
Abstract
The posture undergoes changes during aging and may serve as a marker for the evaluation of the thoracic spine. This study aimed to correlate the variables for the evaluation of thoracic spine mobility and propose predictive equation models from the measurements of the thoracic Schober test and the digital inclinometer in older adults. The mobility of thoracic flexion and extension by levels (T1, T8 and T12) of 41 older adult subjects (66 ± 7 years) was quantified with a digital inclinometer (degrees) and Schober’s test (cm). There was a moderate positive correlation between the digital inclinometer and the Schober test at T1 (r = .69), T12 (r = .60), and total flexion levels T1 to T12 (r = .74). Simple linear regression equations showed that thoracic Schober predicts thoracic mobility measures for these same levels. Moderate to strong correlations were observed between the inclinometer and the Schober Test measurements. The development of predictive equation models based on the thoracic Schober test could potentially enhance the ability to predict spinal mobility in physically independent older adults.
Introduction
Alterations in spinal posture are among the changes that coincide with the aging process. Thoracic kyphosis is a common change among older adults, with a reported prevalence of 20%–40%. This percentage is believed to increase as the population ages (Hijikata et al., 2022). Increased thoracic kyphosis can be a marker of limited spinal mobility. This type of spinal deformity has been associated with low self-esteem, reduced quality of life, decreased ability of older adults to maintain balance, and functional limitations. These changes can lead to an increased risk of falls in this population (Koelé et al., 2020).
Increased thoracic kyphosis and postural stiffness are commonly associated with aging and many pathological conditions. Simple clinical measures are needed to estimate the relative degree of postural stiffness to determine whether clinical interventions, such as exercises, are effective (Koelé et al., 2020). However, research examining thoracic spine mobility and its relationship with spinal posture in older adults who are physically independent is currently scarce (Hijikata et al., 2022).
The evaluation of thoracic spine mobility can be performed using different resources. Analyses by video systems (3D optoelectronics) are considered the gold standard (Negrini et al., 2016). However, the high cost of acquisition, the need for a controlled space, and specialized evaluators make the method clinically unfeasible (Määttä et al., 2022; Norlander et al., 1995; Takatalo et al., 2020). On the other hand, simpler and clinically applicable methods have been investigated in the literature, including the digital inclinometer, which quantifies spine mobility in degrees, and the Schober test, which measures spine mobility in centimeters. Both methods have acceptable validity and reliability in the literature (intraclass correlation coefficient = .95–.98) (Furness et al., 2018; Huang et al., 2022).
MacIntyre et al. (2014) assessed thoracic spine posture using the digital inclinometer and concluded that increased kyphosis could be a marker for mobility limitations in older adults. On the other hand, according to Takatalo et al. (2020), several measuring devices have been used to quantify posture, but as for thoracic spine mobility, it has been neglected in the study of the spine, and further investigations with simple methods for clinical examination of the spine are needed. In addition, it is observed that most studies have been performed with young individuals and rarely in older adults.
The relationship between methods of measuring thoracic spine mobility in people already experiencing aging is unclear, and studies evaluating thoracic spine mobility and the correlation with posture in physically independent older adults are scarce. Instead, many studies focus on exploring changes in kyphosis with functional performance and even with the risk of falls (Hijikata et al., 2022), which is quite useful in helping to identify risk factors for aging; however, this requires a thorough understanding of segmental spinal biomechanics.
Within this context, there is a need to explore a practical and low-cost clinical test to measure the mobility of the thoracic spine in an attempt to improve the models for assessing the spine in older adults. Thus, this study aims to correlate the variables for assessing the mobility of the thoracic spine of physically independent older adults. Furthermore, it is expected to propose models of predictive equations from the measurements, in degrees, obtained by the digital inclinometer and the thoracic Schober test, obtained in centimeters, in order to assist in the biomechanical characterization of the thoracic spine in physically independent older adults.
Methods
Participants
This is a cross-sectional study, which is a type of observational study that measures the outcome and the exposures of interest in a group of people at the same time (Setia, 2016). The participants are older adults and were recruited voluntarily and for convenience in the local community, taking into account the availability of the older adults to be part of the sample and the ease of access to them, who were contacted by telephone according to the register available at the health center. The eligibility criteria for this study were: older adults over 60 years of age considered physically independent, classified in level 3 or 4 of the functional status scale proposed by Spirduso, which characterizes older adults as being able to perform the basic activities of daily living and also the instrumental activities of daily living (Spirduso, 2005); absence of any thoracic spine pain, neurological, metabolic and/or orthopedic disease of high severity, such as spinal surgeries or fractures. Older adults who were unable to perform the proposed movements were excluded. The research was approved by the Ethics Committee of Pitágoras Unopar University (#: 5.103.494).
Patient Preparation
All data were collected in a community sports activity center, which provided adequate lighting and temperature (±22°C). Before the evaluation, each participant answered a brief questionnaire about anthropometric characteristics, the presence of acute (<4 weeks) or chronic (>12 weeks) low back pain, and the level of physical activity using the International Physical Activity Questionnaire (IPAQ). The mobility assessment sessions using spinal movements were a maximum of 1 hour for each participant. All participants were familiarized with the equipment and procedures before the measurements. A trained physiotherapist with ten years of experience in spinal assessment obtained all measurements.
Measurement of Thoracic Spine Mobility with Inclinometer and Tape Measure
The mobility of the thoracic spine was actively measured during flexion and extension movements using the tape measure in the Schober test and by the digital inclinometer “ExaMobile S. A. Laser Level and Inclinometer” integrated into the iPhone 11. For the Schober test of the thoracic spine, the tape measure is placed at the marked points, from the spinous process of T1 to the level of T12, and active flexion of the thoracic spine is requested. After completing the movement, the difference between the initial and final measurements (T1 and T12) is recorded as the Schober test flexion value of the thoracic spine. Normal mobility values are those that show a gain of at least 5 cm on the tape measure (Takatalo et al., 2020).
The integrated digital inclinometer is a fast, convenient, accurate, and reliable method (intraclass correlation coefficient = .95–.98) for measuring thoracic spine angles when compared with other instruments for measuring range of motion in degrees, such as radiography, which is the gold standard for measuring thoracic kyphosis angles (Furness et al., 2018; Huang et al., 2022). To obtain measurements of thoracic spine segmental mobility, the thoracic spine was divided into three levels: upper thoracic at the level of the first thoracic vertebra (T1), middle thoracic at the level of the eighth thoracic vertebra (T8) and lower thoracic at the level of the 12th thoracic vertebra (T12). To ensure the correct measurement of these levels, the spinous processes of T1, T8, and T12 were located first, as suggested by Norlander et al. (1995), where first the last cervical vertebra (C7) is palpated and, with the aid of the tape measure, 15 cm is counted to reach T5. Thereafter, every 3 cm, there is a new spinous process of the thoracic spine. The integrated digital inclinometer was first positioned at the level of T1, where the evaluator fixed with the help of his hands the base of the smartphone in this region so that horizontally, the angulation arrow pointed to ninety (90) degrees and vertically, it pointed to zero (0) degrees. The measurements were obtained with the participant seated to minimize the influence of the lumbar spine on the observed amplitude. With hands positioned crossed on opposite shoulders, the maximum active thoracic flexion was asked, and the angular values of the initial and final positions of the active movement shown on the inclinometer were recorded, after which the participant was instructed to return to the initial position. The same procedure was performed for T8 and T12. To measure the total mobility of the spine in flexion (T1 to T12), the total sum of the mobility values obtained for each level T1, T8, and T12 was considered, which were summed and divided by 3. For the thoracic extension movement, the hands were asked to be positioned at the base of the nape of the neck and asked to extend actively. The values of the initial position and that of the total extension were then recorded. For the Schober test of the thoracic spine, the measuring tape was placed at the marking points from the spinous process of T1 to the level of T12, active flexion of the thoracic spine was requested, and the difference between the initial and final measurements (T1 and T12) was recorded as the Schober test flexion value of the thoracic spine, as suggested by Takatalo et al. (2020).
Statistical Analysis
The sample size calculation was performed based on the estimates assigned for correlation between two spinal evaluation variables (angle x centimeters). Considering an alpha of .05 and, a power of 90%, correlation of .50 (Määttä et al., 2022), the number needed for the present study was 37 participants; the sample size calculation was performed in G*Power version 3.1.5. Descriptive statistics presented the data with central tendency, mean, and standard deviation measures. The parametric distribution of data was verified by the Shapiro-Wilk test. For comparison of categorical data, the Chi-square test of independence was applied. Correlations between variables were performed to identify the association between thoracic Schober test measurements (in centimeters) and thoracic spine flexion mobility measurements (in degrees). The correlation between the variables was classified as: .0 to .30, insignificant correlation; .30 to .50, low correlation; .50 to .70, moderate correlation; .70 to .90, strong correlation; .90 to 1, very strong correlation (Mukaka, 2012). Simple regressions were calculated and analyzed to propose predictive equation models considering the obtained values of thoracic spine mobilities. For all statistical analyses, a significance of p < .05 was accepted, and data analysis was performed using the software packages IBM SPSS Statistics for Windows (Version 20.0. Armonk, NY: IBMCorp) and GraphPrism (Version 6.01).
Results
A total of 41 older adults completed the tests and were included in the analysis of this study. Anthropometric data are presented below in mean and standard deviation and in median and interquartile range [25/75]. The mean age was 66.15 (±7.02) years, height 1.60 m [1.43–1.76], and weight 70.1 kg [50.6–116.0]. Of the 41 participants, 32 were female (78%) and nine were male (22%). Regarding the characterization of the level of physical activity, the occurrence of low back pain, posture classification, and occurrence of falls among the participants included in the study (n = 41), the following data were found: 6 (14.6%) participants had no low back pain, while 35 (85.4%) had chronic low back pain (>12 weeks). The level of physical activity (IPAQ) was considered active for 9 (22%) participants, Irregularly Active A for 18 (43.9%), Irregularly Active B for 11 (26.8%); and sedentary for 3 (7.3%) participants, according to the time of physical activity, in minutes, per week. In this sample, 22 participants (53.7%) had suffered falls in the last 12 months, and 19 participants (46.3%) had not fallen in the same period. However, none had major or disabling consequences.
Prediction Equations for Thoracic Spine Mobility Obtained by Simple Linear Regression for Schober’s Test Values (in cm) and Inclinometer (in Degrees)
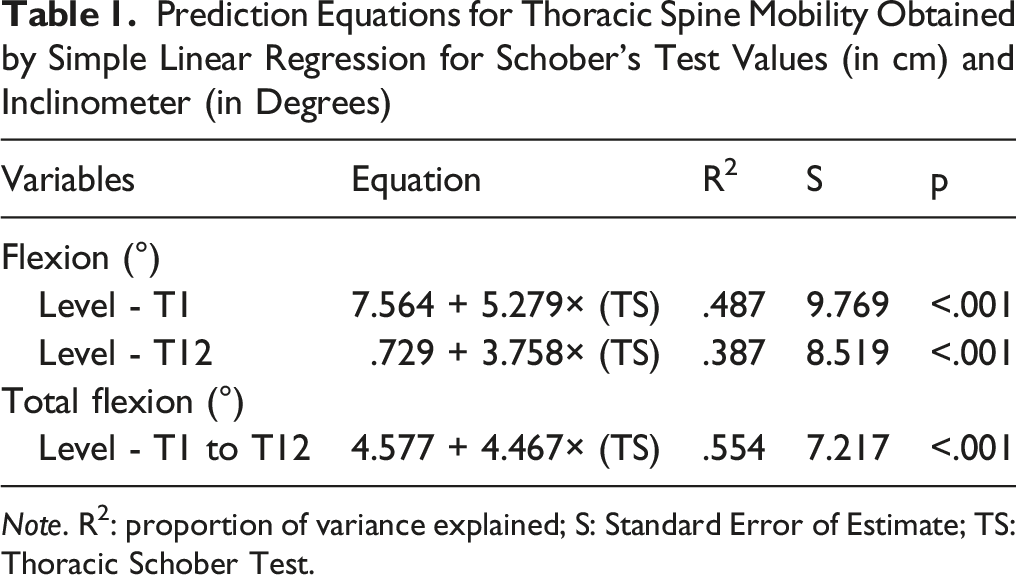
Note. R2: proportion of variance explained; S: Standard Error of Estimate; TS: Thoracic Schober Test.
Discussion
This study investigated the correlation between the thoracic spine mobility assessment variables and the posture classification of physically independent older adults and sought to propose predictive equations between the measurements of this mobility. Overall, moderate to strong correlations were found between the assessment variables (digital inclinometer and Schober test), and predictive values were proposed for thoracic spine mobility using the Schober test.
Studies evaluating the mobility of the thoracic spine and the correlation with posture in physically independent older adults are scarce. However, even with few works available for comparison, although with some peculiarities in methodology and population, we can observe that our results are in agreement with described data of overall increased mobility in thoracic segments from T8 (p = .019) (Ignasiak et al., 2017; Wilke et al., 2017; Määttä et al., 2022), total mobility in flexion from T1 to T12 (p = .018) (Hinman, 2004); and with a moderate positive association between Schober test and spine mobility (r = .53–.69) (Määttä et al., 2022).
Määttä et al. (2022) assessed the thoracic spine mobility of 73 individuals (22–56 years old) using an inclinometer and found greater mobility at the mid-thoracic level of T8, which was associated with worse reported thoracic spine pain (OR = .95; IC 95%: .92–.99). Another in vitro biomechanical study by Wilke et al. (2017) with 68 functional human thoracic spinal units investigated the segmental and neutral zone range of motion of the healthy human thoracic spine by applying for thoracic flexion and extension and found a greater range of motion in the upper half of the thoracic spine from T6-T8, corroborating with the findings of the present study for greater mobility in the T8 segments.
Schober’s test method has been validated in several studies (Rezvani et al., 2012; Tousignant et al., 2005). However, the method is commonly applied in the lumbar region, but the thoracic Schober test is less studied, and despite being a validated and low-cost clinical tool, few studies correlate the Schober test with other chest spine evaluation instruments, such as the inclinometer. Despite the scarcity of studies that have evaluated thoracic spine mobility, we found a similar correlation and simple linear regression results between the Schober test and the inclinometer for thoracic spine mobility in the study by Norlander et al. (1995). Despite being older, this study provides a relevant clinical method to measure the distribution of segmental flexion of mobility in the thoracic spine. We also have the study by Määttä et al. (2022). Although it was conducted in an adult population (22–59 years old), not specifically in older adults, it was the study that came closest in detail to our methodology and objectives. We were able to compare our values and the data obtained in this study.
Regarding the Schober measurements correlated with the inclinometer measurements, a non-linear trend was also observed when the Schober showed low degrees of amplitude, especially when it marked 2 cm of distraction at the T1 and T12 levels, where a non-similar behavior was observed in the inclinometer compared to the other subjects who obtained the same measurement. This fact may be related to the influence of the cervical and lumbar segments on mobility at T1 and T12 levels, respectively, where ROM restriction at these levels may be accompanied by an increase in compensatory mobility of the cervical and lumbar spine and, in these cases, inclinometer values may vary from subject to subject and have interfered with this nonlinear trend (Horton et al., 2005; Mimura et al., 1994; Panjabi et al., 1993; Pooni et al., 1986).
We found a linear regression similar to ours in the study by Norlander et al. (1995). They validated the use of a tape measure for skin distraction (Schober’s test) in assessing segmental mobility of the thoracic spine using the inclinometer (n = 42) and found a positive linear relationship between spine flexion mobility at the T1 and T8 level (in degrees) and Schober’s test (in centimeters) (R2 = .48; p < .001; R2 = .44; p < .001), data similar to the results found in our study. On the other hand, Määttä et al. (2022) did not find a linear regression in their correlations, as their logistic regression model was adjusted for age. The fact that their sample included young and adult participants at the beginning of the aging process made a total difference in our study, which assessed only older people participants. In the present work, it was possible to find a linear model, and through a thorough analysis.
One of the main problems of clinical measurements of the spine is due to the fact that the values expressed in these tests vary not only due to the different degrees of aptitude and experience of the examiners but also due to the lack of standardization of the tests. Ideally, professionals should have at their disposal a simple, standardized, and reliable battery of tests to evaluate patients, and different examiners should achieve similar results when evaluating the same patient (Huang et al., 2022). Within this context, the equations found in our study could simplify this assessment, eliminating the need for this standardization of tests since two instruments for assessing thoracic mobility would not be necessary, but only one, which would be the tape measure.
We highlight as a strength of the findings that the equations also enable a quick analysis of mobility in degrees, without the need for direct application of the inclinometer, which represents a time saving, especially if the professional is not familiar with the inclinometer, where the chances of measurement errors are greater and can lead to incorrect observations. Our study may encourage practitioners to perform thoracic spine mobility assessment in a quick and simplified manner and consider thoracic spine assessment in their clinical practice.
Some limitations may be presented, among them, the results of the present study are from specific equations for postures assessed in sitting, and this could generate different values about their applicability in postures assessed in standing. The total spinal mobility used in this study has not been validated for the older adult population. Although the results indicate a strong correlation, this value should be interpreted cautiously. However, we believe that these equations can be replicated under these conditions, as Määttä et al. (2022) found strong to very strong intra-examiner reliability (Kappa .78 and .87) for postural assessment in sitting and standing positions. However, this should be evaluated. Another limitation would be about the sample characteristics, with the participation of more women (n = 35). At the same time, the number of men was low (n = 6), and our equations need to be confirmed in other populations. Finally, we hope that this study may encourage further research exploring the relationship between mobility measures with other points of interest for aging such as functional performance measures.
Conclusion
The results of this study showed that there are moderate to strong correlations between the variables of thoracic mobility evaluation and insignificant mobility and posture in physically independent older adults. Furthermore, predictive equation models were proposed by means of the thoracic Schober test, obtained in centimeters. With this, we believe that characterization of thoracic spine mobility may support the identification of abnormal movements and/or be used to improve biomechanical models of the spine in physically independent older adults.
Supplemental Material
Thoracic Spine Mobility and Posture: Correlation and Predictive Values in Physically Independent Older Adults
Thoracic Spine Mobility and Posture: Correlation and Predictive Values in Physically Independent Elderly by Ana Paula de Sousa Almeida, Edine Kavano Kitahara Matsui, Fabio Nascimento da Silva, Fernanda Borges de Oliveira Vasconcelos and Márcio Rogério de Oliveira in Evaluation & the Health Professions
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.