
Abstract
Unlike sonographic examinations, sonic fetal heartbeat monitoring has received relatively little attention from scholars in the social sciences. Using the case of fetal heartbeat monitoring as part of midwifery prenatal care in Germany, this contribution introduces music as an analytical tool for exploring the aesthetic dimensions of obstetrical surveillance practices. Based on ethnographic stories, three orchestrations are compared in which three different instruments help audiences to listen to what becomes fetal heartbeat music and to qualify fetal and pregnant lives in relation to each other. In the Doppler-based orchestration, audible heartbeat music is taken as a sign of a child in need of parental love and care cultivated to listen. The Pinard horn makes esoteric fetal music that can be appreciated by the midwife as a skilled instrumentalist alone and helps to enact a child hidden in the belly. The cardiotocograph brings about soothing music and a reassuring relationship with a child but also durable scripts of juridical beauty. This material-semiotic analysis amplifies how well-being is shaped in midwifery prenatal care practices.
Introduction
In the anthropological study of prenatal care, there has been little attention to fetal monitoring technologies that involve sound, compared to those that produce images. Anthropologists have shown how ultrasound pictures, accepted as accurate representations of real fetuses, forge affective relations: “baby’s first picture” (Mitchell 2001) bonds not only a mother, a father, and a family but also wider publics to a lovable child as an individual other (Petchesky 1987, 268; see also Haraway 1992, 312).
But what do sonic productions of fetal heartbeats do? Within sound studies, scholars have investigated the medical practice of stethoscopic listening as a way of acoustically evaluating human bodies. In care practices, knowledge and normativity are closely intertwined, as care practices are oriented toward producing something good (Pols 2015, 83, 87). These goods are not merely moral: they are also medical, juridical, economical, and aesthetic. Aesthetic values can be understood as “genres of activities” (Pols 2013b, 187) that create and organize social relations around what is both pleasing and good. Analyzing this aesthetic dimension, I argue, may help us to better understand fetal monitoring practices. This article, based on research into how midwives in Germany produce and listen to fetal sounds, shows how aesthetic values orchestrate this activity. Articulating how the aesthetics of fetal heart rate monitoring help to bring their participants into life, biologically and socially, this study introduces heartbeat music as an analytical lens onto midwifery prenatal care practices.
Watching and Listening to Fetuses
Visual productions of an embryo’s or a fetus’s beating heart, one of the first organs to develop in human organisms, are considered the most reliable early indication of pregnancy in both obstetric and public circles in high-income countries. In Germany, several weeks after gynecologists have visualized the fetus’s heart ultrasonographically, a handheld electronic device is used, often by midwives, to render the heartbeat audible via ultrasound. From then on, the fetal heartbeat is routinely monitored at every prenatal care visit 1 in order to check the “baby’s well-being in the womb” (Grivell et al. 2015, 2). Listening to fetal heartbeats is more common than is seeing fetal bodies in prenatal care in many parts of the world.
However, anthropologists have tended to study visual more than sonic monitoring technologies. Within the United States, feminists have argued that visual ultrasound technologies make fetuses appear as persons, entitled with individual statuses, rights, and interests (Petchesky 1987; Morgan and Michaels 1999; Mehaffy 2000; Mitchell 2001; Taylor 2008). Pregnant subjects thus hold a paradoxical position: they seem to vanish as subjects and instead become “uterine environments” (Duden 1999, 24) but are still held individually responsible for fetuses understood as their “children.” Petchesky and others have shown that “the visible fetus” has spilled over the borders of medical contexts: as “an autonomous, atomized mini-space hero” (Petchesky 1987, 271), “the fetus” has traveled to globalized publics and was incorporated in mass media, starring in movies, commercials, and also antiabortion campaigns (Taylor 2002, 367-68). The scholarly works from which this article takes inspiration show how these visual “representations” have helped the public to know and recognize “the fetus” and to relate emotionally and socially to the visual artifacts that are supposed to portray the fetus itself. But how do sonic fetuses emerge? How are fetuses perceived and appreciated in heartbeat monitoring done in midwifery prenatal care?
The few social-scientific analyses of fetal heartbeat monitoring focus on how fetuses are known biomedically: Cartwright (1998) shows how electronic fetal monitoring, and more specifically cardiotocography, shapes biomedical US childbirth practices through producing paper artifacts that represent the “physiological status” of woman and fetus. Interpreted by and acted upon by professionals, electronic fetal monitoring gives rise to “specialized knowledge,” Cartwright argues (1998, 241). Analyzing the use of a portable Doppler fetal monitor in Oaxaca, Mexico, Howes-Mischel (2016, 2017) demonstrates how—when medical doctors and pregnant women listen to heartbeats as well as to a doctor’s verbal cues—knowing a fetus medically becomes conflated with knowing a fetus as a socially present person. Owens (2017) has studied fetal heart rate monitoring in the United States in terms of a “risk counterculture” (p. 849): because “collecting information runs the risk of unnecessary intervention and possible harm” (p. 864), less intensive surveilling of the fetal heart rate is understood as a responsible act by care providers, she explains.
My material-semiotic analysis (Haraway 1991, 2004) adds to these lines of research by foregrounding the aesthetic dimensions of knowing fetuses through the production of their heart sounds in midwifery care. Using specific ethnographic cases of “fetal heart sound listening,” as the midwives I observed called it, I show how fetal heart sounds give rise to particular aesthetic, sensorial, and emotional appreciations of the objects of such listening: fetuses. These appreciations transform fetal heartbeat sounds into a kind of music. Introducing music as a methodological tool allows me to explore the aesthetic dimensions of obstetrical surveillance practices. I argue that how this music is produced and listened to qualifies fetal and pregnant lives as good or beautiful in both biological and social terms.
Stethoscopic Listening for Knowledge
Social-scientific interest in medical listening or “auscultating” 2 is not new. Foucault ([1963] 2003, 17, 164-70, 177-84) has argued that empirical medical knowledge and skills have been crafted through objectifying and classifying patients’ bodies acoustically. Next to seeing and touching, the practice of listening to bodies fueled medicine’s revolutionary turn to empirical rationalization in late 18th-century and early 19th-century Europe. What Foucault describes as a fundamental shift in the history of ideas was supported by a rather inconspicuous acoustic technology. According to R. T. H. Laennec, the founding father of auscultation, a rolled stack of papers preceded the stethoscope, the early version of which was a wooden cylindrical ear trumpet that helped to “mediate” between a doctor’s ear and a patient’s body (Lachmund 1999, 420; Sterne 2001, 117; Sterne 2003, 104; Rice 2010, 289).
Scholars of sound rooted in the history of science and science and technology studies (STS) have studied the stethoscope and its uses in further detail by investigating the “genealogy of auscultation” (Lachmund 1999, 420). They explain that a chest-seeing device 3 allowed the auscultation of breathing lungs and pumping hearts, hidden in patient’s chests and only rendered visible in autopsy. Through auscultation and dissection, bodies, specifically hearts, lungs, and gastrointestinal systems, were sensorially identified, categorized, and skillfully evidenced (Lachmund 1999, 424; Sterne 2003, 121-22). As a mediating instrument, 4 the stethoscope made it possible for medical doctors to take not only physical but also social and epistemic distance from their patients’ bodies. It thus helped to consolidate gender- and class-related differences between aspiring middle-class male doctors and hardworking yet poor female patients by privileging the truth and worth of the doctor’s access to his patient’s body as his empirical research object.
A modernist separation between subjects and objects was concretized through separating who knows (the savant doctor) and what is known (the patient’s body as physical evidence of disease; Sterne 2003, 113-20). Clinicians’ bodies became epistemic instruments, aspiring to coproduce “diagnostic objectivity” (Lachmund 1999, 441) when examining patients’ bodies. Concomitantly, patients’ voices became some of the many, formerly absent body sounds, which were then made present and diagnostically relevant (Sterne 2003, 116). Consonant with Foucault’s analysis, historical investigations into auscultation practices and their technological and cultural conditions have emphasized their contribution to standardizing and formalizing medical knowledge and skills (see Lachmund 1999, 423-29, 439-42; Sterne 2003, 101-16; Van Drie 2013, 167; Krebs and Van Drie 2014, 104; Harris and Van Drie 2015, 111-12; Volmar 2018).
Ethnographic studies of listening in contemporary medical environments have followed the argument that sounds produce expert knowledge and status (see Rice 2012, 2013, 2015; Harris and Van Drie 2015; Maslen 2015). 5 These studies take medical training situations, in which auscultative knowledges and skills are explicated, demonstrated, and exercised, as empirical examples. They argue that apprentices are trained to see the contemporary version of the stethoscope as the “hallmark of a doctor” (Rice 2010), whose ways and purposes of listening are directed toward generating knowledge. Listening analytically to “specific characteristics of sound” (Supper and Bijsterveld 2015, 133) serves the purpose of monitoring or diagnosing well-defined clinical signs (Supper and Bijsterveld 2015, 135; Bijsterveld 2018, 73).
In the field of sound studies, scholars have framed sonic approaches to bodies in medicine as “listening for knowledge” (Bijsterveld 2018, 3). These studies have been committed to escaping what Sterne (2003, 15) calls the “audiovisual litany.” According to Sterne (2003, 14), the juxtaposition of seeing and hearing, rooted in the Christian religion and commonly mobilized in “Western intellectual history,” elevates seeing to a technique of ultimate, exterior, and distant rationalization and relegates hearing to subjective and mundane interiors. To counter this, scholars have approached listening as a means for “acquiring knowledge about human bodies…or other research objects” (Bijsterveld 2018, 4). As a consequence, listening changed sides: instead of figuring as the opposite of knowing, listening has become a variant of seeing as knowing via objectification.
These works analyze how and under which conditions listening becomes a legitimate professional technique of knowing sound-producing entities. Sharing sound studies’ aim of overcoming essentialist and generalizing approaches to bodies and senses, I use the case of fetal heartbeat listening practices within midwifery prenatal care in Germany to show how listening to sounds leads to knowing a biophysical object through creating affective social relationships. Analyzing the listening to heart sounds as orchestrations that involve instruments, fetuses, pregnant women, and midwives, which together are coproducers, permits us to understand these practices as musical performances. The staging, producing, listening to, and indulging in sound creates a particular audience: parents and children, experts, and amateurs are all educated and drawn into the performance. As producer-listeners learn to know, or appreciate, the music, specific aesthetic experiences and social relationships are created (see Gomart and Hennion 1999; Hennion 2003, 2005, 2017).
Cultivating their appreciation of heartbeat music, the producer-listeners learn to be moved by “good sounds” (understood to indicate a healthy child) and to dread “bad sounds” or silences. Learning what sounds “beautiful,” they learn how to relate to what emerges, not only the coproducer of the music but also its product, a “healthy” and/or “docile child” as the object of listening.
Listening to Fetal Heartbeat Music
I build on the empirical ethical studies of technologies’ involvement in care practices led by Jeannette Pols and her colleagues (Pols 2012, 2013a, 2014, 2017a, 2017b; Pols and Moser 2009; Mol, Moser, and Pols 2010; Pols and Willems 2011; Van Hout, Pols, and Willems 2015; Ceci, Pols, and Purkis 2017) in my study of how ethical and aesthetic relations are crafted in fetal heartbeat listening. Pols (2014, 176) argues that care practices and their material-semiotic participants are “interrelational attempts” to achieve something good. 6 Care practices not only set out to know the problems of patients: they also strive for something good. But there is always a normative dimension to such knowing, and as such normative judgments cannot be separated from bodies and the sociomaterial relations from which they emerge. Care practices’ aesthetics thus consist of socially, technologically, and sensually produced appreciations, which emerge in a specific care practice oriented toward the “improvement” or stabilization of a patient’s situation (Pols 2017b, 423). Studying care practices in aesthetic terms involves demonstrating how and which kinds of relations oriented toward living well are shaped through the doings (in this case, listenings), which is a form of aesthetics of everyday life. When fetal heart sounds are produced in order to shape good fetal and pregnant lives in midwifery care, these lives are collectively qualified through listening to fetal heartbeats in specific ways.
With these theoretical repertoires, I respond to the following questions: How may we understand fetal heartbeat listening practices as aesthetic, and more specifically, as musical orchestrations? How do sonic monitoring technologies become instruments? How are the positions of the audience, director, and listening object distributed among the participants, the fetuses, the pregnant women, and the midwives?
Methodological Approach
Between February 2015 and March 2016, I accompanied pregnant and birthing women and midwives and observed their interactions in two hospitals, two midwife-led birthing places, an ob-gyn practice, and numerous private homes in Germany. I attended fifty prenatal care visits, thirty births, and fifty home visits to postpartum women, and I conducted twenty semi-structured interviews with midwives and women and held many other informal conversations. Initiating the interviews with a question such as: “What happened in this prenatal care situation?” allowed me to explore my interlocutors’ understanding, and evaluation, of a situation. Answering this question, my interlocutors addressed the practicalities of the midwifery care events I had witnessed earlier: what was done, how, why/what for, and with which effects, thereby becoming their own praxiographers (see Mol 2002, 15). I brought my observations of midwifery practices and the accounts of my interviewees together in order to analyze them thematically. By comparing and contrasting different midwifery care arrangements, what their participants did and became, and the values realized therein, I identified relevant and interesting practices.
In their prenatal care, midwives used three devices to listen to fetal heart sounds. Two electronic devices audibly simulate the fetal heartbeat: the portable Doppler fetal monitor and the cardiotocograph (CTG 7 ). The third instrument, which resembles the historic stethoscope, is called “fetoscope” or, more commonly, the “Pinard horn,” named after the French obstetrician Adolphe Pinard.
Below, I compare three fetal heartbeat listening situations in which these different instruments produced fetal heart sounds in distinct ways, helping to give rise to particular care orchestrations. These situations are specific and yet exemplary: I have witnessed numerous situations very similar to the ones described below. Locating these practices “somewhere in particular” (Haraway 1999, 182), I also show how professional discourses present in midwifery and obstetric textbooks affect the prenatal care practices I describe.
Educating Parental Ears
The Doppler fetal monitors, called “Doptones,” I encountered at my field sites were composed of a wired transducer and the device itself. The transducer is held to the woman’s belly with one hand while the device, equipped with a small electronic display and a loudspeaker, is held in the other. The Doptone is a practical and user-friendly device: hand-sized, it is easy to transport and handle; battery-run, it does not depend on electricity. Doptones record the fetal heartbeat via ultrasound, produce sounds acoustically, and make them audible to everyone in hearing distance through an integrated loudspeaker. 8 These devices were used in both midwife-led and obstetrical surroundings (Figure 1; Online Supplemental Sound File A [Doptone]). The following excerpt from my field notes describes its use in a midwife-led birthing place, in which Doptones were most commonly used for listening to fetal heartbeats throughout pregnancy and birth.
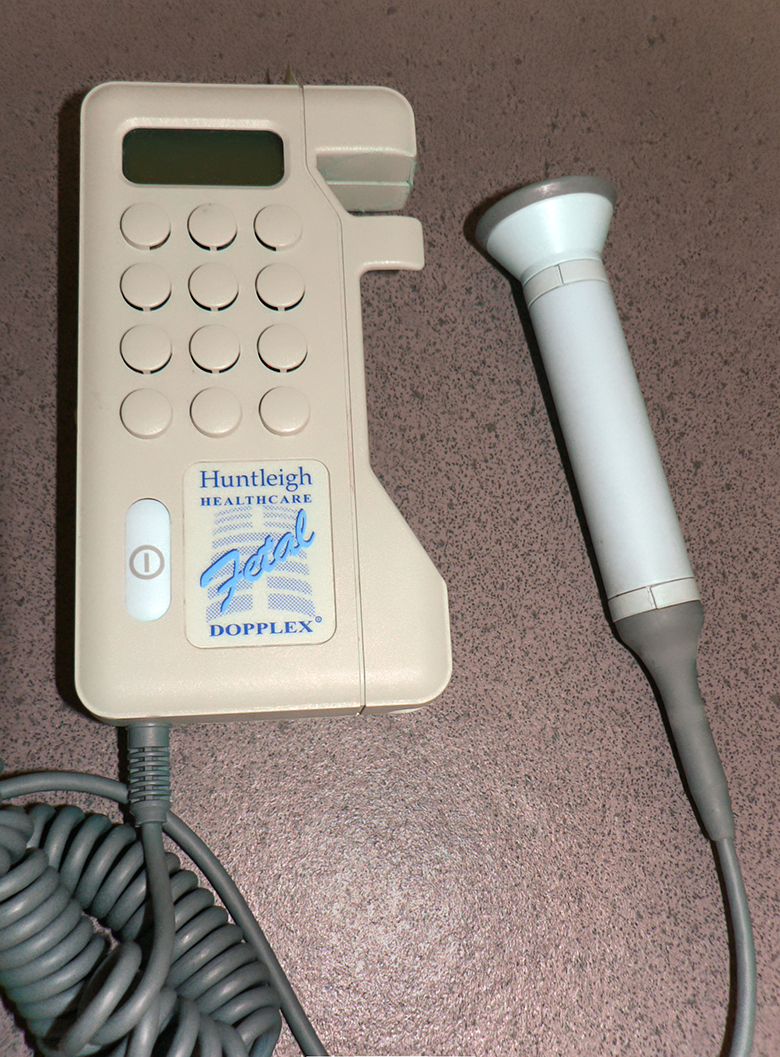
Doptone. Source: By Harmid—own work, Public Domain (https://commons.wikimedia.org/wiki/File:Doptone.jpg).
{kind=link}
When the moment for listening to the fetal heartbeats comes, Karen seems excited. Her belly undressed, she is lying down on the couch while midwife Julia kneels next to her on the ground. Julia rubs her hands and places them on Karen’s belly: “Hello child, how are you doing?” After having palpated Karen’s belly to determine the fetus’s position in Karen’s belly, Julia grabs the Doptone, applies some ultrasound gel to the transducer, and turns on the device. Now taking a seat next to Karen on the couch, she holds the transducer to Karen’s left groin area. We hear a loud crackling tone. Julia moves the transducer several centimeters towards Karen’s navel and a dull electronic beating begins to sound. The beating becomes louder and louder as Julia presses the transducer firmly against Karen’s belly until a steady thumping fills the room. “Oh! That is really fast,” Karen smiles, looking surprised at the device in Julia’s hand. “Yes, it is,” Julia replies, “like a small galloping horse [ein galoppierendes Pferdchen].” We continue listening for a while until Julia turns it off. “Your child is doing really well in your belly,” Julia concludes, in a pleased tone of voice.
Before listening, midwife Julia touches Karen’s belly to make contact with the fetus and determine its position. Julia carries out the so-called Leopold’s maneuvers, named after the German gynecologist and midwifery teacher Christian Gerhard Leopold, in order to figure out where, approximately at least, to place the transducer, so that it produces audible fetal heart sounds. 9 Midwives and obstetricians learn to differentiate between the fast stamping of a fetal heartbeat and a whooshing, a “vascular soufflé produced by uterine as well as fetal vessels” (Gibb and Arulkumaran 2017, 23). Distinguishing maternal from fetal heart rate patterns, in a babble of similar sounds, is crucial for avoiding false interpretations and unnecessary interventions. The listening instrument needs to produce specific sounds that can be valued distinctly. But the audible heart sounds and their evocative verbal coenactment 10 add further possibilities for relating to what we, as a collective of listeners, hear and for concretizing the object of listening. The sounds are announced as fetal “heartbeats” and the object of listening is directly addressed, verbally and haptically, as “the child.” We thus are equipped with particular genres of knowing that guide our attentive listening: the listeners enter a shared acoustic space filled with fetal heart sounds that tell them how the child is doing.
While how to listen and what to listen to are framed and directed beforehand, they take concrete shape in the shared sensorial practice. Karen, who is joyfully committing to the listening procedure, hears these sounds for the first time. She is drawn into listening attentively and cannot but respond spontaneously to what she has been prepared for and is looking forward to hear. The sounds and scratches, followed by a fast and monotonous rhythm, are perhaps different from what Karen expected, as she comments that they are “really fast.” But what do “really fast” heartbeats mean or stand for? The implicit reference to a much slower adult’s heart rate, such as Karen’s own, is appropriate and relevant for the obstetrical surveillance of the fetal heartbeat in pregnancy, relying on different standards of normal heart rates for fetuses and adults. In obstetrical terms, “good” fetal heartbeats are “really fast” in comparison to the resting heart rate of an adult. However, in this situation, “fast” heartbeats are not only a medical state, called tachycardia. Their rhythmic sound makes Karen smile and the midwife’s voice sound pleased. It shows that the “child is doing really well” in Karen’s belly, as the midwife says. As aesthetic artifacts, these heartbeats are attributed with a “connotative, associative-affective character” (Tagg 1987, 282) and, thereby, become socioemotional expressions and symbolic communication (Tagg 1987, 285). 11 We learn to listen to “good” heartbeat music and thereby to a fetus we jointly get to know and relate to as a “healthy child,” cultivating our listening as a “sonic skill” (Bijsterveld 2018). 12
The obstetrical, and aesthetic, metaphor Julia introduces for specifying “fast” heartbeats—sounding “like a small galloping horse”—renders the different interrelated significations of fetal heart sounds evident. Listening to fetal heartbeat music, we learn to be moved by the vigorous and lively sounds we are surrounded by and attached to. When the midwife suggests that the fetal sounds are like those of a “small galloping horse” and that they signify that “the child is doing really well,” she suggests a way of not merely knowing through listening but of feeling sensorially and emotionally. The diagnostic, aesthetic, and social meanings of the heartbeat music produced enact the fetus as a “small galloping horse” that is sounding, moving, and living vigorously and boisterously amongst us. We learn to listen to the fetus in a way to hear Karen’s “child…doing really well” in its element or natural habitat, Karen’s “belly.” The music produced by the Doptone does not merely help to realize the fetus as Karen’s child but also recognizes the child’s existence and its environmental, consisting of its social and biological, conditions for living well.
One of the most popular German alternative birthing manuals, written by a midwife, suggests that fetal heartbeat listening via Doptone is a way to not only check the fetal heart rate but also to train for parenting. Through it, parents learn to become attentive to children’s aural expressions: “Listening to the fetal heart sounds, I can point out to parents that also their ears need to prepare themselves for becoming parents” (Beim Hören der kindlichen Herztöne kann ich die Eltern gleich darauf hinweisen, dass auch ihre Ohren sich auf das Elternwerden vorbereiten müssen; Stadelmann 2005, 29-30). In many of the Doptone orchestrations I witnessed, the future parents were educated in how to listen to fetal heart sounds that were beautiful and good in social terms. Rather than drawing on a widely shared familiarity with human heart sounds as symbols of life and emotions, especially love (Rice 2012, 305; Howes-Mischel 2016, 196), the sonic enactments of “a child” stage the fetus as a fragile and dependent social being who must be loved and cared for in order to thrive.
Creating a Midwifery Art
The midwife-led birthing center where Agnes works is equipped with all three fetal heartbeat monitoring devices that are used in prenatal care: Doptones, Pinard horns (Figure 2), and CTGs. While the CTGs mostly gathered dust in a corner of the room, the Doptones and Pinard horns were used on a daily basis and thus kept within view and reach. Especially when evaluating women further along in pregnancy, midwife Agnes likes to use her Pinard horn, a simple and cheap but elegant device that resembles a wooden champagne flute.

Pinard horn. Source: By Dr. Slow Decay—own work, Public Domain (https://commons.wikimedia.org/wiki/File:Pinard-Rohr.jpg).
{kind=link}
Midwife Agnes suggests concluding the prenatal care visit by “hearkening to the heart sounds” [nach den Herztönen horchen]. Ramona agrees. She lifts her blouse and lies down on the couch. In order to “make it more comfortable,” midwife Agnes stuffs a pillow under Ramona’s knees. Kneeling next to Ramona, she rubs her hands, and places them on Ramona’s belly. “Let’s see if it says ‘Hello,’” Agnes says expectantly. Ramona, holding her blouse and fixing her gaze on the ceiling, nods. Agnes presses the edges of her hands onto Ramona’s belly midway between the costal arch and the navel. Then she moves her hands to the sides of Ramona’s belly and pushes them forcefully towards each other. “The child lies on the right side, head downwards,” Agnes looks up to Ramona. “Tell me if it becomes too much for you and if you cannot lie on your back any longer.” She grabs her Pinard horn and places it between Ramona’s navel and her right groin. Leaning forward, Agnes puts her ear on the earpiece, takes her hand off and listens. Ramona is lying still, breathing shallowly. Agnes moves the horn several centimeters to the left, listens. Then, she moves it downwards, presses the horn more forcefully on Ramona’s belly, so that it seems to sink into the belly, and listens again. After a long silent minute, Agnes grabs the horn, and lifts her head: “Today, I get both of you [Heute kriege ich euch beide].”
The Pinard horn amplifies body sounds but is less “sensitive” than the Doppler ultrasound transducer. In order to “hearken to the fetal heart sounds” with the Pinard horn, to master the technique of auscultating, several conditions need to be met: clinical palpation and auscultation skills are as indispensable as anatomical and physiological knowledge. The fetus’s position in the belly has to be detected as precisely as possible via touch and the midwife needs to be familiar with how and what to “hearken to.” As a rule of thumb, the listening midwife can hear the fetus’s heart beating loudly and clearly, if the instrument is placed as close as possible to the fetus’s back, at heart level. When this spot is found, the heart sounds need to be differentiated from the babble of abdominal sounds, and especially from the pulse of the so-called maternal blood vessels, so that the tool renders audible what is listened to and known as fetal heart sounds. 13
Furthermore, the surroundings—and all the participants, except the listened-to fetus—must keep quiet. Only one of the midwife’s ears is able to listen to the child-in-the-belly, while the other ear is directed upward and opens up toward the room and Ramona. Other sounds than the valuable heartbeat music become “external” and, as such, undesirable; they become disturbing ambient noise in the listening situation. For Agnes to auscultate, Ramona needs to become a patient in its literal and practical sense: she needs to “endure,” to cooperate by permitting and adapting to Agnes’s touching, listening, and talking intervention. Ramona is not allowed to talk, except to say if it “becomes too much” to lie motionlessly on her back, an uncomfortable position that is hard to hold in advanced pregnancies. Her own ways of sensing and knowing “the child” are not part of the listening situation. 14 Ramona may (learn how to) feel the fetus moving in reaction to her excitement, to voices, to Agnes’s touch, and to the pressure exerted on her belly when the Pinard horn is used. However, she cannot feel, hear, or appreciate “the child” the way Agnes does when feeling with her hands and listening with the Pinard horn.
The instrument and how it orchestrates the listening create several divides as they separate out body sounds, distinguishing between the silent and meaningless outside of Ramona’s bounded body and its sonorous and significant inside hosting an unseen fetus. The midwife’s body becomes an extension of the instrument that produces and conveys the fetal heartbeat music from the inside of Ramona’s belly directly and exclusively into the midwife’s ear. As (part of) an instrument, the midwife’s body is spatially close to Ramona’s and the fetus’s bodies, 15 yet distant in regard to its perceptual, epistemic, and aesthetic possibilities. The midwife is staged as the expert-artist who seemingly produces the music on her own while also being the only one able to appreciate that exclusive artifact. Ramona is surrounded by a silence that she (must) coproduce, left to listen to Agnes’s words translating or, more precisely, enacting, the touching and listening objects: Ramona’s body and the child in her belly. Ramona laboriously contributes to bringing about, in strikingly present absence, the heartbeat music and its significations but cannot perceive and appreciate the music herself. Her attention and curiosity, raised by the music she cannot hear as a sign of the fetus she cannot see, are directed toward Agnes’s body, which has privileged access. The Pinard horn orchestration thus grants the midwife the professional authority to bring about, to feel, and to know fetal heartbeat music as a mysterious manifestation of a child in Ramona’s belly, hidden not only from sight but also from hearing. In doing so, the midwife becomes the creator of and the mediator between a fetus’s and a pregnant person’s body, as is illustrated by Agnes’s words: “Today, I get both of you.”
Pinard horns are mainly used in so-called extra-clinical, midwife-led environments, and mostly, if not exclusively, by midwives. They have attained an iconic status in these environments, which are often considered nonmedicalized alternatives to obstetric settings and as such especially “social” (Skeide 2019). Ironically, however, Pinard horns are classic medical tools, developed and initially used by obstetricians to establish and keep physical and social distance from patients’ bodies. It seems that what the stethoscope is to the medical profession today, the fetoscope is to independently working midwives in Germany: it helps to enact identity and belonging and is a symbol of, and tool for, midwives’ knowledgeable craftwork and expertise (see Rice 2010, 300; Harris and Van Drie 2015, 111). Producing fetal heartbeat music with the help of the Pinard horn provides the sociomaterial, epistemological, and aesthetic conditions for bringing about what has been called—often in opposition or in addition to science—the art of midwifery (Kennedy, Anderson, and Leap 2010). The Pinard horn helps to orchestrate midwifery care situations, in which midwives are staged as instrumentalists who develop, use, and refine knowledge repertoires and sets of skills that are highly specialized and demand continuous (clinical) practice in order to produce esoteric heartbeat music.
Beautiful Evidence
CTGs are machines of the size of small home printers, and, as they are rather cumbersome, they are placed on trolleys. These CTG trolleys stand next to a cot or bed; a pregnant woman lies down, two wired transducers are attached to her belly with two large rubber straps, and the CTG registers the fetal heartbeat via Doppler ultrasound and measures, if necessary, the frequency of uterine contractions as tensions of the abdominal wall. 16 Next to widely audible sounds, CTGs produce another, documentary, artifact: they transcribe the fetal heart rate as a jagged curve on scaled paper, which is printed out simultaneously with the recording (Figure 3; Online Supplemental Sound File B [Cardiotocograph]).
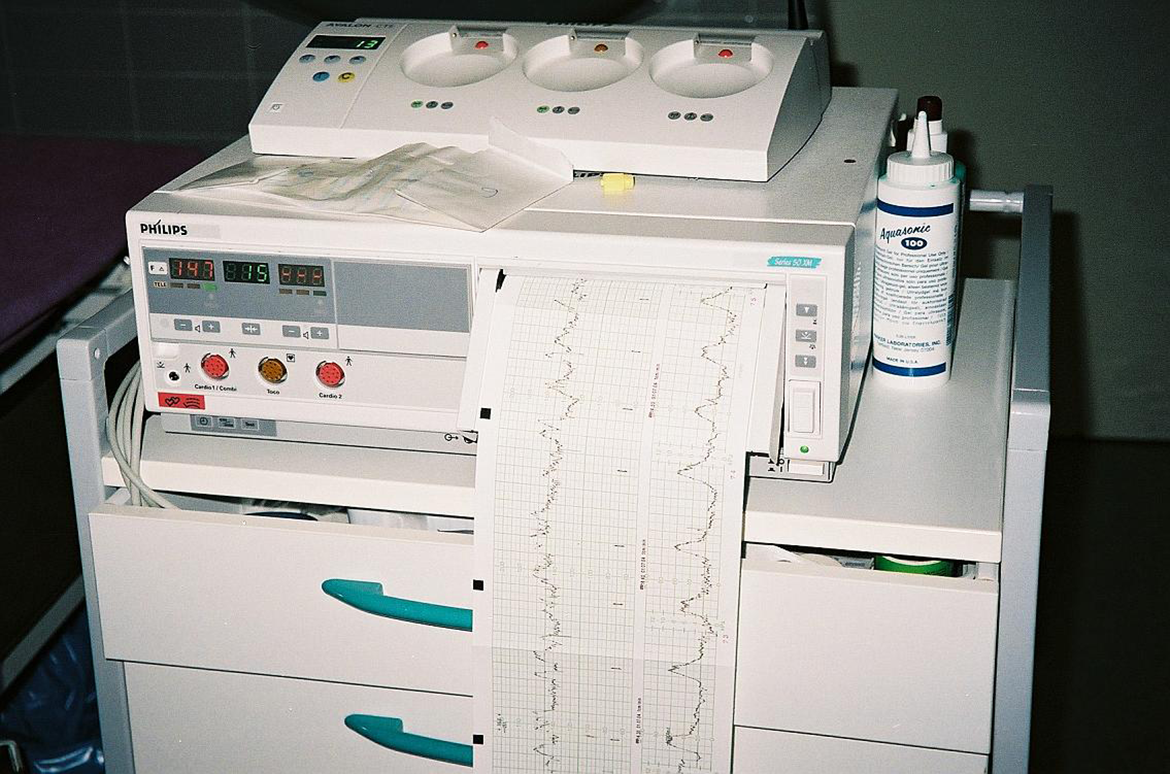
Cardiotocograph. Source: By Jojo—own work, Creative Commons Attribution–ShareAlike 3.0 Unported license (https://commons.wikimedia.org/wiki/File:Kardiotokograf.jpeg).
{kind=link}
It is common, at least in early pregnancies, to use Doptones for fetal heartbeat listening, not only in midwife-led environments but also in ob-gyn practices, where most women are attended to during pregnancy in Germany. Then, from around the twenty-sixth week of pregnancy on, CTGs are used, even though their use is medically indicated only for specific, potentially pathological events, such as preterm labor. 17 Obstetricians as well as midwifery and public health researchers emphasize that this practice is problematic. This is because CTG recordings are no more than “snapshots” whose predictive value is quite limited. While CTG scripts thus may serve as juridical and medical evidence for fetal well-being at the time of assessment (Grivell et al. 2015, 1), the midwives I observed insisted that any (re)assurance that CTGs may provide pregnant women is based on a “false faith,” as the registered heartbeat cannot guarantee fetal well-being in the future. The scripts are used for justifying obstetrical surveillance of fetal well-being and for proving that suitable obstetric measures have been taken in situations in which a “good” fetal health state is doubted or appears “bad.” 18 Without indications, CTGs in pregnancy are unnecessary and potentially harmful interventions that, in addition, facilitate further unnecessary and potentially harmful interventions (Deutsche Gesellschaft für Gynäkologie und Geburtshilfe 2012, 7; Schäfers and Kolip 2015, 6). 19
Midwife Vera, who provides prenatal care in cooperation with an obstetrician in her ob-gyn practice two days per week, shares these concerns with most of her colleagues. Vera thinks that monitoring the fetal heartbeat works better with a Doptone and that “CTGs are mostly unnecessary.” However, she also emphasized that pregnant women “expect to get CTGs” as much as they demand fetal ultrasound.
In the prenatal care I witnessed in ob-gyn practices, the situation turned out to be more complicated than that. While many women, such as Jenny, thought of the CTG as a “necessary evil” that needed to be done in order to “assure that the child is doing well,” others, such as Anna, happily anticipated it. It was “the best part of the prenatal care visit,” Anna told me. As part of rather hasty prenatal care visits—Vera spent half an hour on the entire prenatal exam—the CTG ran for twenty minutes. During that period of time, Anna was on her own in the prenatal care room. Lying on a cot, equipped with a pillow under her cheek and between her legs, the heartbeat listening was her occasion to relax, to doze off even, while being lulled by the steady and soft beating of “the child’s heart,” “the loveliest music to my ears [die schönste Musik in meinen Ohren],” as she put it. Bathing in the heartbeat music the CTG produced, Anna learned to appreciate the intimate, acoustic, one-to-one-encounter with “the child” that the heart sounds provided. The orchestration was limited to this time and place, while also projecting a reassuring, comfortable, and “lovely” relationship to a fetus as “her child.”
For the midwives, however, the CTG produced different, namely medical and juridical, values. For them, “beautiful CTGs [schöne CTGs]” (scripts) were much more important than beautiful heart sounds. As “snapshots,” these papers can prove the fetus’s state of health at a certain moment in time. However, their durable materiality and the visibility of the data they provide also bestow them with a probative force that exceeds the “captured” moment. A panoply of inventive strategies was applied in order to craft “beautiful” scripts depicting a “good” fetal heart rate in the form of a continuous curve running within the ideal range and showing the variations defined as normal (see endnote 19). The coproduced ephemeral sounds often lost their epistemic value in favor of the produced “good,” durable, and “hard” facts, which were often a laborious venture for all participants to create.
One of the requirements for crafting a “beautiful” CTG was to get a clear and continuous signal while recording. In order to achieve that, the transducer sometimes needed to be pressed firmly against the belly. It could become necessary to do so throughout the recording, often by the pregnant woman herself. If “the child does not like the CTG,” as Vera said, and “moved away,” the transducer was moved to other spots on the belly in order to “catch the child,” as Vera put it, and thereby get a continuous curve. Another trick was for the pregnant woman to turn around and to position the transducer on the other side of the belly. If the heart rate curve was either wide or flat—read as signs of an “overly active” fetus or a fetus that “takes a rest” or “sleeps”—Vera tried “to wake it up” by clapping her hands or wiggling the woman’s belly. Sometimes, however, nothing helped. In these cases, Vera suggested trying again some hours later or the next day in the hope that it would work better then.
Aesthetics of Fetal Heart Sound Listening Situations
When fetal heartbeats were monitored in these midwifery prenatal care situations, sounds were produced that helped to know (about) the fetuses, and the music was played that could be appreciated for its affective and associative qualities. Fetal heartbeat music emerged from particular orchestrations, including specific instruments that helped to make distinct kinds of music.
In all three situations, the participants actively engaged in shaping the listening procedures. The situated aesthetic artifacts brought about—the fetal heartbeat music and the CTG scripts—are both material-semiotic coproductions and coactors. And so are the fetuses whose social lives are valued through their fetal heart sounds and music, which are, interrelatedly, made to signify and to prove their well-being.
When the Doptone produced sounds audible to everyone in the vicinity, the aesthetic togetherness of the participants—Karen, the child-in-the-belly, and midwife Julia—revolved around teaching the mother-to-be how to listen to what emerged as fetal heartbeat music. The heartbeat music was evoked as the sign of a healthy child in need of obstetrical surveillance and parental care and love. In the Doptone orchestration, this cooperation in making fetal heartbeat music was rewarded by the music becoming audible, understandable, and appreciable to Karen as well.
When the Pinard horn was used to produce fetal heartbeat music, the midwife alone could listen to and make sense of it, a situation that bestowed on the midwife interpretative authority by excluding how and what the pregnant woman heard and felt. The instrument produced esoteric music for initiated ears that have access to unseen worlds, the fetus-in-the-belly. In this orchestration, the midwife became the key figure, whose appreciations of the heartbeat music were the sole or predominant concern.
The heartbeat music produced by the CTG was as an aesthetic artifact, valued by Anna as soothing background music, part of a relaxing and pleasing situation that contributed to her well-being through building and concretizing a reassuring and “beautiful” relationship with “her child.” Midwife Vera’s aesthetic appreciation was, in contrast, directed toward creating a “beautiful” CTG script. This script could also be understood as musical notations, a visual version of the music “played” via the CTG. Similar to the music made by the Pinard horn, CTG scripts were only to be appreciated by knowledgeable and skilled experts.
Who or what knows fetal heart sounds? Who appreciates fetal heartbeat music in which ways? Which kinds of sounds and objects of listening can be known and appreciated? The answers to these questions partly differ and partly overlap in the three orchestrations I described. In all three cases, however, knowing and appreciating cannot be separated but need to be understood as intertwined practices.
Conclusion
The three monitoring technologies, the Doptone, the Pinard horn, and the CTG, differ in their respective ways of playing fetal heartbeat music. The Doptone groups the pregnant woman as the audience, the midwife as the director, and the fetus as the listening object closely together around tunes that are audible for everyone present. The Pinard horn affords even greater bodily proximity of the audience, director, and listening object but grants the midwife the privilege of combining director and audience positions while shaping both the pregnant woman and fetus into listening objects. Considering the affinity, this instrument engenders especially within independently working midwifery circles, who define their work in contrast to medical approaches as particularly “social,” it is surprising to realize that it is the instrument with the most encompassing objectifying effects. The CTG is the only instrument that allows for the directing midwife to be absent once the instrument plays and sounds well, thereby permitting early intimate encounters between future parents and their children. As the CTG is the only instrument that allows for producing artifacts that are also of medical and juridical value, their “social” potentials are widely neglected, though erroneously, as this analysis shows.
Medical researchers seeking to produce evidence through randomized controlled trials have studied these different fetal heartbeat monitoring devices, comparing their effects in relation to prenatal and perinatal health outcomes. Tracing the aesthetic relations that are built into fetal heart sound-producing and listening practices reveals how biological or obstetrical facts are based on what the different care participants are moved by, what they hold dear and find important, and what they appreciate aesthetically. Thinking with music when analyzing the effects of these different instruments makes clear that they shape very different relationships among the various participants. This relational analysis shows that good fetal heart rates, both sonically and visually produced, belong to a genre not only of facts but also of appreciating and of valuing sounds aesthetically, a way of interpreting sound that used to be reserved for musical practices. The confines of “accepted ‘normal’ limits for fetal heart rate parameters” (Grivell et al. 2015, 7) are affective, interpretative, and relational achievements. Concurrently, knowing a fetus cannot be separated from relating to a lovable, fragile, or unruly child as a material and sensual product of attentive and guided listening and its associated activities. When fetal heartbeat music is appreciated as sonic sign for a child in need of love, care, and obstetric surveillance, “relations that are aesthetically pleasing or good” (Pols 2017b, 423) are created. This necessarily broadens the study of sound in various practices, allowing us to better hear how well-beings are shaped in midwifery prenatal care.
Supplemental Material
Supplemental Material, sj-pdf-1-sth-10.1177_01622439211005176 - Music to My Ears: A Material-semiotic Analysis of Fetal Heart Sounds in Midwifery Prenatal Care
Supplemental Material, sj-pdf-1-sth-10.1177_01622439211005176 for Music to My Ears: A Material-semiotic Analysis of Fetal Heart Sounds in Midwifery Prenatal Care by Annekatrin Skeide in Science, Technology, & Human Values
Supplemental Material
Supplemental Material, sj-wav-1-sth-10.1177_01622439211005176 - Music to My Ears: A Material-semiotic Analysis of Fetal Heart Sounds in Midwifery Prenatal Care
Supplemental Material, sj-wav-1-sth-10.1177_01622439211005176 for Music to My Ears: A Material-semiotic Analysis of Fetal Heart Sounds in Midwifery Prenatal Care by Annekatrin Skeide in Science, Technology, & Human Values
Supplemental Material
Supplemental Material, sj-wav-2-sth-10.1177_01622439211005176 - Music to My Ears: A Material-semiotic Analysis of Fetal Heart Sounds in Midwifery Prenatal Care
Supplemental Material, sj-wav-2-sth-10.1177_01622439211005176 for Music to My Ears: A Material-semiotic Analysis of Fetal Heart Sounds in Midwifery Prenatal Care by Annekatrin Skeide in Science, Technology, & Human Values
Footnotes
Acknowledgments
I would like to thank the pregnant people and midwives who taught me how to listen to fetal heartbeat music. Thanks to the reviewers whose responses helped me to sharpen my arguments as best I could—for now at least. I dedicate this paper to Jeannette Pols.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
The supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.