
Abstract
Background
In-office endoscopic sinonasal procedures under local anesthesia are gaining popularity for managing chronic rhinosinusitis (CRS), reducing wait times and costs. However, concerns remain regarding safety and efficacy.
Objective
To investigate the safety and efficacy of in-office endoscopic sinonasal procedures up to one year postoperatively.
Methods
A retrospective review was conducted of adult patients (≥18 years) with CRS who underwent an in-office endoscopic sinonasal procedure under local anesthesia between January 2020 and December 2023. Patients were excluded if they were diagnosed with a sinonasal tumour. Safety was assessed using adverse events and complication rates, while efficacy was assessed with endoscopic visualization.
Results
A total of 165 patients were included. Intraoperative complications were rare, with two (1.2%) occurring in the CRS cohort. Four episodes of postoperative bleeding (2.5%) occurred, with two (1.3%) emergency department visits and one (0.6%) hospital admission. The median Modified Lund-Kennedy score (n=89) decreased from 4/12 to 3/12 at three (p = 0.0004) and six (p = 0.03) months postoperatively, and to 2/12 at twelve months postoperatively (p = 0.003).
Conclusion
In-office endoscopic sinonasal procedures are a safe, effective, and well-tolerated treatment alternative for appropriate patients with CRS. This represents the largest Canadian study to date evaluating in-office endoscopic sinonasal procedures for CRS.
Keywords
Introduction
Endoscopic sinus surgery (ESS) is an effective treatment for chronic rhinosinusitis (CRS) that cannot be effectively managed with maximal medical therapy.1-3 It is typically performed under general anesthesia in an operating room. However, in-office procedures carried out in outpatient ambulatory settings using local anesthesia alone are being increasingly performed thanks to technological advancements over the past decade.4-6
Wait times for elective procedures in Canada’s burdened healthcare system can be substantial. Among CRS patients, patient-reported outcome measure (PROM) scores and medication use increase from the time of consent to the actual operation. 7 Additionally, severely prolonged surgical wait times can result in less overall symptom improvement postoperatively.8-10 In-office endoscopic sinonasal procedures provide a solution to extended wait times as they bypass the need for pre-operative preparation, operating room scheduling, and enable a faster postoperative recovery.5,6 Decreased healthcare costs are also a direct result, as a typical in-office endoscopic sinonasal procedure costs ∼$2,700 USD, compared to ∼$7,300 USD for ESS under general anesthesia. 11
Prior studies have demonstrated that in-office endoscopic sinonasal procedures are both safe and effective, leading to improvements in patients’ quality of life.4,5,12,13 However, the potential intraoperative and postoperative complications are not well described in the literature, and further data is needed to better characterize postoperative outcomes across broader Canadian patient populations.5,12-14 Despite its increased adoption and known benefits, some surgeons remain hesitant to perform in-office endoscopic sinonasal procedures for CRS due to potential safety and efficacy concerns. The objective of this study was to quantify the immediate postoperative outcomes of in-office endoscopic sinonasal procedures for CRS, as well as the effectiveness of in-office endoscopic sinonasal procedures for CRS for up to one year postoperatively.
Materials and Methods
Inclusion and Exclusion Criteria
Patients were included if they were ≥ 18 years of age, diagnosed with CRS, and had undergone an in-office endoscopic sinonasal procedure between January 2020 - December 2023. Patients were excluded if they had been diagnosed with a sinonasal tumour at the time of their procedure or if they were scheduled for a sinonasal biopsy.
Data Collection
All data obtained were collected retrospectively from adult CRS patients seen at a Canadian tertiary center between January 2020 - December 2023. Collected variables included patient demographic information, medical history, procedure characteristics, safety outcomes, and clinical outcomes. Efficacy was assessed using Modified Lund-Kennedy (MLK) scores. For estimated blood loss (EBL), procedures were categorized as limited if the patient had a single, isolated sinonasal procedure performed, and extensive if the patient had two or more sinonasal interventions performed during the same procedure.
Office Procedures
All in-office procedures were performed by trained rhinologists. Patients were diagnosed with CRS based on the European Position Paper on Rhinosinusitis and Nasal Polyps 2020 criteria.
2
Patients were deemed appropriate candidates for an in-office procedure if they experienced medically recalcitrant CRS. Prior to the procedure, instructions were sent to each patient to be educated on the perioperative period, including procedural steps, potential risks, and alternative options. Selection was additionally determined based on anticipated procedural complexity, suitability for local anesthesia, tolerability of an awake procedure, and patient preference through shared decision making. The extent of each procedure was individualized based on clinical symptoms, endoscopy, and imaging when applicable. Although all procedures were planned preoperatively, occasionally intraoperative findings necessitated modification of the procedural plan. During the procedure, patients were seated in the semi-recumbent position in an operating room bed in an outpatient surgical procedure room (Figure 1). Next, 4% lidocaine-soaked neuropatties were applied to the areas relevant for the procedure, followed by infiltration of 0.25% bupivacaine or lidocaine with 1:200,000 epinephrine in the areas that would be operated on. When required, additional topical or local anesthetic was administered intraoperatively to improve patient comfort. Outpatient surgical procedure room used for in-office endoscopic sinonasal procedures, equipped with surgeon and patient monitors, an endoscopic tower, vital sign monitors, and a crash cart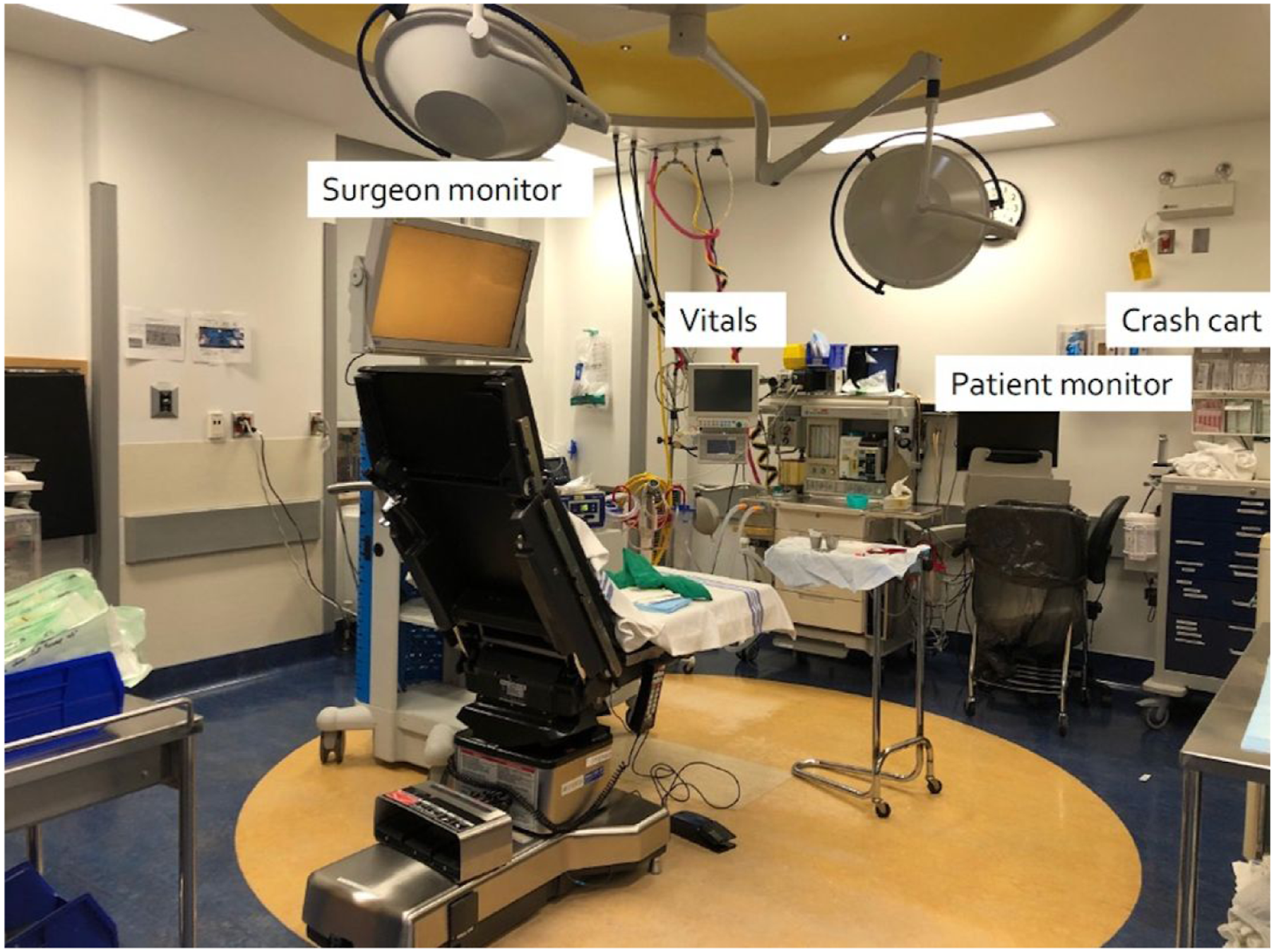
Equipment utilized was tailored to each procedure, however for all cases, the following equipment was required: curved suctions (double bent Kuhns suctions), separately peel wrapped instruments, access to all operating room equipment, 0, 30, and 70 degrees three- and four-millimeter angled Karl Storz endoscopes, a Karl Storz endoscopic tower (Germany), blood pressure and oxygen saturation monitoring devices, an automated external defibrillator, an oxygen tank, and a crash cart. Throughout each procedure, the patients’ blood pressure, oxygen, and comfort levels were monitored to minimize the risk of intraoperative complications. Two registered nurses were present throughout the procedure to assist the surgeon and monitor the patient. In an effort to minimize posterior blood flow into the pharynx, continuous suctioning was provided to maintain a clear surgical field, with hemostasis achieved prior to proceeding with further intervention. Patients were observed for ten minutes postoperatively to ensure no immediate complications and instructed to perform saline nasal irrigation with corticosteroids twice daily starting on the evening of the procedure and until their next clinic visit. Select patients were also instructed to apply mupirocin in their saline nasal irrigations.
Complications and Measures of Disease Severity
Postoperative complications of note were pain, bleeding, emergency department (ED) visits, and hospital admissions. Postoperative pain was defined as pain within the first two postoperative weeks that required additional analgesics. Postoperative bleeding was defined as any sinonasal bleeding (i.e., epistaxis) that occurred within two weeks after the procedure that required medical assistance of any kind. To assess the effectiveness of in-office procedures for CRS, baseline MLK scores were compared to scores obtained at 3-, 6-, and 12-months postoperatively. Patients with multiple follow-up visits contributed to more than one timepoint-specific comparison, but all analyses were conducted independently. The MLK endoscopic scoring system quantifies CRS severity based on the endoscopic appearance of polyps, edema, and discharge within the sinuses. 15 In cases where MLK scores were not explicitly documented in the patient chart, values were calculated using the SinoNasal Endoscopic Score (SiNES), which is recorded during every visit at our clinic. 16 Following the SiNES methodology, the highest domain score per side was used to represent disease severity and converted to the corresponding MLK score.
Data Analysis
Descriptive statistics were calculated for all safety and efficacy outcomes. Median changes from baseline and interquartile ranges (IQRs) for MLK scores were assessed at 3, 6, and 12 months postoperatively using the Wilcoxon signed-rank test. Ninety-five percent confidence intervals (CIs) were generated using bootstrap resampling with 2,000 replicates. Differences in estimated blood loss between limited and extensive procedures were evaluated using the Wilcoxon rank-sum test, and 95% confidence intervals were calculated using the Hodges-Lehmann method. All tests were two-sided, and a p-value <0.05 was considered statistically significant. Descriptive statistics and statistical analyses were calculated and performed using R version 4.4.2. 17
Ethics
This study protocol was approved by our local research ethics board (REB Number: H24-00042).
Results
Demographics
Demographics of CRS Patients (n = 165)
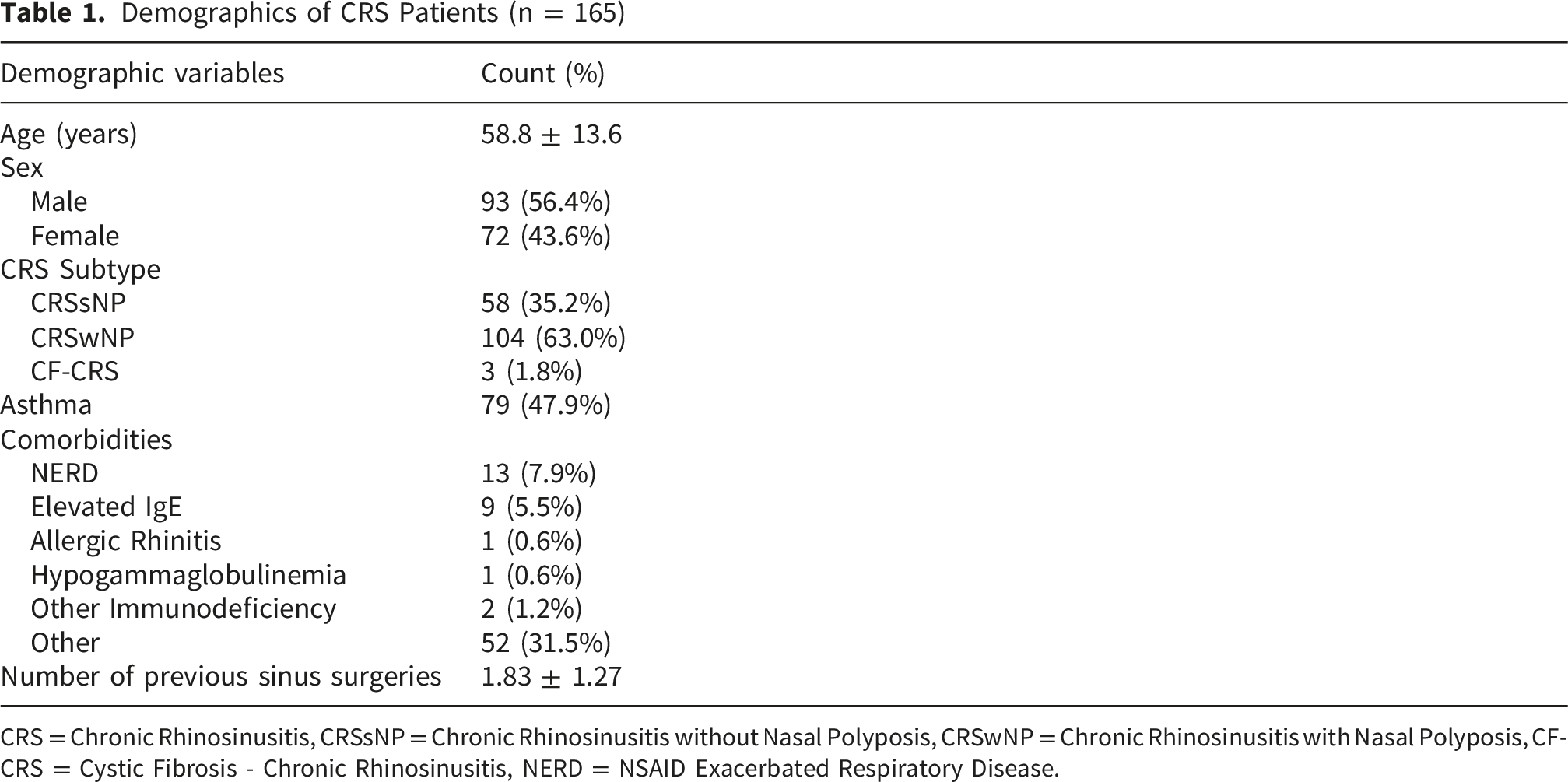
CRS = Chronic Rhinosinusitis, CRSsNP = Chronic Rhinosinusitis without Nasal Polyposis, CRSwNP = Chronic Rhinosinusitis with Nasal Polyposis, CF-CRS = Cystic Fibrosis - Chronic Rhinosinusitis, NERD = NSAID Exacerbated Respiratory Disease.
Procedure Characteristics
Characteristics of in-Office CRS Procedures
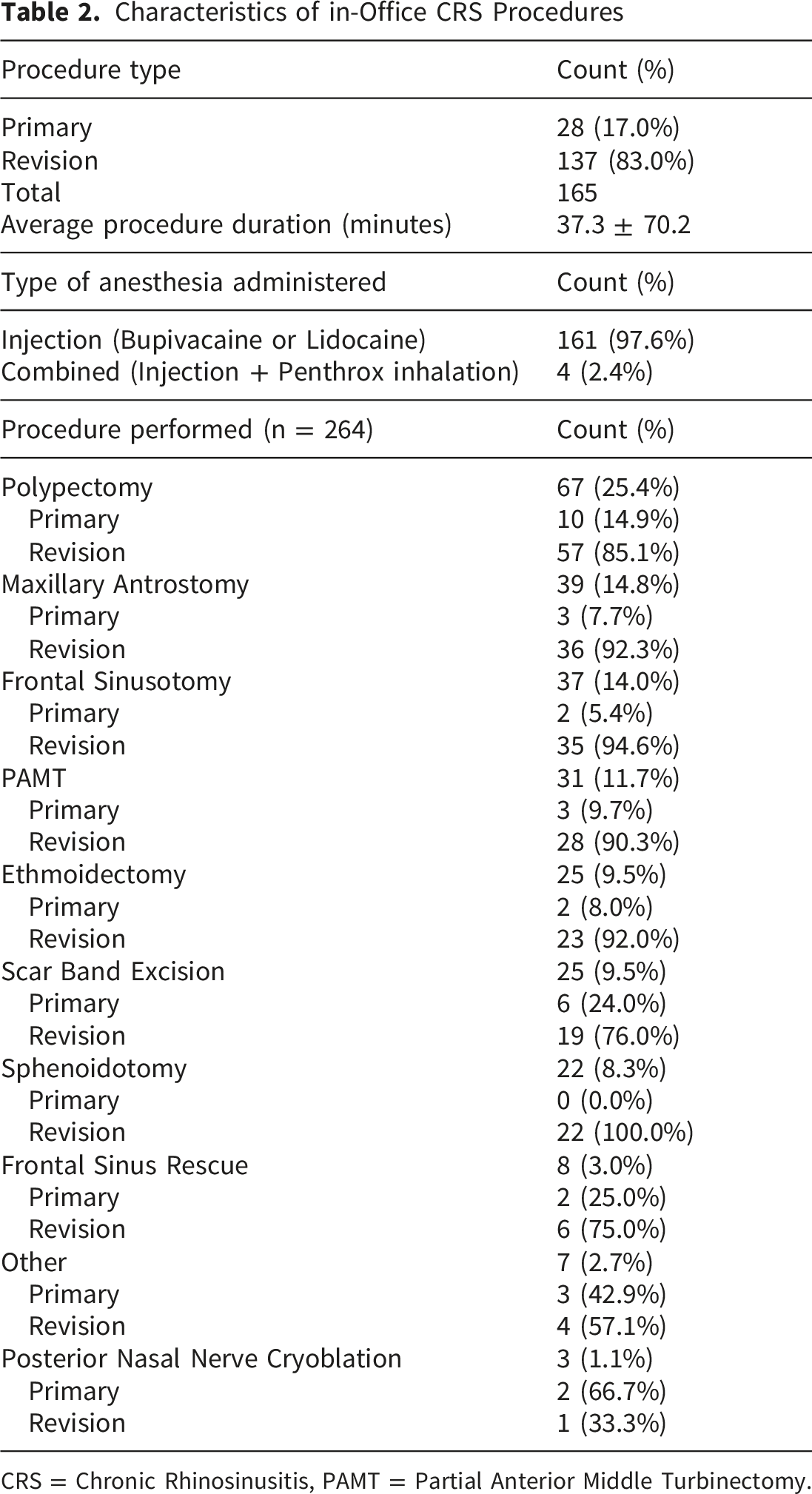
CRS = Chronic Rhinosinusitis, PAMT = Partial Anterior Middle Turbinectomy.
During in-office procedures, EBL was minimal. The overall median EBL (n = 149) was 20 ml (IQR 20-50). For limited procedures (n = 74), the median EBL was 20 ml (IQR 12.5 – 50), compared to 25ml (IQR 20-50) for extensive procedures (n = 75). Although EBL was higher in the extensive group, there was no statistically significant difference (95% CI: -1 to 0; p = 0.069).
Complications
Safety Characteristics and Postoperative Outcomes
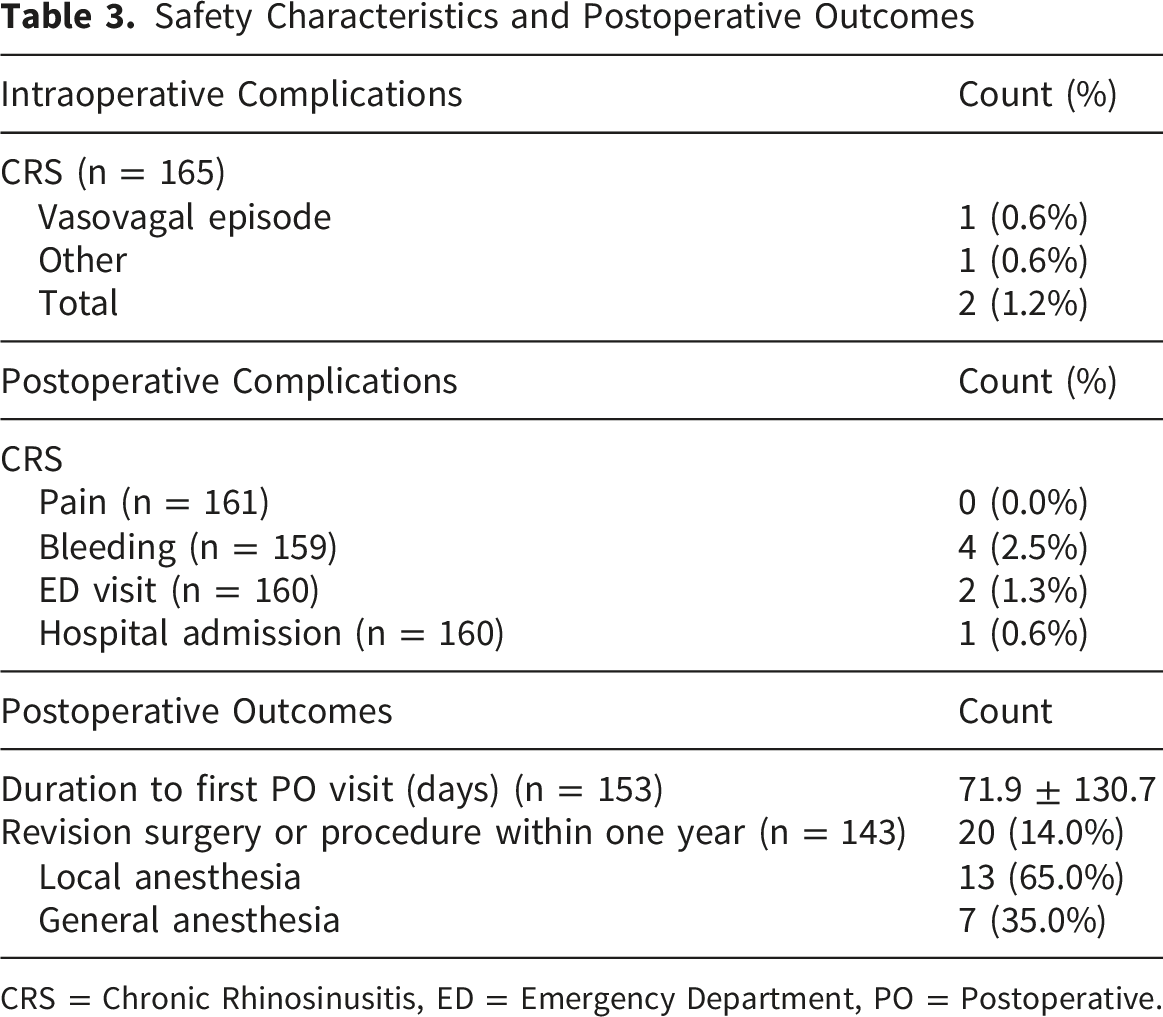
CRS = Chronic Rhinosinusitis, ED = Emergency Department, PO = Postoperative.
Clinical Outcomes
The mean duration to the first postoperative follow-up visit for the CRS cohort was 71.9 days (±130.7) (Table 3). Within one year, 20 (14.0%) patients underwent revision surgery. Of these cases, 13 (65.0%) were dealt with similarly to the initial procedure, and 7 (35.0%) procedures were performed under general anesthesia. Nine additional patients underwent in-office procedures as bridging interventions for symptomatic relief while awaiting already scheduled ESS under general anesthesia. As a result, these cases were excluded from the revision rate analysis as they represented planned management rather than true revisions. The subset of patients who underwent revision surgeon under general anesthesia exhibited persistent or refractory sinonasal symptoms typically localized to the initially treated sinus, suggesting more severe CRS disease. Similarly, patients who underwent revision surgery with an in-office procedure demonstrated persistent symptoms that were not severe enough for surgery under general anesthesia.
A total of 89 patients had MLK scores recorded at baseline and at 3, 6, and/or 12 months postoperatively (Figure 2). The median baseline MLK score of 4/12 (IQR 2-7) decreased by one point to 3/12 at three (IQR 0-5; p = 0.0004) and six months (IQR 0.25-5; p = 0.03) postoperatively, and further decreased to 2/12 at twelve months (IQR 0-5.25; p = 0.003) postoperatively. Change in MLK scores from baseline at 3, 6, and 12 months following an in-office sinonasal procedure (n=89, across all timepoints). The median baseline MLK score was 4/12, which was decreased to 3/12 at three and six months postoperatively, and to 2/12 at twelve months postoperatively. Each dot represents an individual patient’s change in MLK score relative to their baseline. The horizontal dashed line indicates no change from baseline. Black error bars represent 95% confidence intervals. *p < 0.05, **p < 0.005, ***p < 0.0005. MLK = Modified Lund-Kennedy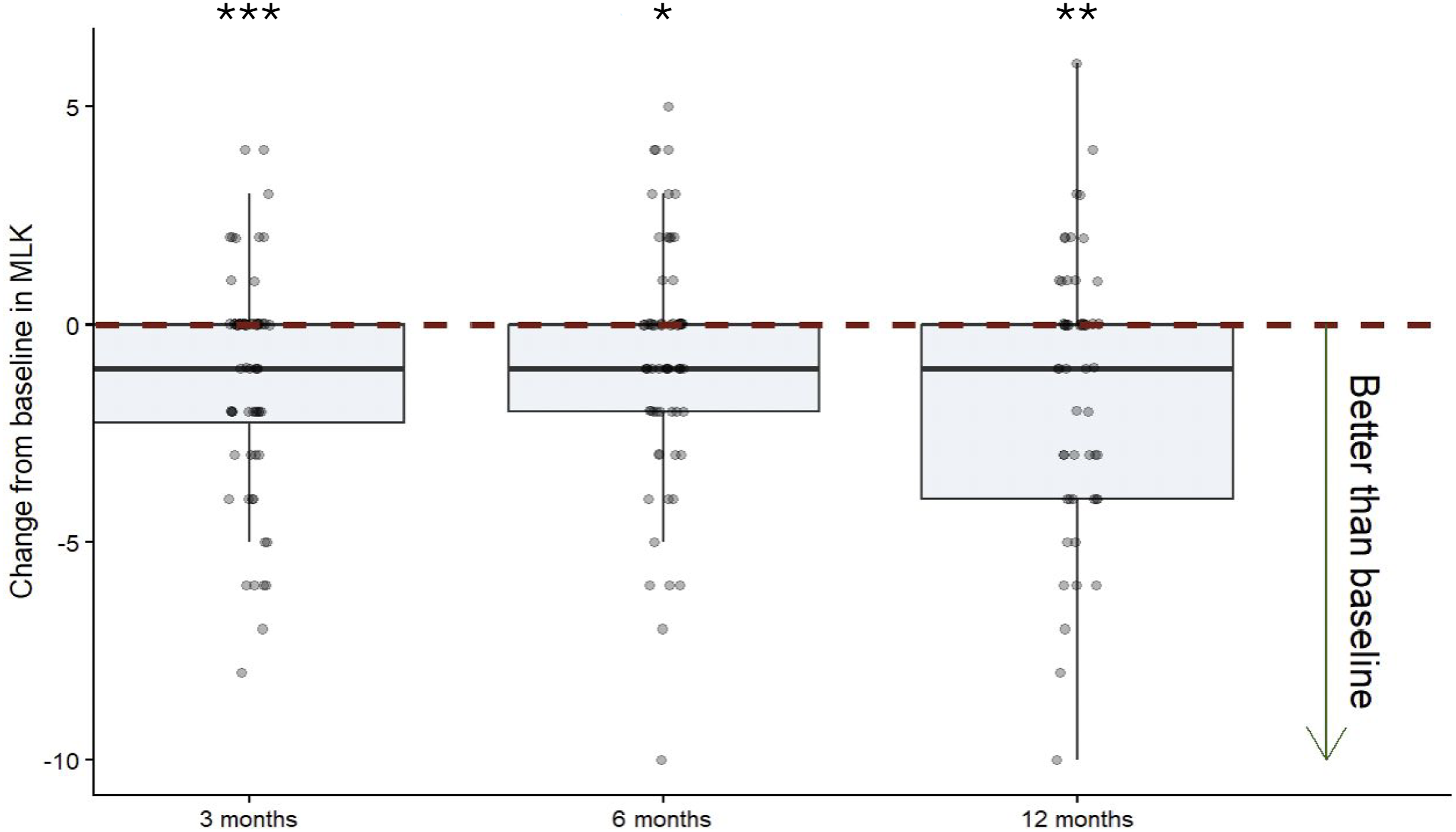
Discussion
This study characterized our in-office cohort of patients and evaluated the safety and efficacy of in-office endoscopic sinonasal procedures for CRS. The majority of procedures performed were revisions (83.0%), which highlights the use of in-office procedures for the management of recurrent disease following a previously performed in-office procedure or ESS under general anesthesia. Typically, primary CRS cases undergo comprehensive ESS under general anesthesia. However, in office-procedures serve numerous roles, including definitive treatment for selected limited disease, adjunctive treatment, and as bridging interventions for symptomatic relief while patients await ESS under general anesthesia.
Our study displays a low intraoperative complication rate of 1.2% for the CRS cohort. This is in accordance with the literature, with studies reporting intraoperative complication rates of in-office ESS for CRS ranging from zero up to 15.9%.5,12-14,18,19 Additionally, our intraoperative complication rate is lower than that reported in a prospective CRS cohort examining perioperative complications associated with ESS under general anesthesia, which was 5.8% of cases among 706 patients. 20 We did, however, observe an intraoperative event of an inadvertent neuropattie ingestion. This did not result in any long-term sequalae, however it highlights an avoidable risk associated with topical anesthetic application during in-office procedures. To address this, we have adopted the use of neuropatties with an attached thread, with the external end visible outside of the nasal cavity to allow for retrieval if displaced into the nasopharynx. Such a modification will further enhance procedural safety and is recommended by our team. Scott et al. reported eight intraoperative complications among 315 patients who underwent an in-office rhinologic procedure, all of which required procedure termination. In our study, no procedures required termination. In contrast, Viera-Artiles et al. recorded one major intraoperative complication amongst a 77-year-old male, who experienced decreased consciousness and severe bradycardia, which necessitated admission to the intensive care unit and advanced cardiac life support. Although we did not collect hemodynamic data, in-office endoscopic sinonasal procedures can result in slight alterations in systolic blood pressure and heart rate, which are more pronounced with older age.13,14
In-office endoscopic sinonasal procedures boast a low postoperative complication rate, with epistaxis being the most common.5,13,18 Our postoperative bleeding complication rate of 2.5% was comparable to a study analyzing postoperative bleeding in patients undergoing ESS for CRS under general anesthesia, which demonstrated a bleeding rate of 6.0% (36/605 patients). 21 Out of the four episodes of epistaxis reported in our study, two patients visited the ED, with one undergoing cauterization of nasal blood vessels. For the patient requiring an ED visit only, ASA was not discontinued before the procedure, indicating that proper hemodynamic control is essential pre- and postoperatively. Scott et al. reported one instance of an infection, which we did not encounter in our study. However, immunosuppression and infection risk are important selection considerations when choosing candidates for in-office procedures.
After excluding nine patients who underwent an in-office sinonasal procedure as a bridging intervention with already scheduled ESS under general anesthesia, the one year revision rate was 14.0% (n = 20), slightly higher than Scott et al’s rate of 7.6% (n = 9). Out of the 20 cases, 7 (35.0%) were revised under general anesthesia, while 13 (65.0%) were revised under local anesthesia. Among patients who underwent revision surgery under general anesthesia, refractory symptoms such as chronic mucus production, continuous purulent drainage, facial pressure, and recalcitrant sinusitis were common. These findings suggest that patients with a history of pronounced symptoms or more severe CRS disease may be more appropriate candidates for ESS under general anesthesia compared to an in-office intervention.
Overall, our revision rate pattern reflects the numerous clinical roles of in-office procedures at our center. In-office sinonasal procedures serve as definitive treatment for patients with less severe CRS as an alternative to ESS under general anesthesia and are also utilized for targeted management of recurrent disease following prior ESS under general anesthesia. Additionally, in-office procedures may be used as bridging procedures to provide symptomatic relief while patients await comprehensive surgery under general anesthesia. Importantly, the revision procedures performed in-office mainly consisted of polypectomies and scar band excisions, which result in minimal discomfort to patients. This method avoids having to schedule patients for a minor procedure in an operating room, minimizing the risk associated with general anesthesia and reducing overall wait times.
In-office endoscopic sinonasal procedures provide system-level advantages that are increasingly relevant in Canada’s publicly funded healthcare environment. By shifting suitable cases away from the operating room, they help alleviate the surgical wait times experienced in Canada and free operating room capacity for patients requiring endoscopic sinus surgery under general anesthesia. Additionally, in-office endoscopic sinonasal procedures are associated with lower per-case costs compared to endoscopic sinus surgery under general anesthesia, while maintaining a high safety profile. 11
No definitive minimal clinically important difference (MCID) exists for MLK scores. However, work by Wangworawut and Hwang demonstrated that patients with baseline MLK scores ≥3 have a higher chance of symptom improvement, with a 14.62% increase in the improvement rate observed between scores of two and three (72.34% vs. 86.96%). 22 Our CRS cohorts’ median baseline MLK score was 4/12, sufficiently above the prognostic threshold, suggesting sufficient disease burden for clinically meaningful improvement. While modest, the median one-point reduction in MLK scores at three and six months, and two-point reduction at twelve months postoperatively indicates treatment efficacy and a potential clinically meaningful difference. Viera-Artiles et al. reported a 4.66 point-reduction in MLK scores among patients with more severe baseline disease, likely explaining the smaller change observed with our less severe patients. Gan et al. also reported a significant reduction in nasal polyp grades following in-office microdebrider-assisted ESS. Collectively, these findings further support the effectiveness of in-office sinonasal procedures as an alternative to ESS performed under general anesthesia. 23
Limitations include missing data and resulting smaller sample sizes. The lack of a comparison group also limits the direct contrast of in-office sinonasal procedures versus ESS under general anesthesia, though such comparisons are inherently difficult due to differing disease severity and candidacy criteria. Additionally, although our performed procedures were heterogeneous, it reflects contemporary tertiary center rhinology practice where in-office procedures serve as adjunctive or definitive treatment, or as bridging interventions while patients await more comprehensive surgery under general anesthesia. Future studies should consider collecting formal patient-reported measurments assessing comfort. Although not collected in our study, patient comfort and tolerability were continuously assessed during procedures, and if necessary, interventions were temporarily paused or modified if discomfort occurred. Despite this, our findings offer valuable insight into the safety and efficacy of in-office sinonasal procedures and support its use in appropriate patients. This is the largest Canadian study to date evaluating postoperative outcomes following in-office sinonasal procedures for CRS, contributing to an area with limited domestic evidence. Future studies should consider prospective methods to ensure more robust and complete data collection.
Conclusion
Overall, our findings support the use of in-office endoscopic sinonasal procedures as a safe and effective option for properly selected patients diagnosed with CRS. Such procedures offer a valuable alternative to traditional operating room-based ESS for patients with milder disease, and as a bridging intervention for symptomatic relief while awaiting surgery under general anesthesia.
Footnotes
Acknowledgements
The authors have no acknowledgements to declare.
Ethical Considerations
This study protocol was approved by the Research Ethics Board of the University of British Columbia (UBC) and Providence Health Care (REB Number: H24-00042). Consent was waived by our institutional ethics board due to the retrospective nature of the study.
Author Contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the Summer Student Research Program award from the University of British Columbia.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.