
Abstract
This paper presents ongoing actions in Dubai on patient dose monitoring in digital radiographic examinations, mammography, interventional procedures, and dental radiological procedures. The aim of Dubai Health Authority (DHA) is to move towards the establishment of local diagnostic reference levels. DHA has participated in national and regional projects under the umbrella of the International Atomic Energy Agency. The need for local radiation protection educational programmes and wider patient dosimetry monitoring and recording emerged from this work.
1. Introduction
Since 2005, the United Arab Emirates (UAE) has participated in the International Atomic Energy Agency’s regional technical co-operation projects. In these projects, radiology and medical physics teams at the Dubai Health Authority (DHA) managed to reduce patient radiation doses by up to 50% for common computed tomography (CT) examinations (head, chest, and combined abdomen and pelvis) (AlSuwaidi et al., 2013). Moreover, patient dose monitoring was initiated within conventional radiology practices, and was further enhanced with the introduction of digital radiology systems at DHA hospitals. This paper presents some DHA patient dosimetric data obtained from the practices of general radiology, mammography, interventional radiology, and dental radiology (both intra-oral and panoramic). The aim of this study was to evaluate radiation exposure levels to DHA patients, and to help to introduce steps towards establishing local diagnostic reference levels (DRLs) for common radiological examinations.
2. Patient Dose Monitoring and Diagnostic reference levels
In relation to patient dosimetry, one of the major differences between digital and conventional film-based radiology is the fact that the radiographers receive immediate and direct feedback related to the patient’s exposure in conventional radiology, by the white/dark appearance of the film. However, in digital systems, image brightness can be adjusted after processing, independent of the exposure level, and overexposure results in an image with less noise; as such, there may be no immediate indication of under- or overexposure. Underexposed images usually lead to the examination being repeated, which unintentionally increases exposure. On the other hand, the lack of negative impact on image appearance as a result of overexposure leads to a phenomenon known as ‘dose creep’; the gradual increase of dose. It is therefore imperative that dose monitoring is undertaken.
At DHA hospitals, an integrated Picture Archiving and Communication System (PACS) and a Radiology Information System (RIS) were installed for the radiology and nuclear medicine departments in 2008. The method of using PACS and the information available within the DICOM header to monitor CT dosimetry data was established at DHA hospitals to keep a record of patient radiation doses (AlSuwaidi et al., 2011a). The establishment of a local or national patient dose registry involves tracking all radiation doses, across all imaging modalities, and thereby aims to enhance the quality of radiology management.
Dose registry provides a dynamic tool for the management of patient exposure. Moreover, in digital radiology systems, cumulative doses can be tracked. However, the advantages of digital radiology systems are coupled with some difficulties related to the manual part that requires operator input, such as patient weight. In some systems, the radiographer has to enter the patient dose from the image modality to the RIS. Hence, automatic transmission of radiation doses from imaging modalities to PACS (and regular calibration of dose quantities) is essential for the establishment of a dose database.
In the UAE and the Gulf region, the actions taken to establish DRLs are very limited. In addition to improvements in patient safety, this dose assessment limitation has provided new opportunities for applied research.
3. Methods and Results
This paper presents DHA’s experiences in dose monitoring and local DRLs, along with comparisons with published international values. This DHA study, and those presented jointly between DHA and other healthcare organisations in the UAE (AlSuwaidi et al., 2011b), are the first published papers on patient dosimetry from the UAE.
3.1. General radiology
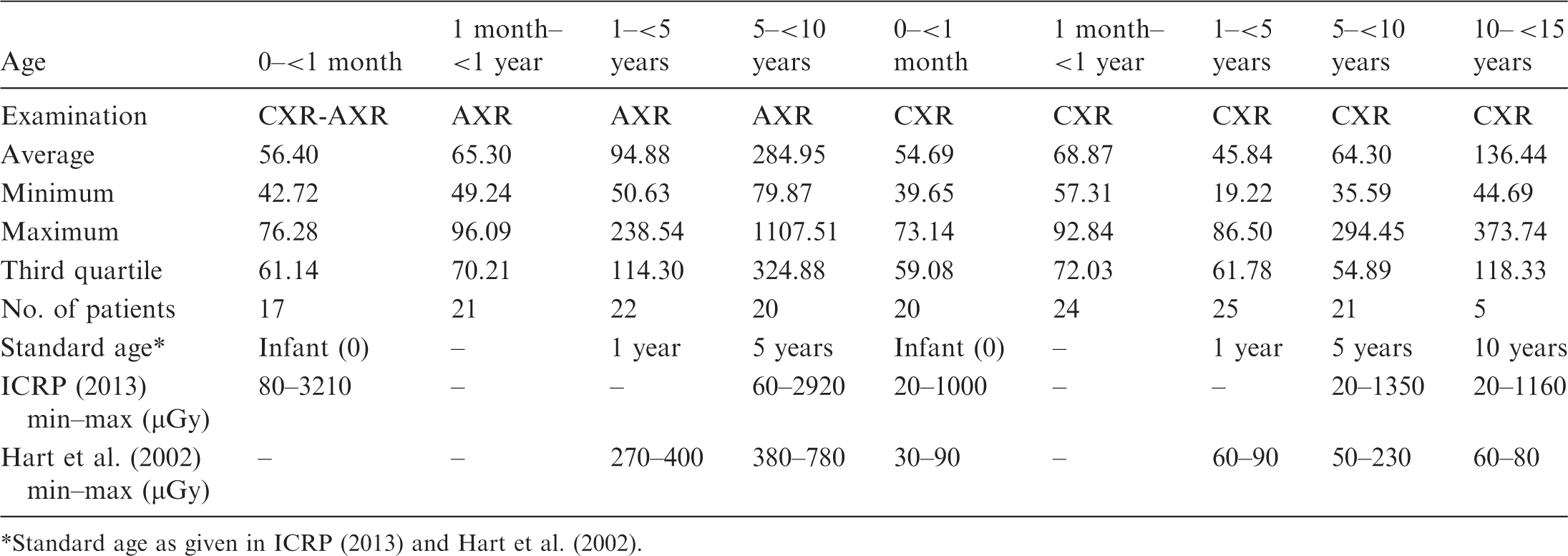
Paediatric and adult dose surveys on digital general x-ray machines are in progress at three primary healthcare hospitals and a children and women’s hospital (LH) within DHA. Chest radiography and full digital radiography using a built-in dose area product (also known as ‘kerma area product’) meter are used for general radiology at the children and women’s hospital and the primary healthcare hospitals, respectively. Dose variations between measured and displayed values, through measurements on phantoms, were examined for these general x-ray systems. The variation ranged from 2% to 29%. The authors aimed to collect dosimetric data for 20 patients in each age group who underwent common radiological examinations [chest, abdomen, pelvis, combined abdomen and pelvis, lumbar spine (antero-posterior and lateral)]. As indicated in Fig. 1, fewer than 20 patients were included in the abdomen and pelvis groups. Adult patient dose data from the MIZ clinic (primary healthcare hospital) are presented in Fig. 1 in comparison with UK values (Hart et al., 2012). Paediatric dosimetric data at the primary healthcare hospitals were not sufficient for analysis at this stage of the study. At the children and women’s hospital, dosimetric data were obtained from 175 patients who underwent chest and abdomen x-ray examinations. In paediatric patients, entrance surface doses given in Table 1 are within the same range as those cited in Publication 121 (ICRP, 2013) and Hart et al. (2002).
Entrance surface dose (mGy) at the MIZ clinic (primary healthcare hospital) compared with adult data from Hart et al. (2002). Incident air kerma (µGy) for chest (CXR) and abdomen (AXR) x-ray examinations in children at the children and women’s hospital. Standard age as given in ICRP (2013) and Hart et al. (2002).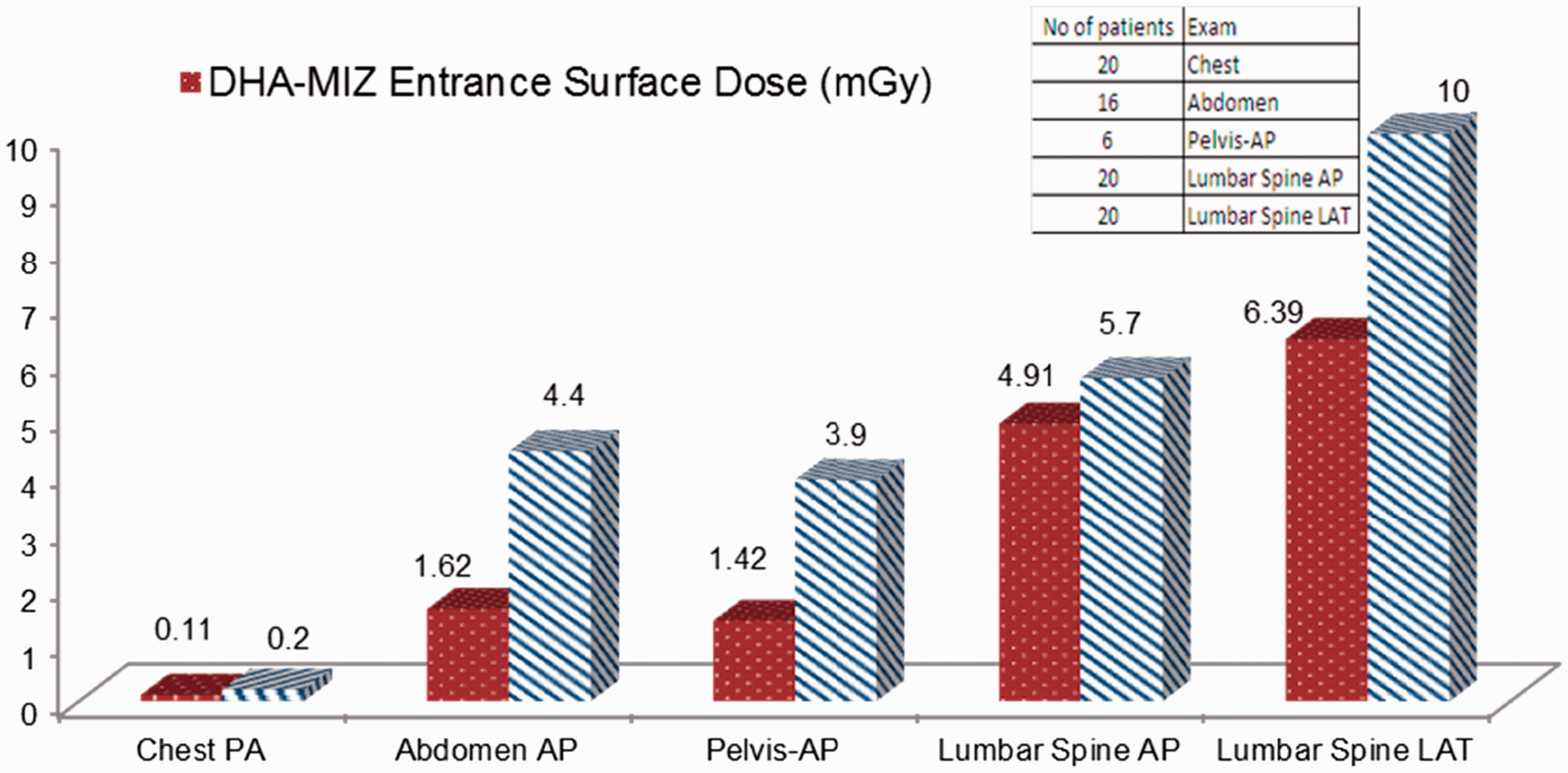
3.2. Mammography
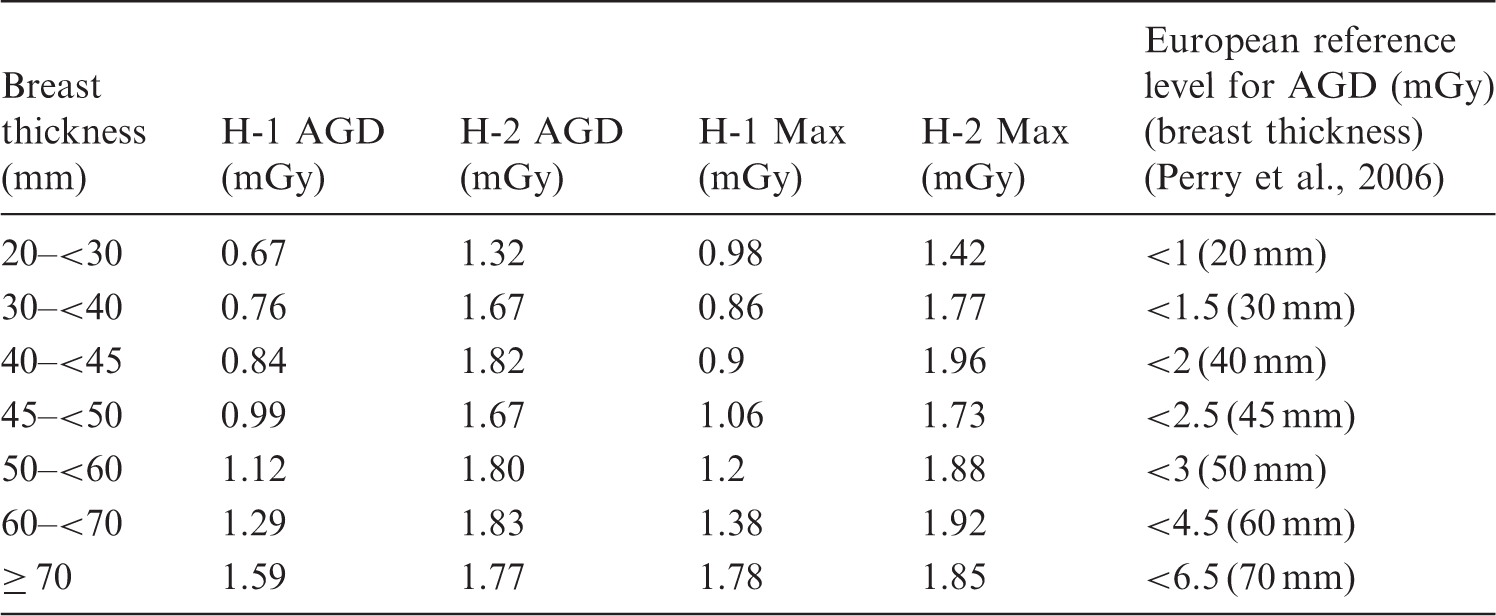
Average glandular dose (AGD) (in mGy) at Hospitals 1 (H-1) and 2 (H-2) within Dubai Health Authority.
3.3. Interventional procedures
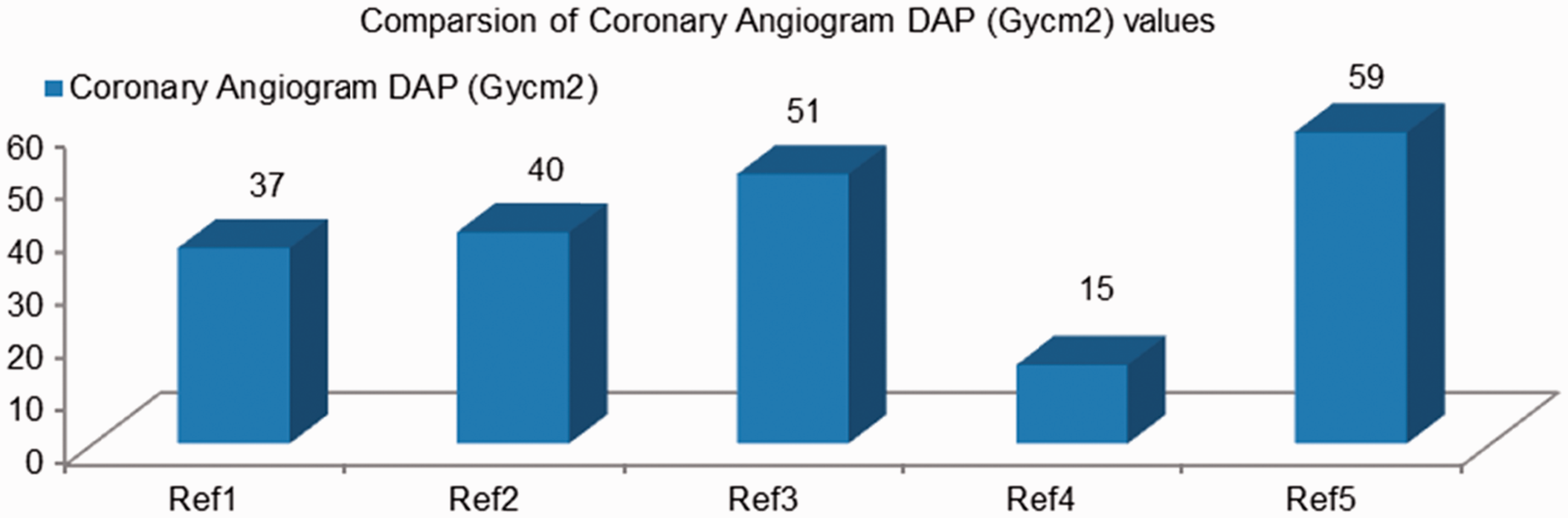
The Philips biplane flat detector system used for interventional procedures (IPs) at Dubai Hospital is fitted with a built-in kerma area product meter. Data were collected for 72 paediatric patients who underwent cardiac procedures. The majority of the cases were therapeutic (occlusion of patent ductus arteriosus, valvuloplasty, and left pulmonary artery ballooning and stenting). DHA’s paediatric results are shown in Fig. 2. Average fluoroscopy times for the frontal C-arm (Plane A) were 7.13, 4.02, and 6.42 s for age groups 0–<1 year, 1–<5 years, and 5–<10 years, while for the lateral C-arm (Plane B), corresponding results were 7.14, 2.81, and 2.22 s. The adult data were based on 30 patients (10 patients for each cardiac procedure) for coronary angiography, coronary angioplasty, and peripheral angioplasty. The dose values from coronary angiography are presented in Fig. 3, along with other published IP dose values (Kuipers et al., 2012) for comparison purposes. DHA’s coronary angiography sample was mixed (femoral and radial access), while all data from Kuipers et al. (2012) were for radial access. UNSCEAR presented IP dosimetric values in the range of 12.7–147.43 Gy cm2 (UNSCEAR, 2008). The wide range of IP dose data is mainly due to the complexity of IPs. The average fluoroscopic time for coronary angiography was approximately 2 min. The doses from the other two adult cardiac procedures showed a wide range of values. Hence, further IP dosimetric data collection is in progress as the present data are not sufficient to propose representative local DRLs.
Dubai Health Authority interventional procedure doses in children. DAP, dose area product; KAP, kerma area product. Dubai Health Authority (DHA) interventional procedure doses in adults. Ref1, DHA, 2013, Dubai; Ref2, Kuipers et al. (2012), Netherlands; Ref3, Sandborg et al. (2004); Ref4, Lange et al. (2006); Ref5, Brasselet et al. (2008), all cited in Kuipers et al. (2012). DAP, dose area product.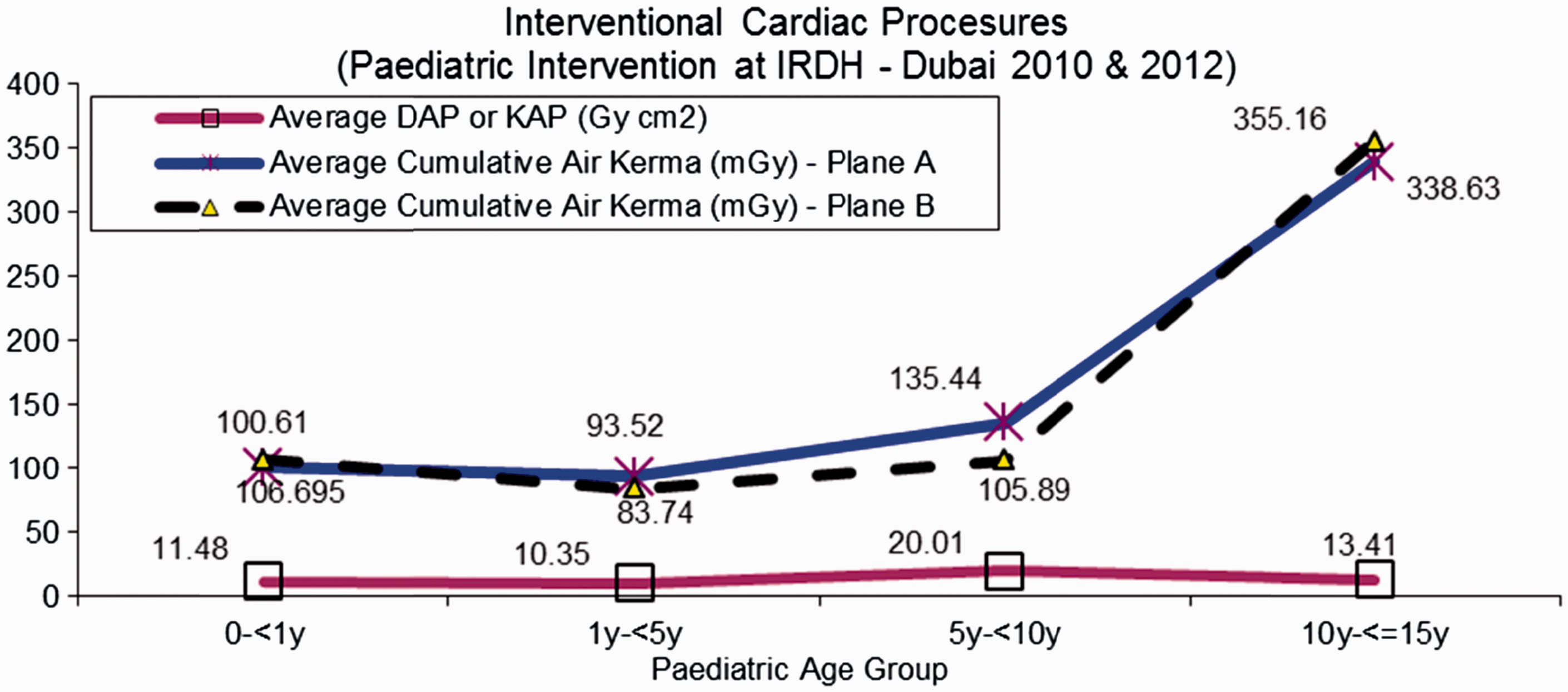
3.4. Dental radiology
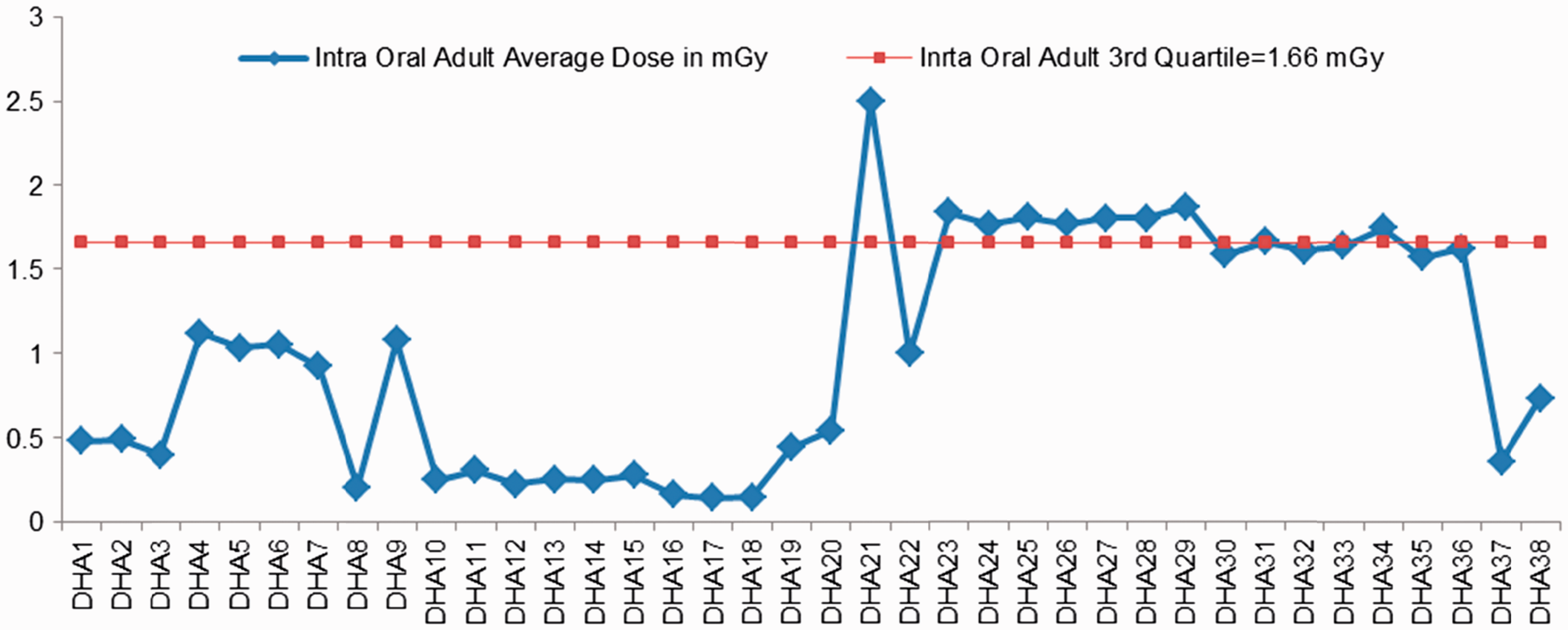
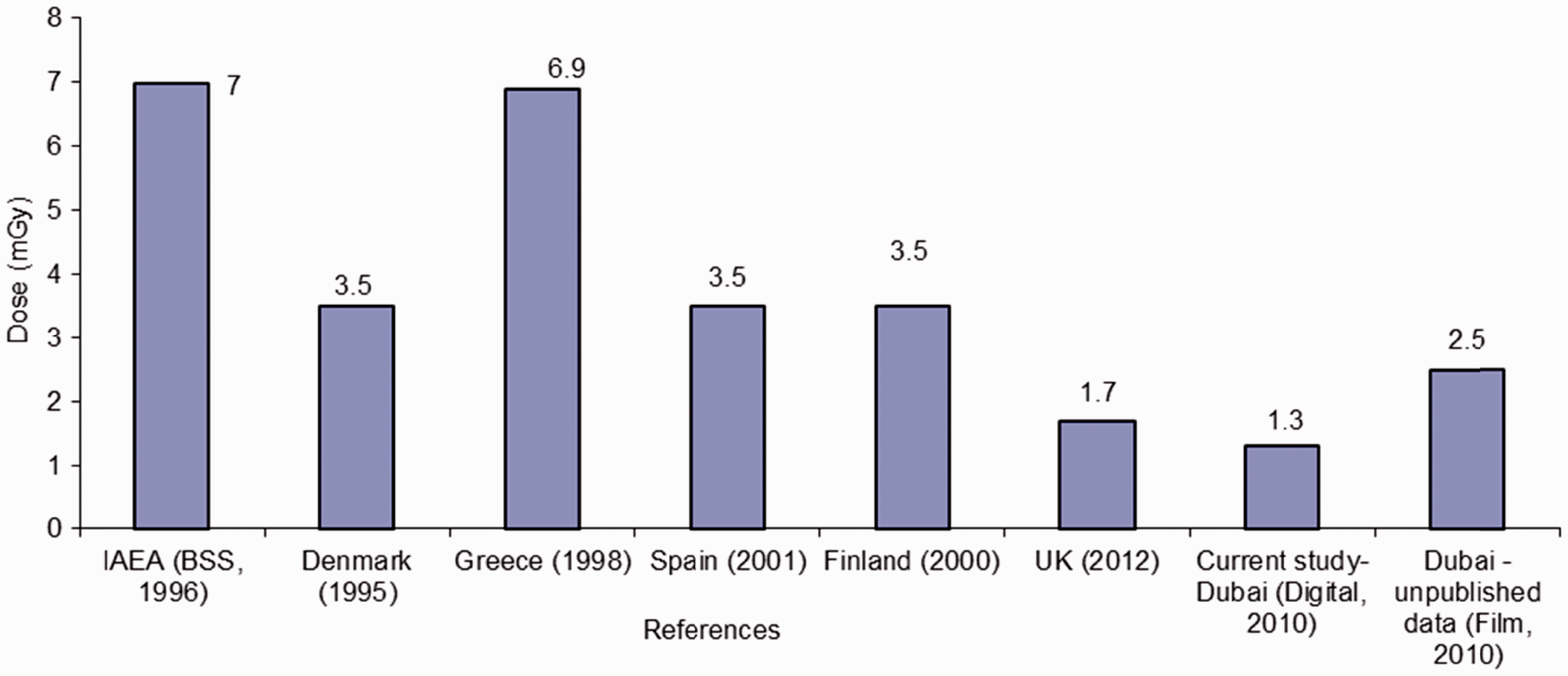
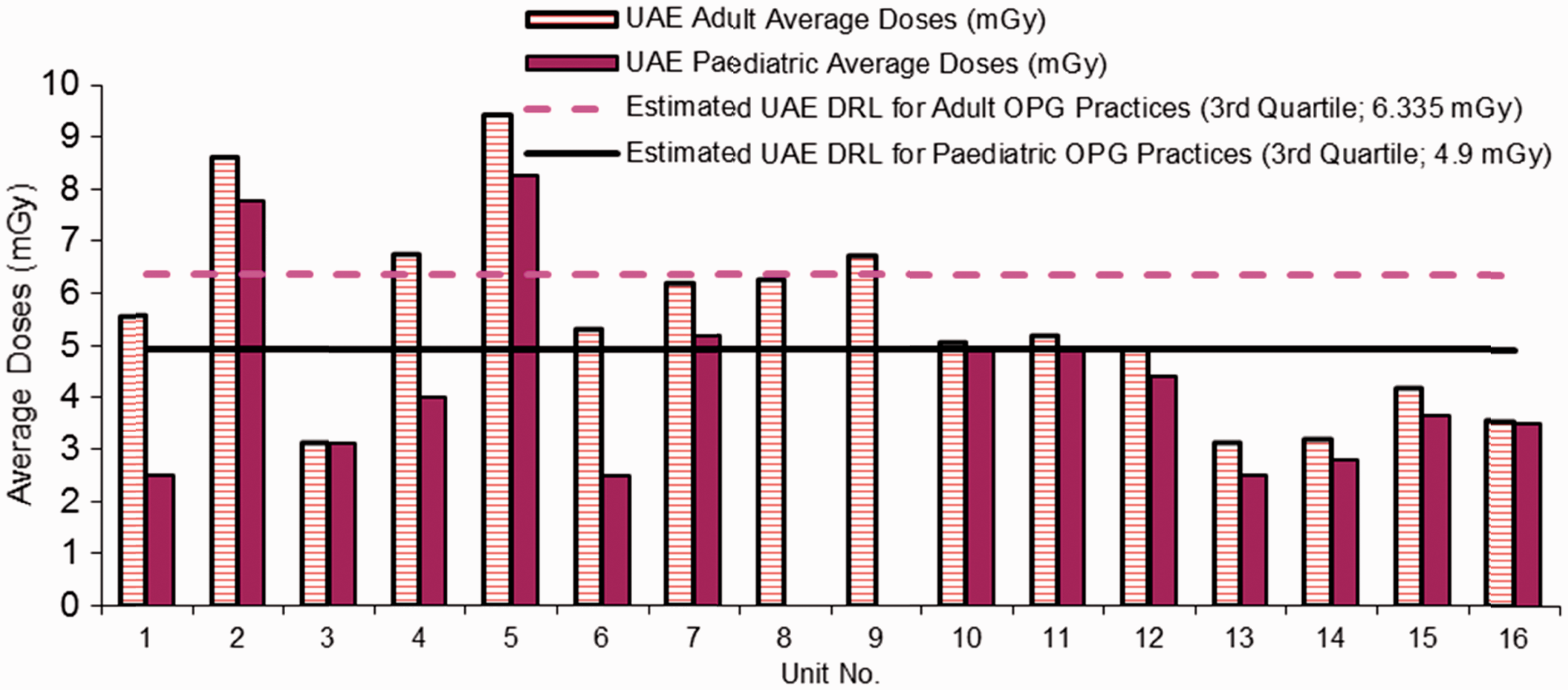
Sixty intra-oral machines (22 conventional film-based intra-oral x-ray machines and 38 digital intra-oral x-ray machines) and nine panoramic (OPG) dental radiology units were included in DHA’s survey. This study presents the dosimetric results of digital intra-oral and OPG systems. Radiation exposures from intra-oral machines were measured using an electronic dental dosimeter (Multi-O-Meter, UNFORS, Billdal, Sweden). The dose survey for the OPG machines was performed using a CT cylindrical ionisation chamber. Exposure parameters implemented in this work reflected those used in clinical situations. The exposures for the intra-oral machines were measured in air at the end of the spacer cone; this estimated the patient entrance dose. Measurements were taken for common intra-oral views: apical (anterior view), pre-molar, molar (posterior view), and bitewing views. This study presents the intra-oral molar (posterior view) dosimetric data in order to compare the results with a UK review undertaken in 2010 and other international references (EC, 2004; Hart et al., 2012). These results are shown in Figs 4–6. Exposures for the OPG systems were measured as the dose at the surface of the image receptor; these results are shown in Fig. 7.
Dubai Health Authority’s intra-oral dose survey (posterior view) in paediatric patients. Dubai Health Authority’s intra-oral dose survey (posterior view) in adult patients. Comparison of intra-oral dose values from Dubai Health Authority with international references* for adults. *References: IAEA (1996), Denmark (1995), Greece (1998), Spain (2001), and Finland (2000) are cited in EC (2004); UK (2010) is cited in Hart et al. (2012). Dubai Health Authority’s panoramic (OPG) dental radiology unit dose survey, 2010–2011, in children and adults. Thanks to Jacek Janaczek and Fatima Al Kaabi, Tawam Hospital, SEHA, UAE for OPG data from seven machines (10–16).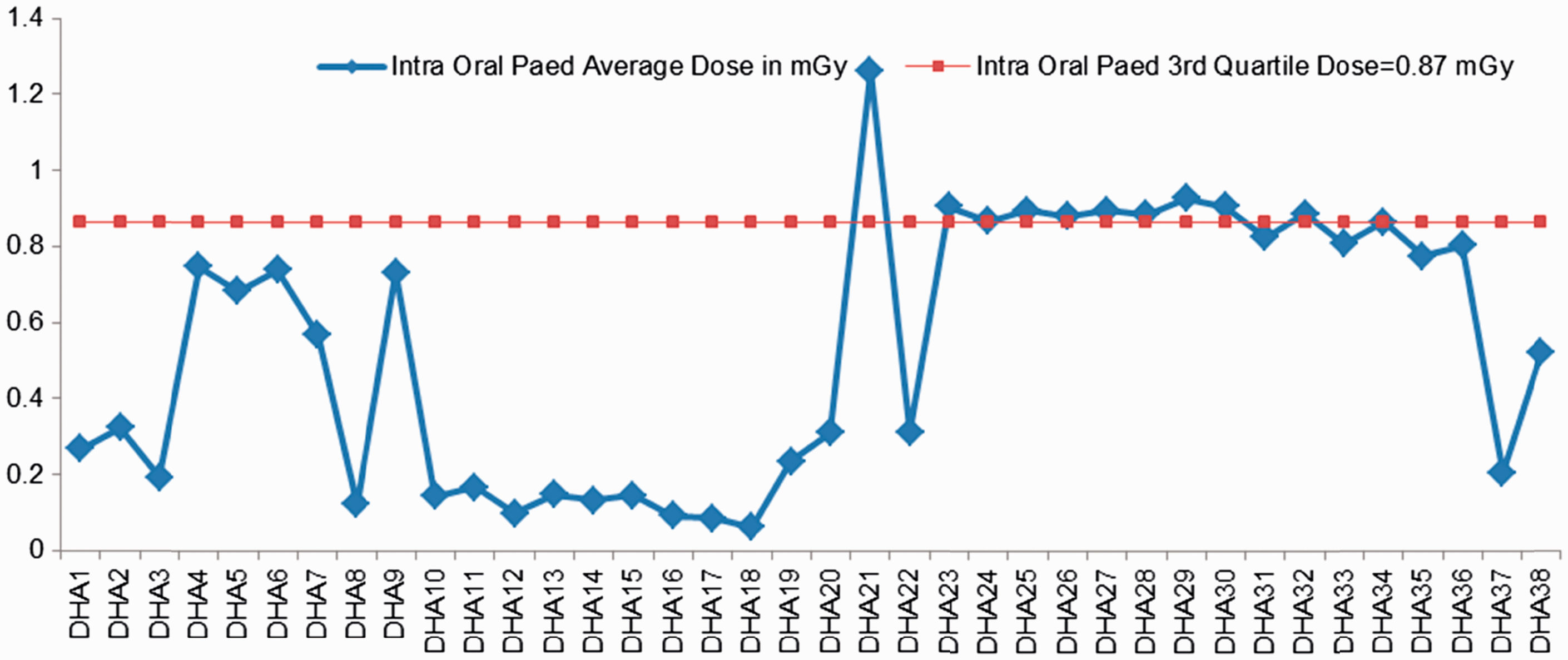
4. Discussion
This article has presented DHA’s patient dose monitoring data; this is the first such study in the UAE. The radiation dose levels compare favourably with those published in the literature. For adult patient doses in general digital practice, doses are lower than those reported by Hart et al. (2012). Furthermore, paediatric entrance surface dose results in this study are within the same range as those mentioned in Publication 121 (ICRP, 2013) and Hart et al. (2002). The literature indicates large variations in paediatric DRLs, and there is no standardisation in quoting these values. The authors have not been able to obtain adequate data for the 10–15-year age group, mainly because the paediatric age group used by DHA is up to 13 years (the age group in this study was up to 15 years to correspond with the common paediatric age group used worldwide). Patient data collection for adult and paediatric groups is currently in progress. DHA mammography results are lower than those reported in a European publication, and the range of dose levels among different breast thicknesses also show lower variation (Perry et al., 2006). However, the results for H-2 did not show the expected increase in dose level with increasing breast thickness. The phantom results of H-2 showed a large degree of variation. As the same individual performed the work at H-1 and H-2, and the results of H-2 were repeated for verification purposes, the variation is likely to be due to the conversion factor used by the software in the mammography system. The conversion factor is not mentioned in the DICOM header. DHA’s results for IP dosimetric monitoring are limited, and the authors intend to obtain further dose data and cover further IPs. The dental dosimetric survey in this study included dental systems that existed at DHA between 2010 and 2011. However, as the dental data were collected as digital dental radiology was introduced, and new dental systems have since been purchased, it is worth undertaking a dose survey review. The authors aim to continue to collect data, and emphasise the need to collect further data on patient dose in order to obtain significant population samples for adult and paediatric patient groups.
Recording and audit of patient radiation exposure are considered to represent integral elements of a quality assurance programme (RCSI, 2011); however, to date, they have not been fully implemented by DHA. Standardisation of automated dose evaluation by manufacturers is required, and this will help to improve patient radiation safety. Automated DICOM dose extraction techniques are essential to handle large samples of patient dosimetric data. A lack of qualified experts and medical physicists in the study region hinders progress in research work related to patient radiation dosimetry and safety.
In conclusion, the authors believe that the following issues are of great importance in patient radiation safety in the UAE:
support of educational programmes; education and instruction of radiology teams to avoid overexposure and ‘dose creep’ in digital radiology practices; recommendation of simple methods for patient dose evaluation, and emphasis on dose recording within patients’ medical reports; and a uniform, accurate, and calibrated dose registry at local and national levels.
This study suggests that there is a need to develop further radiation protection and education programmes, along with patient dosimetric monitoring and recording, within the UAE. These radiation protection requirements are considered to be an essential prerequisite to a radiation safety culture within the healthcare community. An educational programme, DHA’s Radiation Protection Educational Programme, has now been established; this is delivered on a regular basis (every 3–4 months), and is attended by radiologists, radiographers, medical physicists, biomedical engineers, and quality administrative officers from various areas within the UAE. It is hoped that this will facilitate extensive national patient dose monitoring in the future.