
Abstract
Machine learning-driven efficiency is increasingly cast as a way to insure the future sustainability of understaffed healthcare systems. This article offers a glimpse into the potential practical repercussion of efficiency achieved through machine learning by examining how nurses’ practices of care provision are reappraised under machine learning logics. Building on a 4-month ethnographic fieldwork in the context of an innovation project in Dutch intensive care units (ICUs), this article centers, simultaneously, ICU nurses’ daily work, and the problem definitions and assumptions guiding the development of a machine learning dashboard for ICU ward-capacity management. It argues that nurses’ practices are centrally guided by attunement: embodied, indeterminate, affectively laden knowledge-making and action. Conversely, the dashboard torques these practices into a matter of attention: the passive, cognitive filtering of stimuli, disconnected from action. While paving the way for efficiency narratives, attention disregards nurses’ invisible and data work, and it might translate into labor intensification. This article thus proposes that moving from attention to attunement might both do justice to the complexity of nurses’ practices and provide more empirically solid policy foundations in the wake of healthcare workforce shortages.
Introduction
Data-driven technologies such as artificial intelligence (AI) and machine learning are being foregrounded as a way to guarantee healthcare systems’ future sustainability (Dowling 2019; Topol Review 2019) in the midst of workforce shortages afflicting them (WHO 2022). This argument, albeit made across care settings, has traction in acute care, where patient-to-nurse ratios are particularly low (AACN 2024), and especially in intensive care (Meissen et al. 2022), where workforce shortages have become exceptionally politicized after the COVID-19 pandemic (Navuluri et al. 2023). Due to the complex conditions of the patients they house, as well as the plethora of technologies and data mobilized for their care, intensive care units (ICUs) have been described as rather unique care settings (Marshall et al. 2017; Montgomery et al. 2024). Intensive care strikes a balance between heavy reliance on data (Meissen et al. 2022) and embodied clinical knowledge-making. Descriptions of intensive care have indeed emphasized the centrality of sensory knowledge emerging in practices such as “feeling the quality of the pulse, listening to the sound of the systolic and diastolic pressures, the observation of the color and temperature of the skin and extremities” (Morley and Spark 1970, cited in Montgomery et al. 2024).
This article responds to Montgomery et al.’s (2024, 376) recent call to pay attention to what happens to “embodied and sensory dimensions of practitioners’ work” as acute care transitions toward increased datafication and automation. It does so by considering the development of a machine learning–powered dashboard, aimed at making the work of ICU nurses more efficient. As we have argued elsewhere (Carboni 2024; Carboni et al. 2025), AI begins reconfiguring clinical settings even before it is integrated in clinical practices. In some cases, expectations around implementation generate urgency for professional and organizational adjustments (Carboni et al. 2023; Henriksen and Bechmann 2020; Hogle 2016). In other cases, such as the one we examine here, AI's envisioned affordances (i.e., the organizational and professional reconfigurations it allegedly makes possible) trigger a reappraisal of the nature of pre-existing practices, with potentially significant organizational and professional repercussions.
To illuminate such process of reappraisal, we juxtapose narratives and problem definitions informing emerging machine learning technologies with everyday care practices in the ICU—including, specifically, how nurses produce, use, and ensure the reliability of the data mobilized in their care. We find that machine learning surfaces nurses’ attention as the object through which to intervene on workforce shortages. Attention is a concept with a long history in Western modernity, which we briefly review as we survey extant literature in the first part of this article. Here, we bring together interdisciplinary scholarship that theorizes forms of attending, and empirically studies experiences related to attention in healthcare settings. This section is informed, and indeed structured, by two dominant ways of conceptualizing attention found in the literature. The first, emerging in Western postmodernity and coevolving with new media (and AI), casts attention as a passive filtering capacity in information- and stimuli-rich environments. We find that this notion of attention undergirds policy and research parlance in medicine and nursing, translating into concepts and practices of triaging, rationing and prioritization.
In contrast, phenomenological and anthropological approaches to attention raise the possibility of approaching attention as an active doing (Pedersen Morten, Albris and Seaver 2021). In this view, attention emerges as an epistemic practice inextricable from action, and thus implicated in the building of worlds. We refer to this notion through the concept of attunement, intended as an embodied, affectively laden disposition toward a situated environment. Rooted in theories stemming from feminist care ethics (Fisher and Tronto 1991; Puig de la Bellacasa 2017), attunement emphasizes the epistemic and ethical relevance of staying open to multiple rhythms and emerging patterns, rather than singling out an exclusive focus. Notions related to our heuristic of attunement often emerge in sociological investigations of experiences and practices in (acute) care settings (Carmel 2013; Montgomery et al. 2024; Moreira 2004).
Our empirical analysis traces practices of attunement and notions of attention as they emerged in each of our two field sites. Looking at ICU nurses’ practices, we mobilize attunement to show how their ways of attending to composite objects of care made up of bodies, technologies and data overflow narrow conceptualizations of attention. In our second field site, the innovation project, our analysis centers the development of a dashboard for ICU ward capacity management. Analyzing the dashboard's envisioned workings, as well as the problem definitions guiding its design, we show how, in this context, machine learning's affordances enable project leaders and dashboard developers to reframe nurses’ care work as attention. In closing this article, we argue that this operation is problematic insofar as it attempts to torque care practices into something that can easily be made efficient. This effaces the potential tradeoffs of such efficiency—namely, labor intensification and disregard for nurses’ invisible work, including their data work. We argue that moving from attention to attunement might not only do justice to the complexity of nurses’ care and data practices, but also provide solid, empirically grounded foundations for technology design and policy-making in a context of healthcare workforce shortages.
From Attention to Attunement
The Political Economy of Attention in Practice
Our perspective in this article builds heavily on work historicizing currently taken-for-granted notions of attention, commonly thought of as a “disengagement from a broader field of attraction, whether visual or auditory, for the sake of isolating or focusing on a reduced number of stimuli” (Crary 2001, 1). In this sense, historian Jonathan Crary's foundational work argues that current notions of attention crystallized in the nineteenth century alongside imperatives and techniques of “paying attention” that are not only culturally specific but, crucially, intrinsically tied to emerging technologies. Indeed, the notion of attention as a filter was mainstreamed in the 1970s, in a context where the “attention economy” was gaining prominence in the wake of new media and digitalization. Economist and psychologist Herbert Simon (1971) decreed the end of the information economy (Davenport and Beck 2001; Goldhaber 1997), purportedly supplanted by a new regime in which attention emerged as a scarce commodity (Zulli 2018).
Attention is described in this literature as a cognitive capability that can be either on or off, and thus attracted, deviated, and economized (Bucher 2012; Crogan and Kinsley 2012). Moreover, its scarcity is both caused by new media (through information overload) and potentially solved by them (by “only provid[ing] users with the information that they need to know” (Bucher 2012, 8)). Attention as a filter becomes a generative notion in the context of machine learning where, as shown by historian of technology Orit Halpern (2014), it is mobilized as a core concept of AI. Likewise, cultural geographer Louise Amoore (2020, 17) emphasizes how algorithms are filters that function by discarding “much of the material to which [they have] been exposed.”
Although this terminology is not often mobilized in empirical studies of medical work and nursing, the notion of attention sketched above features in policy and research parlance, translating into concepts and practices of triaging, rationing, and prioritization (Van Pijkeren, Wallenburg and Bal 2021; Waterworth 2003). Attention, we argue, is the very mechanism scaffolding rationing, as well as the cognitive (and inherently political) process of task selection that enables prioritizing, and sometimes leaving care undone.
Research in medicine and nursing often asks which tasks caregivers attend to first (Felder et al. 2024), what care they leave undone because of time and resource constraints (Scott et al. 2019), and how this affects patients’ experiences and outcomes (Papastavrou, Andreou and Vryonides 2014). Scott et al. (2019), for instance, emphasize the fraught decision-making nurses face when selecting which tasks they should attend to, and which can be left undone. In a similar vein, Felder et al. (2024, E123) argue that rationing has become integral to the politics of welfare states. Especially in the context of workforce shortages compounded by COVID-19, [n]urses play an important role in mundane rationing practices because of their key position in the organization and delivery of patient care…This implies that they need to make difficult and situated decisions about which patients to spend time with, care for, transfer to others, put on a waiting list, or strategically ignore.
There are, however, empirical studies of rationing and triaging that propose a slightly diverging angle. For instance, Van Pijkeren, Wallenburg and Bal (2021) analysis of a triaging system in elderly care alerts us to efforts to economize and ration caregivers’ attention that do not eliminate the need for different kinds of attending to patients. In the case they analyze, nurse aids’ idiosyncratic knowledge of patients, and the gut feeling they developed for subtle shifts in their health, emerge as a central component of clinical knowledge-making. This inefficient form of knowledge cannot be rationalized, even in attempts at economizing doctors’ attention and care provision. A similar type of idiosyncratic and relational knowledge has been surfaced as a crucial component of clinicians’ engagements with algorithmic predictions, which are, themselves, meant to direct their attention to urgent cases (e.g., Maiers 2017).
These investigations of attention alert us to the lived experience of care provision in overstimulating and resource-poor care settings, as well as to the ethicopolitical import of care allocation choices nurses (have to) make. As a heuristic, attention resonates with policy parlance foregrounding rationing and triaging. However, as we have begun to see, it falls short of accounting for other forms of attending that—while overflowing dominant notions of attention as passive receiving and filtering of stimuli—are no less central to intensive care provision. To begin to chart these practices of attending, in the next section we assemble attunement as an alternative heuristic.
Assembling Attunement
Our discussion of attunement builds on theorizations and empirical examinations of care in practice (Mol 2008; Mol, Moser and Pols 2010). Building on feminist care ethics, this scholarship foregrounds care as a disposition toward and an engagement with situated, more-than-human worlds. Care encompasses practices of maintaining and repairing these worlds so as to live in them “as well as possible” (Fisher and Tronto 1991, 40). These practices, as articulated in María Puig de la Bellacasa's (2017) foundational work, are a matter of embodied and affectively charged labor. Moreover, care is crucially ethicopolitical: it operates noninnocent choices, it inevitably excludes some, and it might even be associated with some forms of violence (Martin, Myers and Viseu 2015). We offer a reworking of the concept of attunement to already generative discussions of care. Attunement, we argue, provides a heuristic to analyze the microlevel, phenomenological aspects of care. In other words, we assemble under this notion the affective and ethical aspects of care in practice. Moreover, attunement emphasizes the sensory dimension of care (e.g., Tsing 2015), as well as its epistemic import, highlighting how care is not just about maintaining worlds but, simultaneously, about producing a specific, embodied and relational, type of knowledge about them.
Anthropologist Kathleen Stewart (2011, 452) provides an exploration of attunement as an active living through, sensing out and participating in the emergence of the worlds we inhabit. For Stewart, bodies attune to atmospheres, the “force-field[s] in which people find themselves.” Attuning entails the labor-intensive process of tuning one's senses, physical actions, and sense of potentiality to an atmosphere's affordances, all the while remaining open to emergence and potentiality. Recently, Tim Ingold (2022) discusses attunement as a way of developing “wisdom” in inherently uncertain worlds. Ingold emphasizes how attunement is a form of sensory education, of sensitizing one's perceptual system. In turn, this sensitizing, as Sara Ahmed (2010, 2014) reminds us, is a matter both of work on the self and of bodies’ experiences, habitus, and positionality. Attunement thus emerges as an embodied disposition developed within and toward a specific environment, which entails a learning process as much as a reshaping of one's body. It is an ongoing accomplishment, which lies in the progressive, reciprocal adaptation of a body and the objects it interacts with. For Ingold (2022, 23), “to observe, it is not enough merely to look at things. We have to join with them, and to follow…Attending to these ways, we also respond to them, as they respond to us.”
Our notion of attunement aims to capture the embodied, relational knowledge that stems from staying open to, responding to and participating in, worlds’ emergence (Kenney 2019). Resonating with the epistemic dimensions of attunement, STS scholar Anna Tsing (2015, 23) offers the notion of arts of noticing as the practice of “watching the interplay of temporal rhythms and scales in the divergent lifeways that gather.” Arts of noticing point to a way of knowing that, unlike attention, is not only about isolating a specific object, but about considering it in its temporal, spatial, and ontological relations with other objects. Tsing's (2015, 46) arts of noticing center indeterminacy, a “particular kind of attention to the here and now of encounter, in all its contingencies and surprises.” This is an open mode of perceiving that enables picking up and even centering on the unexpected, rather than filtering it out as noise. When put into conversation with our emerging notion of attunement, Tsing's arts of noticing emphasize the inextricability of embodied knowing and situated acting. Moreover, in contrast to attention, attunement is an open mode of perceiving that does not preselect a single focus, but rather takes in a complexity of multispecies interconnections, participating in the emergence of more-than-human worlds.
Our heuristic resonates in analyses centering the nature and experiences of care provision in and beyond acute settings, stemming from medical sociology and sensory anthropology. First, studies of embodied learning in clinical settings, spearheaded by Harris (2021) and Maslen (2017) alert us to the centrality of sensory skills to the making of clinical knowledge. This learning is a process of becoming attuned to patients’ bodies (Harris 2021), technologies and data (Maslen and Harris 2021), and care settings (Harris 2011). Sensory attunement is also actively practiced in daily clinical work. Moreira (2004) analyzes surgeons’ bodily experiences in the operating room, describing how they “devise strategies to become ‘tuned with’ the sensorial affordances of the operating area, learning to be affected by the objects presented to them as a strategy of learning how to act upon them.” As he claims, surgeons actively submit “to the perceptual differences of this world in order to better act within it” (Moreira 2004, 123). Attunement in clinical practice is thus configured as an open, indeterminate form of attention stemming from the entwinement of knowledge-making, action and embodied work on the self. In this sense, Montgomery et al. (2024) also argue that clinical knowledge emerges from moments in which professionals’ bodies, patients’ bodies, and clinical space mutually constitute one another.
Speaking more directly to the question of attunement in acute care, and to how it is (or fails to be) reconciled with other sources of information, Carmel (2013) describes intensive medicine as a craft in which knowledge is applied and adapted in constant interaction with the material world. He articulates how clinicians carefully weigh quantitative data returned by the plethora of ICU technologies against their embodied experience of patients’ bodies. He thus joins a strand of scholarship that emphasizes the importance of sensory knowledge in settings such as anesthesiology (Goodwin 2010), neurosurgery (Moreira 2006), and neonatal intensive care (Mesman 2010). Speaking to the nature of care in acute settings, Stonington (2020) describes how the inherent uncertainty and the fast tempo of acute disease that clinicians muddle through in the ICU translates in them not aiming to develop an actual knowledge of patients’ conditions. Rather, they attempt to combine all available sources of information about the ever-changing constellation of problems that are ICU patients’ bodies. By orchestrating this plethora of information, clinicians can, at best, hope to suspend their uncertainty long enough to “make a move” on patients. They thus inhabit an ever-shifting relation to patients and their disease, 1 constantly adjusting their stance toward it.
In contrast with empirical studies of attention surveyed above, sensory ethnographies of care settings tend to focus on physicians’ practices and experiences. However, as Davina Allen's (2014) influential work shows, nurses perform crucial organizing work coordinating different aspects of care across care settings—and a great deal of their organizing work is supported by embodied forms of sensemaking. Building upon these insights, our notion of attunement opens up avenues to chart these embodied practices of knowledge-making and care provision before they begin to morph under the pressure of ambitions for data-driven efficiency. As a heuristic, attunement suggests a broad, more-than-human analytical focus, zooming in on the embodied, affectively charged practices through which nurses navigate and sustain care provision in a complex environment.
Methods
This article builds on 4 months of intensive ethnographic fieldwork conducted by the first author (CC) in the adult ICU wards of a large Dutch academic hospital. Access to this ICU was gained thanks to the second author's (RW) involvement in a grant application for the development and implementation of “inclusive AI” in the ICU. Ethics approvals were granted by the Research Ethics Review Committee at the lead author's department and by the hospital's Internal Review Board.
The fieldwork took place between March and June 2022 and comprised two sites: the ICU wards and the innovation project. Across sites, data collection was guided by the study's overarching questions, encompassing nurses’ reception of the innovation project, their experiences and practices of care on the ward, and the appraisal of nursing work driving the design of machine learning technologies. On the ward, CC shadowed nurses throughout their 8h shift, taking extensive fieldnotes. She had long informal conversations with nurses (around 10 in each shift) about their experiences and their strategies for caring for and interpreting both patients’ bodies and technologies. She observed nurses’ routine checks on patients, consultations with intensivists, and patient transfers. She also joined nurses during breaks and participated in their informal discussions.
To increase nurses’ acceptance of and trust in AI technologies, the project team at the hospital organized a series of meetings they referred to as “inspiration sessions.” During these weekly 30min sessions, nurses were informed about AI technologies currently available for ICUs, and asked to write down “points for improvement” to “future-proof” their ICU. The first author observed six out of the seven sessions held, and helped to collect nurses’ input by transcribing the sticky notes they filled in. Although these sticky notes were barely discussed during the sessions, CC took extensive fieldnotes detailing the nurses’ reactions to the information presented to them, and the issues they brought up.
Thus, albeit she was assigned no care responsibilities, CC's presence in the ICU inevitably and, to a degree, by design, intervened on the field itself. Firstly, her presence, data collection and constant communication with nurses contributed to justifying the project's aim. Moreover, the project's leaders required her to identify moments in the nurses’ workflow that could be made “more efficient” through data analytics. To this end, she produced a visualization of nurses’ workflow based on her ethnography. To gather material for this visualization, CC focused her observations on how nurses produced, used, and ensured the reliability of the data mobilized in ICU patients’ care.
Being tasked with this visualization put us in an ethically fraught position. On the one hand, we wanted to contribute to the project, generating knowledge that was meaningful to the people who granted us access. On the other, we were wary of the framework of efficiency that was being imposed on the visualization itself. This discomfort increased as fieldwork proceeded and learned that physicians often discussed nurses as idle, often sitting around and “drinking coffee.” Moreover, it gradually emerged that this efficiency was aimed at stretching current patient-to-nurse rations, and introducing more tasks, such as “learning moments.” The interactive visualization (Figure 1) we produced attempted to strike a balance between showing what steps in the workflow produced data, and which ones relied on data: we aimed to show the complexity and value of nurses’ practices and the potential tradeoffs of “automating” them, rather than pinpointing moments to be optimized.
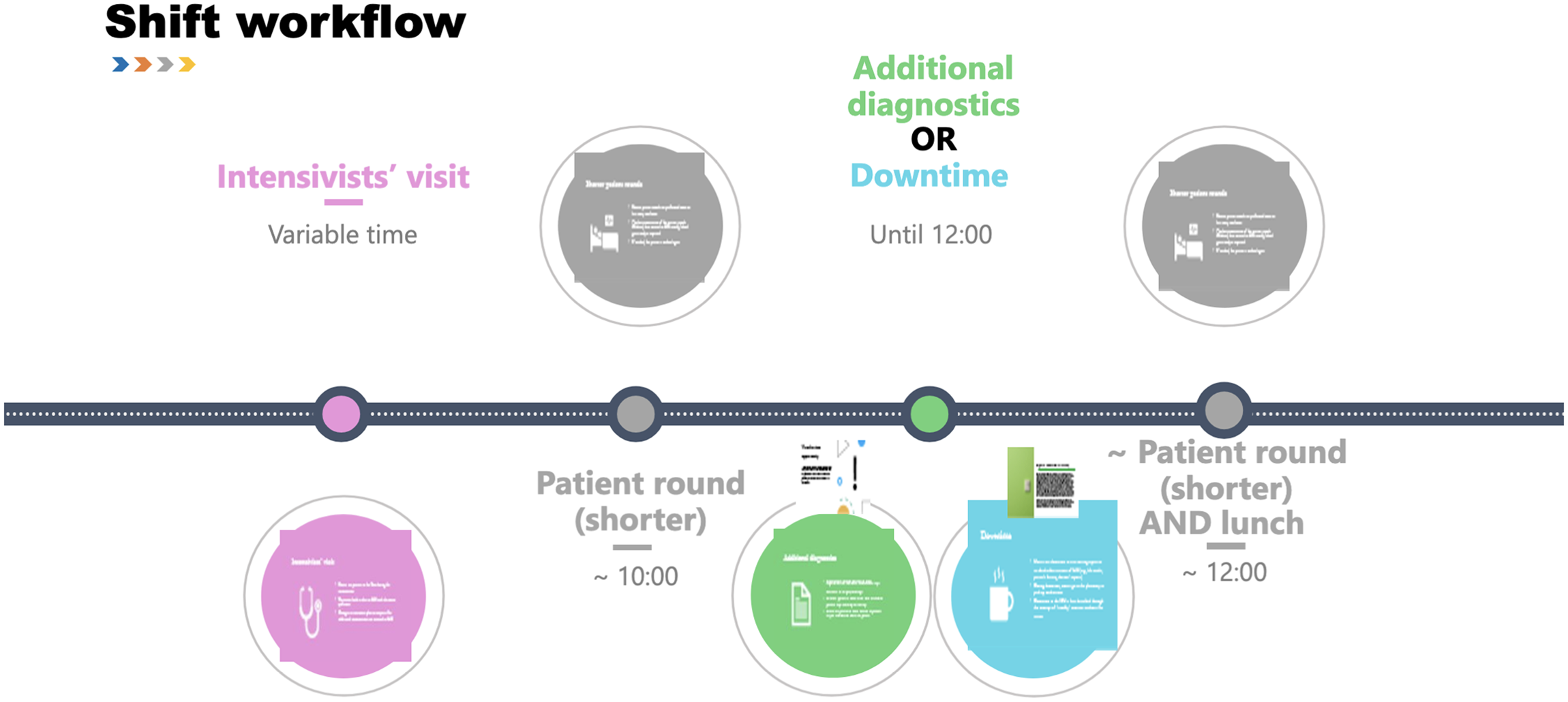
A screenshot of the interactive visualization we provided to the department. While nurses' workflow is represented linearly, by clicking on each step, users can access explanations and vignettes illuminating nurses' invisible care and data work.
Fieldnotes informing both the visualization in Figure 1 and this article was coded inductively in Atlas.ti. Coding was shaped by CC's lived experience in the ICU—from the missed sleep, to the emotional shocks and exhaustion, the overstimulation caused by all kinds of alarms, and being exposed to nurses’ frustration over their labor conditions. Tracing how nurses navigated and created working knowledge out of the sociotechnical ensemble of ICU patients’ bodies and care technologies resulted in codes on issues such as data error (correction), sensing, tinkering, time, efficiency, information flow, and knowledge- and decision making. CC provided the initial analysis, which was strengthened through joint discussions among all co-authors. RW, in particular, was directly involved in streamlining the overall argumentation.
Preliminary insights, as well as the visualization, were discussed with the innovation project's leaders, including the head and manager of the ICU. These discussions brought new issues to management's attention (e.g., the relevance of nurses’ invisible data work for data quality, and ultimately for machine learning's outputs). However, despite our attempts at nuancing concepts of care and efficiency, at its core, the project ultimately maintained its original ambition of making nurses’ work more efficient through data.
Attention and Attunement in Intensive Care Nursing
Tracing Attunement in Nurses’ Practices
ICU patients are connected to myriad technologies, some of which take over or support vital functions (e.g., mechanical ventilators, the extracorporeal membrane oxygenation machine, ECMO), while others measure and display their vital signs in real time (e.g., heart rate, blood pressure, oxygen saturation). Finally, patients are attached to intravenous (IV) pumps administering medications. ICU nurses’ object of care is this composite made up of bodies, technologies, and data. The very technologies that keep patients alive also produce the real-time data that provide a proxy for monitoring patients’ health—and, incidentally, also make the ICU an attractive environment for the application of AI technologies (Hadweh et al. 2025).
In tracing nurses’ attunement practices, we describe how, in order to know and act, they orient their bodies to composite care objects. This also entails fixing sensed discrepancies that might point to instances of dis-attunement among care objects’ components. As this analysis shows, attunement practices are at the heart of both patient care and the production of clinical data.
Dis-Attuned Machines
Although they prepare for it during their handover with colleagues from the previous shift, and by scanning previous reports in the electronic health record (EHR), nurses’ attunement to their care object begins when they step inside the patient's room. Routinized moments of attunement punctuate nurses’ workflow: at the start of the shift, and then every 2 h, they conduct a “patient round,” during which they check technologies’ settings and alarm thresholds. The first patient round is time-consuming: nurses first attune to each technology, checking that their settings match clinical notes, and that they are well-positioned and working properly. The latter aim, especially, requires attuning to different components of the composite care object they work with (including the patient's body), to notice potential discrepancies: Tom moves to the ventilator, examining not only the tubes and the values displayed on its screen, but also the pressure of the cuff—an inflatable balloon sitting inside the patient's throat, which ensures the tubes don’t move…He measures the cuff's pressure with a barometer, explaining that usually, if the pressure is insufficient, “you can just hear it.” A while later, when we come back in to wash the patient, Tom invites me to get closer to the patient's face. I hear a gurgling sound. “This means there's not enough pressure,” Tom explains. He proceeds to pump air into the cuff. (Field notes, cardiac ICU, March 2022)
Dis-Attuned Patient's Body
In other cases, it is the patient's body that might need to be re-attuned. If, as we saw above, checking life-supporting machinery might entail getting close to and sensing the patient's body, the second part of the patient round, which aims at directly examining the patient's bodily functions, combines moments of sensing the patient's body (e.g., looking at pupils, feeling limbs’ temperature) with an emerging attunement to the data that act as a proxy for the body's physiological functions: vital signs. While nurses become attuned to technologies by sensing patients’ bodies, as we see below, they can, vice versa, become attuned to patients’ bodies by looking at numbers on a monitor: Having checked all the machines’ settings, Tom moves to the patient's bed…Since the patient's oxygen saturation levels are low, he informs me he will check for mucus in his ventilator tube. With a little suction tube, he removes some mucus from the tube. The saturation data on the vital signs monitor go up quickly. (Field notes, cardiac ICU, March 2022)
During patient rounds nurses attune themselves to their care object, and while doing so, also attune different components of it (i.e., technologies, patients’ bodies), ensuring they are working well together. Attunement also entails attuning the care object to oneself, making it work for oneself by tapping into its automated agencies—for instance by replacing medication pumps close to running out at a convenient time, or setting alarm thresholds. Thresholds also vary because different ranges of “normal” apply to different patients: as a nurse explained, “the normal saturation level for a patient with COPD [Chronic Obstructive Pulmonary Disease] could be cause for concern in someone who is healthier” (Field notes, general ICU, May 2022). Setting thresholds shows how the very possibility of alarms meaningfully participating in the care object is predicated on nurses’ being attuned to a patient's body, understanding what can be expected from it.
Dis-Attuned Data
Instances of dis-attunement are routinely spotted and intervened upon during patient rounds. However, some signs of dis-attunement, which are subtle and do not trigger an alarm, are most easily spotted by nurses in between patient rounds: Looking at her patient's vital signs monitor, Nina notices something strange in his arterial line tracing. Since the peaks of the tracing are overshooting, she suspects there might be a data artifact. We enter the room, where she tries flushing the patient's arterial line. The tracing on the screen becomes a little flatter, but apparently not enough. She explains that these artifacts sometimes have to do with the way patients hold their hands: the cannula is inserted in their wrist so, if they bend it, the measurements might be altered. She tries to put a cushion underneath the patient's arm—but also this doesn’t seem to change things much. She figures that the cannula must have moved slightly as the patient moved his hand, and will need replacing since “he's had it for a while already.” (Field notes, general ICU, May 2022)
Identifying potential dis-attuned data, however, is not sufficient: re-attuning the care object is an embodied activity that needs to account for the porous boundaries between a patient's body and technology—thus probing various possible origins of the dis-attunement. Dealing with data artifacts entails opening up the enacted nature of data, produced at the interface of potentially faulty sensors, potentially misplaced cannulas, and inconveniently bent joints. Nurse Nina quoted above knows that, for data to provide reliable insight into the patient's body, different components of a care object must be attuned. Investigating the causes of data artifacts, and trying to eliminate them, entails a time-consuming, open-ended process of attending to and acting with both technologies and the patient's body.
Shifting Modes of Attunement
So far, we have teased out different aspects of nurses’ attunement practices concerning care objects inside ICU rooms. In this last section, we follow the care object as it extends outside patients’ rooms in the form of pagers, monitors, and their alarms. When in the corridor, nurses are supposedly not “paying attention” to their patients—that is, not providing direct patient care. Sitting at their desks, they talk to each other and perform administrative tasks, such as filling in the EHR, ordering tests, and checking lab results. However, even in the corridor, nurses maintain a level of attunement to their care objects—a certain degree of orientation toward technologies and real-time data and, through them, toward the bodies inside the rooms. Crucially, through monitors and alarms, the object of nurses’ attunement is also expanded to the unit's aggregated patient population.
Alarms might appear as technologies of attention, rather than attunement. Yet, as we saw above, their functioning relies on nurses’ attunement when setting appropriate thresholds. Moreover, by being on the ICU, nurses develop ways to attune to alarms themselves. Indeed, since alarms are constantly going off, attunement to the ICU environment also entails distinguishing different types of alarms, and ignoring some of them. Gradually, even just by being on the ward, one starts disregarding blue alarms (indicating disconnected sensors) and stops being startled by yellow ones (signaling slight deviations from set thresholds), unless they keep recurring. Paradoxically, in the vignette below, it is the dis-attuned ethnographer, whose responses are unaligned with the other bodies in the same environment, that brings into relief nurses’ own attunement to data and alarms: Sitting at the desk, Velma and Victor are sharing grievances about the pharmacy. I keep being distracted by a red alarm in room 10. Above our heads, the part of the monitor displaying the electrocardiogram keeps turning red and displaying “ASYSTOLE,” and Velma and Victor's pagers keep beeping, though they both keep silencing them…At last, I bring up how “things seem not going well in room 10.” Velma giggles and tells me not to worry: “It's just the sensor malfunctioning. This patient has blood pressure; had it been an asystole, everything would be flatlining.” She turns off the monitor's alarm and resumes her conversation. A bit later, the alarm goes off again while Velma and Victor are in their respective patients’ rooms. This time, they both jump out quickly to check what's going on and if their help is needed. (Field notes, cardiac ICU, April 2022)

A view of the monitors above nurses' desks. The monitors display the vitals of all patients currently in the ward, providing nurses with an overview that allows them to dismiss false alarms and understand where their help might be required.
During downtime, when nurses are in the corridor, alarms do manage to spur their re-attunement, surfacing a specific object of care: Deborah and I, together with most of the other nurses, are sitting in the middle of the corridor drinking our coffees and chatting, when an alarm goes off. The monitor above the desk in front of which we’re sitting starts blinking, the blood pressure value turning red. All the nurses suddenly go silent, turning their heads toward the monitor, and immediately jump out of their chairs. A second later, Jamie emerges from the room, and yells, “Cart!” Deborah runs to get the crash cart and pushes it in front of the door, while another nurse gets the defibrillator (which is still plugged into the wall, so another nurse needs to run after her and unplug it). As I follow them, I see a doctor performing a heart massage among a cacophony of alarms. (Field notes, general ICU, May 2022)
Having to re-orient one's body to act in an abruptly emerging atmosphere is practically and emotionally disruptive. This vignette testifies to the affective components of attunement, to how re-attuning to a rapidly changing situation is more than a simple shift from “distracted” to “attentive.” Alarms and the emotional response they generate teach us that care objects themselves are affectively charged, and that re-attuning to a new care object, going from downtime to emergency, is not just about turning on an attention switch, or moving to a different focus. Re-attuning is both cognitively and affectively charged, and attunement to emergency situations takes a toll on clinicians. As we show below, these affective and embodied experiences of re-attunement were effaced in the machine learning-driven appraisal of nursing work as a matter of attention, which emerged in the innovation project we studied.
Harnessing Attention: A Glimpse into Machine Learning-Driven Efficiency
As mentioned above, our fieldwork stretched beyond the walls of the ICU, following nurses as they attended the so-called “inspiration sessions” organized by the project team and meant to kickstart the innovation project. Led by Jim, the intensivist in charge of the project, and seeking to “involve nurses from the start of the innovation trajectory,” these 30min sessions were held weekly for almost 2 months. At the beginning of each session, nurses were invited to think about aspects of their work that would be different in an ideal “future-proof ICU.” This was followed by a 20min presentation by Jim on AI applications in ICUs.
When asked what they would like to be different in the ICU of the future, nurses tended to bring up workforce shortages—an issue that had been thrown into sharp relief since the COVID-19 pandemic: Someone asks if they can also say that they just need more personnel. Jim doesn’t seem enthusiastic, but says that “that's also a possibility”…[In a later session] Jim mentions laughing that nurses in the previous sessions have come up with points about parking spots and more personnel. Regardless, the point about more personnel also comes back in the sticky notes that nurses hand over to me at the end of the session. (Field notes, inspiration session, April 2022)
Although this was not communicated at the start of the project, it soon emerged that collecting sticky notes was not exactly a sincere attempt to build an “inclusive AI” at the large Dutch academic hospital where we conducted our fieldwork. The project team (constituted of intensivists and hospital managers, as well as one nurse) had already settled on a technology to be piloted: a machine learning-powered dashboard for ICU ward capacity management, which would display available beds and personnel, as well as predictions of patients’ states. Two PhD candidates had already been hired to help develop it. To be built with support from a major data analytics company, the dashboard would analyze real-time patient data and, through an undisclosed machine learning model, predict each patient's near-future “care needs.” As one of the department's intensivists explained in an interview to a Dutch magazine in 2022, stable patients would be displayed as green, the ones “in need of more attention as orange,” and the ones in a critical situation as red. The intensivist also explained that being “green” would not entail that a patient needs “no attention,” but rather that nurses could “focus on the human dimension. Alternatively, they could assist colleagues dealing with unstable patients, thus allocating their time more efficiently.” Ultimately, as emerged from conversations with management, the dashboard's goal was to allow stretching current staffing protocols, making it possible to assign more patients to each nurse.
Focusing on how the assumptions about users’ practices and responsibilities inscribed the dashboard, we can begin to unpack how its expected functioning builds on a specific appraisal of nurses’ care practices, and how that shapes the opportunities envisioned for intervening on them. The dashboard promises a continuous analysis of real-time data. Based on this analysis, it would assign patients to categories of (in)stability. In other words, the dashboard would sift through myriad data points continuously produced for each patient, combine them, and single out the patients who require nurses’ immediate attention. This means, first, that the analytics built into the dashboard would function as an automated filter of sorts, reminiscent of modernist notions of attention (see Halpern 2014). Second, this filtering would be mobilized for algorithmic management (Jarrahi et al. 2021): based on machine learning outputs, nurses would be able to prioritize their care tasks, thereby allegedly optimizing their time allocation. Thus the dashboard would both embody a model of attention as a filter, and impose it on nurses’ practices. Appraising their care provision in terms of attention makes nurses’ work into an object suitable for algorithmic management, while disregarding the centrality of attunement to their practices.
As we have seen above, modernist iterations of attention cast it as a passive capacity, something eminently cognitive, which functions by singling out one focus from a multitude of stimuli. On this basis, the dashboard assumes that attention can be easily refocused from one task (and from one patient) to another. Provided a worthy focus is identified, nurses should be able to disengage from other stimuli and tasks, to attend to the ones that data analytics flag as urgent. This, in turn, assumes that nurses’ practices can be neatly divided into (delegable) tasks. It also seems to propose that nurses have no affective investment in their patients’ care beyond ensuring their immediate survival, and that they can easily disengage from their care to turn to more pressing matters. Working with a notion of attention as a passive filter, the dashboard turns nurses into recipients of data analysis, failing to consider how data itself is imbricated in and sustained by nurses’ care practices. Finally, it also appears to reduce nurses’ work to attending to (unstable) patients: if they are to utilize their attention efficiently, nurses are to move quickly from one urgent care task to the next. Indeed, chopping up ICU patients, as it were, into urgent tasks, appears as the only way in which patient-to-nurse ratios could be stretched. The dashboard's contribution to solving workforce shortages would, in essence, be a matter of labor intensification—of cramming more (stressful) tasks into each nurse's shift.
A crucial corollary of this point is that, to optimize the use of nurses’ attention, the dashboard's script operates a redistribution of responsibility, particularly as it relates to patient safety. If deciding what counts as “urgent” and what deserves nurses’ attention is a question of autonomy and professional judgment, a considerable part of the responsibility for such decision would be diverted from the nurses themselves to the dashboard's data analytics. Although nurses’ attention has been described as politically and potentially biased and unjust (Felder et al. 2024), it is worth noticing here how this dashboard attempts to turn what is a matter of professional judgement and ethics (Scott et al. 2019) into a technical question solely predicated on data.
During the inspiration sessions, nurses requested to be themselves the ones to decide which patients would qualify as green, orange, or red. Insofar as it aims to override algorithmic outputs and put nurses in charge of their time allocation, a similar attempt to preserve professional autonomy would somewhat defeat the very purpose of mobilizing machine learning in the first place. We do, however, wish to take such moments of resistance seriously. Therefore, in closing, we articulate the professional and organizational implications of attempting to reframe nurses’ attunement as attention.
Discussion and Conclusion
Building on an ethnographic case study, this article has discussed the potential practical implications of attempting to make intensive care more efficient through machine learning. This analysis has contributed to existing STS literature on care and knowledge practices in datafied healthcare in several ways. First, we have offered an in-depth ethnographic exploration of nurses’ data and care practices, proposing the concept of attunement as the how of prioritization and rationing practices. Attunement, as we argue, represents an empirically grounded heuristic to think about work in data-rich and technology-dense care settings. Attunement enables us to open up microlevel practices of care and knowledge-making. It proposes approaching these practices as embodied, more-than-human accomplishments, in which different actors adjust themselves to each other, becoming accustomed and alert to their respective rhythms, expressions and needs. As per our ethnographic vignettes describing the panicked exhaustion following abrupt re-attunement in emergency situations, attunement also sheds light on some political aspects of these practices. But it does so not by emphasizing the biases (Felder et al. 2024) and difficult choices (Scott et al. 2019) at the heart of care rationing, as often proposed in articulations of the politics of attention. Rather, the notion of attunement foregrounds the affective and physical toll that acute care, despite its alleged inefficiencies, takes on those who provide it (Van den Broek 2017; Wiedemann 2021), and the lack of organizational recognition for the labor-intensive character of attunement (see also Ahmed 2014; Ingold 2022).
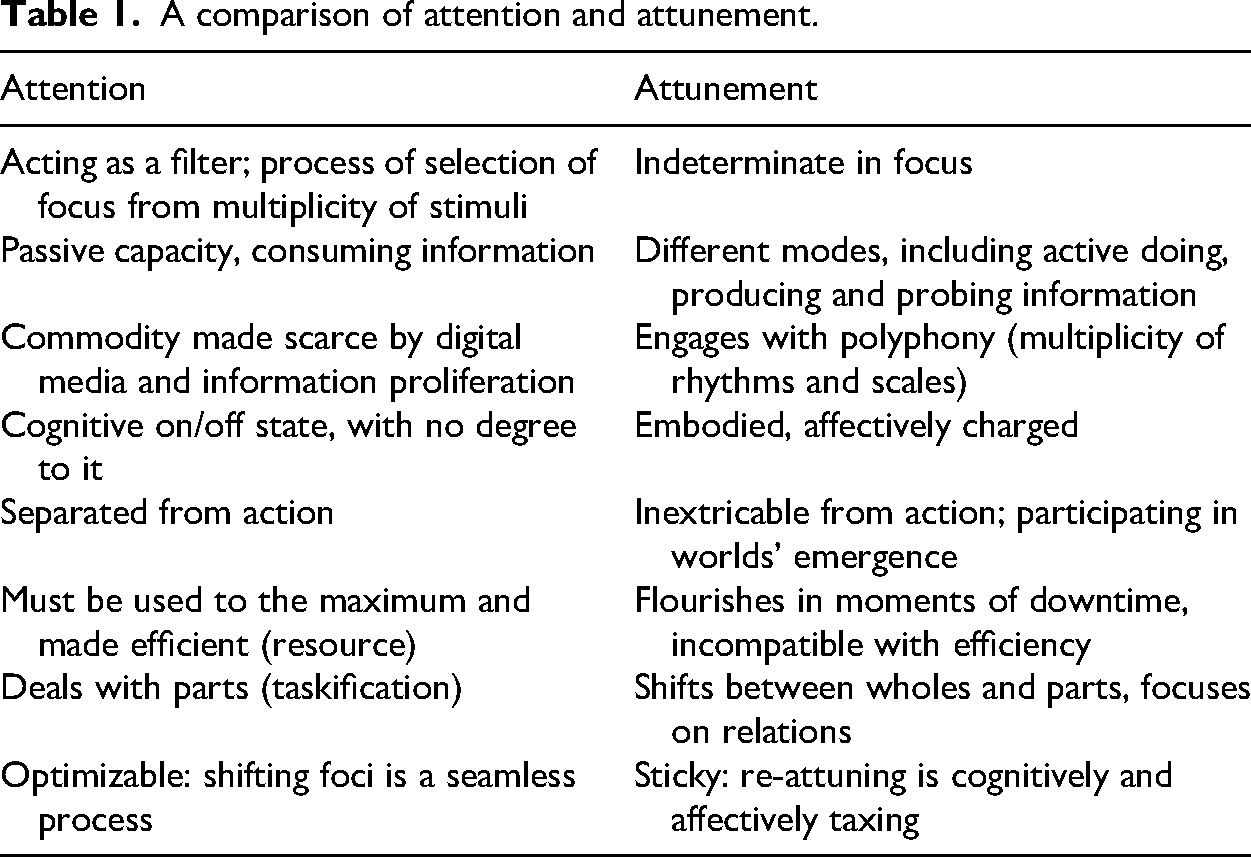
Second, we have thematized attention as a managerial object constituted through machine learning. We have argued that data analytics risk entrenching modernist notions of attention as a suitable way of appraising and intervening on care practices. As we have shown, the dashboard's appraisal of nurses’ work rested on several assumptions that strongly resonate with modernist notions of attention: attention as a merely cognitive state; data analytics as easily redirecting attention, potentially ad infinitum, without considering nurses’ own emotional state; and downtime as lack of attention. Our ethnography showed that these assumptions do not match ICU nurses’ attunement practices. Whereas frameworks centered on attention posit nurses’ externality to the technologies and the data deployed in the ICU, their attunement practices are rooted in the experience of affecting and being affected by ICU care objects. Table 1 offers a summary of the main differences between attention and attunement.
A comparison of attention and attunement.
Third, our analysis provides an empirically grounded reflection on the organizational and professional ramifications of emerging machine learning technologies. Our argument that professional practices need to be discursively reframed in order to make them into objects for machine learning's appraisal and intervention bears analytical implications. We have shown it is relevant to analyze how work and workers are being reimagined in an era of machine learning—specifically, whose work machine learning technologies try to make more efficient, and what types of work might fall outside the scope of efficiency improvement. In our case, nurses were singled out as targets of increased efficiency (Maslen 2017; Mort, May and Williams 2003). Moreover, the efficiency the dashboard purported to achieve rested on a disregard both for the invisible work (Oudshoorn 2008) of attunement, and for the visible but undervalued work of data production (Bossen 2019). This raises questions about when, how, and by whom these less “urgent” tasks would be performed, as well as how nurses would experience work practices that are increasingly oriented toward urgency. Albeit falling outside the scope of the present article, charting clinicians’ reactions to attempts at algorithmically turning their attunement into manageable attention strikes us as a worthy focus for future research.
Our analysis also bears important implications for practice. Investing in technologies, and specifically machine learning, is increasingly viewed as a viable strategy to increase efficiencies and thus ensure healthcare systems’ future sustainability (Agyeman-Manu et al. 2023; Siegel 2023). Our analysis of attunement in practice urges caution around narratives of technologically achieved efficiency. First, efficiency is often construed as eliminating downtime, in an attempt to keep professionals in a constant state of productivity. However, tasks that are not urgent, such as dwelling on sensed discrepancies and investigating their possible origin, are crucial for both patient safety and for the production of reliable data (which would, in turn, be fed to machine learning). The importance of this care and data work should be inscribed within any technology that attempts to intervene on attention in acute care settings. Although proposing alternatives for technology design falls beyond both the scope of this article and our expertise, making the concept of attunement central to technologies in clinical settings might provide avenues to bring technology design more in sync with the needs and rhythms of care provision. In closing, we invite decision-makers, clinicians and technology developers to think, jointly, about what might happen if we started thinking about care work as driven not solely by data and attention, but by attunement to bodies, technologies, and data themselves.
Footnotes
Acknowledgments
The authors would like to thank all the participants who shared their time and insights with us. We are also thankful to the Digital Culture group at Copenhagen University for providing valuable comments that greatly helped sharpen this paper’s argument, and to the anonymous reviewers and ST&HV editors who engaged generously with our manuscript. This article, and the PhD project as part of which it was written, was made possible through the financial support of the Medical Delta program Journey from Prototype to Payment, and of the Erasmus School of Health Policy & Management.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.