
Abstract
Major current efforts within Committee 2 of the International Commission on Radiological Protection (ICRP) involve the development of dose coefficients for inhalation and ingestion of radionuclides, and those for exposure to environmental radiation fields. These efforts build upon changes in radiation and tissue weighting factors (Publication 103), radionuclide decay schemes (Publication 107), computational phantoms of the adult reference male and female (Publication 110), external dose coefficients for adult reference workers for idealised radiation fields (Publication 116), models of radionuclide intake (Publications 66, 100 and 130), and models of radionuclide systemic biokinetics (Publication 130). This paper will review the overall computational framework for both internal and external dose coefficients. For internal exposures, the work entails assessment of organ self-dose and cross-dose from monoenergetic particle emissions (specific absorbed fraction), absorbed dose per nuclear transformation (S value), time-integrated activity of the radionuclide in source tissues (inhalation, ingestion, and systemic biokinetic models), and their numerical combination to yield the organ equivalent dose or effective dose per activity inhaled or ingested. Various challenges are reviewed that were not included in the development of Publication 30 dose coefficients, which were based upon much more simplified biokinetic models and computational phantoms. For external exposures, the computations entail the characterisation of environmental radionuclide distributions, the transport of radiation particles through that environment, and the tracking of energy deposition to the organs of the exposed individual. Progress towards the development of dose coefficients to members of the general public (adolescents, children, infants and fetuses) are also reviewed.
1. INTRODUCTION
A central responsibility of Committee 2 of the International Commission on Radiological Protection (ICRP) is the development of reference dose coefficients for radiation exposure of workers (irradiation scenarios under occupational settings) and members of the general public (irradiation scenarios under environmental settings). Members of Committee 2 also work in concert with members of Committee 3 regarding dose coefficients for medical exposures, particularly for radiopharmaceuticals administered either for diagnostic imaging or therapeutic treatment. Dose coefficients are broadly defined as a quantity that, when multiplied by a measurement of either radionuclide intake, air kerma, particle fluence, or environmental radioactivity concentration, will yield an organ equivalent dose or the effective dose to the exposed individual. They may be specific to monoenergetic radiation fields, radiation fields composed of a spectrum of energies, or radiation emissions specific to a given radionuclide or a mixture of radionuclides. For workers, equivalent dose coefficients are defined for the reference adult male and reference adult female, and these are sex-averaged in the calculation of effective dose. For members of the general public, dose coefficients may be defined for infants, children, and adolescents of various defined reference ages. They may also be defined for pregnant females, where the organs of interest are those in the developing fetus.
For internal exposures to adult workers, a dose coefficient is defined as either the committed equivalent dose in organ or tissue T per inhalation or ingestion activity intake, hT(50), or the committed effective dose per intake, e(50), where 50 is the dose-commitment period in years over which the dose is calculated. In some cases, the term ‘dose per intake coefficient’ is used. Internal dose coefficients require the development and subsequent implementation of three general types of component models, as demonstrated graphically in Fig. 1.
Three major models needed to calculate internal radiation dose by radionuclides following inhalation, ingestion, or wound entry. These include: (A) a model of radionuclide biokinetic behaviour within the body tissues; (B) the energies and yields of all radiations emitted by the radionuclide in the source organs; and (C) anatomical models of the exposed individual allowing assessment of both self-dose and cross-dose to target organs of interest in radiological protection.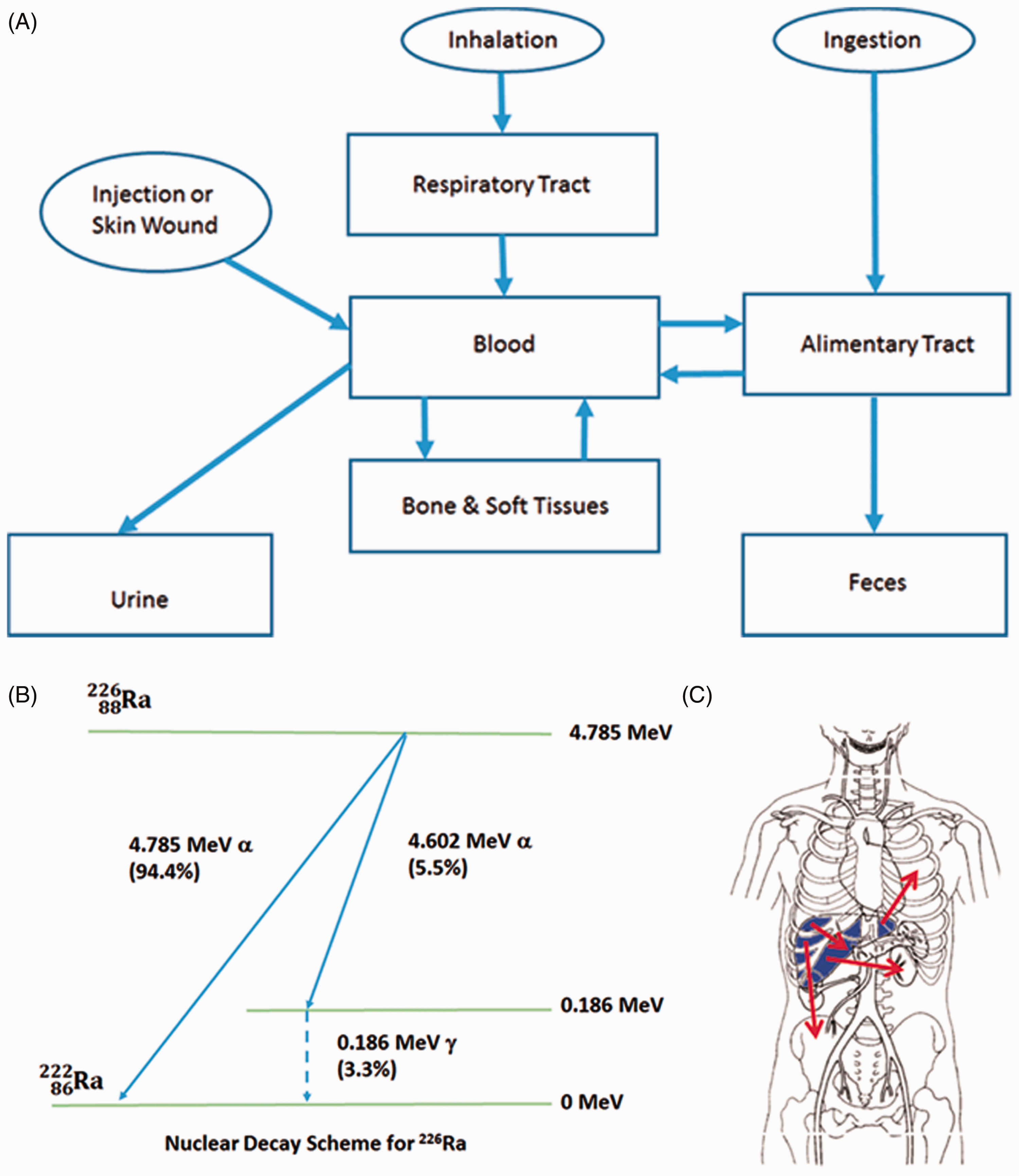
The first is a model of radionuclide intake (ingestion, inhalation, or possibly wound absorption), its subsequent uptake to blood as well as various ‘source’ organs, its release back to blood, and ultimately its excretion from the body (Fig. 1A). Both physical decay within the body and the ingrowth of radioactive progeny are considered. The second is a component model of radionuclide nuclear transformation, including full accounting of the types of radiation particles emitted, their energies or energy spectra, and their relative emission frequencies (Fig. 1B). Finally, a component model of the internal anatomy of the exposed individual is employed, along with radiation transport computation, to follow all radiation particles from their sites of emission in the various source organs to their sites of energy deposition within various target organs for which a dose estimate is sought (Fig. 1C). It is noted that source organs are, by definition, also target organs. Other target organs are those tissues within the ranges of the emitted radiation particles, including secondary processes such as bremsstrahlung x-ray emission. The quantity sought in these simulations is the specific absorbed fraction (SAF), defined as the fraction of emitted particle energy in the source organ that is deposited per unit mass in the target organ. Over many decades, ICRP has further refined these different classes of component models, applying new scientific data and computational techniques as they become available. In many cases, specific models are developed within Committee 2 and its various Task Groups as part of their overall mission to develop the next generation of reference dose coefficients.
For external exposures, the dose coefficient relates a dose quantity – either the organ equivalent dose or effective dose – to a calculated or measured quantity such as air kerma, particle fluence, or radioactivity concentration. As illustrated in Fig. 2, there are two broad classes of external exposures. The first, shown in Fig. 2A, are exposures to broad fields of radiation particles that, in an idealised sense, reflect exposures in occupational irradiation settings. Dose coefficients may thus be assigned based upon particle type, particle energy, and irradiation geometry. For example, antero-posterior irradiation infers that the radiation particles impinge on the worker from his or her front (anterior) surface. Right lateral irradiation infers that the radiation particle field impinges on the worker from his or her right body side. The second class of external dose coefficients, illustrated in Fig. 2B, relates the organ or effective dose rate to either a measurement of air kerma 1 m above the ground, or to radioactivity concentration in either contaminated air, water, or soil. The latter can be further defined as a function of soil depth, thus allowing the user to apply measurements of depth-dependent radionuclide soil activity to the dose assessment. ICRP has recently refined its values of reference dose coefficient for idealised occupational radiation fields (ICRP, 2010). New efforts are underway to define, for the very first time, reference dose coefficients for environmental exposures.
Two exposure scenarios considered for calculation of external dose coefficients in radiological protection: (A) idealised uniform radiation fields of relevance to occupational exposures; and (B) radiation fields from radionuclides in contaminated air, water, or soil. AP, antero-posterior; PA, postero-anterior; LLAT, left lateral; RLAT, right lateral; ROT, rotational; ISO, isotropic.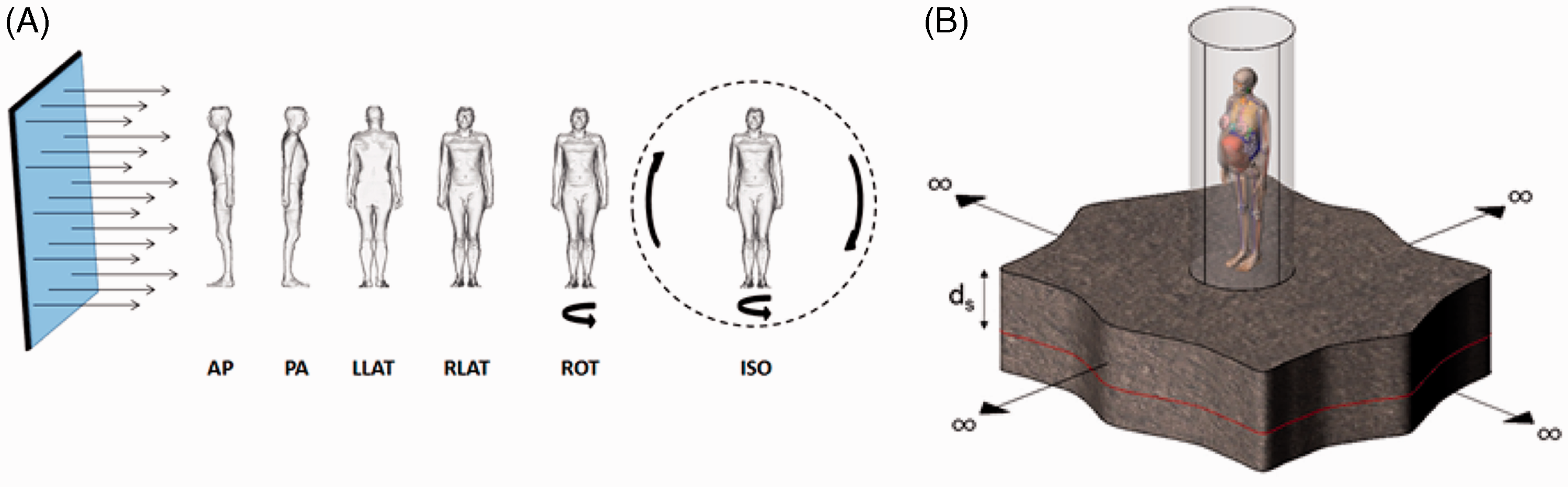
2. COMPUTATIONAL FRAMEWORK FOR INTERNAL DOSE COEFFICIENTS
In prospective radiological protection, internal dose coefficients are defined for either inhalation or ingestion of radionuclides. Models do exist that allow for the consideration of entry of radionuclides into the body via wound absorption, but this pathway is considered strictly in the context of accidental dose reconstruction. Models for radionuclide airway deposition, particle airway clearance, and blood absorption are contained in the ICRP Human Respiratory Tract Model given in Publication 66 (ICRP, 1994), with updates provided in Publication 130 (ICRP, 2015). Models for radionuclide ingestion and gastrointestinal tract translocation are contained in the ICRP Human Alimentary Tract Model given in Publication 100 (ICRP, 2006). Both models provide a way of simulating the entry of radionuclides into the blood of the circulatory system, after which one must invoke a model for systemic biokinetics.
The compartment models of the respiratory and alimentary tract coupled with those of the systemic biokinetics define a system of first-order differential equations. The solution to the set of equations is the time-dependent distribution of the radionuclide and its radioactive progeny, if any, in mathematical compartments that are associated with anatomical regions in the body. Let M is the number of compartments describing the kinetic model;

Given the initial conditions specified for the compartments,
The system of N × M ordinary first-order differential equations must be solved using suitable numerical methods. The system is generally solved for the initial conditions that
To calculate the numerical values of the dose coefficients, it is necessary to associate the biokinetic compartments of Eq. (1) with anatomical regions in the body; so-called source regions indexed by rS. The source regions may or may not be a living tissue. For example, the contents of the alimentary tract are not living tissues, and may consist of more than one kinetic compartment. The number of nuclear transformations of chain member i occurring in source region rS,


The committed equivalent dose coefficient in target region rT of the reference adult male, wR is the radiation weighting factor for radiation type R; and


A number of tissues used to compute the effective dose are considered to be represented by a single target region, rT. In cases where more than one tissue region defines the target tissue, fractional weighting of the equivalent dose must be made. The committed equivalent dose coefficients for tissue T in the reference adult male,


The committed effective dose coefficient,

3. MODELS FOR RADIONUCLIDE BIOKINETIC DISTRIBUTION
Following intake by either inhalation or ingestion, a fraction of the radionuclide enters the blood and body fluids of the body. The subsequent fate of the radionuclide in the body is computationally handled by a systemic biokinetic model. Models are specific to individual elements and apply to all their radioisotopes. In its first comprehensive report of reference dose coefficients for internal exposure, ICRP employed systemic biokinetic models in Publication 30 (ICRP, 1980) as shown generically in Fig. 3. Radioactivity in the ‘transfer compartment’ is transferred exponentially to one or more compartments of the body tissues. As the radionuclide is then released from the source tissues, it is assumed to be eliminated directly from the body in excreta (urine or faeces). Individual source organs may be represented as either one, two or three compartments, each with their own fractional uptake from blood and biological half-time.
General structure of biokinetic models of radionuclides in Publication 30 (ICRP, 1980).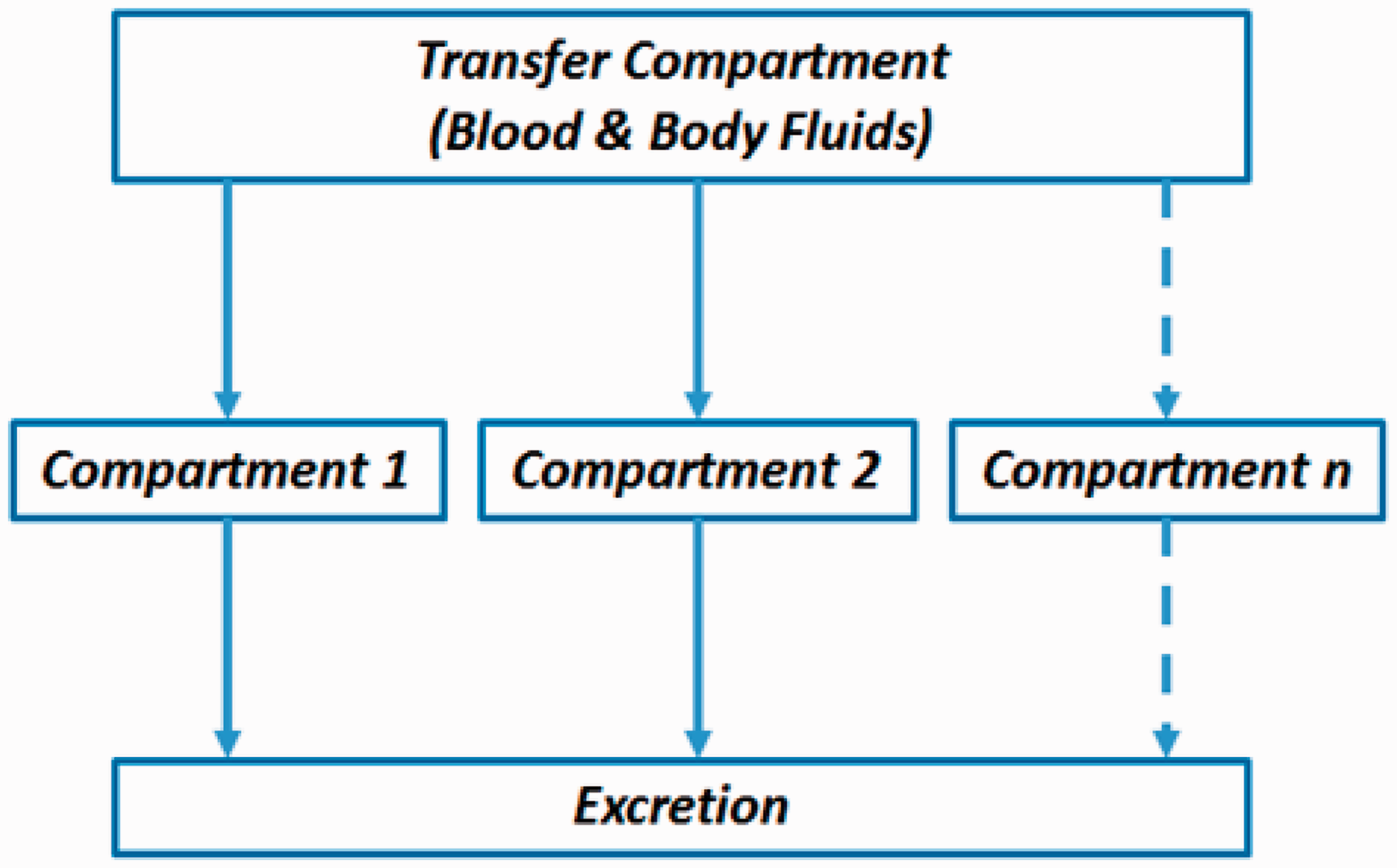
As an example, the element caesium in Publication 30 (ICRP, 1980) is assumed to have only one source tissue – the total body. However, that one source tissue is partitioned in the systemic biokinetic model for caesium into two source compartments – one with an uptake fraction of 0.1 that clears rapidly from the body, and the other with an uptake fraction of 0.9 that clears more slowly from the body:




Beginning in the early 1990s, Committee 2 and its Task Groups began to adopt more physiologically realistic models of radionuclide systemic biokinetics that permitted explicit consideration of the initial distribution of the radionuclide in the circulatory system, and its subsequent re-entry to blood following organ elimination. This approach employs the construction of a biokinetic compartmental model of radionuclide distribution in the body.
Fig. 4 shows the current ICRP systemic model for caesium and its various radio-isotopes. The various labelled compartments thus represent ‘pools’ of the element within the body, with the connecting arrows representing transfer coefficients defining the fraction of the source compartment that is transferred to the receiving compartment per unit time. Caesium in the blood is thus shown to localise to bone, liver, the alimentary tract contents, and various soft tissues of the body; the latter are modelled by three separate compartments with differing transfer rates. Caesium in the blood is further localised in the kidney tissues as well as processed to urine; it is stored temporarily in the urinary bladder, and then excreted. This and other models of the various elements are thus based upon combinations of measured data (animal or human) and fundamental knowledge of organ/tissue physiology and elemental metabolism. The use of compartmental systemic models developed by ICRP has a wide range of applications beyond radiological protection, including human toxicology, industrial hygiene, and pharmacodynamics.
Example structure of the physiologically realistic biokinetic models used presently by the International Commission on Radiological Protection. This particular example shows that for systemic distribution of caesium in the adult worker.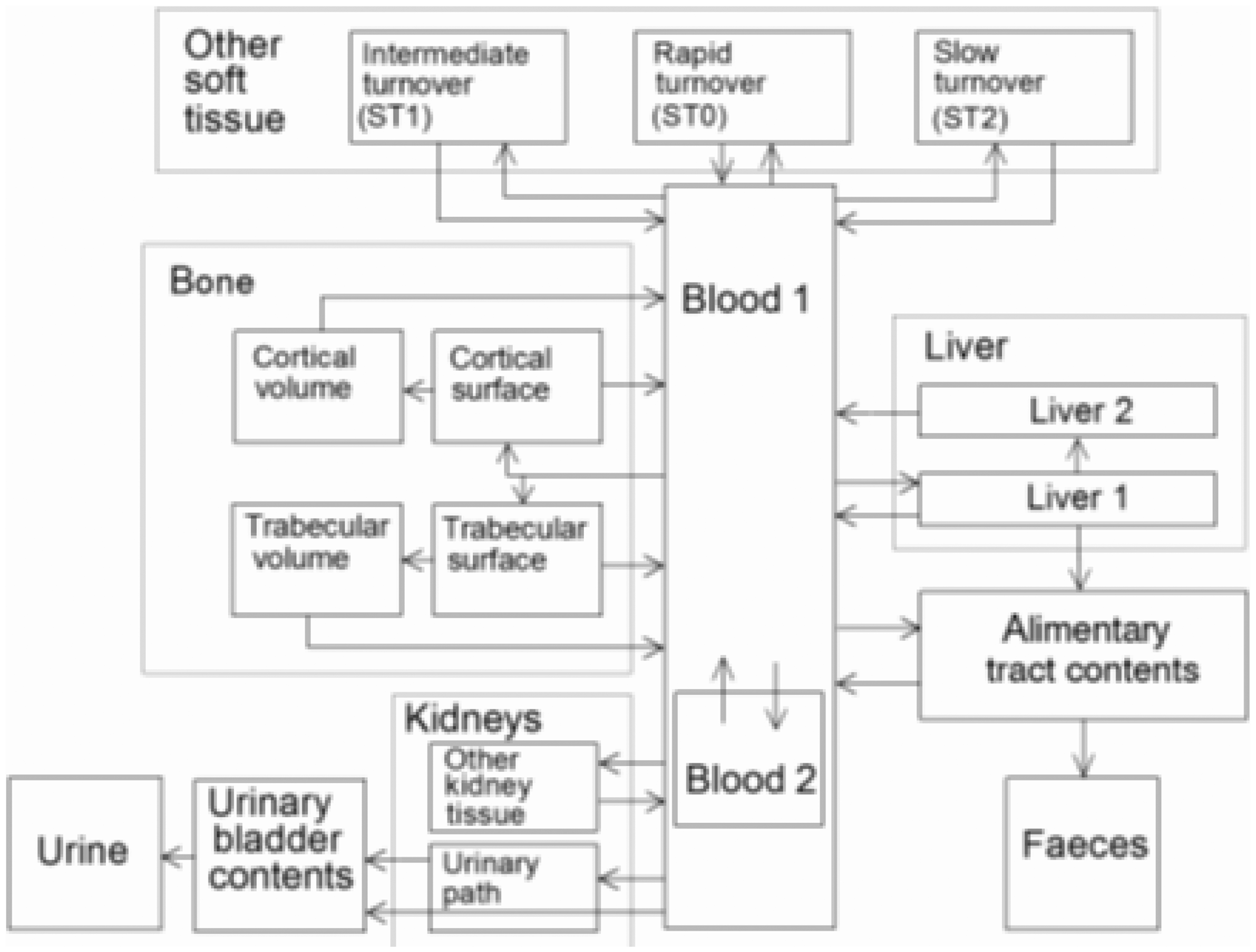
4. MODELS OF RADIONUCLIDE DECAY AND RADIATION EMISSION
The major component model needed for the calculation of a dose coefficient is that for the nuclear transformation of the radionuclide. By definition, a nuclear transformation is a process by which the ratio of neutrons to protons (N/P) in the nucleus is altered in a manner that ensures a more stable balance of attractive and repulsive nuclear forces. Four main modes of nuclear transformation are α particle emission (N/P ratio increases), β particle emission (N/P ratio decreases), positron emission (N/P ratio increases), and orbital electron capture (N/P ratio increases). Each of these forms of nuclear transformation has various major associated radiations, including γ-ray and conversion electron emissions (both forms of release of excess nuclear binding energy), and characteristic x-ray and Auger electron emissions (both forms of release of excess electronic binding energy). Models of nuclear transformation entail detailed accounting of the energies, energy spectra, and percentage yield relative to all nuclear transformations that are energetically possible.
The first major compilation of radionuclide decay schemes was released by ICRP in Publication 38 (ICRP, 1983); this included energies and yields of both primary and associated radiations emitted from 820 different radionuclides. Data were restricted to radionuclides with physical half-lives exceeding 10 min. The report provided abbreviated tables of decay data along with a schematic diagram of the decay scheme for each radionuclide. These data were used in the computation of dose coefficients in the Publication 30 series (ICRP, 1979a,b, 1980, 1981a,b, 1982a,b).
In 2008, ICRP released its second extensive compilation of radionuclide decay data in Publication 107 (ICRP, 2008). This report covered some 1252 radionuclides and included all nuclides with a physical half-life of >1 min for which the nuclear structure information was judged sufficient for a meaningful assessment of emissions. Data were provided in Publication 107 for 922 radionuclides with a half-life of >10 min and for 330 radionuclides with a half-life of <10 min. This report departed from the formation of Publication 38 (ICRP, 1983) in that it included the decay data in electronic form as a CD with associated software with rapid look-up capability software.
5. ANATOMICAL MODELS FOR REFERENCE ADULTS
The third and final component model needed for the computation of reference dose coefficients is a three-dimensional (3D) model of the exposed person, with definitions of both internal organ anatomy and outer body surfaces. Until very recently, ICRP relied heavily on the use of so-called stylised or mathematical models of organ anatomy, such as those from Oak Ridge National Laboratory (ORNL). A graphical representation of the ORNL adult model is shown in Fig. 5. Body and organ surfaces are defined using geometrical 3D surface equations such as spheres, cones, ellipsoids, and toroids. These models are generally hermaphrodites with both male and female sex organs included.
Stylised anatomical model of the hermaphrodite adult used in previous reports of the International Commission on Radiological Protection.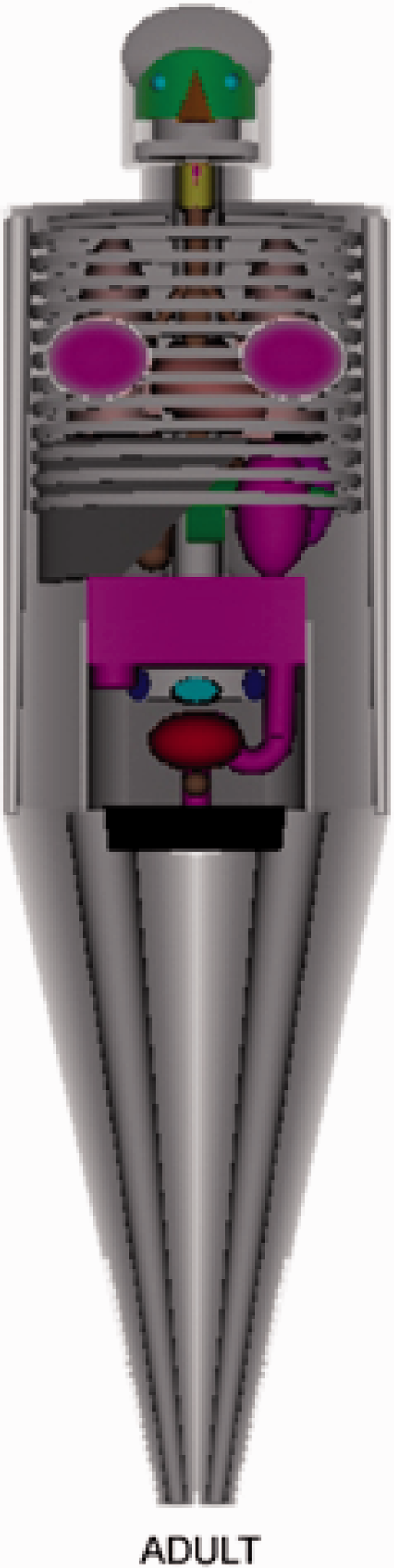
Following issuance of the 2007 Recommendations (ICRP, 2007), the Commission released new computational phantoms of ICRP reference adult male and reference adult female in Publication 110 (ICRP, 2009). These reference computational phantoms are digital 3D representations of human anatomy and are based on human computed tomographic data. They are consistent with the information given in Publication 89 (ICRP, 2002) on the reference anatomical parameters for both male and female adults. The reference computational phantoms (or models) were constructed by modifying the voxel models (Zankl and Wittmann, 2001; Zankl et al., 2005) of two individuals (Golem and Laura) whose body height and mass closely resembled the reference data. The organ masses of both phantoms were adjusted to ICRP data with high precision, without altering their realistic anatomy significantly. The phantoms contain all target regions relevant to the assessment of human exposure to ionising radiation for radiological protection purposes (ICRP, 2007).
Each phantom is represented in the form of a 3D array of cuboid voxels. Each voxel is a volume element, and the voxels are arranged in columns, rows, and slices. Each entry in the array identifies the organ or tissue to which the corresponding voxel belongs. The male reference computational phantom consists of approximately 1.95 million tissue voxels (excluding voxels representing the surrounding vacuum), each with a slice thickness (corresponding to the voxel height) of 8.0 mm and an in-plane resolution (i.e. voxel width and depth) of 2.137 mm, corresponding to a voxel volume of 36.54 mm3. The number of slices is 220, resulting in a body height of 1.76 m; the body mass is 73 kg. The female reference computational phantom consists of approximately 3.89 million tissue voxels, each with a slice thickness of 4.84 mm and an in-plane resolution of 1.775 mm, corresponding to a voxel volume of 15.25 mm3. The number of slices is 346, and the body height is 1.63 m; the body mass is 60 kg. The number of individually segmented structures is 136 in each phantom, to which 53 different tissue compositions have been assigned. The various tissue compositions reflect both the elemental composition of the tissue parenchyma (ICRU, 1992) and each organ’s blood content (ICRP, 2002) (i.e. organ composition inclusive of blood). Fig. 6 shows frontal (coronal) views of the male (left) and female (right) computational phantom.
Publication 110 (ICRP, 2009) reference computational phantoms of the adult male and female.
Following the release of Publication 130 (ICRP, 2015), the Commission will issue an entirely new generation of inhalation and ingestion dose coefficients to replace those previously contained in Publication 30 (ICRP, 1980) and subsequent reports. As part of this effort, new SAF and radionuclide S values are computed and utilised in the computation of the Occupational Intakes of Radionuclides series based upon Publication 110 (ICRP, 2009) reference adult phantoms. Example values of photon and electron SAFs are shown in Fig. 7 for both the reference adult male and reference adult female. In each case, the radiation source is the kidneys, and the target organ is the adrenal glands. An entirely new feature of these data is the explicit treatment of electron transport as shown in Fig. 7B. Prior computations of ICRP dose coefficients assumed full absorption of electron and β-particle kinetic energy in the source organ, in which case the SAF value (adrenals ← kidneys) would be zero. As shown in Fig. 7B, however, SAF values (adrenals ← kidneys) at electron energies of several hundred keV are comparable in magnitude to those for photon emissions in the adult kidneys.
Values of specific absorbed fractions for (A) photon sources and (B) electron sources localised in the kidneys of Publication 110 (ICRP, 2009) reference phantoms. The target organ in each case is the adrenal glands.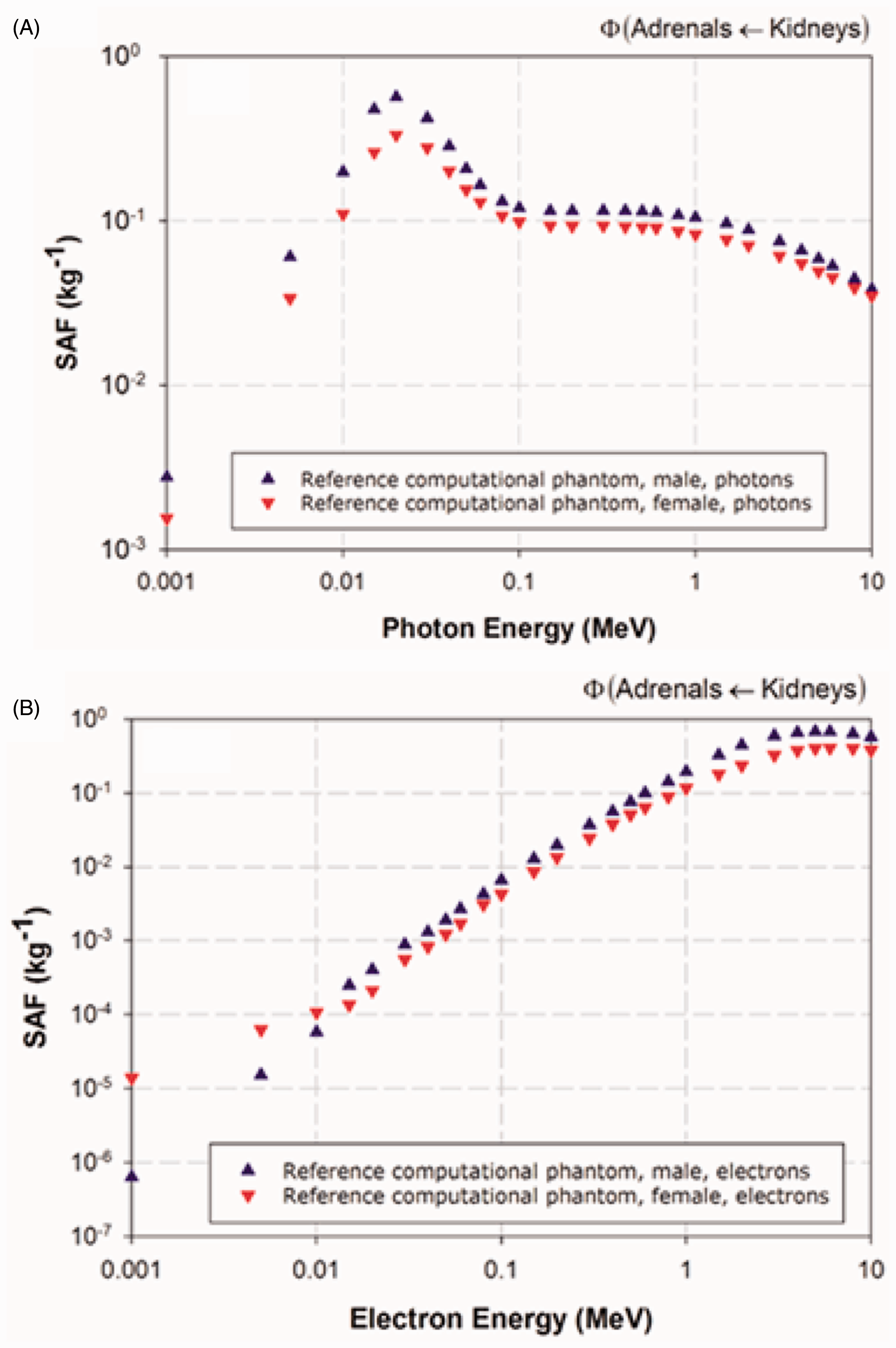
6. ANATOMICAL MODELS FOR MEMBERS OF THE GENERAL PUBLIC
Following the Chernobyl nuclear reactor accident in April 1986, it became abundantly apparent that dose coefficients to members of the general public – including infants, children, and adolescents – were needed for radiological protection guidance in both post-accident dose assessment and environmental clean-up standards. Consequently, ICRP embarked on a series of reports for which age-dependent biokinetic models and anatomical phantoms were employed. Age-specific dose coefficients for both radionuclide ingestion and inhalation were published in Publications 56, 67, 71 and 72 (ICRP, 1990, 1993, 1995, 1996). Similarly, dose coefficients needed for reporting organ and effective dose to the developing embryo and fetus were the focus of Publications 88 and 95 (ICRP, 2001, 2004). In these report series, SAF values for photons were computed using the ORNL series of paediatric and pregnant female stylised phantoms (Stabin et al., 1995; Eckerman et al., 1996).
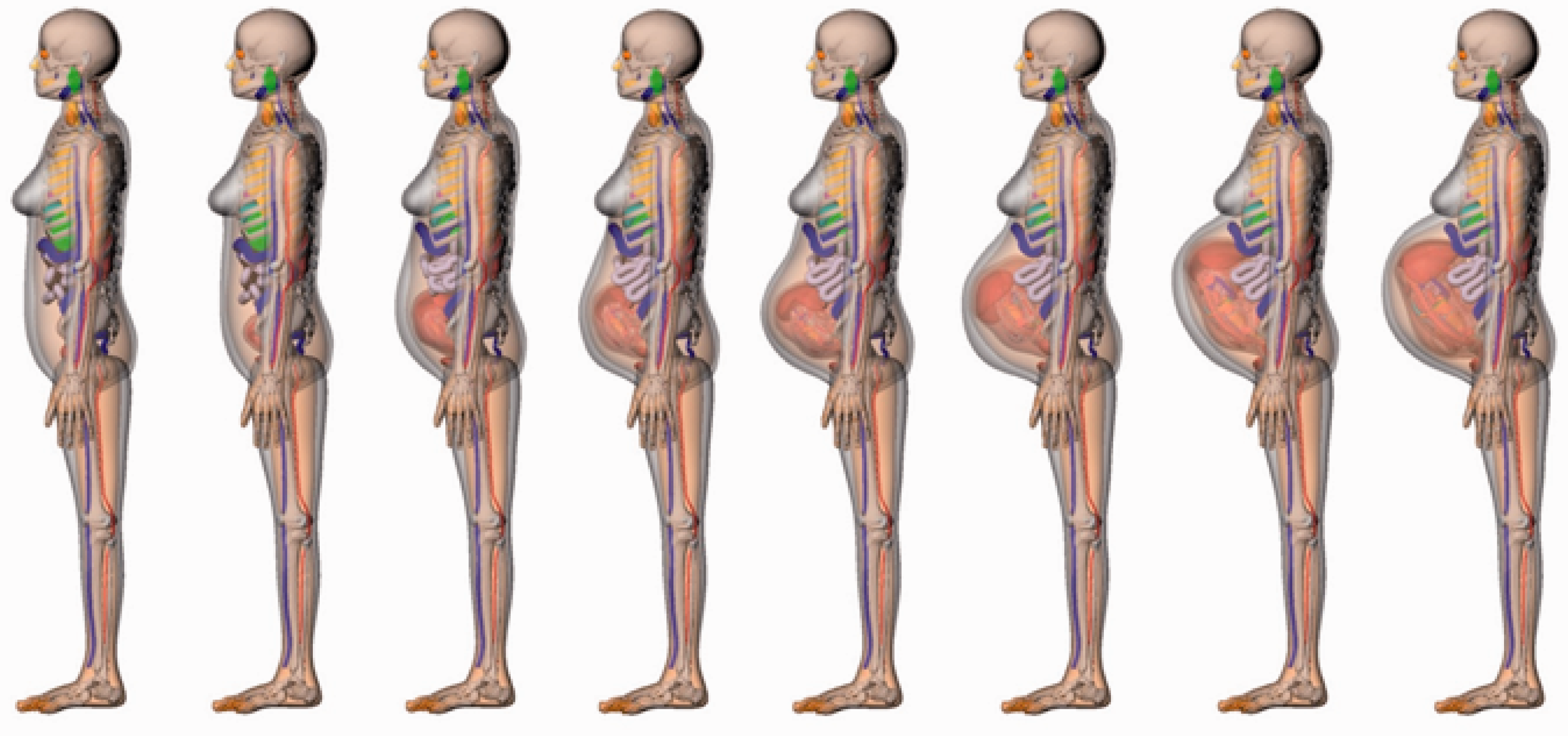
As a major update to these series of reports on public exposures, Committee 2 has recently developed a new generation of reference voxel phantoms of ICRP paediatric reference individuals to include newborn, and 1, 5, 10, and 15-year-old males and females. The basis for this new series of reference phantoms is the University of Florida/National Cancer Institute series of anatomical models shown in Fig. 8 and documented in Lee et al. (2010). These phantoms include all the major tissues and organs included in Publication 110 (ICRP, 2009) adult reference phantoms. For the updates to Publications 88 and 95 (ICRP, 2001, 2004), a new series of reference computational phantoms of the adult pregnant female have been adopted by ICRP as shown in Fig. 9. These particular anatomical models were constructed for use in assessment of in-utero organ doses for the offspring of nuclear facility workers at the Russian Mayak plant, and people living along the nearby Techa River (Maynard et al., 2011, 2015a,b). They include explicit models of all fetal organ structures, including gestation-period-specific ossification centres of the fetal skeleton.
Future basis of new International Commission on Radiological Protection reference computational phantoms of children and adolescents. Future basis of new International Commission on Radiological Protection reference computational phantoms of the adult pregnant female (8–38 weeks post-conception).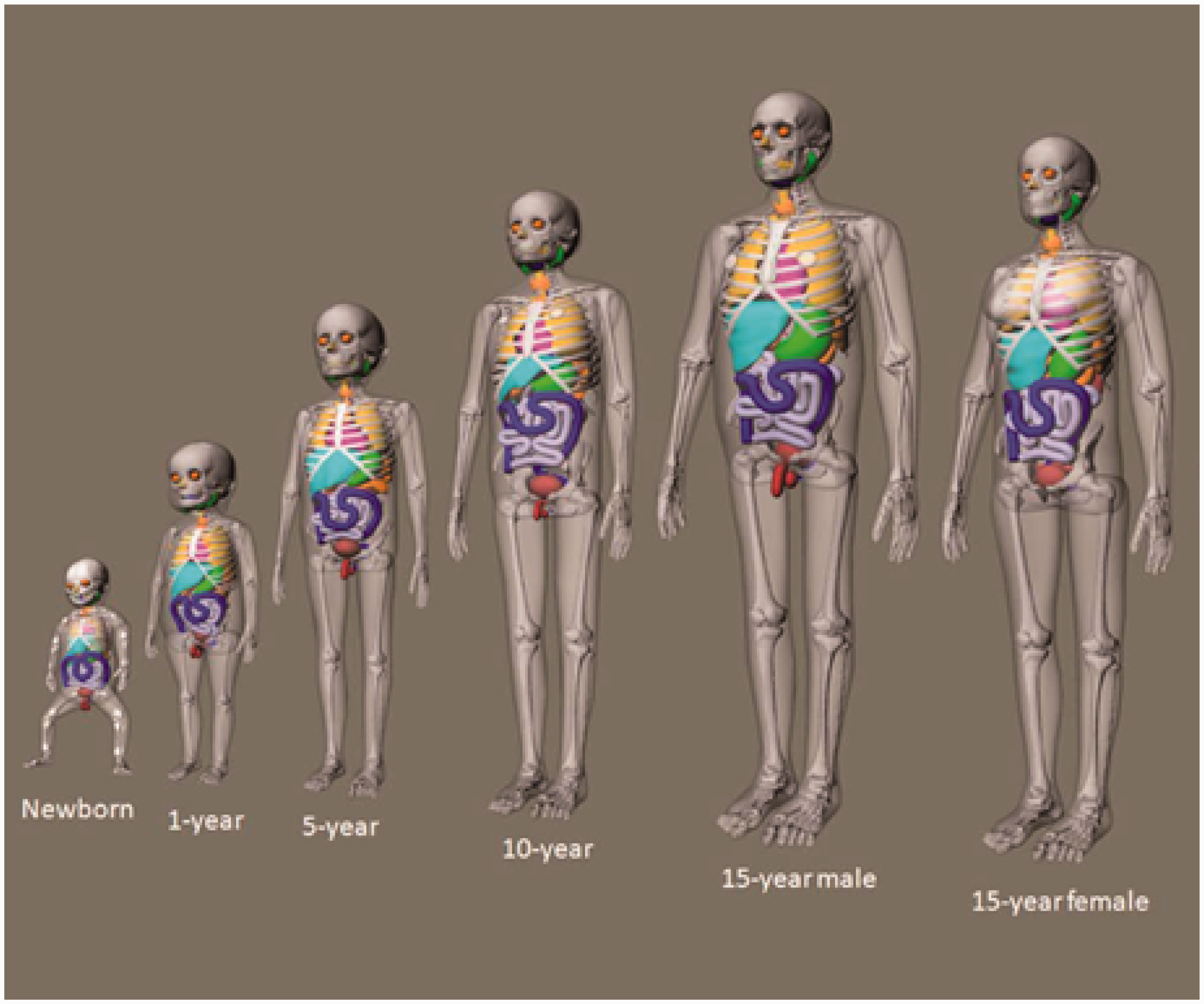
7. COMPUTATION OF EXTERNAL DOSE COEFFICIENTS
As noted previously, ICRP has issued Publication 116 (ICRP, 2010), a comprehensive report on dose coefficients for idealised external fields of ionising radiation of relevance to occupational exposures. In this report, Committee 2 performed extensive Monte Carlo radiation transport simulations using Publication 110 (ICRP, 2009) adult reference phantoms, and considered monoenergetic fields of external photons, electrons, neutrons, protons, muons, pions, and helium ions. Values of effective dose, normalised to particle fluence incident to the exposed phantoms along six different irradiation geometries, are shown in Fig. 10A and 10B, respectively, for mono-energetic photons and neutrons. The report also compared these new external dose coefficients with the operational quantities of ambient, directional, and personal dose equivalent, reviewing their ability to assess the effective dose conservatively by radiation particle, energy, and irradiation geometry. Dose coefficients for both effective dose and sex-specific organ equivalent dose are provided in electronic formats that accompany Publication 116.
Examples of effective dose coefficients for exposures to uniform fields of external monoenergetic: (A) photons and (B) neutrons.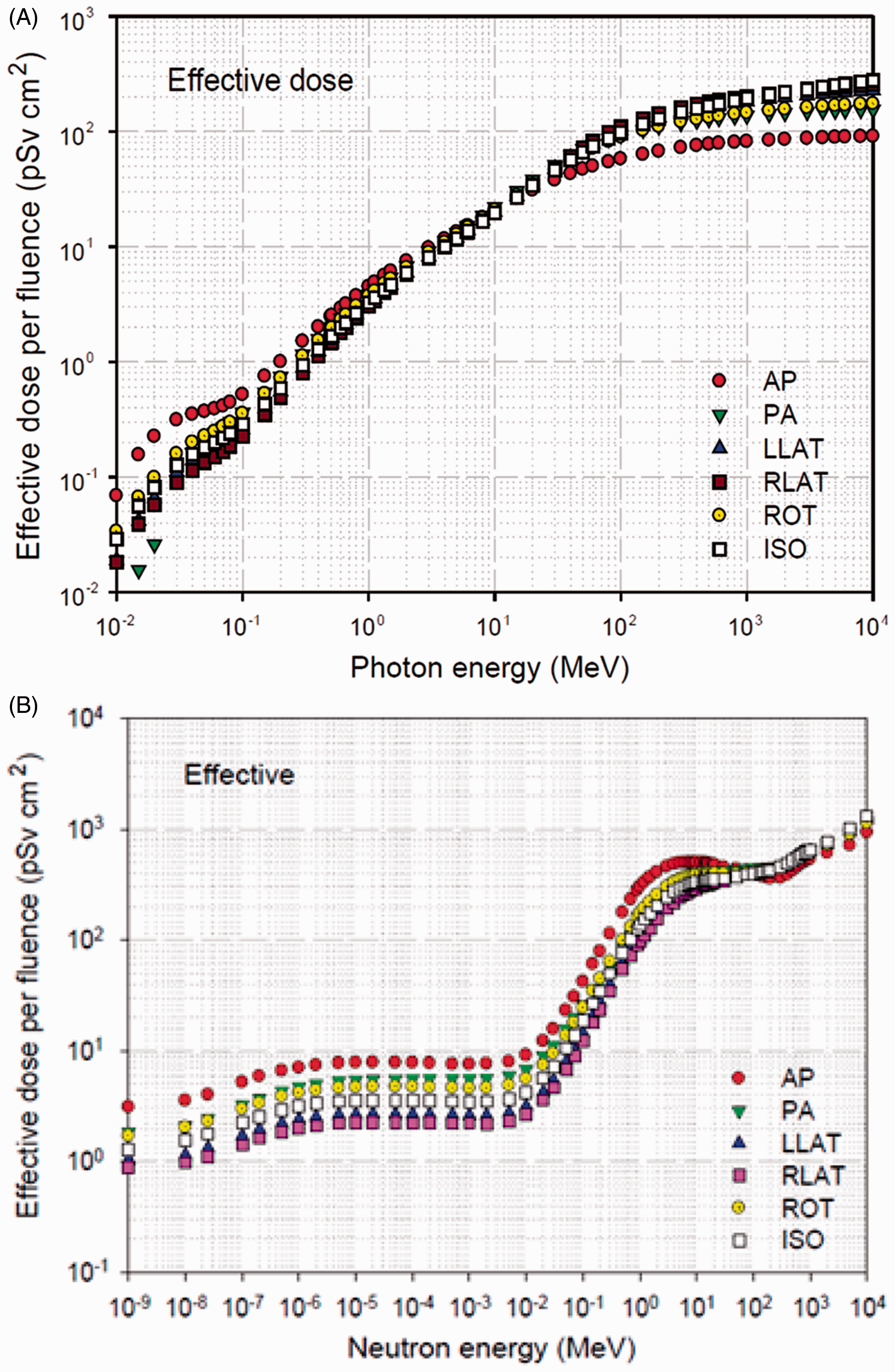
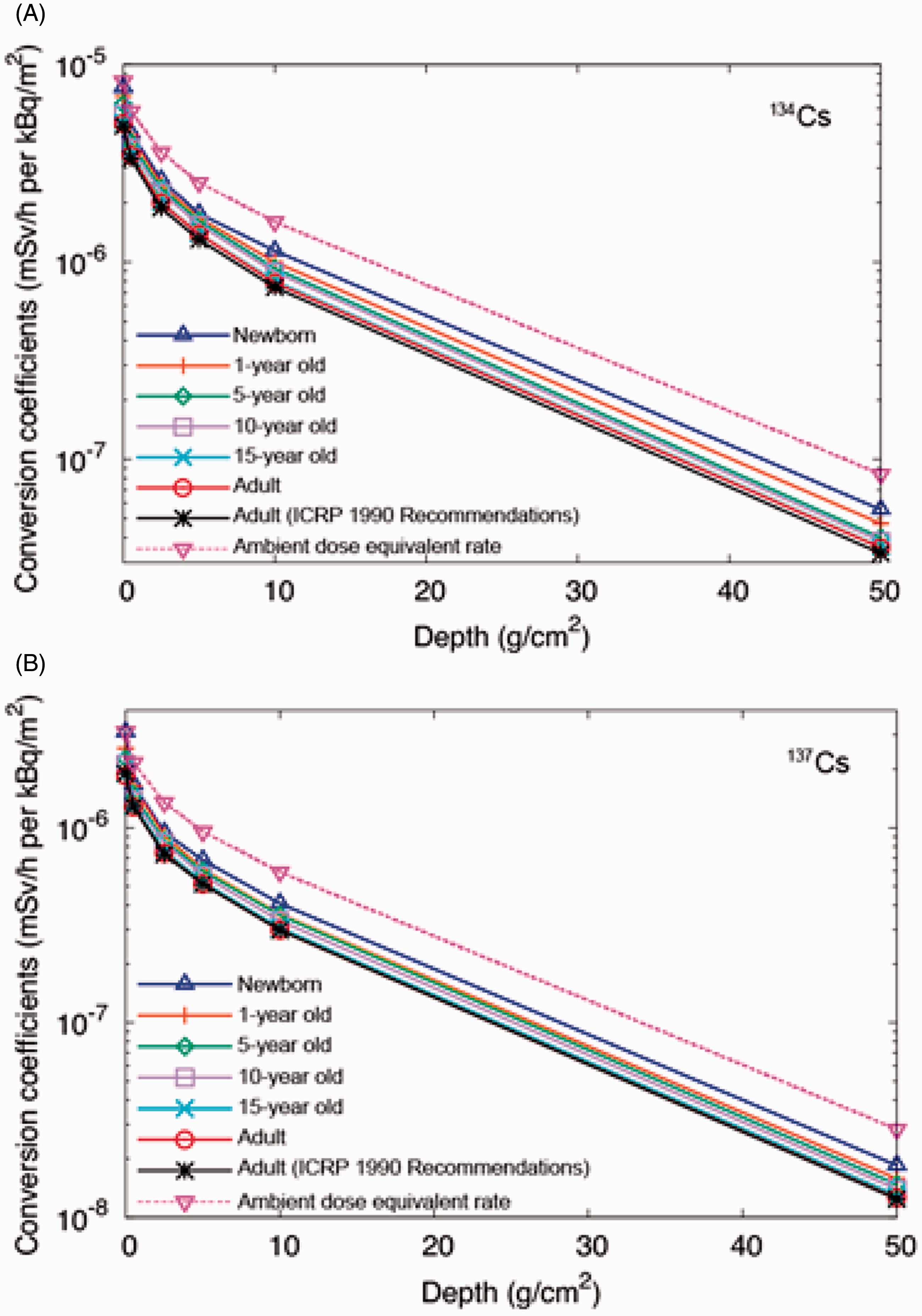
Following the nuclear accident in Fukushima, Japan, ICRP embarked on a major effort to produce reference dose coefficients for environmental radionuclide exposures using both Publication 110 (ICRP, 2009) adult reference phantoms, and the newly established ICRP paediatric reference phantoms of Fig. 8. This work is presently ongoing within Committee 2 and Task Group 90. As shown in Fig. 11, the computations are performed in two stages. First, environmental sources of external photons and electrons are simulated in the environment, and transported to a cylindrical coupling surface. At the cylindrical surface, the energies and angles (polar and azimuthal) are scored for a second series of transport calculations in which different computational phantoms (e.g. 1-y-old male or 15-y-old female) are inserted. In this fashion, environmental transport from modeled contaminated air or soil only needs to be performed once for each particle type and energy. Integration of the monoenergetic dose coefficients over the full emission spectrum of a radionuclide of interest thus yields the radionuclide-specific dose coefficient at a unit environmental concentration. For contaminated soil, the calculations are performed as a function of soil depth, after which one may consider differing soil concentration profiles as either measured or assumed. Example dose coefficients for soil contaminated with Cs-134 and Cs-137 are given in Fig. 12A and 12B, respectively (Satoh et al., 2015). In each case, values of the ambient dose equivalent are shown to conservatively estimate the effective dose rate per soil activity concentration, as a function of depth, and even for the most highly exposed individual (i.e. reference newborn).
Graphical depiction of the cylindrical coupling surface used for assessment of dose coefficients for environmental exposures. Examples of effective dose coefficients for exposure to soil contaminated with: (A) Cs-134 or (B) Cs-137 as a function of soil depth.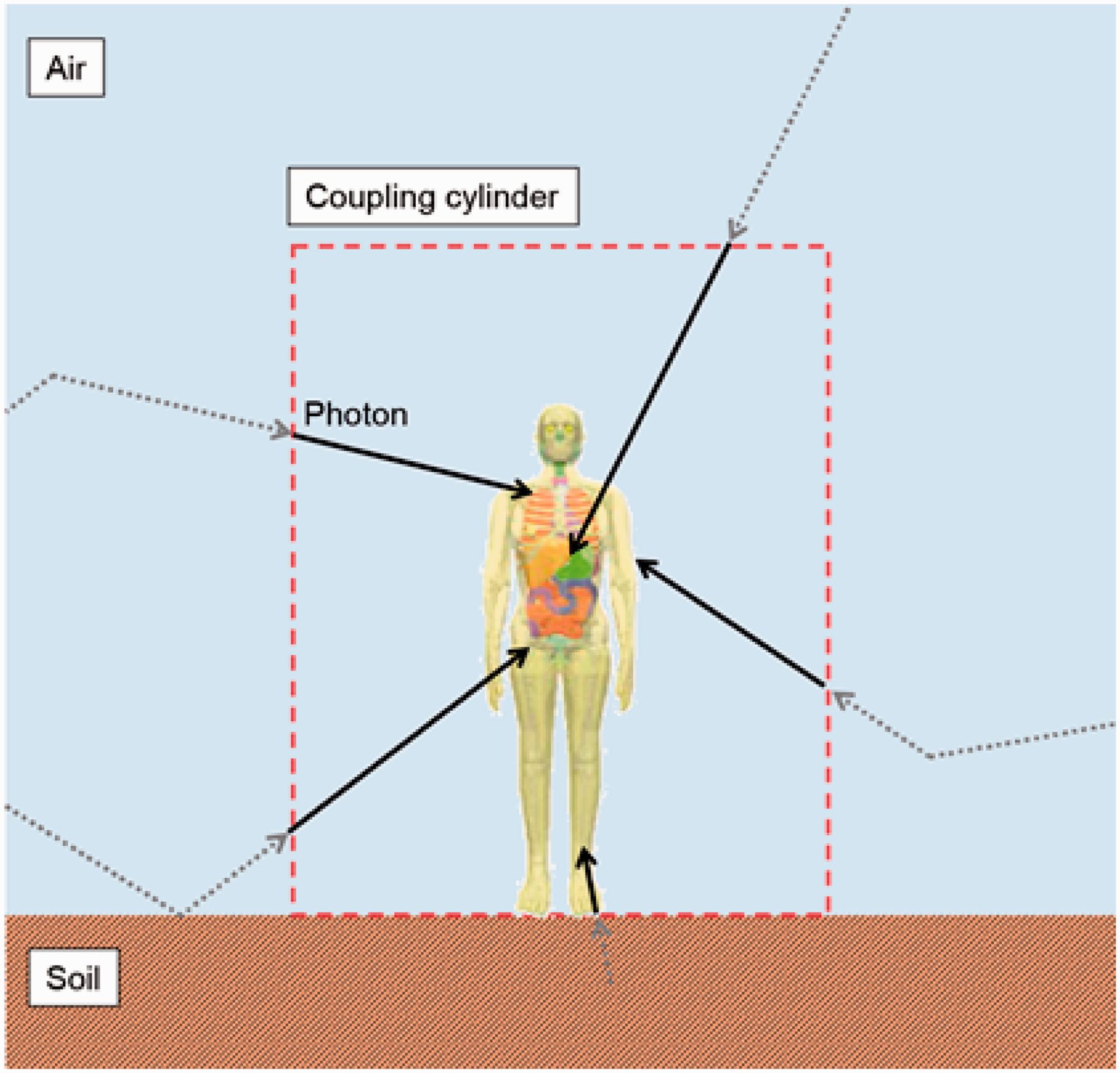
8. SUMMARY AND FUTURE DEVELOPMENTS
This paper has reviewed the computational framework for computing dose coefficients for both internal and external radiation fields as needed for both retrospective dose assessment and prospective planning for radiological protection. Three component models are needed to compute the dose coefficient. These are: (1) biokinetic models of radionuclide intake and systemic distribution; (2) models of radionuclide decay modes, particles, energies, and yields; and (3) anatomical models of the exposed individual, where they could be adult workers or members of the general public. While no further development of radionuclide decay data is envisioned within Committee 2 beyond those reported in Publication 107 (ICRP, 2008), further and ongoing work is being performed with respect to systemic biokinetic models and anatomical phantoms. Improved models will be applied to derive dose coefficients for workers, and dependent on the availability of informative data, age-dependent parameter values will be applied in the application of these models to specify dose coefficients for children. For pregnant females, Publication 88 (ICRP, 2001) provided detailed compartmental models for some elements that considered placental transfer and intrafetal radionuclide organ distribution explicitly. When human and/or animal data were limited, Committee 2 resorted to the use of ratios of organ activity concentrations in the fetus to that in the maternal organ. It is anticipated that newer data will permit Committee 2 to include more physiologically realistic maternal and fetal biokinetic models, and move further away from reliance on organ concentration ratios.
ICRP will issue new reports on reference paediatric and pregnant female phantoms. As with the adult reference phantoms of Publication 110 (ICRP, 2009), these reference anatomical models will be in the form of voxelised phantoms. While providing more anatomically realistic representations of internal anatomy than the older stylised phantoms, voxel phantoms have their limitations, especially with respect to small tissue structures (e.g. lens of the eye) and very thin tissue layers (e.g. stomach wall mucosa and stem cell epithelium). Committee 2 has thus employed more organ-specific stylised models in its work on internal photon, electron, and α particle SAFs that replace those computed directly in the computational reference voxel phantoms. Another example of this is the use of stylised models of the eye and skin as given in the annexes to Publication 116 (ICRP, 2010).
These issues have arisen due to two specific limitations in radiation transport computation. First, smaller structures in voxel phantoms can only be modelled by decreasing voxel resolution at the expense of total matrix size of the phantom. Second, radiation transport codes could only be utilised as their geometric input mathematical expressions (as in stylised phantoms) or cuboidal arrays (as in voxel phantoms). Newer generations of the Monte Carlo radiation transport codes, however, permit the input of computation phantoms assembled as polygon meshes, where organ surfaces and outer body contours are modelled using triangular arrays of vertices. As such, the very small structures that were crudely modelled in voxel phantoms, or left out altogether, can now be included in the structure of the reference phantom. These polygon mesh phantoms can thus include all the necessary source and target tissues defined by ICRP, thereby completely obviating the need for supplemental stylised models (e.g. respiratory airways, alimentary tract organ walls and stem cell layers, lens of the eye, and skin epithelial layers). This work of converting the voxelised phantoms of Publication 110 (ICRP, 2009) to polygon mesh models of the reference adults is an ongoing task for Committee 2 (Nguyen et al., 2015; Kim et al., 2016).