
Abstract
Objective:
Few studies have detailed the physical activity and postural patterns (e.g. lying or sitting) in older adults with declining activities of daily living (ADL). Therefore, we aimed to address this issue by quantifying physical activity using an accelerometer and measuring time spent in various postures among older adults in assisted-living residences.
Methods:
We quantified physical activity using an accelerometer (ActivPAL) and measured time spent in various postures in 35 older adults (mean age: 89.1 years) with chronic conditions residing in two assisted-living residences in Japan. ActivPAL was attached to the thigh and trunk of patients to distinguish between sitting and lying postures.
Results:
Participants had a mean count of 6.2 comorbidities, and they were divided into three groups (fully independent, requiring minimal assistance and requiring care) based on their activities of daily living capacity using the Barthel Index. Residents aged ⩾90 years walked a mean of 1109.1 steps and spent 167.3 min upright per day. Fully independent participants walked a mean of 3587.6 steps daily; those requiring minimal assistance walked 1681.0 steps daily; and those requiring care walked 428.9 steps daily.
Conclusions:
Our findings indicated that step count, number of sit-to-stand transitions, stepping time, and upright time decreased significantly as activities of daily living capacity decreased. Comorbidity type and number of comorbidities were not related to their lying time except for depression status. Lying time was associated with depression status.
Introduction
The World Health Organisation recommends that weekly physical activity should include 150–300 min of moderate-to-vigorous-intensity aerobic activity, 2 days of muscle-strengthening activities, and three sessions of multicomponent physical activity.1,2 However, given the tendency for physical function to decrease with age, whether these recommendations are appropriate for adults over the ages of 75 or 90 years remains to be determined.3,4 A previous study reported that community-dwelling older adults walk 864–15,847 steps per day 5 ; and older adults aged ⩾80 years exhibit a sedentary behaviour (SB) for an average of 10.6 h during waking hours. 6 Moreover, adults in these age groups often have multiple comorbidities, such as cardiovascular diseases and musculoskeletal disorders; therefore, more specific physical activity recommendations may be necessary. Several interdisciplinary studies have examined the importance of physical activity in the oldest old (i.e. people aged ⩾90 years); these studies have reported relationships among age-related reductions in motor, physical, and cognitive abilities as well as sharp rises in dementia incidence in people aged ⩾90 years.7,8 Moreover, multimorbidity has a negative relationship with physical activity in older adults. 9 Multimorbidity and physical activity of older adults were associated with increased medical expenditure.10,11
In addition to the social burden associated with such comorbidities, very low levels of physical activity, excessive bed rest, and extended bedridden periods can lead to various physiological changes in the musculoskeletal, respiratory, genitourinary and cardiovascular systems in older adults.12,13 For example, the supine position decreases lung volume, resulting in atelectasis, and interrupts mucociliary clearance of the airways. 12 In addition, the supine position impairs coughing to clear secretions. 12 These functional changes predispose individuals to pneumonia; moreover, low performance status, such as total confinement to the bed or chair, has shown a positive association with pneumonia. 14 Furthermore, the supine position affects the bladder function of voiding, leading to urinary retention. 12 This change predisposes individuals to urinary tract infections, and being bedridden is reportedly associated with urinary tract infections. 15 To promote expectoration and urination, light physical activity and postural adjustments (e.g. increased time spent sitting versus time spent lying down or increased frequency of sit-to-stand transitions) might aid in preventing pneumonia and urinary tract infections in the older population. However, to the best of our knowledge, few studies have investigated the detailed physical activity and posture assessment of older adults, including the differences between lying and sitting postures, and the association between those assessment and their comorbidities. Another study 16 using a questionnaire assessed the lying time for older adults; a more precise evaluation using an accelerometer would be needed.
Clarifying current physical activity levels and detailed postural patterns, including sitting and lying, in this population is critical for determining the appropriate daily physical activity or posture for very old adults or older adults with multiple chronic conditions. In the present study, we aimed to address this issue by quantifying physical activity using an accelerometer and measuring time spent in various postures in older adults in assisted-living residences. In addition, we explored how the activities of daily living (ADL) in this population and comorbidities were associated with the participants’ physical activity and posture.
Methods
This is a preliminary report, a subset at a starting point in time in a prospective cohort study on physical activity and posture in older adults residing in two assisted-living residences. We recruited patients residing in two facilities; each facility administered home-based care provided by primary care physicians in each clinic. Participants ⩾65 years of age receiving regular home care visits and residing in two assisted-living residencies were recruited between 2 July 2020 and 30 June 2021. Patients with terminal illnesses were excluded. The Ethics Committee of our institution approved the study design (reference 20200217-3). Written consent for study participation was obtained from each patient and/or their family.
Data collection
Data collected for this study included age, sex, smoking history, alcohol history, nutritional status, muscle strength, ADL, required level of care, comorbidities, number of medications received and physical activity. Physical activity is reportedly related with health conditions such as muscle strength, nutritional status, comorbidities, and medications.9,17,18 We aimed to investigate the condition of patients in our target population and how factors, including muscle strength, nutritional status, comorbidities, and ADL level, affected the physical activity of our participants.
Nutritional status and muscle strength
Nutritional status was assessed using the body mass index (BMI), serum albumin levels, and maximum calf circumference. Handgrip strength was measured to assess muscle strength.
Activities of daily living
Functional capacity for ADL was assessed using the Barthel Index.
19
The Barthel Index assesses performance across 10 ADLs (feeding, bathing, grooming, dressing, bowels, bladder, toilet use, transfers, mobility and stairs), with scores ranging from 0 to 100 points. The maximum score of 100 indicates full independence in physical functioning, whereas the minimum score indicates complete dependence (i.e. bedridden). A score ⩾85 corresponds to independence with minimal assistance, whereas a score
Required level of care
The required level of care was categorised using the levels adopted by the Japanese long-term care insurance system. 21 In this system, a care-needs certification committee comprising experienced professionals in public health decide patients’ care level based on documents that include (1) the examination report by a municipal certification examiner and (2) the primary physician’s written opinion, including ADL assessment and cognitive function evaluation. Participants were divided into those requiring support (support level: 1–2) and those requiring long-term care (care-need level: 1–5) based on expert evaluations of mental and physical status. Higher levels correspond to lower ADL ability and lower cognitive function, indicating a greater need for support. Based on a previous study conducted in a home care setting, 22 participants were categorised into three groups according to their care-need levels: low (support level: 1–2), middle (care-need level: 1–2), and high (care-need level: 3–5).
Comorbidities
The presence of multiple health conditions is negatively associated with physical activity 9 ; there was a positive relationship between multimorbidity and polypharmacy. 18 Therefore, we gathered data on health conditions, including depression status, dementia scale, and multimorbidity status, and medications. Depressive symptoms and cognitive function were assessed using the Cornell Scale for Depression in Dementia23,24 and the Revised Hasegawa’s Dementia Scale, 25 respectively.
Multimorbidity was defined as the presence of two or more comorbidities from the following list of 17 health conditions: hypertension, diabetes, dyslipidemia, stroke, cardiac diseases, chronic respiratory diseases, digestive diseases, kidney diseases, urological diseases, arthritis or rheumatism, lumbar diseases, neurological diseases, mental disorders, endocrine diseases, malignancy, vision abnormalities and skin diseases. 26 Comorbidities were identified from medical records and confirmed by the attending physician of each patient.
Measurement of physical activity
Physical activity and posture were assessed using ActivPAL (ActivPAL4TM: PAL Technologies Ltd, Glasgow, UK) for 24 h/day for 4 days. In addition to ActivPAL, several wearable monitoring devices, such as ActiGraph (ActiGraph, Pensacola, FL, USA) and SenseWear 2 (BodyMedia, Pittsburgh, PA, USA), were used to measure physical activity. These three wearable monitors were appropriate for measuring SB and light-intensity physical activities (LPA), which have been proven to have a high test-retest reliability. 27 Particularly, ActivPAL was observed to have the highest overall criterion validity in measuring SB and LPA compared with the other two devices. 27 ActivPAL is recommended for assessing low-intensity activities and SB in older adults. 5
ActivPAL was used to examine physical activity in older adults. 28 Participants wore the device on their thigh and chest for six consecutive days. Daily physical activity levels were calculated by averaging data from four full days (24 h/day). Data from the first and last days (attachment/detachment days) were excluded. We used data on step count, number of sit-to-stand transitions, stepping time (min), and upright time (min) from the daily summarised data of ActivPAL software, PALanalysis.
In addition to the thigh monitoring device, a trunk monitor was attached to aid in assessing changes from the sitting to the lying posture, as previously described. 29 The system was designed to detect the inclination of the thigh, which reflects activities such as stepping, upright (standing posture including stepping activity), or sitting/lying (sedentary posture). The synchronised data were collected from the two devices and analysed in 15-s periods. Data, such as lying and sitting times, were derived from the 15-s period data. When both the thigh and trunk devices indicated sitting/lying, the posture was judged as lying. When the thigh device indicated sitting/lying but the trunk device indicated an upright posture, the position was judged as sitting.
Statistical analyses
The t-test was used to analyse continuous variables to compare physical activity/posture according to age classification. Kruskal–Wallis and Fisher’s exact tests were used to analyse continuous and categorical variables for comparing data including sex, age, serum albumin, grip strength, BMI, and comorbidities among the ADL levels classified into three groups. The Jonckheere–Terpstra test was used for trend analyses to compare physical activity and posture with ADL level. The level of significance was set at p < 0.05 for all tests. Spearman’s correlation was judged 0.3 or more as a meaningful relation and was used to explore the association between lying time and comorbidities. Multivariate linear regression analysis was used to further examine the association of physical activities with ADL. These analyses were adjusted for age, grip strength and serum albumin level. Serum albumin status and grip strength were indicators of older adults at risk of poor health; serum albumin status was related to serum albumin level; and whole-body muscle mass and grip strength were related to lower-extremity strength in older adults.30,31 We analysed the association between physical activities and ADL considering participants’ nutritional status and lower-extremity strength. STATA 17 (STATA CORP, College Station, TX, USA) was used for analysis.
Results
A total of 112 residents were selected from two facilities. We recruited participants whose primary physician or staff in the two assisted-living residences agreed that the patients met the study criteria. Among the 112 residents, 40 agreed to participate in this study. Among them, 35 wore the thigh and trunk devices for four full days. A total of five patients could not wear their accelerometer fully, and the data of these patients were excluded before the analyses. The mean age was 89.1 years (ranging 79–97 years), and 15 residents were men (43% of all residents). Grip strength was 21.3 ± 5.0 kg-force for men and 13.4 ± 4.5 kg-force for women (Table 1). No current smokers and four (11.4%) current alcohol drinkers were included. Patients had a mean of 6.2 comorbidities (range, 3–12), the most common of which were hypertension (68.6%), kidney diseases (62.9%), neurological diseases (54.3%), and cardiovascular diseases (51.4%).
Characteristics of patients (n = 35).

NA: not applicable; SD: standard deviation; HDS-R: Hasegawa dementia scale-revised; BMI: body mass index; ADL: activities of daily living.
Figure 1 shows the 24-h physical activity and behaviour. As older adults’ activities were limited in terms of LPA, their physical activities and behaviours were only SB (sitting and lying) or low-intensity physical activity (standing and stepping). During the night (9 PM–6 AM), participants sat approximately 8.7 min/h and laid approximately 47.8 min/h. During the daytime (6 AM–9 PM), participants moved (standing or stepping) approximately 9.7 min/h, laid for approximately 19.1 min/h, and sat approximately 31.3 min/r. Lying minutes/hour for the hours of 7 AM, 11 AM and 5 PM were shorter compared to other daytime hours, and the mean time was 6.8 min, which was significantly shorter than the mean lying time of other daytime hours (p-values < 0.001).

The 24-h physical activity and posture (n = 35).
Table 2 shows physical activity levels and postural patterns for all patients based on age (<90 years or ⩾90 years). Their mean ages were 84.1 ± 3.7 years (<90 years) and 93.0 ± 2.3 years (⩾90 years). The mean daily values for all participants were 1598.9 steps; a stepping time of 22.1 min; an upright time of 175.4 min (including standing and stepping time); and a sedentary time of 1263.6 min (21.1 h), including 550.9 min (9.2 h) of sitting and 712.7 min (11.9 h) of lying. Adults ⩾90 years of age walked a mean of 1109.1 steps/day and had a mean upright time of 167.3 min/day. Although residents aged <90 years were more active than those aged ⩾90 years, this difference was not significant.
Physical activity/posture in all patients according to age classification (n = 35).

SD: standard deviation.
Analysed using t-test.
Table 3 shows physical activity levels and postural patterns according to ADL level. Patients with full independence in ADLs had a mean age of 88.7 years (range: 80–97 years), mean grip strength of 21.4 kg-force (range: 13.7–28.2 kg-force), mean BMI of 22.5 kg/m2 (range: 16.3–26.8 kg/m2), and mean daily step count of 3587.6 (range: 1838–9964). Significant decreases in step count, number of sit-to-stand transitions, stepping time, and upright time were observed as ADL ability decreased (all p-values < 0.001). No increases in sitting time were observed as ADL ability decreased. The lying time significantly increased with low ADL (p = 0.03). With a low level of ADL, the grip strength and albumin level significantly decreased (p < 0.01 and 0.03, respectively). The number of comorbidities, age, sex, and BMI did not show a significant difference in each ADL level.
Physical activity/posture and ADL level (n = 35).
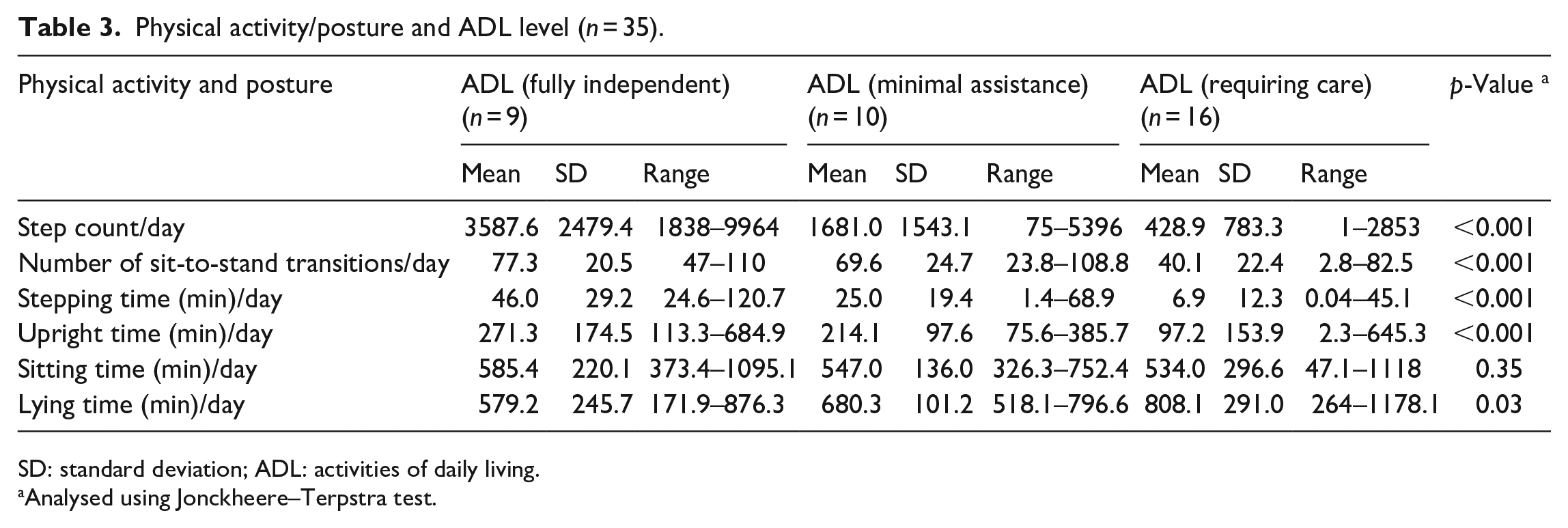
SD: standard deviation; ADL: activities of daily living.
Analysed using Jonckheere–Terpstra test.
Tables 4–7 shows that multivariate linear regression analyses for physical activity, including step count, number of sit-to-stand transitions, stepping time, and upright time, indicated significant positive relationships with the ADL level when adjusted by age and grip strength or age and albumin level (all p-values < 0.05). Lying time was positively associated with depression status (Spearman’s correlation = 0.33), although other comorbidities and number of comorbidities were not related (Spearman’s correlation < 0.3).
Multivariate linear regression analysis for step count/day.

Multivariate linear regression analysis for number of sit-to-stand transition/day.

Multivariate linear regression analysis for stepping time (min)/day.

Multivariate linear regression analysis for upright time (min)/day.

ADL level: activities of daily living level (classified by three levels); CI: confidence interval.
Discussion
Our findings revealed the physical activity and posture of older individuals with a mean of 6.2 comorbidities residing in assisted-living residences in Japan. In addition, we found that step count, number of sit-to-stand transitions, stepping time, and upright time decreased significantly as ADL ability decreased. Moreover, regarding comorbidities, depression status was related to lying time.
Our participants (mean age: 89.1 years) walked a mean of 1598.9 steps (range: 1–9964) per day, and people aged ⩾90 years walked a mean of 1109.1 steps. Similarly, a previous study on continuing care residents indicated that participants, with a mean age of 82.3 years, walked a median step count of 1906 steps (range: 38–12,636). 32 The reason for the lower step count in our study may be related to the older mean age of our participants (6.8 years older) relative to those in the study of Chan et al. 32
In addition, our study suggests that older adults exhibit an increase in lying time without an increase in sitting time in accordance with lower ADL ability. Another report suggested that physical activity of older adults decreased with functional limitation. 33 However, because posture, such as sitting or lying, in older adults was not assessed in detail in previous studies, it remains unclear whether posture (e.g. sitting or lying) in older adults is altered with a decline in ADL performance. Our findings showed that sitting time tended to be reduced with a decrease in ADL, although the relationship was not significant. SB generally includes sitting and lying; however, sitting may be considered a physical activity for older adults. Although lying time per day was positively related to comorbidities or the number of comorbidities, 9 there was no significant relationship between lying time and any comorbidities or the number of comorbidities except for depression status. Furthermore, a previous study 34 indicated that lower physical activity was associated with the risk of depression. This relationship may be explained by the association of lying time with depressive symptoms or other factors, such as the amount of time spent on interpersonal communication or hobbies, 35 because lying time depends on how much time participants have in their rooms and how they choose to spend it. These previous studies34,35 discussed the relationships between high intensity behaviour such as standing, running or sports. Meanwhile, our study showed an association between low-intensity behaviour such as lying time and depression status. This finding suggests that depression status is an important consideration for the care of older adults with lower physical activity levels and those who have been bedridden for a long time.
Furthermore, we examined the 24-h physical activity and behaviour. Few studies have reported a decrease in 24-h movement for older adults with decreased ADL and multiple comorbidities. One of these studies reported similar values to our results for nighttime activity, SB, and stepping time. 28 However, detailed information about chronic health problems and lying time were unclear. The bedridden posture may cause several and new health problems; this result may have important implications for the daily care of older adults. Notably, during the daytime (after 6 AM and before 9 PM), lying time decreased at 7 AM, 11 AM and 5 PM. These hours corresponded to the mealtimes for residents in our study (breakfast starts at 7:30–8:00 AM; lunch starts at 11:30 AM–12:00 PM; dinner starts at 4:30–5:30 PM). A similar trend was observed in each ADL level (Supplemental material file). This finding may indicate that regular eating behaviour induces physical activity or avoidance of excessive bedridden posture.
This study had some limitations. First, the sample size was small, which might have led to under-powered analyses. This may explain why we could not observe a difference in physical activity levels between residents aged <90 years and those aged ⩾90 years. Second, the step count assessment may not have been precise for older adults. A total of five patients presented with an average of 0–10 steps daily. Although ActivPAL is reportedly more accurate than other devices, 36 very short steps are difficult to count given the small degree of change in the axial gradient; thus, step counts may have been underestimated. Therefore, upright time may be a more reliable indicator of light physical activity than step count for older adults who walk with very short steps. Third, our statistical analyses using physical activity employed summarised measures from the device software. Another presentation method, a distributional presentation from the accelerometer data, may provide more sophisticated physical activity data. 37 Nonparametric functional regression models, such as kernel ridge regression using this distributional presentation, may show additional insights.
Conclusion
Data obtained in the present study provides a reference for physical activity and posture time in older adults residing in two assisted-living residences. Our study revealed that in older adults, physical activity was reduced, and lying time increased, as ADL decreased; this finding was similar to that of previous studies. In addition, our study found that sitting time tended to decrease with a decrease in ADL. Furthermore, lying time was associated with depression status. Our results emphasise the need for precise measurement of physical activity levels and ADL ability in this population, including assessments of upright time and sitting time. Further studies are required to determine the impact of physical activity and posture on disease-causing factors in older adults.
Supplemental Material
sj-docx-1-smo-10.1177_20503121231220798 – Supplemental material for Accelerometer-measured physical activity and posture among older adults in assisted-living residences
Supplemental material, sj-docx-1-smo-10.1177_20503121231220798 for Accelerometer-measured physical activity and posture among older adults in assisted-living residences by Tsunetaka Kijima, Kenju Akai, Shiho Amagasa, Shigeru Inoue, Shingo Yamagata, Yutaka Ishibashi, Hironori Tsukihashi and Tetsuya Makiishi in SAGE Open Medicine
Footnotes
Acknowledgements
We thank all study participants and staff of the assisted-living residences for their contributions to recruitment and data collection.
Data availability statement
The datasets used for the current study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a JSPS KAKENHI (Grant Number JP19K16950). The Department of General Medicine, Faculty of Medicine, Shimane University, is an endowment department, supported by Oda City.
Ethics approval
Ethical approval for this study was obtained from Shimane University Institutional Committee (APPROVAL NUMBER/20200217-3).
Informed consent
Written informed consent was obtained from each patient and/or his or her family before the study.
Trial registration
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.