
Abstract
The accident at Fukushima Daiichi nuclear power plant occurred following the huge tsunami and earthquake of 11 March 2011. After the accident, there was considerable uncertainty and concern about the health effects of radiation. In this difficult situation, emergency responses, including large-scale evacuation, were implemented. The Fukushima Health Management Survey (FHMS) was initiated 3 months after the accident. The primary purposes of FHMS were to monitor the long-term health of residents, promote their well-being, and monitor any health effects related to long-term, low-dose radiation exposure. Despite the severity of the Fukushima accident and the huge impact of the natural disaster, radiation exposure of the public was very low. However, there were other serious health problems, including deaths during evacuation, increased mortality among displaced elderly people, mental health and lifestyle-related health problems, and social issues after the accident. The Nuclear Emergency Situations – Improvement of Medical and Health Surveillance (SHAMISEN) project, funded by the Open Project For European Radiation Research Area, aimed to develop recommendations for medical and health surveillance of populations affected by previous and future radiation accidents. This paper briefly introduces the points that have been learned from the Fukushima accident from the perspective of SHAMISEN recommendations.
1. INTRODUCTION
The accident at Fukushima Daiichi nuclear power plant occurred as a result of the huge earthquake and tsunami of 11 March 2011. After the accident, there was considerable uncertainty and concern about the health effects of radiation. In that extreme situation, emergency responses (including large-scale evacuation) were implemented. Three months after the accident, Fukushima Prefectural Government decided to undertake the Fukushima Health Management Survey (FHMS). The primary purposes of FHMS were monitoring the long-term health of residents, promoting their well-being, and monitoring any health effects related to long-term, low-dose radiation exposure (Yasumura et al., 2012). The survey consisted of two major components: the basic survey and the detailed survey. The basic survey estimated the external radiation exposure of all 2 million residents of Fukushima Prefecture. The detailed survey comprised four surveys: a thyroid ultrasound examination (360,000 children aged < 18 years); comprehensive health check (210,000 residents of evacuation areas); mental health and lifestyle survey (210,000 residents of evacuation areas); and pregnancy and birth survey (16,000 pregnant mothers in Fukushima) (Fig. 1).
Fukushima Health Management Survey (Yasumura et al., 2012).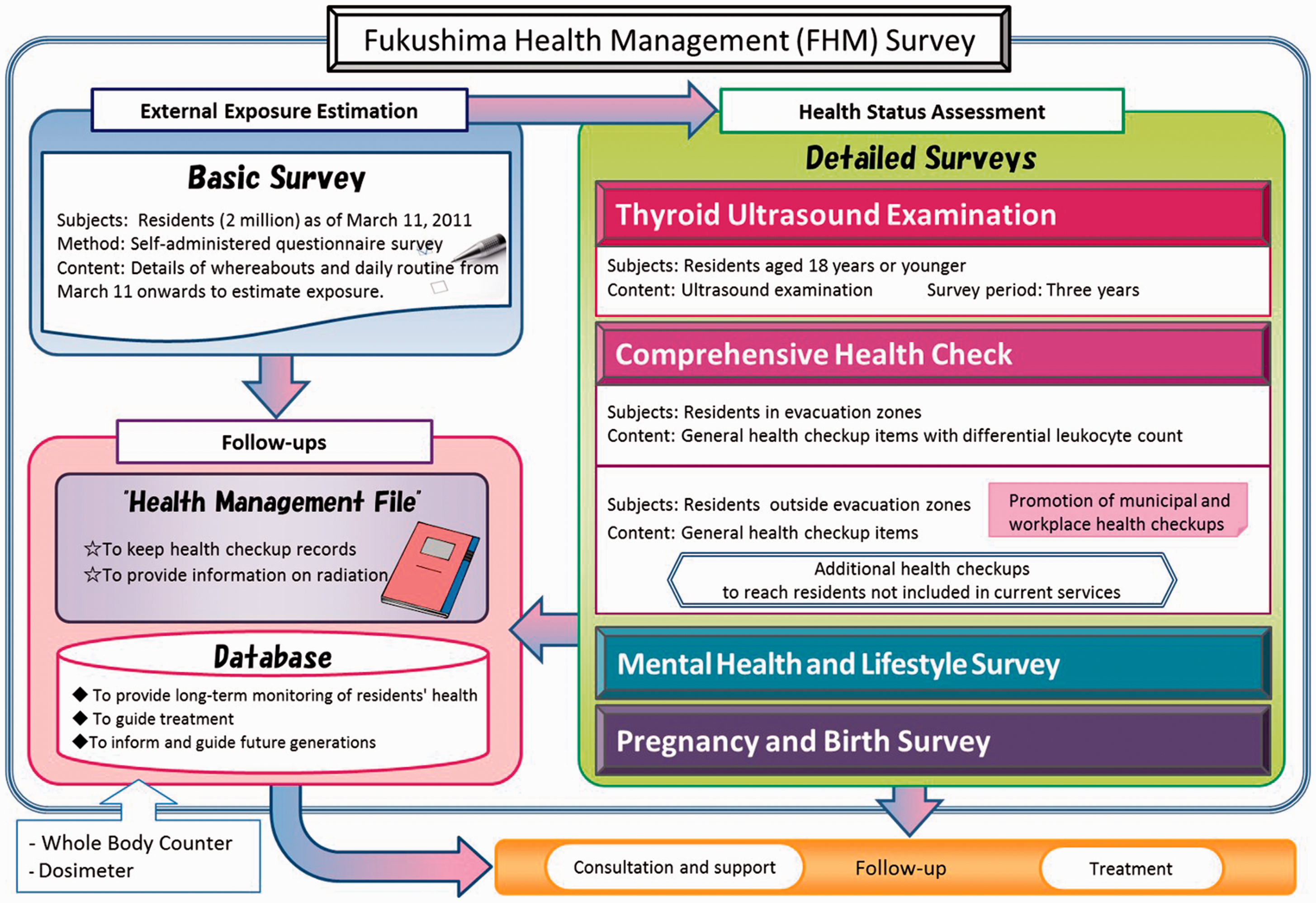
Following the experiences of the populations affected by Chernobyl, Fukushima, and other radiation accidents, the Nuclear Emergency Situations – Improvement of Medical and Health Surveillance (SHAMISEN) project was launched, funded by the Open Project For European Radiation Research Area (SHAMISEN, 2017). The purpose of SHAMISEN is to develop recommendations for medical and health surveillance of populations affected by previous and future radiation accidents. This paper will briefly introduce what has been learned from the Fukushima accident from the perspective of SHAMISEN recommendations.
2. RESPONSES IMMEDIATELY AFTER THE ACCIDENT
2.1. Communication to the public
After the nuclear accident in Fukushima, uncertainty over its extent and gravity resulted in vacillating responses and contradictory statements made by administrative authorities, plant operators, and scientists. Recent advances in information and communications technology resulted in the transfer of tremendous quantities of information via various media regarding the accident (Friedman, 2011). This information provided opportunities for people across the world to learn about the ongoing situation; however, it also created problems due to anxiety and incorrect explanations. The lack of initial information accelerated public anxiety, and the situation was exacerbated by the lack of journalists with specialised knowledge, which led to the proliferation of inaccurate information. Restrictions on information disclosure by the authorities resulted in public distrust. In this disordered situation, experts in radiological emergencies often appeared in various media, and they undertook the role of risk and crisis communication. The scientific messages they conveyed were based on accumulated evidence from atomic bombing victims in Hiroshima and Nagasaki, as well as from the Chernobyl accident; their statements played a significant role in enhancing public understanding about the impacts of the accident on health. However, their statements also exposed the experts to unexpected criticism, and drew the attention of various citizens’ groups (Fukushima Nuclear Power Plant Accident Plaintiff Group, 2011). Following the Fukushima accident, risk and crisis communication to the public arose as an important issue that demanded the involvement of experts in radiological emergencies.
SHAMISEN states that nuclear accident preparedness protocols need to include strategies for crisis communication and risk communication. These strategies should identify in advance who will provide information to decision makers, how this flow of information to and from local and national authorities will be coordinated, and what channels will be used to communicate such information to the public (SHAMISEN, 2017). Experts have to be trained to acknowledge and convey possible differences in opinion, as well as the uncertainties associated with any emergency situation.
2.2. Radiological protection for the public
In response to the accident, the Japanese Government issued a series of emergency evacuation orders between 11 and 13 March 2011 to residents living within a radius of 3, 10, and 20 km of Fukushima Daiichi nuclear power plant. Over 97% of residents living within a 20-km radius had been evacuated by 15 March 2011, when the largest radioactive plume was released (Hayano and Adachi, 2013). In the early stages following the accident, there was confusion regarding whether residents needed to take stable iodine tablets; the confusion was due to a complicated administrative procedure and disrupted communication. Other protective measures by the Japanese Government included strict control over local food and water consumption, and modification of behavioural patterns (avoidance of outdoor activities); these were implemented mainly at the discretion of local residents.
Radiological protection for the public in Fukushima was achieved mainly through the above measures. However, several criticisms were raised (Ohtsuru et al., 2015). First, no designated locations for evacuees outside the 10-km zone were assigned in the plans. Accordingly, over 20% of evacuees had to relocate at least seven times as the evacuation zone expanded. Second, evacuated residents lacked sufficient information about radiation levels and the evacuation procedure. They had no information about how to make preparations, and no advice or instructions on how to protect themselves or for how long they would have to vacate their homes. Third, the evacuation shelters were located north-west of Fukushima Daiichi nuclear power plant, where high levels of radioactive deposition were recorded. This situation mainly arose because of a lack of adequate plans, insufficient information on radiation levels, communication disruption, and loss of function of the local nuclear emergency response headquarters at the off-site centre (Ohtsuru et al., 2015).
Emergency evacuation of hospitals and nursing care facilities was accompanied by life-threatening problems. At the time of the accident, there were more than 2200 patients or elderly people at nursing care facilities within a 20-km radius of Fukushima Daiichi nuclear power plant (Tanigawa et al., 2012). Most of the individuals in that zone were transported by defence force helicopters or charted buses to shelters in Fukushima Prefecture by 15 March 2011. No medical personnel were in attendance during or after the evacuation, and no care, medicine, or food and water were provided. Once the patients and elderly people reached the shelters, no appropriate medical care was available. Due to concerns about possible radiological contamination, significant difficulties were encountered in finding facilities that would accept these individuals. During or soon after evacuation, more than 50 inpatients and elderly people at nursing facilities died. Hypothermia, deterioration of underlying medical problems, and dehydration were suspected as the causes of death. Lack of medical support before, during, and after the evacuation was regarded as the major reason for evacuation-related loss of life. This experience underscores the danger of unprepared evacuation for populations with special needs (Tanigawa et al., 2012).
SHAMISEN states that plans need to identify individuals who are vulnerable to radiation (e.g. pregnant women, children), those requiring special care (e.g. patients, nursing home residents, people with disabilities), and those with unique needs (e.g. prison inmates) (SHAMISEN, 2017). Plans and arrangements for evacuation should include evacuation routes, means of transport, and destination, taking into consideration the special needs of different groups of evacuees (e.g. patients, nursing home residents). In the event of a disaster, information about personal protection to residents (i.e. how to protect themselves from external and internal exposure) should be disseminated without delay. The timing and support for sheltering and evacuation should be optimised to reduce radiation exposure, avoid negative health effects arising from evacuation or relocation, and provide the necessary medical and psychological assistance.
3. HEALTH SURVEILLANCE AFTER THE ACCIDENT AND RELATED ISSUES
3.1. Basic survey
To estimate radiation exposure doses, FHMS obtained personal behavioural data using a questionnaire survey. The doses for the first 4 months after the accident were determined by superimposing the behavioural data of residents on gamma-ray dose-rate maps. As of the end of December 2015, the survey had estimated individual doses for approximately 550,000 people (27% of Fukushima residents). The survey found that 25 mSv was the highest estimated external individual dose, and the average dose was 0.8 mSv (Fukushima Prefectural Government, 2016). The limitations of the survey included a low response rate and the timing of the survey. The basic survey was initiated on 30 June 2011, almost 4 months after the accident. That delay could have affected the accuracy of individuals’ memories of their behaviour.
There were major limitations in dose estimation following the Fukushima accident (Ishikawa, 2017). First, the figures for external exposure dose were not based on direct measurements. There was a significant shortage of measuring instruments and support staff immediately after the accident. Second, measurements of internal contamination for short-lived radionuclides, such as 131I, were very limited. Third, most of the data later obtained from white blood cell measurements in Fukushima were not incorporated into the personal dose estimations in the basic survey.
SHAMISEN states that a system of procedures and tools for dose assessment based on individual measurements should be developed in advance (SHAMISEN, 2017). To measure and assess the dose in emergencies, it is necessary to establish guidelines with a focus on critical groups (those potentially most exposed, i.e. emergency workers, and those most vulnerable to radiation exposure, e.g. children and pregnant mothers), including plans for rapid measurements and deployment of measuring instruments. It is also essential to draft procedures for the management of large amounts of data.
3.2. Thyroid ultrasound examinations
In FHMS, thyroid examination was initiated using sophisticated ultrasound technology; it targeted Fukushima children aged ≤18 years at the time of the accident (initially approximately 360,000 children). As of 30 April 2015, 300,476 (80.7%) children had participated in the survey; of these, 2294 (0.8%) children needed confirmatory examinations, and 108 (0.036%) had possible or confirmed malignancy (Fukushima Prefectural Government, 2016). The prevalence of thyroid cysts and cancer was much higher than expected. An UNSCEAR report (UNSCEAR, 2016) noted that the likelihood of a large number of radiation-induced thyroid cancers in Fukushima Prefecture, such as after the Chernobyl accident, could be discounted; the absorbed doses to the thyroid after the Fukushima accident were substantially lower. The sensitive ultrasound thyroid screening had been expected to detect a large number of thyroid cysts and solid nodules (including a number of thyroid cancers) that would not normally have been detected without such intensive screening.
Thyroid ultrasound examination in Fukushima was initiated as a survey on a voluntary basis to monitor the health conditions of children; approximately 300,000 children participated in the survey. However, a high detection rate of thyroid tumours caused considerable concern among both children and parents (Normile, 2016). In an attempt to address this issue, Fukushima Medical University (FMU) started programmes to achieve better communication with children and their parents (Midorikawa et al., 2016). First, FMU held explanatory community meetings about the thyroid examination for the parents of children being tested. The meetings took place in smaller facilities, such as schools. Since 2013, over 150 such meetings, with more than 8000 participants, have been held. Second, immediate postexamination individual counselling began in October 2014, 3 years after the start of the examinations. Third, in-school class dialogues were initiated in 2015. In that programme, FMU teams conducted classes about the thyroid examination for students at elementary, junior high, and high schools. The aim was to provide better understanding of the meaning of the examination and interpretation of results. By the end of 2016, approximately 5000 children (most of them in Grades 5–6 of elementary school and junior high school) took part in the classes. These efforts were effective in facilitating understanding about the thyroid examination and associated diseases. Although the thyroid examination was proposed on a voluntary basis for individuals, difficulties have been encountered in such a large-scale screening programme for assuring proper informed decisions about undergoing thyroid examination by children and parents (Midorikawa et al., 2017).
In Fukushima, a high prevalence of thyroid tumours was observed; however, that was not due to the effects of radiation, but because of the sudden attention paid to the disease by well-meaning physicians (SHAMISEN, 2017). Unfortunately, there are no internationally agreed criteria for selecting individuals who should undergo long-term follow-up. The majority of cases of thyroid cancer show good prognosis and slow evolution. SHAMISEN states, therefore, that thyroid cancer screening should be proposed on a voluntary basis for individuals who wish to be monitored, as long as they receive appropriate information and support.
3.3. Disaster-related deaths among the elderly and health problems related to relocation and long-term displacement
By May 2011, 165,000 residents had evacuated, either voluntarily or forcibly (Hasegawa et al., 2015). The evacuation and relocation had adverse health effects, particularly among elderly people requiring nursing care and hospitalised patients. After the accident, the mortality rate among evacuated elderly people requiring nursing care increased approximately three fold in the first 3 months compared with before the accident; it subsequently remained approximately 1.5-fold higher (Yasumura et al., 2013). Repeated relocation from one shelter to another and the frequent changes in living environment posed significant adverse effects on elderly health. Deaths were caused indirectly by the earthquake and tsunami, and were therefore certified by the local government as disaster-related deaths (DRDs). The DRDs in Fukushima accounted for 56% of all DRDs (1704 of 3089 DRDs in total) that occurred during the first 52 months after the earthquake (Ichiseki, 2013). Although the number of evacuees had decreased to 58,000 by July 2017, the DRDs in Fukushima increased to 2147 (60%) of the 3591 DRDs (as of 31 March 2017) in the Tohoku region (i.e. Iwate, Miyagi, and Fukushima Prefectures) (Reconstruction Agency, 2017a).
Psychological distress was another health problem. FHMS found that the proportion of individuals, including children, with psychological distress (14.6%) was far greater than in other areas affected by the earthquake and tsunami (6.2%), and the Japanese population under normal circumstances (4.2–4.4%) (Hasegawa et al., 2015). The proportion of residents requiring support for depressive symptoms and anxiety has gradually decreased over the 7 years since the accident; however, it is higher than the general population. Likewise, the pregnancy and birth survey in 2011 found that one-quarter of the surveyed mothers had depressive symptoms; the highest proportion was observed in Soso region, where Fukushima Daiichi nuclear power plant is located. A gradual decline was evident in the proportion of mothers with depressive symptoms; however, in 2014, 20% of the surveyed mothers had depression (Goto et al., 2015).
The biggest concern with depressive symptoms is suicide. In Japan, Tohoku is known to have a high suicide rate. Iwate and Miyagi Prefectures were severely damaged by the earthquake and tsunami. Soon after the disaster, the suicide rate decreased temporarily in Iwate and Miyagi; thereafter, it gradually increased. However, in Fukushima, the suicide rate did not fall as much as in the other two prefectures, and it then increased more rapidly (Ohto et al., 2015). The National Police Agency defines disaster-related suicide (DRS) as follows: a body being found at a shelter or temporary house; the victim being a resident of a shelter or temporary house; the person being an evacuee whose original residential area was severely damaged by an earthquake or tsunami; and the suicide motivation being associated with the disaster (i.e. indicated in a suicide note). According to a police report, Fukushima had the highest number of DRSs among the three affected Tohoku prefectures from 2012 to 2016 (Fig. 2) (National Police Agency, 2017).
Number of disaster-related suicides in three prefectures affected by the Great East Japan Earthquake (National Police Agency, 2017).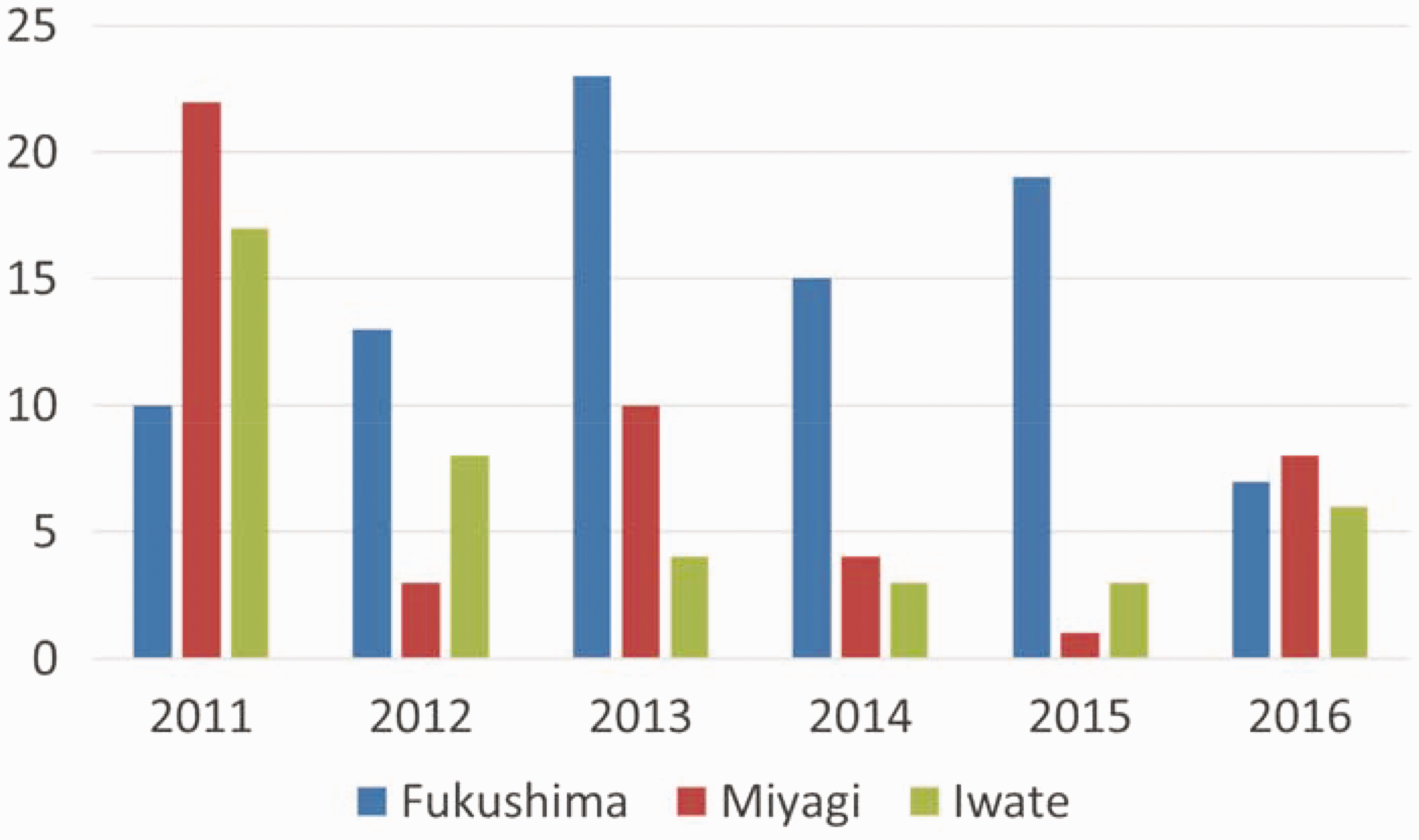
To address psychological issues following the accident, the Mental Health Support Team of FMU has provided brief telephone counselling for approximately 4000 evacuees at risk of psychiatric disorders, such as post-traumatic stress disorder and depression, every year (Maeda and Oe, 2016). By way of official support for the evacuees, Fukushima Prefectural Government established a plan called the ‘Active Plan of Countermeasures for Suicide’. This plan aimed to establish social support through the following measures: reinforcing a network among government, municipalities, hospitals, employers, schools, and private organisations; creating circumstances with family and friends or in workplaces such that a person at risk feels comfortable about receiving consultation; and training support staff among municipalities, counselling agencies, and related support institutions to play a key role as gatekeepers. In 2012, entrusted by Fukushima Prefectural Government, Fukushima Mental Health Welfare Association established the Fukushima Mental Health Care Centre to provide mental health intervention programmes. This centre has six branches in Fukushima. The staff of approximately 50 people consists of psychiatrists, social workers, clinical psychologists, nurses, and occupational therapists; they provide active outreach services and group interventions for evacuees suffering from psychological stress. However, the number of staff members working with the affected population of Fukushima is insufficient. More support staff are needed to reach out to people at risk.
With regard to other health issues, FHMS reported increased proportions of obesity, glucose intolerance, liver dysfunction, and hypertension after the accident (Fukushima Prefectural Government, 2016). Another study analysed the data of 27,000 residents who lived near Fukushima Daiichi nuclear power plant before the accident and received follow-up examinations afterwards (Ohira et al., 2017). Evacuation was associated with increased risk of becoming overweight or obese; the hazard ratio following evacuation was 1.82 for men and 1.52 for women. Increased hazard ratios for hypertension, dyslipidaemia, and diabetes were also associated with evacuation (Satoh et al., 2015). The study suggested that evacuation would lead to a predisposition to cardiovascular diseases if the attendant problems were not addressed properly.
The Fukushima accident revealed severe health problems caused by relocation or long-term displacement, such as DRDs, mental health problems, and lifestyle-related diseases (e.g. diabetes, hypertension, and increased body weight). The evacuees experienced separation from their families, loss of their homes and employment, and having to move to unfamiliar places. Some of them had left behind traditions and culture that had developed over many generations. Complex psychosocial issues arose, including disagreements within families and in society about the potential health consequences of the accident and issues related to compensation. Evacuation also had significant social and economic costs.
To minimise the adverse effects of evacuation on the physical and mental health of evacuees and communities, SHAMISEN states that plans for lifting evacuation orders need to be established as soon as possible (SHAMISEN, 2017). The criteria for lifting evacuation should be based on an assessment of radiation exposure doses in evacuated areas; however, the actual decision needs to be made through consultation with stakeholders. Such decisions should be based not only on radiological criteria, but also on social, cultural, and economic aspects. Appropriate support has to be supplied to affected populations if long-term evacuation or relocation appears likely. The objectives of health and medical surveillance are to evaluate whether individuals affected by an accident are suffering from certain health conditions. That is a basis for providing support and treatment as required.
3.4. What has been learned from the Fukushima accident and SHAMISEN recommendations
Despite the severity of the Fukushima accident and huge impact of the natural disaster on the region, the radiation exposure of the public was very low. However, other serious issues were encountered, including deaths during evacuation, increased mortality among displaced elderly people, mental health and lifestyle-related health problems, and social issues after the accident. This experience suggests that these areas had not been addressed sufficiently in previous accident response planning. Most existing recommendations for preparedness and responses for a nuclear and radiological emergency have a technical focus on radiation; less attention is paid to general health and psychological, social, and ethical issues. The information provided tends to be directed towards decision making by experts, rather than for supporting affected populations (SHAMISEN, 2017).
The management of radiological accidents raises a number of ethical issues. One central question is whether or not the response to the accident causes more good than harm. The majority of radiation protection actions, such as evacuation, are directed at reducing the effect of exposure to ionising radiation; however, most actions carry direct and indirect consequences, which can have a large impact on the welfare of affected populations. Ethical considerations are also important in the design and implementation of health surveillance and epidemiological studies.
The Fukushima accident revealed that it is essential to balance the risks of radiation with other health and social effects after the accident; it is also necessary to develop specific measures towards mitigating the overall health risks, and minimising adverse effects on well-being. According to the World Health Organization, ‘Health is a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity’ (WHO, 1948). The effects include psychosocial and health impacts caused by stress and anxiety; direct negative health impacts of emergency evacuation; and socio-economic, cultural, and other social impacts. The long-lasting social and economic disturbances can also be linked to a range of lifestyle-related diseases among affected populations.
SHAMISEN states that it recognises the need for a holistic approach to accident management and health surveillance to achieve the aim of doing more good than harm. A multi-disciplinary approach is needed if health surveillance is to identify and alleviate psychosocial impacts; that includes the participation of psychologists, mental health specialists, sociologists, radiation protection experts, radiation epidemiologists, and other stakeholders who are able to take into account the concerns and expectations of local populations.
In April 2017, the evacuation order was lifted in most of Tomioka and part of Namie. By that time, the area where residents were not allowed to return was one-third what it had been in 2012 (Fig. 3). However, only 10% of the original population in municipalities where the evacuation order has been lifted have returned to their home towns (Reconstruction Agency, 2017b). A survey for Tomioka residents showed that only 16% of respondents wished to return (Reconstruction Agency, 2017b). In the survey, 44% of respondents had already settled in new places. More than half were concerned about inadequate social support, such as poor access to medical services, disrupted public transportation, and shortage of commercial facilities, schools, and job opportunities. As reasons for not returning, they also cited concerns about radiation exposure and the safety of Fukushima Daiichi nuclear power plant. Fukushima Prefectural Government has been addressing the needs of returnees, and it has established a revitalising plan, including development of medical services in collaboration with FMU. The revitalisation of community welfare is a particularly important consideration, although it is often challenged through mistrust in the authorities; as such, the participation of local health practitioners and actors should be encouraged (SHAMISEN, 2017).
Municipality and population around Fukushima Daiichi nuclear power plant (1 April 2017) (Reconstruction Agency, 2017b).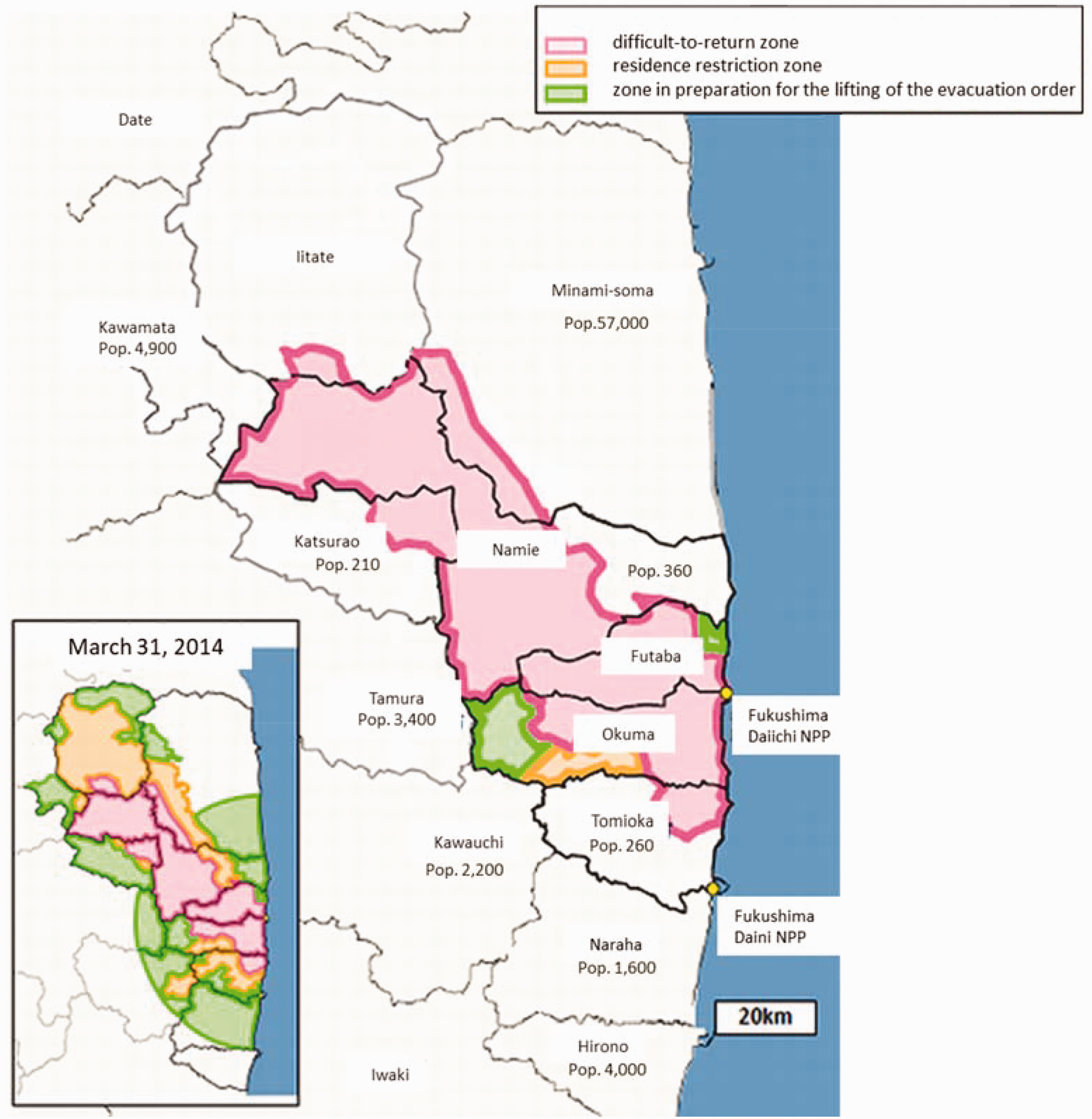
Footnotes
Acknowledgements
The author wishes to thank the organiser of the EU-OPERRA SHAMISEN project for providing FMU with an opportunity to share experiences in Fukushima with experts from the European Union.