” responses were collapsed into a single category. We then created a dichotomous variable where 1 indicated that caregiving negatively impacted health (“Made it worse”) while 0 indicated no perceived negative impact.
Mediators
We incorporated two measures as mediators that evaluated (1) perceived choice in taking on the caregiving role (yes/no) and (2) the extent to which the caregiving role provided caregivers with a sense of purpose or meaning in life. Sense of purpose was measured with one item (“My role as a caregiver gives/gave me a sense of purpose or meaning in my life”) with response options including a 5-point Likert Scale ranging from 1 (strongly disagree) to 5 (strongly agree). Those who responded 1–3 were recoded as 0 (no/low sense of purpose), and those responding a ‘4’ or ‘5’ were coded as 1. These variables served as indicators of coping as guided by our conceptual model.
Data Analysis Plan
We conducted a one-way analysis of variance (ANOVA) for continuous variables and chi-square tests for categorical variables to compare all demographic, caregiving-related, and outcome variables (physical strain, emotional stress, and health impacts). Next, we conducted ordered logistic regression models to identify potential factors associated with physical strain and emotional stress, and binary logistic regression models to assess their associations with caregiving-related health impacts. Following our conceptual model, we constructed hierarchical analytical models with odds ratios. The first step included background and contextual variables (e.g. care-recipients’ and caregivers’ demographic characters) as the base model. Next, we added caregiving-related stressors, including subjective financial strain and objective financial impacts. Finally, we incorporated our mediators of perceived choice in the caregiving role and sense of purpose from caregiving. To note, subjective and objective financial strain were included simultaneously at each additional step of the analysis. While these two variables are moderately correlated (r = 0.499), post-regression diagnostic tests indicate that multicollinearity is not a concern in our models, as all variance inflation factors (VIFs) are below 2. Pseudo R2 and likelihood-ratio tests were used to assess whether adding variables at each step significantly improved model fit. Seemingly unrelated regression (SUR) was used to estimate mediation pathways and to obtain direct and indirect effects, controlling for all covariates (Preacher & Hayes, 2008). Standard errors and 95% confidence intervals were obtained using bootstrapping with 1,000 replications. We also conducted a sensitivity analysis excluding care recipients who resided in long-term care settings, as caregivers of these individuals likely experience differential financial strain and health-related outcomes. Population weights were applied in regression models to obtain proper statistical inference. Participants with missing data were excluded from analyses. To assess the potential impact of missing data, we performed a simple imputation sensitivity analysis, using mean imputation for continuous variables and mode imputation for categorical variables. All analyses were conducted with STATA 17 (StataCorp); a p-value of <.05 was used to denote statistical significance.
Results
Characteristics of Care-Recipients and Caregivers
Sample Characteristics (N = 1,223)
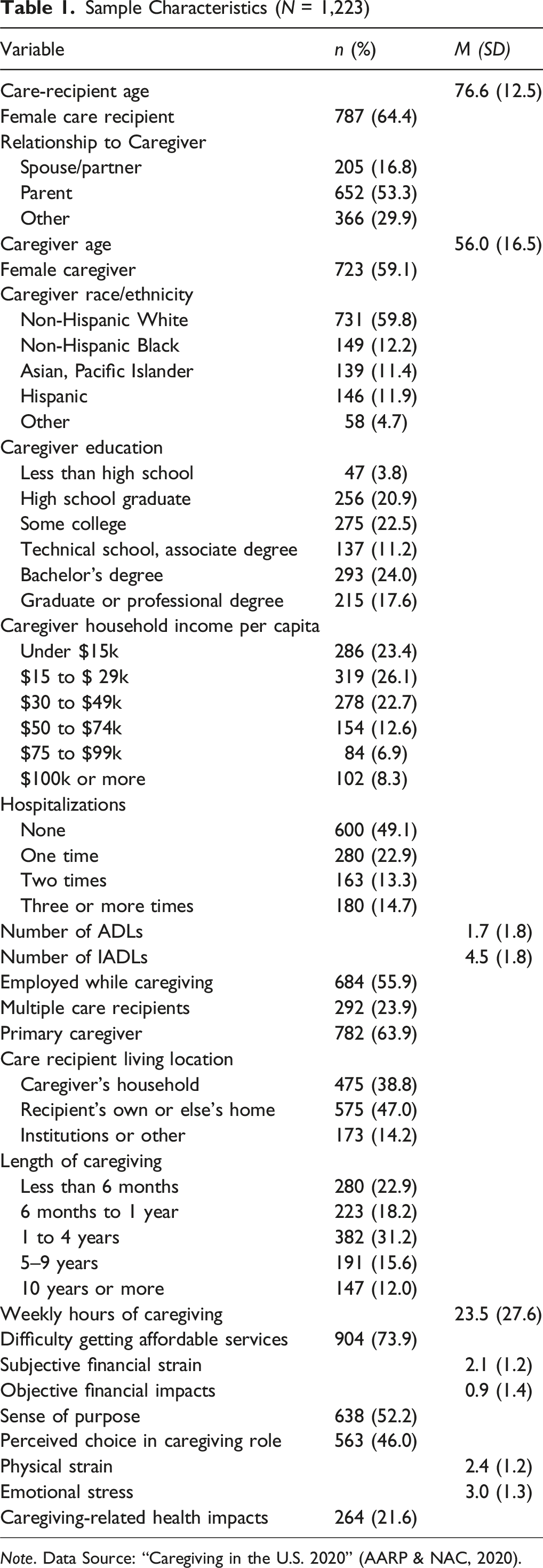
Note. Data Source: “Caregiving in the U.S. 2020” (AARP & NAC, 2020).
Multivariate Analyses
Factors Associated With Health-Related Outcomes
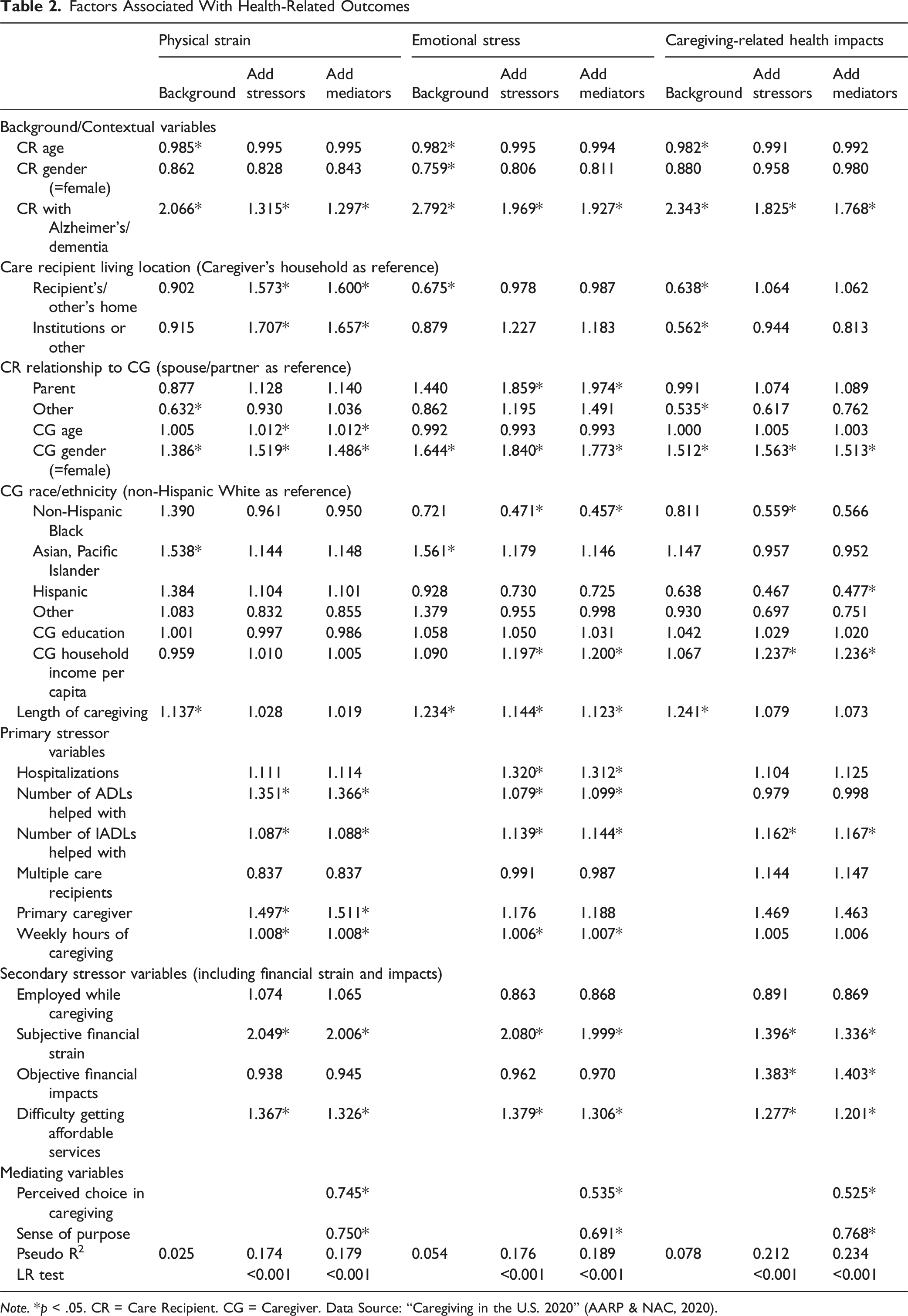
Note. *p < .05. CR = Care Recipient. CG = Caregiver. Data Source: “Caregiving in the U.S. 2020” (AARP & NAC, 2020).
Factors Associated With Physical Strain
Summary of Mediation Analysis
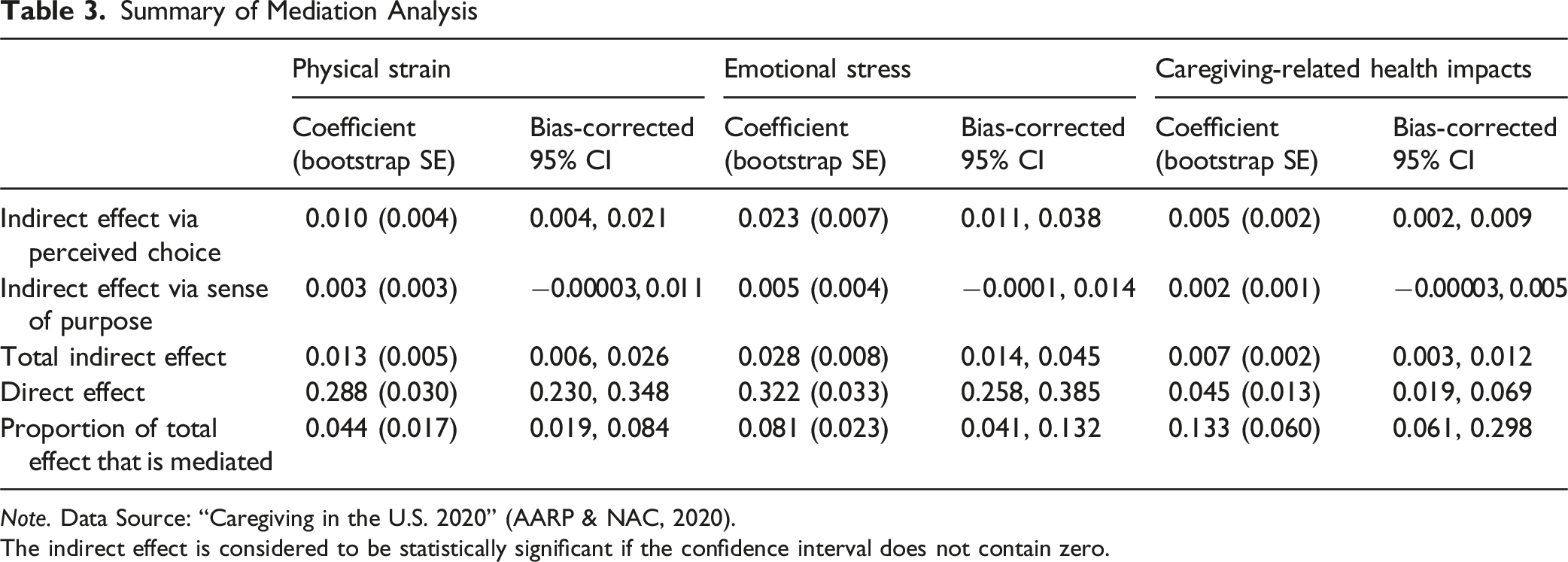
Note. Data Source: “Caregiving in the U.S. 2020” (AARP & NAC, 2020).
The indirect effect is considered to be statistically significant if the confidence interval does not contain zero.
Factors Associated With Emotional Stress
For the emotional stress outcome, caregivers for an individual with ADRD were 1.93 times (OR = 1.93, p < .001) more likely to report greater emotional stress. Other significant background characteristics that emerged as predictors of elevated emotional stress included providing care for a parent versus spouse (OR = 1.97, p = .003), female caregiver gender (OR = 1.77, p < .001), higher household income per capita (OR = 1.20, p < .001), and longer legnth of caregiving (OR = 1.12, p = .015). Further, non-Hispanic Black caregivers reported lower emotional stress compared to non-Hispanic White caregivers (OR = 0.46, p < .001).
When examining primary and secondary caregiving stressors, care-recipient hospitalizations (OR = 1.31, p < .001), higher ADL (OR = 1.10, p = .015) and IADL (OR = 1.14, p < .001) assistance, more weekly caregiving hours (OR = 1.01, p = .012), and difficulty accessing services (OR = 1.31, p < .001) all significantly predicted higher emotional stress. While objective financial strain did not significantly predict emotional stress, caregivers experiencing higher subjective financial strain were approximately twice as likely to report elevated emotional stress compared to those with lower financial strain. When sense of purpose (OR = 0.69, p = .002) and perceived choice (OR = 0.54, p < .001) were included in the model, the odds ratio for subjective financial strain was reduced from OR = 2.08 to 2.00. Inspection of 95% bootstrap bias corrected confidence intervals (Table 3) showed a statistically significant indirect effect for perceived choice in the caregiving role. Although the direct effect remained significant, results indicate the relationship between subjective financial strain and emotional stress was partially mediated by perceived choice in the caregiving role, accounting for 8.1% of the total effect. However, the indirect effect via sense of purpose was not significant.
Factors Associated With Caregiving-Related Health Impacts
For the outcome of caregiving-related health impacts, ADRD status (OR = 1.77, p = .002), female caregiver gender (OR = 1.52, p = .027), and higher household income per capita (OR = 1.24, p = .001) were significantly associated with negative health impacts. Hispanic caregivers, in contrast, had lower odds of reporting negative health impacts compared to non-Hispanic White caregivers (OR = 0.48, p = .015). Among care-related stressors, greater IADL assistance (OR = 1.17, p = .013) and difficulty accessing affordable services (OR = 1.20, p = .013) also significantly predicted negative health impacts. In contrast to the above models, results showed that both objective (OR = 1.40, p < .001) and subjective (OR = 1.34, p = .001) indicators of financial strain were significantly associated with negative caregiving-related health impacts. Sense of purpose (OR = 0.77, p = .001) and perceived choice in the caregiving role (OR = 0.53, p = .001) were significantly associated with a lower likelihood of reporting negative caregiving-related health impacts. When examining these two variables as mediators, confidence intervals (Table 3) showed a statistically significant indirect effect for perceived choice in the caregiving role. Although the direct effect remained significant, results indicate the relationship between subjective financial strain and caregiving-related health impacts was partially mediated by perceived choice in the caregiving role, accounting for 13.3% of the total effect. However, the indirect effect via sense of purpose was not significant.
Marginal Effects of Financial-Related Strain
Given that subjective financial strain emerged as a significant predictor across all three study outcomes, we estimated the marginal effects of increasing subjective financial strain on the predicted probability of each health-related outcome (Figure 2). Results showed that as financial strain increased from minimal to very high levels, the predicted probability of experiencing physical strain increased from 61% to 95%. Similarly, the probability of experiencing emotional stress increased from 78% to 98% as financial strain increased. In contrast, perceived negative health impacts demonstrated a more modest relationship, with predicted probability increasing from 16% to 32% across increasing levels of financial strain. Marginal effects of subjective financial strain on health-related outcomes.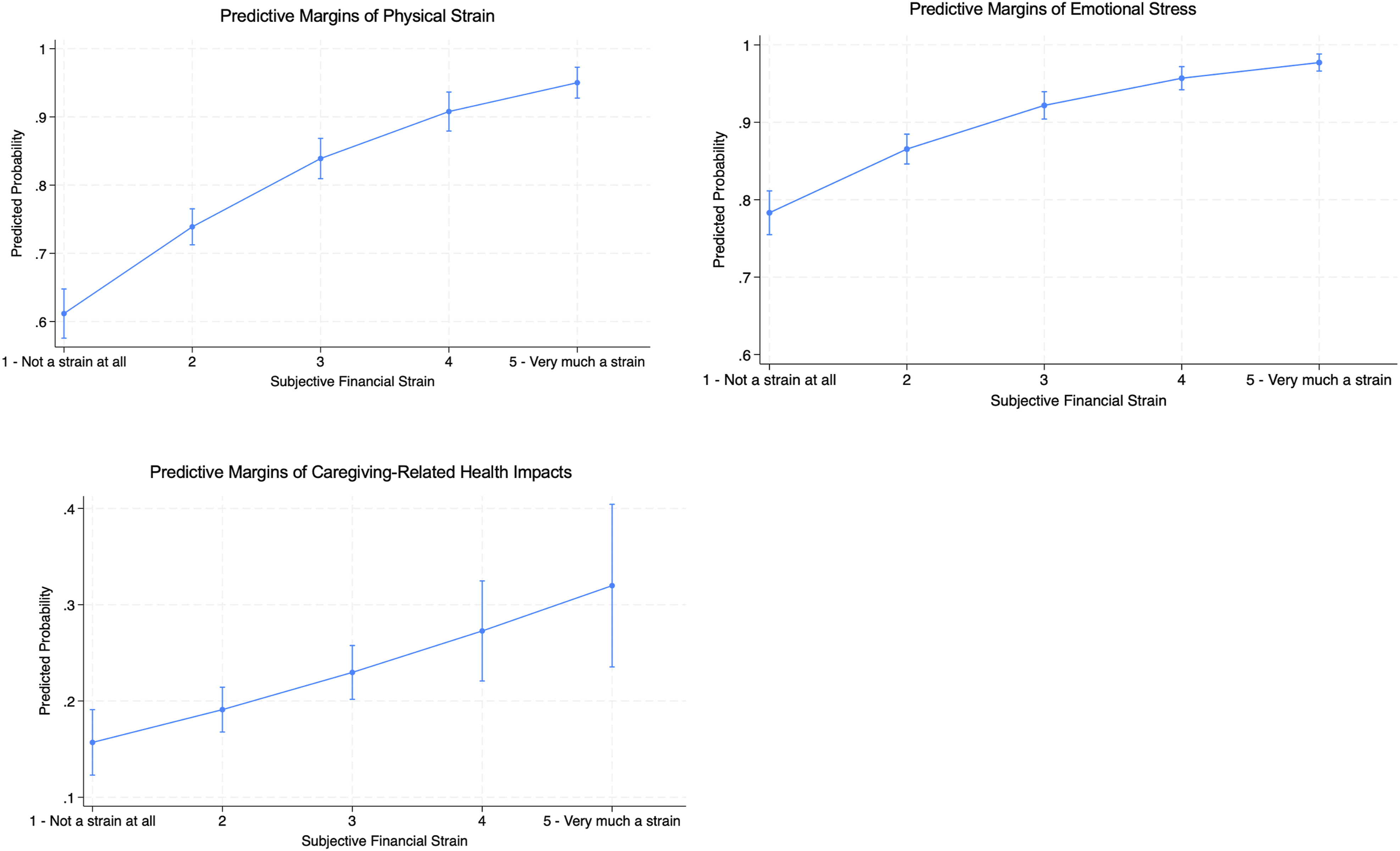
Sensitivity analyses using simple imputation yielded consistent results with the primary findings (Supplemental Materials, Table S1). Sensitivity analyses excluding care recipients residing in institutions or other settings also yielded similar results to the full sample (Supplemental Materials, Table S2); caregivers’ subjective financial strain remained significantly associated with higher levels of physical strain (OR = 2.07, p < .001), emotional stress (OR = 2.07, p < .001) and an increased likelihood of experiencing negative health impacts (OR = 1.31, p = .005).
Discussion
This study is the first to our knowledge to examine the influence of financial strain on family caregiver outcomes using Pearlin’s stress process model as a guiding theoretical framework (Pearlin et al., 1990). Study findings provide insights on how objective and subjective metrics of financial stress in family caregivers contribute to physical strain, emotional stress, and negative health impacts. Although objective financial impacts was not associated with physical strain or emotional stress, it was significantly associated with negative impacts on caregivers’ health. Moreover, caregivers who reported high subjective financial strain were more likely to report higher levels of physical strain and emotional stress, as well as negative health impacts, compared to those with lower levels of subjective financial strain.
Consistent with our modified application of Pearlin’s stress process model, we examined perceived choice in caregiving and sense of purpose as coping-related psychological resources that shape how financial strain is appraised and influence health outcomes. Findings showed that perceived choice in the caregiving role partially mediated the relationship between subjective financial strain and health-related outcome variables—specifically lower physical strain, emotional stress, and caregiving-related health impacts, thereby attenuating the negative effects of subjective financial strain. These findings align with the material–psychological–behavioral model of financial hardship (Tucker-Seeley & Thorpe Jr, 2019), which emphasizes that material conditions (e.g., objective financial impacts) and psychological appraisals (e.g., perceived financial strain) represent distinct but related dimensions of financial stress. The more consistent associations observed for subjective financial strain suggest that psychological appraisals of financial hardship may be especially salient for caregiver health and well-being, even when objective financial impacts are modest. In contrast with literature (e.g., Drentea & Reynolds, 2015; Frankham et al., 2020; Lee & Zurlo, 2014) showing that variables such as mastery and social support can impact the associations between caregiver burden and depression, our results found these mediating variables only partially influence the relationship between subjective financial strain and health outcomes. While adaptive internal coping strategies are one important mechanism that can positively influence how caregiving is experienced and perceived (Pearlin et al., 1990), these characteristics alone may not be sufficient to counterbalance the subjective and objective stress uniquely derived from the financial aspects of care provision. It is possible that psychological resources alone are not enough to compensate for the fundamental resource limitations imposed by financial challenges.
Difficulty accessing affordable services was also a significant factor contributing to poorer caregiver outcomes. Caregivers often rely on external services, such as meal delivery, transportation, respite care, and home health services, to meet the complex needs of their care-recipients while managing their own lives. Consistent with the Conservation of Resources theory, intensifying care demands will deplete resources from other responsibilities, such as job demands, ultimately leading to greater levels of work-related stress, as well as physical and emotional strain (Dugan et al., 2020). When services are not affordable, caregivers are forced to take on additional responsibilities themselves, which intensifies their workload and the associated costs of care provision. Such stressors further increase risk for adverse physical, emotional, and health outcomes.
Results are also consistent with a substantial body of prior research identifying ADRD caregiving as particularly burdensome due to the intensive and unpredictable nature of disease progression. For example, prior research has shown that ADRD caregivers provide substantially more physical and medical assistance than other caregivers and experience greater overall burden (Freedman et al., 2022), underscoring the importance of considering care-recipient diagnosis as a contextual characteristic that shapes caregiving demands, particularly with respect to IADL assistance and care intensity (Dauphinot et al., 2015; Kang et al., 2014).
Our findings also highlight practical implications to support caregivers. For example, expanding subsidies, tax credits, and direct financial assistance to reduce the economic burden of caregiving would enable caregivers to afford essential support. Increasing the availability of publicly funded respite care and in-home services, either at no-cost or discounted rates, could provide caregivers with critical relief and reduce strain. Additionally, enhancing a caregiver’s sense of control and purpose can mitigate the negative impacts of caregiving. Strategies such as accessible counseling, peer support, and stress management programs can help caregivers develop knowledge, share their experiences, build resilience, and maintain a sense of purpose. Advancements in digital platforms continue to enhance the accessibility of these services, which can be effective interventions in relieving the distress associated with inadequate knowledge, skills, and information (Shin & Choi, 2020). These interventions aimed at reducing caregivers’ subjective financial strain, increasing access to affordable services, and enhancing perceived sense of purpose could collectively empower caregivers and alleviate caregiving-related health impacts.
Despite these important findings, our study has limitations. First, the cross-sectional design precludes the ability to imply causal inference regarding the temporal relationship between subjective financial strain and health-related outcomes. Future longitudinal studies using repeated measures are needed to assess the directionality of these associations. Additionally, the secondary data used in this study does not include direct measurements of caregiving-related costs, which could be compared against household income to provide a more accurate assessment of financial strain. Further, our analytic sample included family caregivers of older adults residing in both the community and in long-term care settings, and caregiver experiences in these settings may differ in ways that limit the generalizability of the observed associations. Lastly, our model may have excluded other important mediating factors, such as social resources and individual coping strategies that also may influence or mediate the negative effects of stressors. These factors should be explored in future research.
Conclusion
Overall, results of this study contribute to the development of a better understanding of financial strain among family caregivers and its association with negative health-related outcomes. Taken together, findings highlight how financial strain—conceptualized as both material conditions and psychological appraisals—operates within the caregiving stress process to shape caregiver health and well-being. Results underscore the importance of addressing both economic constraints and psychological resources to mitigate adverse outcomes for caregivers in high-intensity roles.
Supplemental Material
Supplemental Material - Health-Related Consequences of Financial Strain Among Family Caregivers in the U.S.
Supplemental Material for Health-Related Consequences of Financial Strain Among Family Caregivers in the U.S. by Yujun Zhu, Susan Enguidanos, Carissa Liu and Francesca B. Falzarano in Research on Aging.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partially funded the USC Center for Advancing Family Caregiver Financial and Workplace Security which is supported by the Administration for Community Living (ACL), U.S. Department of Health and Human Services (HHS) through award number 90CGPS0005-01-00 as part of a financial assistance award with 75% funded by ACL/HHS and 25% funded by non-government source(s). Research reported in this publication was also supported by the National Institute on Aging of the National Institutes of Health (NIH) under Award Number R00AG073509 (PI: Falzarano). The contents are those of the author(s) and do not necessarily represent the official views of, nor an endorsement by ACL/HHS, NIH, or the U.S. Government.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The “Caregiving in the U.S. 2020” public use data files are publicly accessible on the National Alliance for Caregiving website. This study is not preregistered.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.