
Abstract
Pediatric Health Related Quality of Life (HRQoL) among childhood cancer survivors (CCS) measures the impact of illness and treatment from the patient’s perspective. However, parents often serve as proxies when the child cannot provide information directly. Studies of agreement between parents’ proxy assessment and child’s self-report have shown discrepancies. Understanding the reasons for discrepancies is under studied. Thus, this study examined the agreement of 160 parent-CCS dyads on the child’s domains of HRQoL by mean difference, intra-class correlation coefficients, and Bland-Altman plots. Differences in agreement were assessed by patients’ age, ethnicity, and whether or not they lived with their parents. Overall, the Physical Function Score showed good agreement between parents and CCS (ICC = 0.62), while the Social Function Score had fair agreement (ICC = 0.39). CCS were more likely to rate their Social Function Score higher than their parent. The lowest agreement for the Social Function Score was found for 18–20 years old’s (ICC = .254) versus younger or older CCS, and among non-Hispanic whites (ICC = 0.301) versus Hispanics. Differences in agreement varied by patient age and ethnicity, suggesting that other factors, including emotional, familial, and cultural factors, may influence parental awareness of CCS HRQoL.
Introduction
Given the improvement in cancer treatment and subsequent survival, there has been an increased focus on health-related quality of life (HRQoL), which refers to the patient’s perception of their physical and mental health (Centers for Disease Control Prevention, 2000). Since 1975, the annual childhood (age 0–19) cancer rate has increased by 0.6–0.7%, while the 5-year survival rate for childhood cancer increased from 62% to about 84% (American Cancer Society, 2021). As a result, the number of childhood cancer survivors (CCS) increased from 70,868 to 500,000 (Howlader et al., 2015; Dijk-Lokkart et al., 2019). CCS experience adverse effects from cancer and treatment, such as worse overall health, more mental health issues, and more activity limitations compared to their healthy peers and siblings (Eilertsen et al., 2011; Hudson et al., 2003). Improvement in HRQoL is an important goal of health care (Eiser & Varni, 2013). Parents often make health decisions as a proxy for their children (Varni et al., 2007), and they may be asked to report on their child’s condition (Anderson et al., 2020). Therefore, understanding the agreement between CCS and their parents regarding the child’s HRQoL is important in assessing the extent and accuracy of the parent’s knowledge of their child’s condition (in comparison to the child’s viewpoint).
Previous studies indicate CCS rate themselves higher in HRQoL than do their parents (Parsons et al., 1999, 2012; Russell et al., 2006; Speyer et al., 2009), and other studies indicate parents of CCS rate their child’s HRQoL lower than healthy children (Russell et al., 2006; Theunissen et al., 1998). Agreement varies by QOL domain (Eiser & Morse, 2001), with some studies reporting higher agreement found for physical aspects of health compared to emotional or social aspects (Fluchel et al., 2008; Yeh et al., 2005), and other studies reporting contrary conclusions (Czyzewski et al., 1994; Theunissen et al., 1998).
Disagreement between parent and child reporting may occur for different reasons. Parents may know more about their child’s health information than the child does, or parents may report more behavioral symptoms, while children may report more subjective symptoms (Edelbrock et al., 1986). Disagreement may also be related to the child’s age or degree of relationship with their parent (Seiffge-Krenke & Kollmar, 1998), or it may occur due to language and cultural barriers between foreign born Hispanic parents and their US born children (González et al., 2010). However, both the parent and child points of view may be important because they provide clinically relevant information which may impact clinical decision making (Eiser & Varni, 2013; Pickard & Knight, 2005). We analyzed agreement between CCS and their parents with the following objectives: (1) to assess the agreement of responses within parent-child dyads to questions regarding health-related quality of life; and (2) to determine if agreement within dyads is associated with age of CCS, parent ethnicity, and whether CCS lives with their parent.
Methods
Source of Subjects
CCS and their parents were from the ‘Project Forward Pilot Study’ which has been previously described (Hamilton et al., 2019; Milam et al., 2015). Cancer patients were identified from the Surveillance, Epidemiology, and End Results (SEER) Cancer Registry for Los Angeles County, if they were diagnosed with cancer at age ≤18 years between 2000–2007 at Children’s Hospital Los Angeles (CHLA) or Miller Children’s Hospital, Long Beach. However, at the time survey assessment for this study in 2009, CCS were between the ages of 14–25 years and were, on average, 7 years past their date of diagnosis.
After approval from the USC, CHLA, Miller’s Hospital, the California Committee for the Protection of Human Subjects Institutional Review Boards, and the California Cancer Registry, a courtesy letter was sent to physicians to determine if there was any reason not to contact the CCS (no objections received). Then a survey (and postage paid return envelope) was mailed directly to CCS 18+ and permission was sought from them to contact their parents to mail them a similar survey to complete. For CCS <18 years of age, parents were contacted first to obtain consent to contact the CCS who was a minor, and the survey for the parents was also included in the mailing. Extensive follow-up methods, including phone calls, second mailings of materials, postcard reminders, and personal visits, were used to increase response from both CCS and their parents. All respondents received a $20 gift card and entry into a $300 lottery. Among 470 eligible CCS, 235 (50%) CCS and 173 (37%) parents participated. This analysis is based on the 160 dyads (34%) where both the parent and the child from the same family participated. Reasons for non-participation included refusal by either the survivors, parents, or lost follow-up (i.e., invalid contact information) (Hamilton et al., 2019). Response to the CCS survey was higher for women and those from higher socioeconomic areas. Response to the parents’ survey was higher for parents of younger survivors (Hamilton et al., 2019).
Variables
Both the parent and CCS assessed the child’s health status using the Pediatric Quality of Life Inventory (PedsQL) using versions appropriate to the child’s age. The PedsQL is a standardized instrument that assesses patients’ and parents’ perceptions of HRQoL in pediatric cancer patients (Varni et al., 2002). The 23-item PedsQLTM 4.0 Generic Core Scales were scored from 0 (lowest health-related quality of life) to 100 (highest health-related quality of life) scale. PedsQL is reliable (α = 0.88 child self-report; α = 0.93 parent proxy-report) and valid (Varni et al., 2002). The minimum clinically meaningful difference (MCID) is 4.5 points (Varni et al., 2003).
Demographic and Clinical Characteristics of Child-Parent Dyads (n = 160)
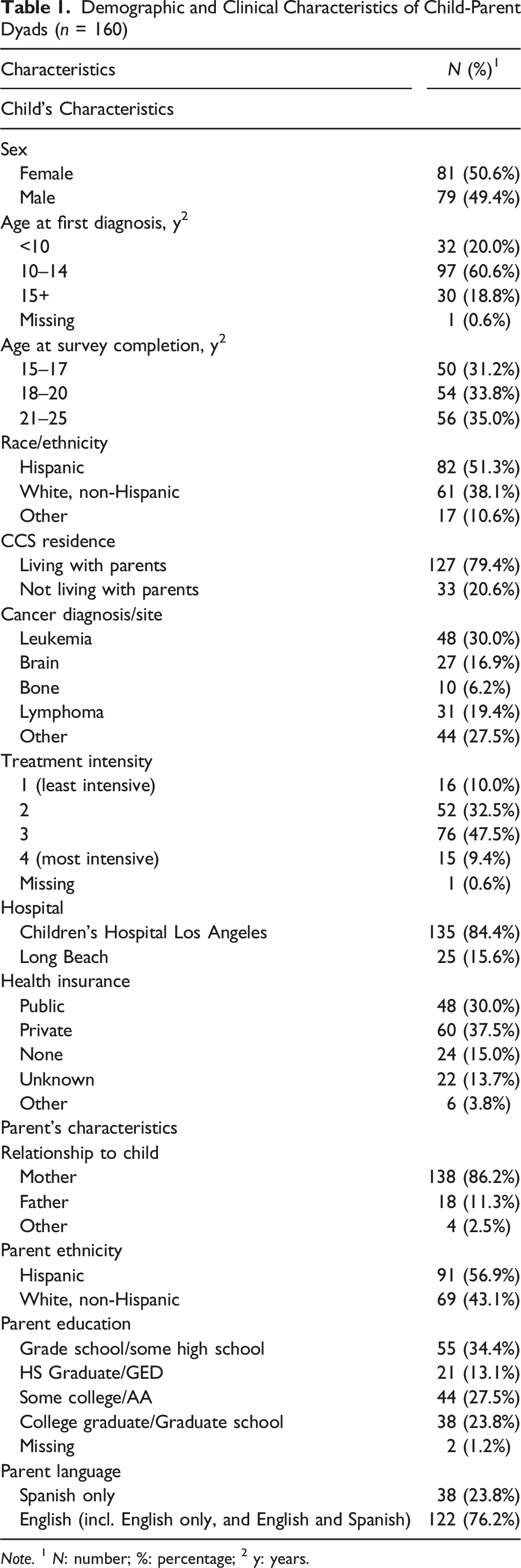
Note. 1 N: number; %: percentage; 2 y: years.
Statistical Analysis
For the PedsQL, a continuous variable, we calculated the intraclass correlation coefficient (ICC) to assess the magnitude of agreement of the child’s HRQoL between parent and child (Eiser & Morse, 2001; McGraw & Wong, 1996; Theunissen et al., 1998). The ICC was calculated from a two-way mixed effect model where raters (parent/child) were considered as fixed effects and subjects were treated as random effects. ICCs <0.40 were considered poor to fair agreement, 0.41 to 0.60 were considered moderate agreement, 0.61 to 0.80 were considered good agreement, and 0.81 to 1.00 were considered excellent agreement (Bartko, 1966). The ICC analysis was conducted for the total sample and stratified by child age groups, parent ethnicity, and whether CCS were living with parents. These variables were selected because they were potentially related to agreement between the parent and child (e.g., parents may be more aware of HRQoL of younger CCS or those living at home) and due to interest in identifying subgroups where agreement between the parent and child may differ (e.g., by ethnicity).
We used the Bland–Altman plot to show the differences of PedsQL score between dyads (parent score-child score) against the averages of dyads ((parent score + child score)/2). A linear regression line of the rater differences against the rater average was used to detect potential proportional bias (Giavarina, 2015). We used SPSS Version 22.0 to calculate ICC’s and MedCalc software to draw Bland-Altman plots. All other statistical analyses used SAS 9.4 version for Windows.
Results
The 160 CCS included in the dyads were evenly divided by gender, 60.6% were 10–14 years old at diagnosis, and 30% were diagnosed with leukemia (Table 1). Over half of parents and CCS self-reported their ethnicity as Hispanic (51.3% of CCS and 56.9% of parents) and nearly 80% of CCS lived with parents. The majority of parents who completed the survey were mothers (86.2%). Over a third (34.4%) of parents completed grade school or some high school, 23.8% completed more than college graduate degree, and 23.8% only spoke Spanish.
Agreement on the PedsQL Score
Mean PedsQL Scores
The mean scores were higher when rated by CCS than the parent for the Total Scale, Physical Functioning, Emotional Functioning and Social Functioning Scores, while CCS rated scores were lower than the parent’s for the School Functioning Score (Supplemental Table 1). For the Social Functioning Score, CCS rated themselves statistically significantly higher than their parents did (p = 0.005); the absolute mean difference was 5.02, which was larger than the minimum clinically meaningful difference (MCID = 4.5 points) (Varni et al., 2003). Domains for which a significant difference was not found included Physical, Emotional, and School Functioning. Additionally, Supplemental Table 2 demonstrates the kappa value and range for each question of the PedsQL.
ICC
Most domains of the PedsQL in the total sample showed moderate agreement (0.41 < ICC <0.60; Supplemental Table 3). The Physical Function Score showed good agreement (ICC = 0.62), and the Social Function Score had fair agreement (ICC = 0.40). After stratification by CCS’s age at survey completion, the ICC was highest (ICC = 0.67) for CCS aged 21–25 years old at survey completion for the Physical Functioning Scale, and was lowest (ICC = 0.25) for the Social Function Scale for CCS aged 18–20. In addition, when we stratified by parent Hispanic ethnicity, the ICC was highest (ICC = 0.71) for non-Hispanic dyads for the Physical Functioning Scale, and it was also lowest (ICC = 0.30) for non-Hispanic dyads for the Social Functioning Scale (Supplemental Table 4). Generally, ICCs for most of the domains of the PedsQL were moderate for Hispanic dyads (0.44–0.58). When we stratified on whether CCS lived with parents, we found that in general dyads in which CCS lived with parent had lower agreement (Supplemental Table 5). Dyads in which CCS did not live with parents had better agreement for the Physical (ICC = 0.78) and Emotional Functioning Scale (ICC = 0.60).
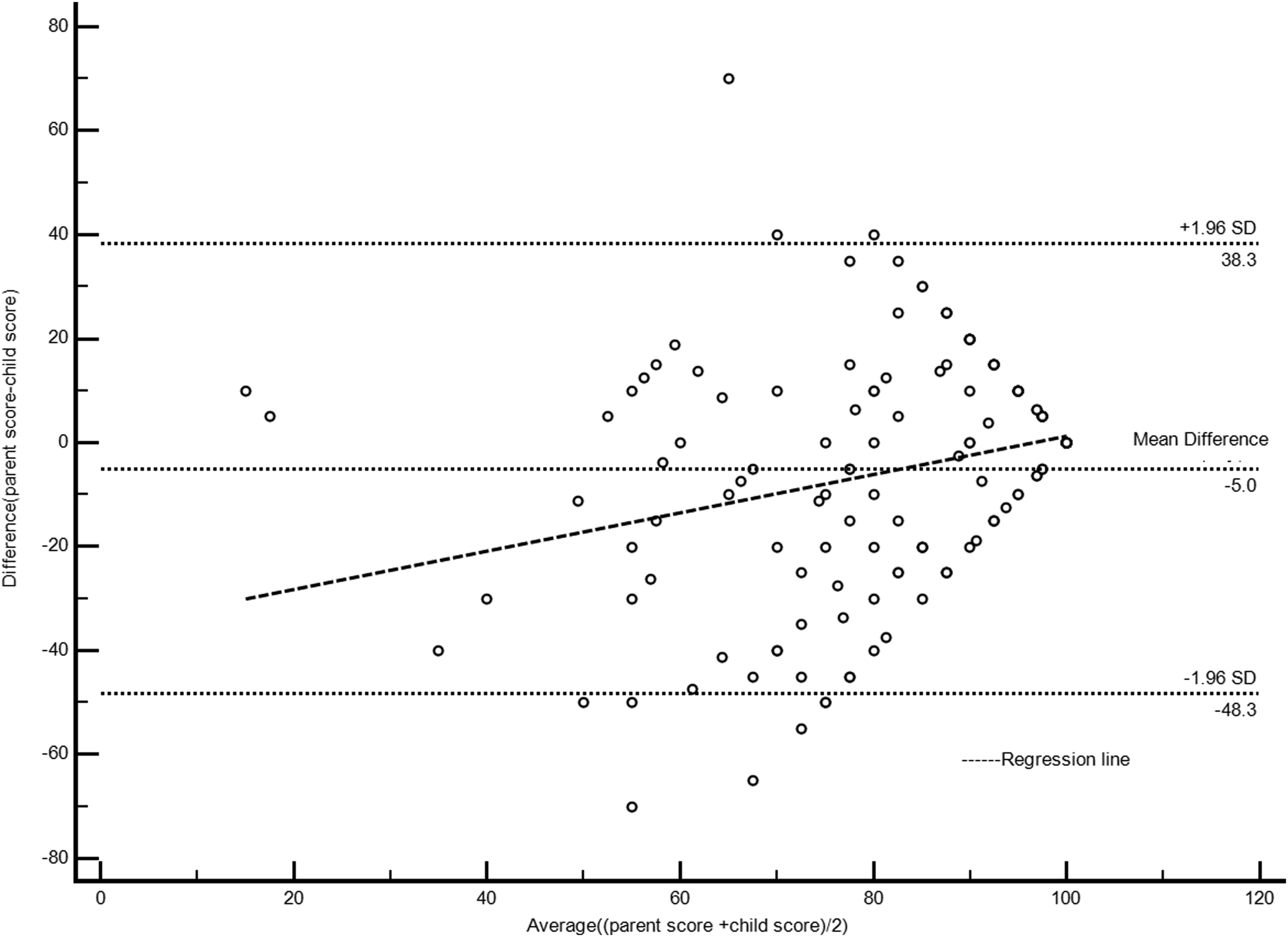
Bland-Altman Plots of PedsQL
Bland-Altman plots displaying the parent-CCS averaged score versus the parent-child difference were used to determine if parent-child differences in ratings were related to the magnitude of ratings. The mean difference for PedsQL total score was −1.4, which was not statistically significant from 0 (p = 0.30) (Figure 1). Consistent with the comparison of means and ICC scores, the Bland-Altman plots for the PedsQL™ Social Function Score (Figure 2) revealed a significant mean difference of −5.02 (bias) (p = 0.005), indicating relatively poor agreement between CCS and parent reports. The plots for the other function scores (Physical, School, and Emotional) all had more negative outliers than positive outliers, indicating that more parents rated CCS health-related quality of life lower compared to ratings by CCS (than vice versa; figures not shown). We did not see any systematic association of magnitude with difference in any plot. The only significant positive linear regression line (p = 0.0003) for Social Functioning Score (Fig. 2) indicated that as the parent-child averaged score increased, the negative parent-child differences became smaller, despite CCS consistently rating themselves higher than their parents did; suggesting there might be proportional bias for this score. Bland–Altman Plot of PedsQL Total Score Including Regression Line Bland–Altman Plot of PedsQL Social Functioning Score Including Regression Line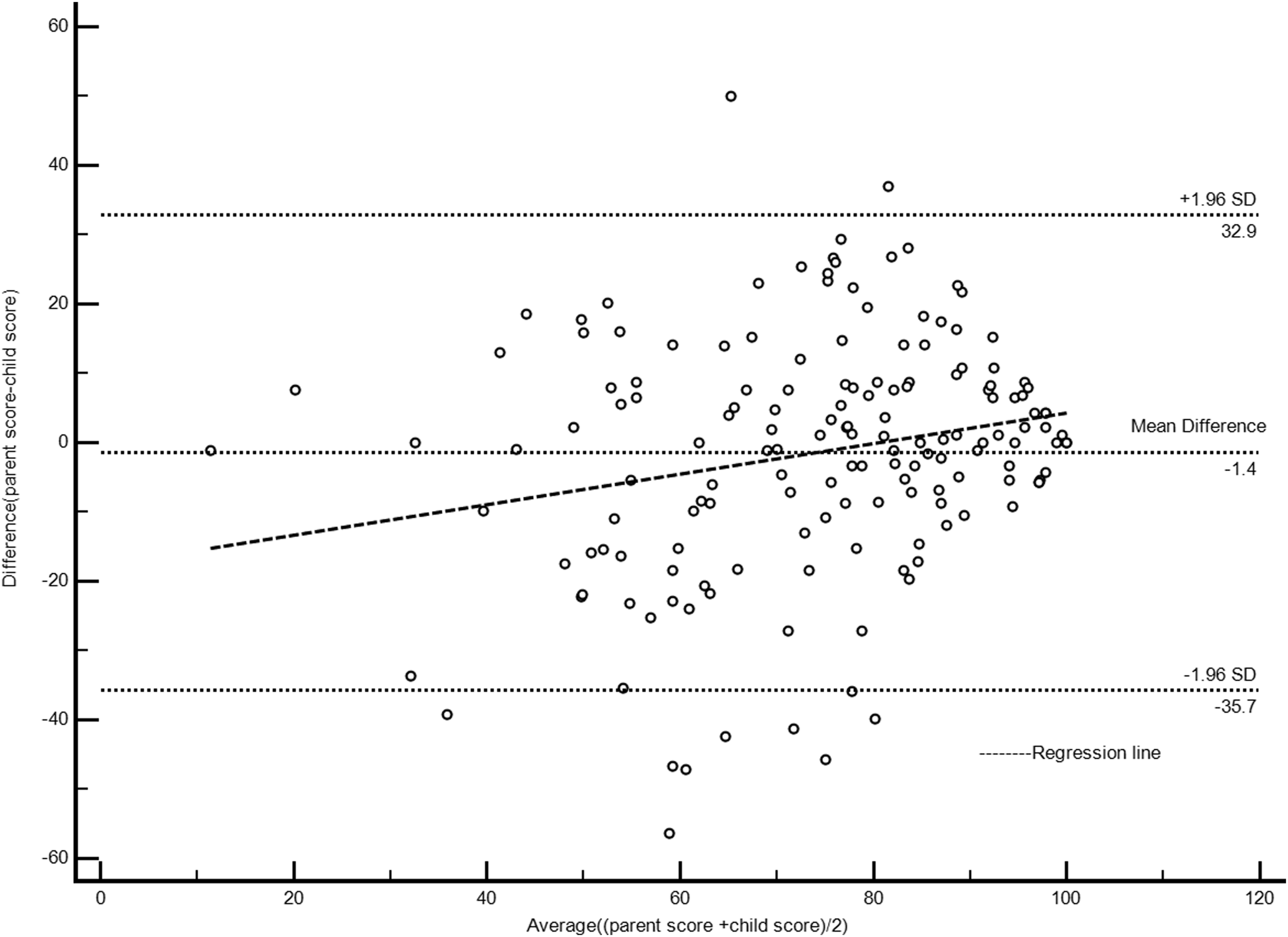
Discussion
This study, with 160 CCS-parent dyads, is one of the largest studies to compare parent and child differences in assessment of child’s HRQoL among CCS. Similar studies have been based on sample sizes which ranged from 27-95 dyads (Fluchel et al., 2008; Levi & Drotar, 1999; Parsons et al., 1999; Speyer et al., 2009; Yeh et al., 2005). Our sample also included a large representation of Hispanic subjects (51.3% vs. 17.4% in the US population) and found different levels of agreement by CCS age, parent ethnicity, and whether CCS lived with parents. In comparison to previous studies that analyzed agreement of responses between child and their parents regarding HRQoL, we observed higher mean scores for both parent and CCS across all domains. For instance, compared to a study that examined HRQoL among older children and adolescents with a variety of chronic pain conditions which found a Total score 54.4 (based on child reports) and 50.1 (based on parent reports) (Vetter et al., 2012), CCS and parents in our study reported a higher Total Scale score (mean scores of 74.85 and 73.41, respectively), which may be due to the 7 year average time since diagnosis in our sample. A recent systematic review revealed that it is feasible to integrate the use of parent reported outcomes into routine clinical care at pediatric medical specialty practices, and doing so can have an impact on increasing discussions about illness-related HRQoL concerns between patients, parents, and medical providers (Anderson et al., 2020).
Overall, there was moderate agreement between CCS and parents in most domains of the PedsQL. However, CCS in our study reported better quality of life than did their parents with the exception of the School Functioning domain, which is consistent with prior findings (Parsons et al., 1999, 2012; Russell et al., 2006; Speyer et al., 2009). Reasons for discrepancies between parent and CCS reporting on symptoms related to the child’s cancer have been examined by conducting qualitative interviews involving parent and child when discrepancies occurred to better understand reasons for the differences (Tomlinson et al., 2021). Two themes that emerged were the child’s lack of communication with the parents on how they were feeling and the parents’ projection of how they assumed the child would feel. Both of these issues could be reduced by encouraging greater communication between parents and children (Tomlinson et al., 2021).
The highest dyad agreement on the PedsQL was found for the Physical Functioning domain and the lowest agreement was for the Social Functioning domain, again consistent with previous studies (Fluchel et al., 2008; Yeh et al., 2005). Furthermore, the Bland-Altman plots revealed greater inter-rater variation in scores for the Social Functioning domain, and indicates that there may be proportional bias, meaning that differences between parent and child were correlated with the value of score. This suggests that when good health was more apparent (i.e., average score was higher) there was less difference in ratings between parents and CCS. The relatively poor agreement for CCS Social Functioning Score may be due to the difficulty for parents to directly observe their child’s social behavior. Also, some important aspects of social functioning are best assessed from the perception of the target child, such as peer relationships and quality of friendships (Alderfer et al., 2015).
At the same time, since the mean difference between CCS and parent was larger than the minimal clinically meaningful difference for social functioning, it is important to consider why parents consider CCS social functioning worse than do their children (Eiser & Varni, 2013). It may simply be that since parents cannot observe CCS in their social environment it is harder for them to assess this domain; however, it may also be that parents have different perceptions of CCS social behavior because their child does not frequently communicate regarding these issues with their parents (Eiser & Varni, 2013; Tomlinson et al., 2021). Future qualitative research is needed to understand the social functioning perceptions of parents, communications with their children, and how it may impact their own well-being or interactions with medical providers. This may especially be important to investigate among parents of young adults between the ages of 18–20, as we found the poorest agreement in this age group (compared to younger or older CCS) when stratified by CCS current age.
One barrier for effective long-term follow-up is a lack of knowledge of long-term survivorship care guidelines among CCS and the non-specialist physicians caring for them (Skinner et al., 2006). The findings of high dyad agreement for CCS physical functioning is likely helpful for physicians who may need to assess these factors via parent proxy-reports when pediatric patients are unable to provide self-reports. Furthermore, across the different stratifications by age, parent ethnicity, and whether CCS lived with parents, we found consistently moderate agreement for CCS physical functioning. Notably, the majority of CCS in our study were young adults (aged 18–25) and lived with their parents, which may indicate that despite their age, parents are still very much involved in their survivorship care. For example, previous studies suggest that even when CCS are young adults their parents help them transition to adult care, help them navigate conversations with providers, and their family influence their cancer-related follow up care (Casillas et al., 2010; Milam et al., 2015). Clinically, our results suggest that if parent reported outcome data are reviewed at the medical visit, such as PedsQL scores from parents or CCS and if either report low physical functioning it is relevant for clinicians to intervene and provide supportive services (Anderson et al., 2020).
Dyad agreement for School Functioning was consistently moderate, with differences in dyad agreement for the Emotional and Social Functioning, especially when stratified by parent ethnicity. Lower dyad agreement was observed among non-Hispanics; while Hispanic dyads had moderate agreement for these domains. Other studies with predominantly non-Hispanic CCS-parent dyads have indicated poor agreement for the Emotional and Social Functioning domain (Eiser & Morse, 2001; Yeh et al., 2005). Given our large proportion of Hispanic dyads, we were able to examine agreement in these domains stratified by ethnicity. These findings suggest that among non-Hispanic dyads there may be less communication about how CCS are feeling and their social relationships.
Overall, our study findings have important implications for clinical practice and research. First, it is feasible to integrate the use of parent reported outcomes into routine clinical care at pediatric medical specialty practices, and doing so can help clinicians flag when a clinical or supportive service is needed (Anderson et al., 2020). Further, the variability in agreement of the PedQL, especially among the stratified groups points to the need to train clinical practice on how to deal with the differing information they may receive. Secondly, results support the importance of referral systems to help CCS with social, school functioning, or emotional aspects of their health. In terms of research, our current findings suggest that we need to explore what may be driving the differences in dyad agreement between Hispanics and non-Hispanics. Once we have a better understanding of those differences then interventions can be created that specifically target dyads needs.
Our study has some limitations. One limitation of this study was that dyads including older CCS (i.e., >17) were less likely to be included because initial contact with older CCS did not require parental consent and required the CCS to provide the parent’s contact information. Some older CCS did not invite a parent to participate, or their parents declined (Hamilton et al., 2019). Second, the majority of parents who participated were mothers with only 11% being fathers. Thus, our results may not be generalizable to older CCS and is largely based on mothers’ perspective. Another limitation was that participants represented survivors treated at two large pediatric hospitals; thus, conclusions cannot be generalized to other areas of the country. However, the hospitals selected were major children’s hospitals in Los Angeles. Finally, this is a study of agreement, not validity. Because these measures are self-report, it is difficult to determine if the parent’s view is of higher validity than the child’s. However, because the focus is on the child’s quality of life, their perception may be most important to their ability to function and deal with survivorship issues. Further, we did not examine psychological factors in relation to agreement. While we may expect that psychological variables may affect the mental health related scores on the PedsQL we did not hypothesize that it would impact agreement overall. However, future research may want to explore this relationship among a larger sample size. Lastly, because these data were cross-sectional, causality and directionality cannot be implied. Future studies should collect longitudinal data to examine HRQoL and dyad agreement over time. In particular, it would be beneficial to assess HRQoL throughout the cancer continuum, starting during treatment and moving into survivorship.
Conclusion
In summary, we found better agreement between parent-CCS dyads for ratings of child’s physical quality of life than for social functioning, especially when scores were lower for social functioning. Communication differences by ethnicity and age may explain these discrepancies. Further studies are needed to establish the optimal predictors of levels of parent-child agreement and how these measures may be used to improve HRQoL among this vulnerable population.
Supplemental Material
Supplemental Material - Factors Associated With Agreement Between Parent and Childhood Cancer Survivor Reports on Child’s Health Related Quality of Life
Supplemental Material for Factors Associated With Agreement Between Parent and Childhood Cancer Survivor Reports on Child’s Health Related Quality of Life by Carol Y. Ochoa-Dominguez, Ann S. Hamilton, Xueyan Zhuang, Wendy J. Mack, and Joel Milam in Evaluation & the Health Professions
Footnotes
Acknowledgements
The collection of cancer incidence data used in this study was supported by the California Department of Public Health pursuant to California Health and Safety Code Section 103885; Centers for Disease Control and Prevention’s (CDC) National Program of Cancer Registries, under cooperative agreement 5NU58DP003862-04/DP003862; the National Cancer Institute’s Surveillance, Epidemiology and End Results Program under contract HHSN261201000140C awarded to the Cancer Prevention Institute of California, contract HHSN261201000035C awarded to the University of Southern California, and contract HHSN261201000034C awarded to the Public Health Institute. The ideas and opinions expressed herein are those of the author(s) and endorsement by the State of California Department of Public Health. Additionally, research was supported by the National Cancer Institute of the National Institutes of Health under Award Number F99CA264294 (PI: Ochoa, Carol).
Authors Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Xueyan Zhuang, Joel Milam and Ann Hamilton. The first draft of the manuscript was written by Xueyan Zhuang and Carol Ochoa and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the L. K. Whittier Foundation, National Cancer Institute (F99CA264294), National Institute on Minority Health Disparities.
Availability of Data and Material
Code Availability
The codes used are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.