
Abstract
Respiratory epithelial adenomatoid hamartoma (REAH) represents a category of tumor-like lesion arising from congenital developmental anomalies, characterized by aberrant differentiation or maturational arrest of multiple tissue lineages during embryogenesis. The predominant anatomical site involves the nasal cavity, specifically the nasal septum, with additional potential locations including the middle meatus and ethmoidal sinuses. Definitive diagnosis generally requires histopathological examination. These uncommon nasal neoplasms are amenable to complete excision through endoscopic surgical approaches performed under general anesthesia. A 55-year-old patient with nasal vestibular REAH presented with nasal obstruction, intermittent nasal pruritus, and diminished olfactory function. Clinical examination detected an ovoid mass in the right nasal vestibule, while radiological imaging demonstrated soft tissue density in the corresponding area. The diagnosis of REAH was confirmed through histopathological assessment after complete surgical excision. The patient fortunately experienced no procedure-related complications throughout the perioperative course and follow-up period. Postoperative surveillance through scheduled follow-up examinations is essential to prevent local recurrence.
Introduction
The most common anatomical location of respiratory epithelial adenomatoid hamartoma (REAH) is the nasal cavity, with the nasal septum being particularly prevalent, followed by structures such as the middle meatus and ethmoid sinus, 1 whereas the nasal vestibule is a less common location for this lesion. Owing to an absence of pathognomonic diagnostic features, this entity is frequently subject to misdiagnosis in clinical practice. 2 The majority of REAH cases exhibit benign biological behavior, characterized by indolent progression and self-limited proliferation. Following growth arrest, the lesion remains and may lead to compressive and obstructive symptoms, rendering surgical excision the primary therapeutic option. 3
Case Report
A 55-year-old female was admitted due to right-sided nasal congestion, intermittent nasal itching accompanied by hyposmia for over 1 month without an apparent cause. One month prior to admission, the patient developed right nasal congestion, intermittent nasal itching, and hyposmia without obvious cause. She received symptomatic supportive treatment but experienced no significant improvement in the aforementioned symptoms. A non-enhanced sinus computed tomography (CT) scan performed locally indicated a “nasal cavity mass.” Subsequently, the patient’s symptoms progressively worsened. Specialized examination revealed: no external nasal deformity, deviated nasal septum, fair nasal patency, and a roundish mass palpable in the right nasal vestibule. Paranasal sinus CT indicated (Figure1): (1) soft tissue shadow in the right nasal vestibule, suggestive of polyp and (2) mild inflammation of the right maxillary sinus. The patient underwent resection of the nasal vestibular mass via a transoral vestibular approach under general anesthesia. A horizontal mucosal incision was made ~0.5 cm above the right labiogingival groove. The mucosa and submucosal tissue were incised, followed by blunt and sharp dissection along the periosteal surface superiority to elevate a mucoperiosteal flap, adequately exposing the inferior margin of the pyriform aperture and the nasal floor. Under nasal endoscopy, the tumor was visualized at the nasal floor, measuring ~1 × 1 cm, with firm consistency and a complete capsule. The tumor was completely enucleated and extracted through the labiogingival incision, then sent for pathological examination. Intraoperative and postoperative histopathological examination revealed: gross description: (right nasal vestibular mass) an irregular fragment of grayish-white and grayish-brown tissue measuring 1.3 × 1 × 0.4 cm, with a gray-white and gray-brown solid-cystic cut surface and a slightly rough cystic lining. Diagnosis (Figure 2): (right nasal vestibule) REAH.
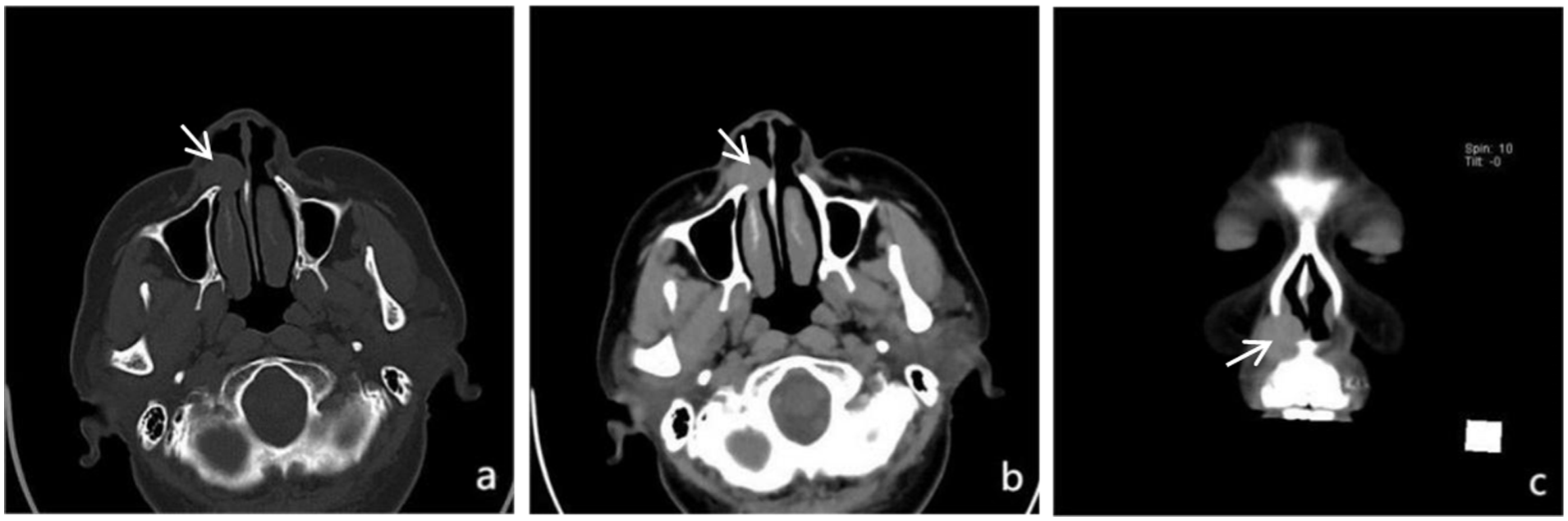
Axial (a, b) and coronal (c) CT images of the paranasal sinuses demonstrate a soft tissue shadow in the right nasal vestibule (indicated by the arrow).
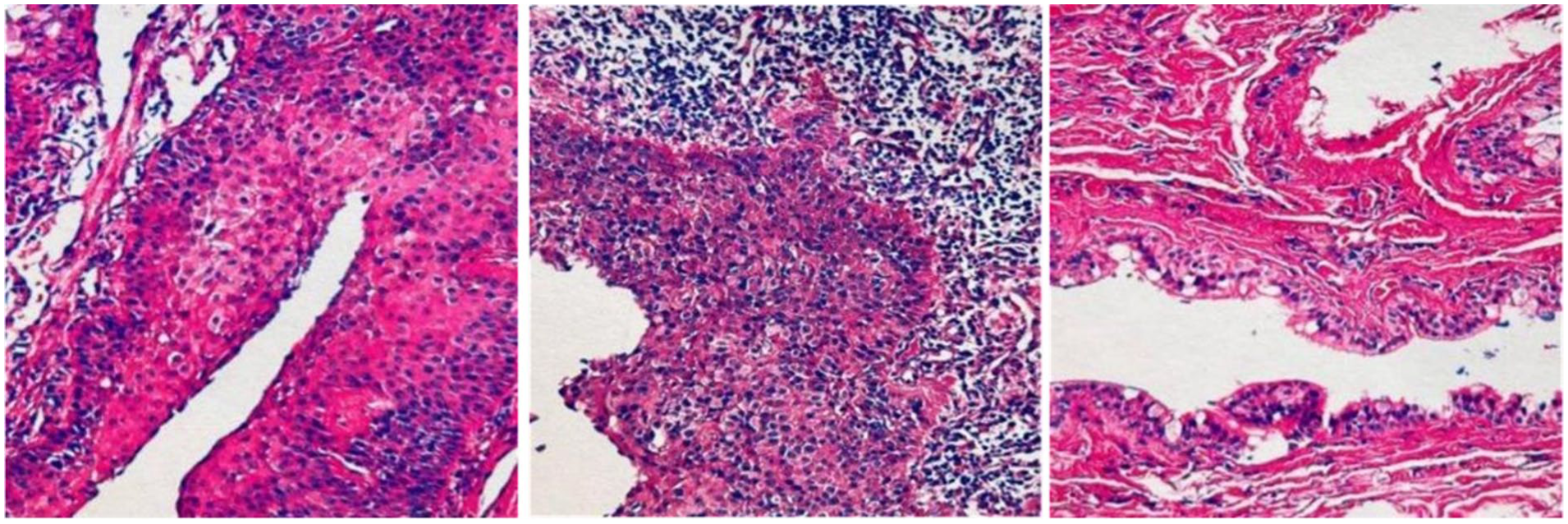
Histopathological examination of the surgical specimen.
Discussion
REAH was initially introduced by Wenig and Heffner, 4 this entity represents tumor-like lesions arising from congenital developmental anomalies, characterized by aberrant differentiation or maturational arrest of multiple tissue lineages during embryogenesis. 1 Previous studies have shown that REAH is predominantly located within the nasal cavity, favoring the nasal septum and olfactory cleft. It may also affect areas such as the middle nasal meatus and ethmoid sinus, whereas its incidence in the nasal vestibule is exceptionally uncommon.5,6 Schertzer et al 7 further demonstrated in their research that REAH is prone to occur in the central nasal compartment characterized by significant allergen exposure; in contrast, the REAH case described in the present study arose from the nasal vestibule, a location that deviates from the predilection sites cited in prior publications. Common clinical presentations comprise nasal obstruction accompanied by diminished olfaction, epistaxis, and nasal discharge. 3 Investigations by Zhang et al 8 demonstrated that REAH commonly presents concurrently with other sinonasal disorders, including chronic rhinosinusitis, inverted papilloma, and vascular tumors. The absence of pathognomonic clinical manifestations, physical findings, and radiological characteristics contributes to its low diagnostic yield, with definitive preoperative diagnosis remaining elusive in virtually all cases. 2 Histopathological evaluation constitutes the diagnostic gold standard.
The most indicative radiological feature of REAH on computed tomography of the paranasal sinuses is olfactory cleft widening. When the olfactory cleft width exceeds 10 mm and simultaneously meets the following 3 criteria: (1) presence of bilateral olfactory cleft masses; (2) mass size ratio between the 2 sides <2; (3) absence of bone destruction around the masses, REAH should be highly suspected. 8 Magnetic resonance imaging findings of REAH are non-specific, typically showing iso- to mild hypointensity on T1-weighted sequences, heterogeneous hyperintensity on T2-weighted sequences, and exhibiting either homogeneous or heterogeneous contrast enhancement. 9
The characteristic pathological feature of REAH is glandular proliferation composed of ciliated respiratory epithelium, with glands typically appearing round or oval and separated by stromal tissue. Notably absent are marked nuclear atypia, while focal glandular structures demonstrate thickened eosinophilic basement membranes. 10 Immunohistochemical analysis reveals CK7 and p63 (basal cell layer) positivity, with negative staining for CK20, CDX-2, and S-100. 11 Investigations conducted by Ozolek and Hunt 12 demonstrated overlapping immunohistochemical characteristics among REAH, inverted papilloma, and chronic rhinosinusitis. REAH often presents concomitantly with nasal polyps (NP). Comparative studies indicate significantly reduced expression levels of IL-4, IL-5, IL-33, and Occludin in REAH versus NP, alongside elevated TNF-α expression, 13 offering discriminative biomarkers for pathological differentiation.
Endoscopic surgical excision with complete removal of pathological tissue represents the primary treatment approach for this disease. 14 The principal surgical consideration for nasal vestibular REAH, being a benign lesion, involves maintaining limited resection margins to avoid compromising nasal mucosal integrity and olfactory neuroepithelium, thus safeguarding physiological nasal function. 15 Compared to NP, REAH tends to bleed more readily during surgery; therefore, comprehensive preoperative preparation is essential to prevent significant intraoperative hemorrhage. The surgical approach should involve subcutaneous resection of the neoplastic tissue with maximal preservation of the overlying cutaneous layer to enable optimal reconstruction of the defect. In cases complicated by postoperative nasal stenosis or structural deformity, simultaneous rhinoplasty is indicated.
Conclusion
REAH represents a benign nasal entity distinguished by pathognomonic histological features, requiring both radiological characteristics and histopathological examination for definitive diagnosis. This case represents a rare instance of nasal vestibule-originated REAH, which is distinctly different from the classic predilection sites such as the nasal septum and olfactory cleft reported in previous literature. Meticulous preoperative assessment and standardized endoscopic surgical techniques are pivotal to achieving successful therapeutic outcomes while maintaining nasal physiological function. Further investigation into the pathogenetic mechanisms and molecular signatures of REAH will substantially improve diagnostic precision and enable more targeted therapeutic interventions.
Footnotes
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent for Publication
Written informed consent was obtained from participant prior to the study, for the purpose of publication in accordance with ethical guidelines.
Author Contributions
This paper is a case study achievement, completed through the division of labor and close collaboration among all authors. The specific contributions of each author are as follows (in the order of authorship): YaNan Li: responsible for the overall design and demonstration of the case study plan, and led the selection, contact, and access of case subjects; undertaken the collection and standardized collation of core case data, and completed the coding and preprocessing of case data; composed the core chapters of the paper, constructed the overall framework of the paper, and sorted out the logical context; integrated revision suggestions from all authors to complete the first draft and final draft of the paper; participated in the response to review comments and content revision after submission. Xin Pan: focused on the extraction of key issues and the construction of analytical frameworks in the case study; assisted in the collection and verification of supplementary case data, and participated in the in-depth interpretation of case data; responsible for the composition of the Results and Discussion and theoretical refinement sections of the paper, providing academic support for case analysis; reviewed the rigor of the case analysis logic and the reliability of conclusions, and put forward targeted revision suggestions. XuDong Wei: served as the general person in charge of the research project, responsible for the direction control and resource coordination of the case study; proposed core research questions and case selection ideas, and guided the optimization and improvement of the research plan; reviewed the overall academic quality, the innovation and theoretical value of case analysis of the paper, and was responsible for the authenticity of the research conclusions; led the entire process of communication including paper submission, response to review comments, and final publication. All authors have read and approved the final published version of the paper, confirmed the authenticity of case study data, the objectivity of analysis, and the rationality of authorship, and agreed to jointly assume responsibility for the academic content of the paper.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was financially supported by the Major Scientific Research Projects for Technological Innovation in the Health Industry of Gansu Province (GSWSZD2024-02).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data are available and shared.