
Abstract
This study aimed to examine the association between different contextual factors (e.g., facility size, rurality, and perceived needs) and the adoption of a policy or strategy related to opioid prescribing practices in healthcare settings. Cross-sectional survey data was collected from a convenience sample of physicians (N = 68). Logistic regression models were used to examine the effects of contextual factors on the dependent variables. Less than half reported having a policy restricting opioid prescribing practices, and 81% reported having one or more strategies for the safe use of chronic opioid therapy. After adjusting for other contextual factors, small practice size was positively associated with having a policy restricting opioid prescribing practices. This exploratory study provides insights for further investigation of how various contextual factors can influence policy adoption in different healthcare settings and practices to address major public health threats.
The US Department of Health and Human Services has declared the opioid crisis as an ongoing public health emergency (US Department of Health & Human Services, 2022). The medical use of opioids as pain relievers starting in the late 1990s has been associated with steadily accelerating overuse statistics and other negative sequela over the past 20 years (Kolodny et al., 2015; Scholl et al., 2019). Over 10 million Americans misused prescription opioids and 1.6 million Americans were estimated to have opioid use disorder (OUD) in 2019 (US Department of Health and Human Services, 2022). Increased prescribing of opioids in healthcare settings has been suggested as the major contributor to the beginning of the first opioid wave epidemic nationwide (Centers for Disease Control and Prevention [CDC], 2021). While prescribing rates by primary care providers have declined in the past few years prior to the COVID-19 pandemic, analyses suggest that high-risk prescribing behaviors (e.g., daily potency and prescription duration) persisted (Zhu et al., 2019; Zuger, 2019). Increased opioid prescribing was observed during the COVID-19 pandemic (Lee et al., 2021) and potentially contributed to increased street prices of prescription opioids (Mutter et al., 2022).
In light of the now-recognized national opioid crisis and potential risks associated with prescription opioids, strategies for OUD prevention have received increasing attention from researchers, practitioners, and policymakers. Suggested strategies related to prescription opioids include, but are not limited to, patient education (Syed et al., 2018), establishing an appropriate pain expectation in patients (Holman et al., 2014; Syed et al., 2018), provider education (Gorfinkel et al., 2019), prescription monitoring (Hawk et al., 2018), and opioid prescribing guidelines (Howard et al., 2018). A systematic literature review of the types and efficacy of strategies in an orthopedic surgeon’s practice setting identified multiple patient- and provider-focused interventions and concluded that prescribing guidelines were the most universally effective strategy (Lovecchio et al., 2019). The authors of the review also noted that this field of research is still in its infancy (Lovecchio et al., 2019), and limited evidence exists regarding the factors or mechanisms related to the processes and outcomes of implementing these strategies.
Implementation of these strategies involves many moving parts in a healthcare setting, which include the strategy itself, individuals involved in the implementation process and outcomes, and the implementation context (Chaudoir et al., 2013). Other than the strategy itself, extant literature have indicated the importance of providers in implementing the changes in healthcare settings (Haffajee & French, 2019). For example, targeted naloxone distribution and medication-assisted treatments are listed under the CDC’s evidence-based strategies to reduce opioid overdose or prevent fatal effects from opioid overdose among people using opioids or those experiencing opioid dependence (CDC, 2018). Based on an electronic survey of 4225 clinicians, Jones and McCance-Katz suggested significant associations between medication-assisted treatment with buprenorphine and multiple clinicians’ characteristics (e.g., certified in addiction psychiatry) (Jones & McCance-Katz, 2019). A comprehensive review of providers’ awareness indicated the gap between support for naloxone distribution programs and actual prescribing of naloxone. Despite the support for the program, providers’ lack of confidence, knowledge, and awareness of naloxone laws served as risk factors for their willingness to prescribe naloxone (Okoro et al., 2018).
Contextual factors for implementing a strategy or intervention in a healthcare setting include a broad scope of characteristics of settings and circumstances of implementation (Nilsen & Bernhardsson, 2019). This can include, but is not limited to, geographical location (e.g., rural or urban), resource availability, and the perceived magnitude of the issue (e.g., the seriousness of the OUD issue) in the local community or practice setting. Implementation of any changes in a healthcare setting can be costly, involve disruption of usual activities, and require additional staffing. Thus, smaller facilities or rural facilities, which are likely to lack resources, may have barriers associated with implementing a strategy or intervention. Jones and McCance-Katz found that clinicians practicing in a larger facility, such as a hospital or health system, were more likely to use medication-assisted therapy with buprenorphine than office-based solo practices (Jones & McCance-Katz, 2019). While limited studies exist about the effects of contextual factors on the adoption of strategies related to opioid prescribing in healthcare settings (Alexandridis et al., 2019), evidence have suggested an association between contextual factor(s) and the adoption of innovations in a healthcare setting. For example, Towne and his colleagues found that small practice size was a potential barrier to the adoption of electronic health records (EHR) in a residential care facility (Towne et al., 2016). Towne and his colleagues noted conflicting rates of EHR adoption in residential care settings in rural areas throughout Texas versus the United States (Towne et al., 2016). This observation can be related to the variation in the magnitude of a problem or need, which contributes to the local support and regulations regarding a policy or strategy implementation.
The objectives of this exploratory study were to examine the association between different contextual factors and the adoption of a policy or strategy related to opioid prescribing practices in healthcare settings. It was hypothesized that small facility size and rurality would be barriers to implementing an opioid-prescribing policy or strategy in a healthcare setting, but the provider’s perceived local needs for safe opioid-prescribing strategies would be a facilitator. In addition, this study examined and compared opioid prescribing of physicians with and without a policy or strategy regarding opioid prescribing practices in their healthcare settings. This study can provide insights into: (1) how different contextual factors of the healthcare setting are associated with the institutional adoption of a strategy related to opioid prescribing practices, and (2) the association of the strategy adoption and physicians’ opioid prescribing patterns.
Materials and Methods
Data Source
This study used cross-sectional, anonymous online survey data that was collected from a convenience sample of physicians. Participants were recruited through multiple channels (e.g., primary care-based medical groups, a professional medical organization, and medical education conferences) between December 2017 and February 2019. The survey was collected from 74 physicians who were currently practicing in Texas or Minnesota at the time of assessment. Of 74 responses, 68 responses were collected between December 2017 and February 2018. An additional 6 responses were collected during January and February 2019 after a medical education conference. Over 16% (n = 10 out of 61 with ZIP Code data available) of the respondents practiced in Minnesota, and the remainder practiced in Texas (n = 51). Based on the available ZIP Code and description of practice setting (e.g., size and existing policy or strategy related to opioid use), six survey responses that might represent the same practice locations were excluded. Therefore, this study included 68 physician responses. The current study was reviewed and approved by the Texas A&M Institutional Review Board (IRB 2018-0404D).
Measures
The primary outcome variables of interest were whether physicians’ healthcare system or practice had any policy restricting opioid prescribing and strategies to support safe initiation, monitoring, and discontinuation of chronic opioid therapy. The primary outcome variables were dichotomous variables with no policy or strategy as the referent category (=0). For those who reported having any policy or strategy related to chronic opioid therapy, participants were further asked about the type of strategy implemented in their practice (e.g., documentation of patient medical records, patient prescriber agreements, Prescription Drug Monitoring Program (PDMP), patient education and communication, drug testing, pill counts, mobile health technology for monitoring opioid use and misuse, provider education, and others). For those who reported not having any strategy to support safe chronic opioid therapy, participants were asked about barriers (e.g., not a priority, lack of staff, provider or institutional resistance to change, patient resistance to change, difficulty using the PDMP, and others) that prevented their practice from implementing a strategy.
Contextual factors considered in this study were the size of the practice setting, geographic location, and providers’ perceived local needs. Participants were asked to describe the size of the practice setting based on the number of physicians in their practice. Valid responses for the question were solo (1 physician, n = 3), small (2–5 physicians, n = 11), medium (6–29 physicians, n = 7), and large (30 or more physicians, n = 36). The first three response categories (i.e., solo, small, and medium) were merged due to low frequencies. Participants were also asked to describe the type of geographic area they practice in. The valid responses for the question were major urban area (n = 30), suburban area (n = 21), small town (n = 4), and rural area (n = 2). The last three response categories (i.e., suburban, small town, and rural area) were merged due to low frequencies. Provider’s perceived local needs for policy and strategies to support safe opioid prescribing practices were examined using the following question: “Are safe opioid prescribing practices an issue in your community or practice setting?” The provider’s perceived local need was a dichotomous variable with no issue as the referent category (=0).
The survey also asked physicians about their age ranges, sex, race, ethnicity, practice duration, and the number of outpatient Schedule II, III, and IV opioid prescriptions written per month over the past 3 months. Response categories with small frequencies were merged, such that age, race, and practice duration were dichotomized with age younger than 55 years old, non-White, or practice duration of less than 16 years as the referent category (=0). Regarding the questions about the number of Schedule II, III, and IV opioid prescriptions written to outpatients per month over the past 3 months, the valid responses were: none, 1–5, 6–10, 11–15, 16–25, and 26 or more per month. Two dichotomized variables were generated for each question about Schedule II, III, and IV opioid prescriptions. The first dichotomized responses were used with none as the referent category (=0). The second dichotomized responses were used with 1–5 per month as the referent category (=0) and 6 or more per month as an alternative response.
Analyses
Characteristics of the study participants and their practice setting, as well as policy and strategies related to opioid prescribing in the practice settings, were described using frequencies and percentages. Logistic regression was performed to examine bivariate associations between the adoption of policy or strategies related to opioid prescribing and each contextual factor (e.g., size, location, and need). Next, multivariable logistic regression was used to examine the association between the contextual factors and policy or strategy adoption. Separate regression models were performed to predict the implementation of a policy restricting opioid prescribing, any strategies supporting the safe use of chronic opioid therapy, and each support strategy. Last, descriptive assessments (e.g., frequencies and bar graphs) and logistic regression were used to examine bivariate associations between prescribing any outpatient Schedule II opioids and having a policy restricting opioid prescribing or strategies supporting the safe use of opioid therapy. Logistic regression was not repeated for the Schedule III and IV opioids because all or most participants reported prescribing Schedule III and IV opioids. Instead, additional logistic regression was performed after excluding those who prescribed ‘none’ to examine the bivariate association between prescribing a few (i.e., 1–5) versus more (6 or more) opioid prescriptions and having a policy or strategies related to opioid prescribing practices. Separate regression models were performed to predict Schedule II, III, and IV opioids. All statistical analyses were performed using SAS 9.4, and a significance level (i.e., rate of false positive) of .05 was used.
Results
Study Sample Description
Study Sample Description
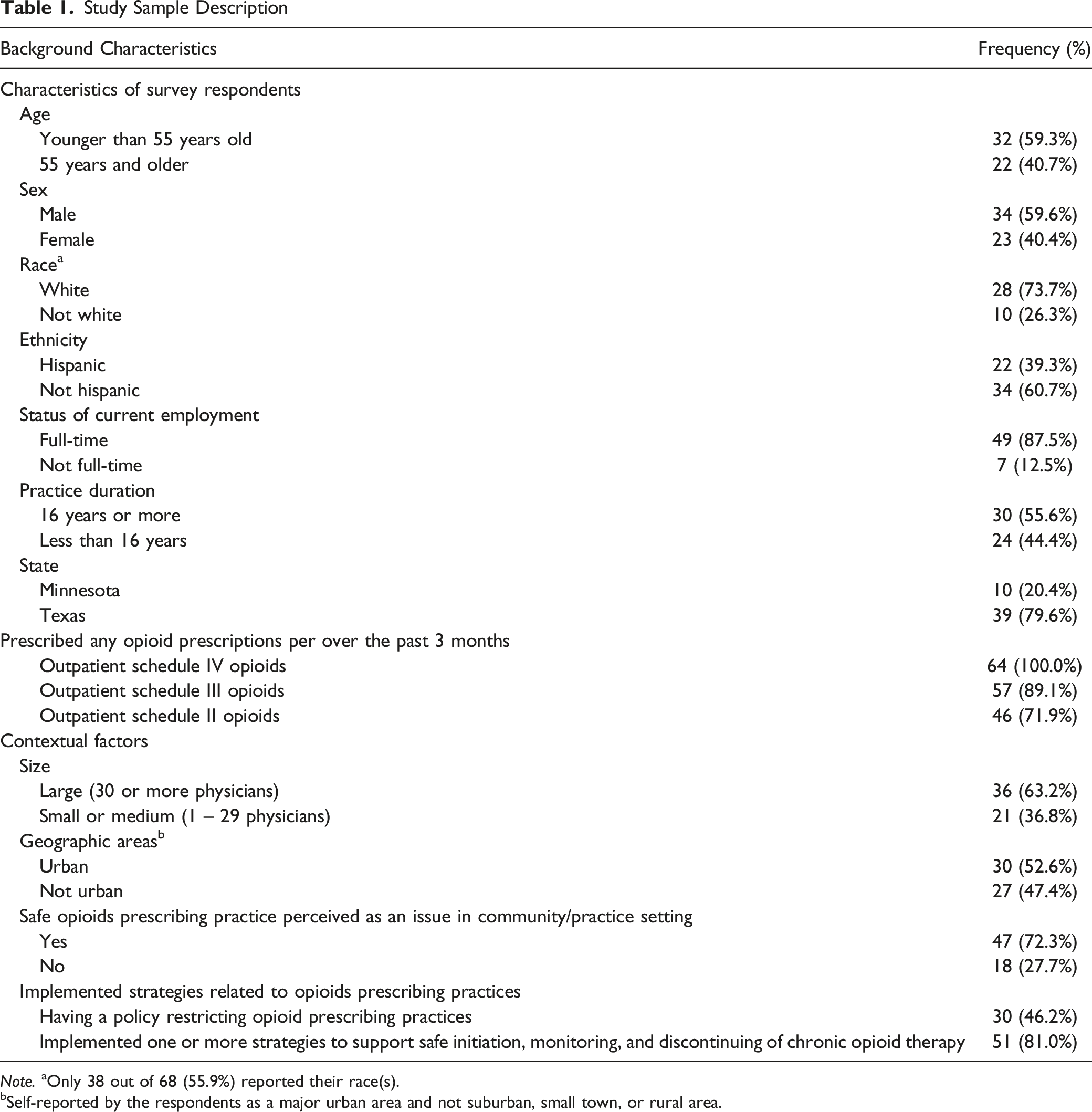
Note. aOnly 38 out of 68 (55.9%) reported their race(s).
bSelf-reported by the respondents as a major urban area and not suburban, small town, or rural area.
Strategies to Support Safe Chronic Opioid Therapy
Strategies Implemented to Support Safe Initiation, Monitoring, and Discontinuing of Chronic Opioid Therapy
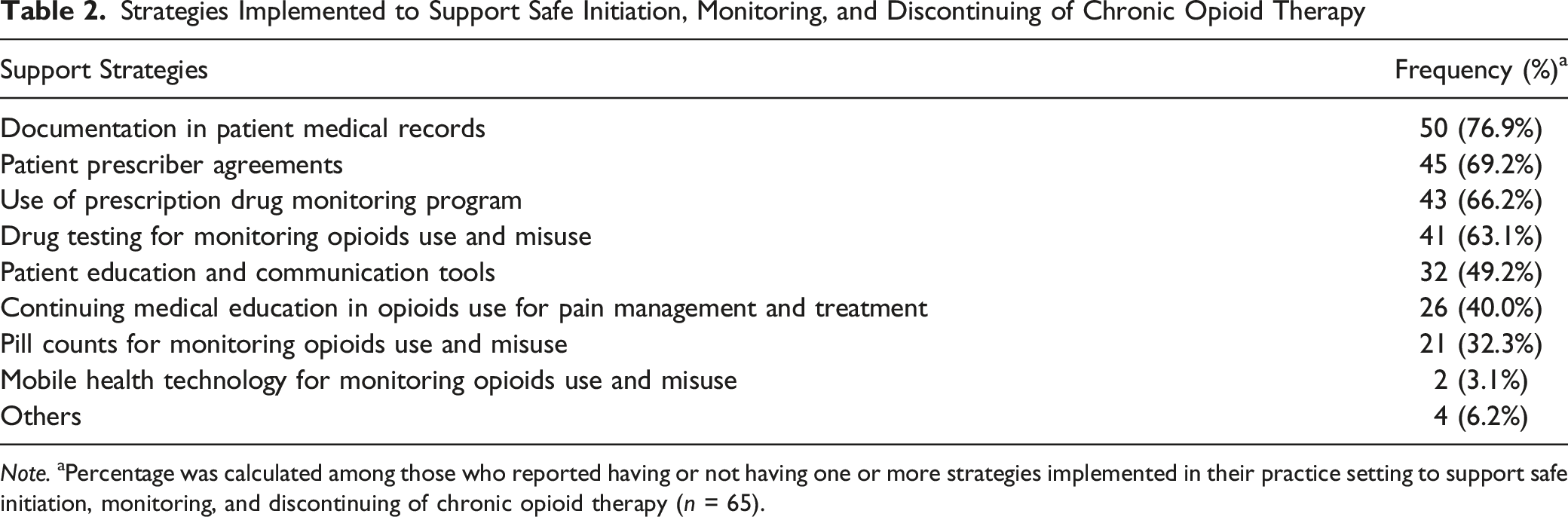
Note. aPercentage was calculated among those who reported having or not having one or more strategies implemented in their practice setting to support safe initiation, monitoring, and discontinuing of chronic opioid therapy (n = 65).
Among the physicians whose practice setting did not implement any support strategies for chronic opioid therapy, reported barriers included the issue not being a priority (45.5%), lack of support staff (45.5%), patient’s resistance to change (45.5%), other providers or institutional resistance to changes (27.3%), and difficulty with enrolling or accessing the PDMP (9.1%).
Contextual Factors
Unadjusted and Adjusted Odds Ratio Between the Contextual Factors and Implementation of Opioid Restricting Policy and Safe Chronic Opioid Therapy Support Strategies
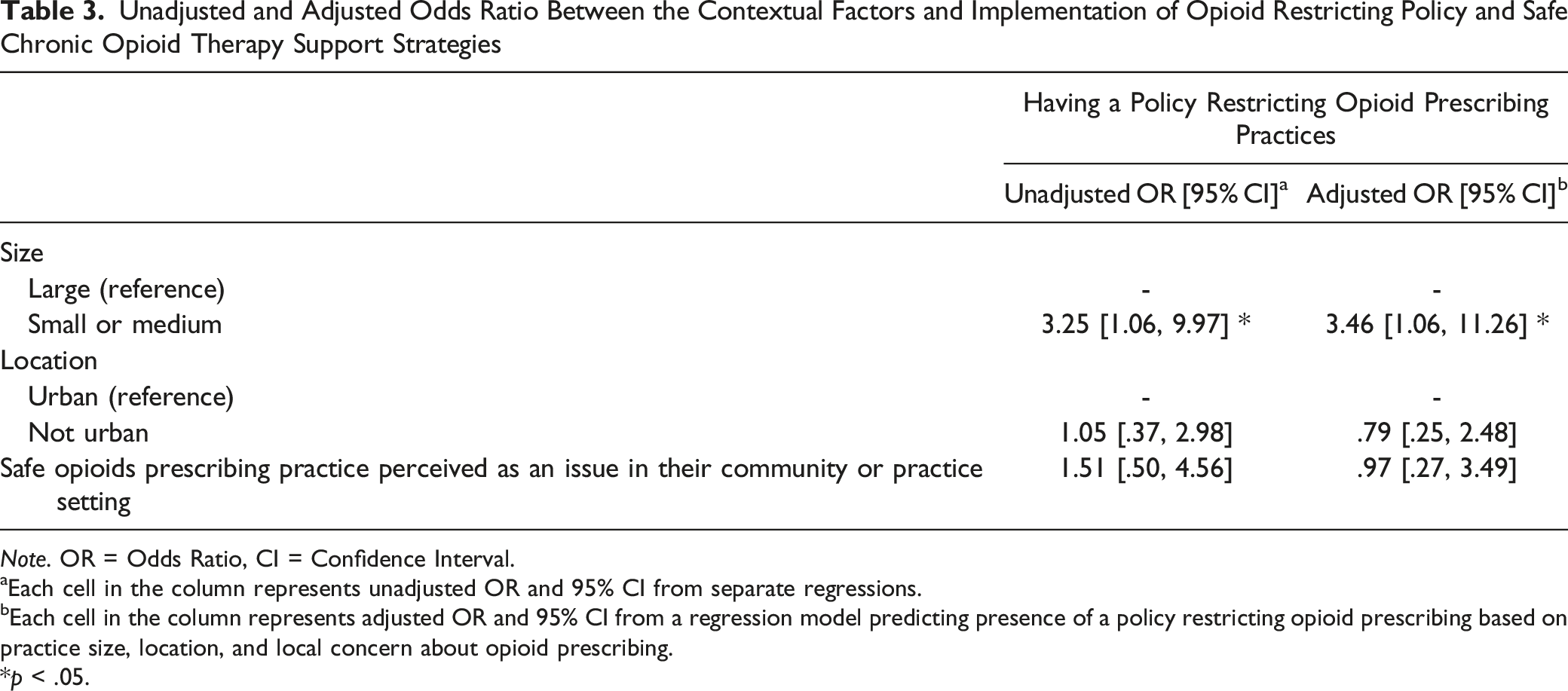
Note. OR = Odds Ratio, CI = Confidence Interval.
aEach cell in the column represents unadjusted OR and 95% CI from separate regressions.
bEach cell in the column represents adjusted OR and 95% CI from a regression model predicting presence of a policy restricting opioid prescribing based on practice size, location, and local concern about opioid prescribing.
*p < .05.
Strategies and Opioid Prescribing Practices
No statistically significant associations were observed between opioid prescribing practices and having a policy restricting opioid prescribing or a strategy for supporting safe prescribing of chronic opioid therapy (p > .05). Physicians who had a policy restricting opioid prescribing were less likely to write outpatient Schedule II opioid prescriptions than physicians who did not have such a policy (odds ratio (OR) = .36, 95% confidence interval (CI) = [.12, 1.03], p = .052), but with marginal statistical significance. Physicians in a practice setting that implemented drug testing for monitoring opioid use and misuse wrote more outpatient Schedule IV opioid prescriptions than physicians in a practice setting that did not implement the strategy (OR = 3.64, 95% CI = [1.11, 11.94], p = .033). No specific support strategies had a statistically significant association with physicians’ opioid prescribing practices (p > .05).
A closer look at the data showed a U-shaped (bimodal) distribution of monthly number of outpatient Schedule II and IV opioid prescriptions written. For example, over the last 3 months, 18 (28.1%) physicians reported not prescribing any Schedule II opioid prescriptions; 21 (32.8%) reported prescribing 1–5 prescriptions per months; 6 (9.4%) reported prescribing 6–10 prescriptions per month; 5 (7.8%) reported prescribing 11–15 prescriptions per month; 3 (4.8%) reported 16–25 prescriptions per month; and 11 (17.2%) reported prescribing more than 25 prescriptions per month. The bimodality indicates different patterns of opioid prescribing among physicians. The bimodality in the number of outpatient Schedule II and IV opioid prescriptions written was not observed or was less visible among physicians who practiced with a policy restricting opioid prescribing.
Discussion
The current study examined the association between the contextual factors of healthcare settings and having a policy restricting opioid prescribing or one or more strategies for supporting the safe use of chronic opioid therapy. A greater likelihood of having a policy or strategy related to opioid prescribing practices was hypothesized to be associated with large facility size, urban location, and having a greater issue with opioid prescribing in the community. In this exploratory study, only practice setting size was significantly associated with having a policy restricting opioid prescribing.
Contrary to expectations, physicians from a smaller practice (i.e., less than 30 physicians) were more likely to report having a policy restricting opioid prescribing than physicians from a large practice (i.e., 30 or more physicians). Bateman and Choudhry (2016) described a policy that restricts opioid prescriptions as a radical approach because restricting limits on opioid prescribing practices cannot account for all possible clinical situations and may increase burdens for both patients and healthcare providers. Despite its potential benefits, this approach has also been described as an extreme end of a pendulum swing that may have unintended consequences (e.g., uncontrolled pain) (Rieder, 2018). One of the most commonly discussed critiques of such an approach is its over-simplified nature which can limit individualized care in some clinical situations (Bateman & Choudhry, 2016). A larger practice setting is likely to cover broader specialty areas and provide care for more diverse conditions compared to a smaller practice setting. To handle the increased differentiation and complexity, a larger practice setting is more likely to have some complex, administrative procedures than a smaller practice setting (Pugh et al., 1968). Therefore, an over-simplified policy such as the restriction of opioid prescriptions may not be suitable or implemented easily in a larger practice setting. Furthermore, while the study was not performed in a healthcare setting, Bloodgood’s study illustrates that smaller and larger organizations have different motivations and rates for adopting organizational changes (Bloodgood, 2006). This finding also converges with a finding from a Dutch study that observed a systematically higher proportion of cancer patients receiving chronic high-dose opioid prescriptions in larger practices (Kalkman et al., 2023).
Over 80% of participating physicians reported having one or more strategies for supporting the safe use of chronic opioid therapy, with most of them having 4-to-7 different strategies implemented in their practices. The study data were collected primarily in late 2017 and early 2018, with a few responses in early 2019, and the observed rates may reflect the increased attention towards the opioid crisis over the past decade. Between 2008 and 2016, there have been some major increases in state-level policies related to opioid prescribing and addiction treatment policies (Haffajee & French, 2019). For example, compared to 2008, 13 more states recommended or mandated PDMP, 44 more states supported naloxone access and distribution programs, 35 more states provided Good Samaritan protection for individuals who respond to a drug overdose, and 10 more states implemented some laws that regulated pain management clinics in 2016 (Holman et al., 2014).
The descriptive analyses on physicians’ use of opioid prescriptions based on a policy restricting opioid prescribing practices indicated that having a policy restricting opioid prescribing might differentially influence physicians with different rates of opioid prescription use. An alternative explanation would be that the decision to implement a policy restricting opioid prescribing might depend on physicians’ opioid prescribing patterns. While the causality cannot be drawn from this study, this study finding highlights the important relationship between institutional policy and physicians’ prescribing behavior. While the association was only marginally significant, physicians who had a policy restricting opioid prescribing reported lower odds of writing outpatient Schedule II opioid prescriptions than physicians who did not have such a policy. The lack of statistical significance might be due to the small sample size such that the analysis might be underpowered.
Using drug testing for monitoring opioid use and misuse was positively associated with the likelihood of prescribing more Schedule IV opioids. A possible explanation for this observation might be that drug testing for monitoring opioid use and misuse was more likely to be implemented in a healthcare setting where physicians prescribed more opioids. Another possible explanation might be that physicians felt more comfortable with prescribing more opioid prescriptions with drug testing. It should also be noted that while there have been studies examining rates of using drug testing (Turner et al., 2014) and effects of aberrant drug test results on clinical decisions (e.g., whether to continue, change, or discontinue opioid therapy) (Morasco et al., 2019), limited studies have examined the effects of having drug testing itself on opioid prescribing behaviors. Further work is required to establish the relationship, and particularly causality, between the implemented strategies to support the safe use of opioid therapy and physicians’ opioid prescribing practices.
Limitation
This study has a number of limitations. First, the study used self-reported online survey data from a small, convenient sample that may not be widely generalizable. Therefore, the study findings must be interpreted with caution. For example, rurality was determined based on self-report rather than objectively assessible geographical criteria (e.g., population size). Despite the small sample size, the sample was collected from diverse sources (e.g., primary-care-based medical groups, a professional medical organization, and medical education conferences) and areas (e.g., Texas and Minnesota). Furthermore, additional information about the survey respondents (e.g., physician specialty) would provide better insights into their practice context. Second, the small sample size can limit the study’s statistical power and can potentially limit the study’s ability to detect a true effect, particularly for the statistically non-significant findings. For example, the retrospective power for predicting having a policy restricting opioid prescribing practices based on each examined factor using logistic regression was .49 (practice size), .05 (location), and .56 (local issue). Examination based on location had particularly low power due to the similar likelihood of having a policy/strategy between urban and non-urban areas. The majority of the non-urban category was from a suburban area (n = 21) with limited representation of small towns (n = 4) and rural areas (n = 2). Future examination of the geographic factor can benefit from expanding the representation of small-town and rural health care settings. Third, this study examined the presence of a strategy related to opioid prescribing practices and the associated barriers of not having a strategy. However, it should be noted that having a strategy does not equate to actively engaging in or maintaining that strategy. For example, despite the availability of PDMP, providers may not use it for many different reasons (e.g., technical difficulty accessing the tool). Fourth, the tested regression models were not comprehensive. While adopting a policy or strategy in a healthcare setting involves multiple factors related to the involved individuals, intervention, and environment, the regression models used in this study focused primarily on environmental factors. The rationale for the decision was two-fold. Unless it was a solo practice, contextual factors should have a greater impact on having a policy or strategy in a healthcare setting than characteristics of individual physicians. Also, the small sample size limited the number of variables that could be controlled in the model. The study’s comprehensiveness can also be further improved by accounting for different types of policies and strategies implemented in each setting, instead of using a broad definition of policy and strategy. Last, while this study focused on contextual factors of a practice setting, the sampling unit was at the physician-level. Therefore, six survey responses judged to represent the same practice locations were excluded from the analyses based on physicians’ ZIP Codes and practice setting descriptions (size and existing policy or strategy related to opioid use). This exclusion should help provide a unique presentation for each practice setting in the sample. The inclusion of the six survey responses did not influence the direction and statistical significance of the observed associations and had little influence on adjusted odds ratio (e.g., aOR for practice size, with 6 survey responses = 3.49 vs. aOR for practice size, without 6 survey responses = 3.46).
Conclusion
This study looked at the association between the adoption of strategies for safe opioid prescribing practices and the size and rurality of care settings and perceived problems of opioid prescribing. While the study is exploratory, the present study adds to a growing body of literature about strategies and policies to address the opioid crisis. Although the current study is based on a small sample of participants at one point in time, the findings suggest that practice size was associated with having a policy restricting opioid prescribing. Further investigation of this association with other covariates (e.g., specialties) is warranted. More comprehensive models that involve multi-level factors are needed to understand better the decision and process of adapting policies and strategies related to clinical practices (e.g., opioid prescribing) at individual provider and institutional levels. Furthermore, different opioid prescribing patterns among physicians in practices with and without a policy restricting opioids suggest questions in need of further investigation as well.
Footnotes
Acknowledgments
We thank all physicians who participated in this study and our clinical and academic partners who helped with the recruitment.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.