
Abstract
Respiratory epithelial adenomatoid hamartoma (REAH) is a rare benign lesion of the upper airway. It exceptionally affects the nasal cavity pathway. Its resemblance to other nasal masses poses diagnostic challenges. We report a case of REAH in a 59-year-old man presenting with left nasal obstruction and nocturnal snoring evolving over 2 years. Nasal endoscopy revealed a rhinopharyngeal mass, which was confirmed as REAH by histopathological examination of the biopsy performed under endoscopic guidance, resulting in complete lesion removal. Two years of follow-up showed no recurrence. This case is reported due to its rarity and the risk of misdiagnosis.
Introduction
Head and neck hamartomas are exceptionally rare, often posing a diagnostic challenge due to their resemblance to other pathological entities. Among these, respiratory epithelial adenomatoid hamartoma (REAH) is an uncommon benign epithelial proliferation predominantly affecting the nasal cavity and paranasal sinuses. First described in 1995, REAH has since been recognized as a distinct histopathological entity, although its pathogenesis remains unclear.1,2
While REAH is typically found in the nasal passages, reports of nasopharyngeal involvement are exceedingly rare. Given its clinical and radiological similarity to more aggressive lesions, such as inverted papilloma, low-grade adenocarcinoma, and even nasopharyngeal carcinoma, misdiagnosis is a significant concern. As a result, histopathological examination remains the gold standard for establishing a definitive diagnosis.1-3
Here, we report a case of nasopharyngeal REAH in a 59-year-old patient, initially suspected to have a malignant neoplasm. This case highlights the importance of considering REAH in the differential diagnosis of nasopharyngeal masses and underscores the need for histological confirmation to prevent unnecessary aggressive interventions.
Case Presentation
A 59-year-old man with a history of type 2 diabetes and a 25 pack-year smoking history presented with left-sided unilateral nasal obstruction and nocturnal snoring, without epistaxis, evolving over two years. He had no otologic symptoms or visual disturbances.
Rhinological examination revealed a congestive appearance of the nasal mucosa, hypertrophy of the inferior turbinates, and nasal endoscopy showed an asymmetric bulging of the posterior wall of the nasopharynx on the left side due to a single, centimeter-sized, nodular lesion with a smooth, shiny surface, which did not bleed upon contact. The rest of the nasopharynx was free of lesions. Cervical examination showed no cervical lymphadenopathy. Otologic examination revealed bilateral retracted tympanic membranes without effusion. Cranial nerve examination was unremarkable.
The clinical and anamnestic findings suggested a benign-appearing nasopharyngeal tumor, prompting an endoscopically-guided biopsy under local anesthesia on the day of consultation, which allowed complete removal of the lesion. The post-biopsy course was uneventful.
The final histopathological diagnosis of the tumor biopsy confirmed a respiratory epithelial adenomatoid hamartoma (REAH) of the nasopharynx. Macroscopically, the two brownish tissue fragments measured 10 and 6 mm, respectively. Histologically, the sections showed ciliated respiratory epithelium resting on a sometimes thickened, eosinophilic basement membrane. The underlying stroma contained numerous regular, sometimes dilated, seromucous glands without atypia. There was vascular congestion with hemorrhagic suffusion (Figures 1 and 2).
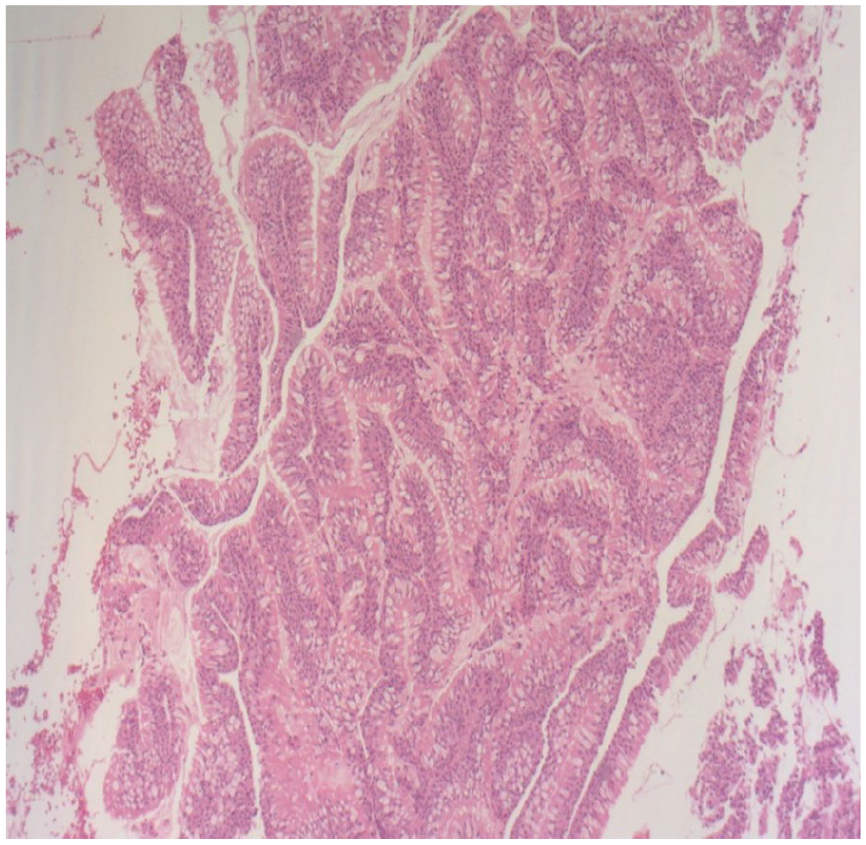
The histological images, stained with hematoxylin and eosin, depict a tissue sample with a well-organized glandular proliferation, a characteristic of a respiratory hamartoma.
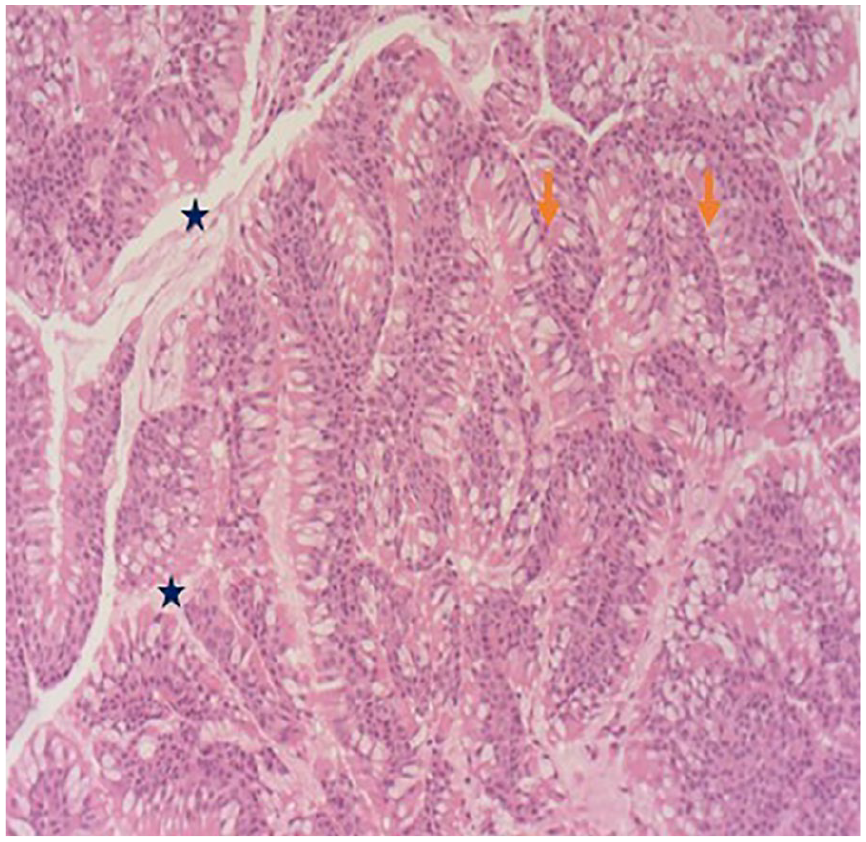
Higher magnification of the histopathological section of the nasopharyngeal lesion stained with hematoxylin and eosin (H&E), demonstrating the glandular proliferation characteristic of REAH. The glands are lined by ciliated respiratory epithelium (orange arrow ) with pseudostratified nuclei, and the luminal spaces are filled with mucinous secretions. The stroma surrounding the glands appears loose and edematous, consistent with benign features (blue star). There is no evidence of cellular atypia, mitotic figures, or invasive growth.
The patient was treated with intranasal corticosteroids and nasal irrigation. His clinical course under medical treatment was favorable, with resolution of initial symptoms, and no endoscopic recurrence observed over a two-year follow-up period.
Discussion
Respiratory epithelial adenomatoid hamartoma (REAH) is a benign glandular proliferation with an unclear pathogenesis. It can present either as an isolated lesion or in association with inflammatory conditions such as nasal polyposis.1,2 A male predominance has been reported.1,3,4
The most affected age group ranges from the third to ninth decade, with a peak incidence in the fifth decade.1,2,4,5
To the best of our knowledge, only five cases of nasopharyngeal REAH have been reported in the literature,6-10 and our case would represent the sixth case. Table 1 provides a summary of these individual cases.
Summary Table Including Cases of Nasopharyngeal REAH Reported in the Literature.
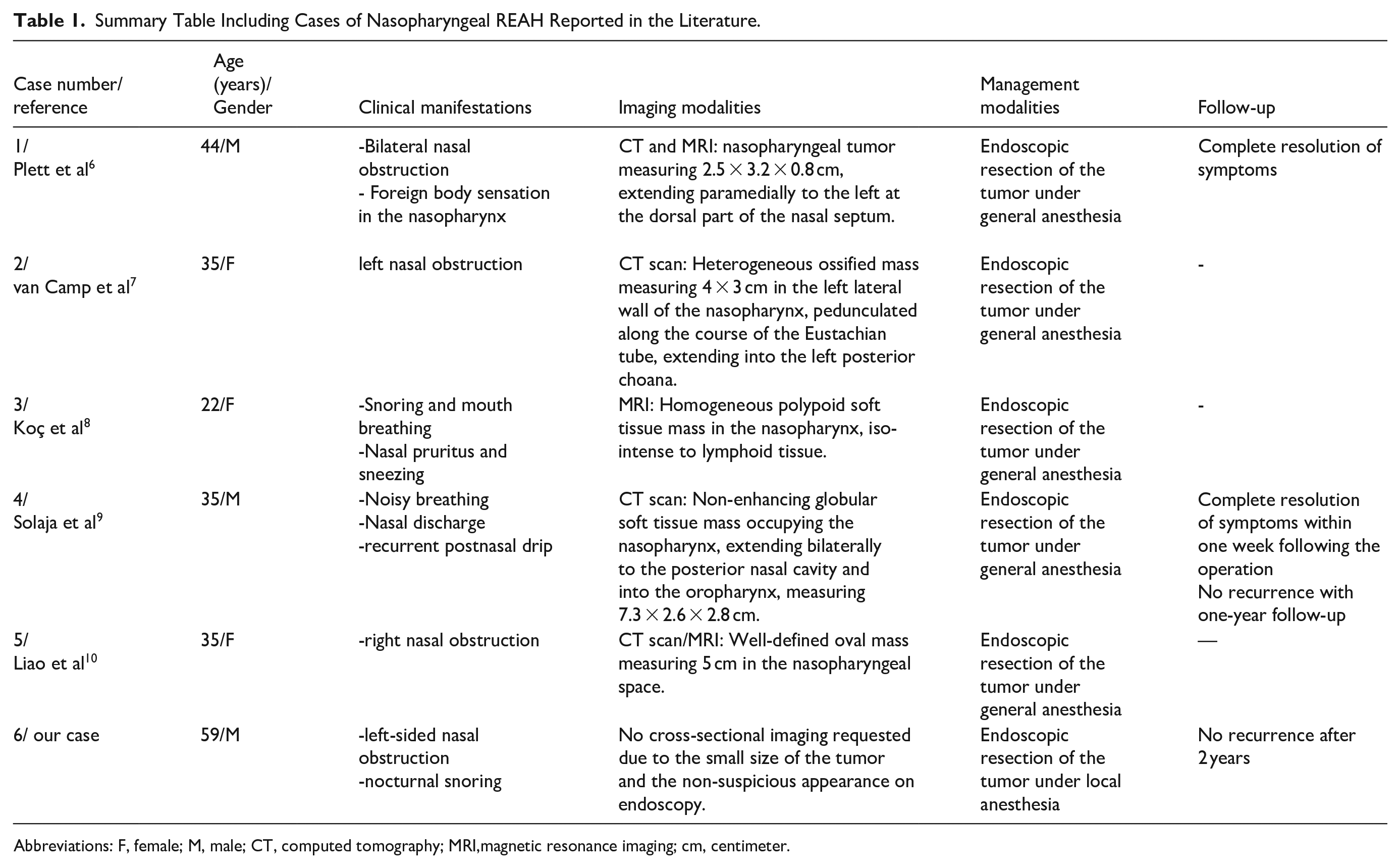
Abbreviations: F, female; M, male; CT, computed tomography; MRI,magnetic resonance imaging; cm, centimeter.
Patients typically present with nonspecific symptoms such as unilateral nasal obstruction, epistaxis, or rhinorrhea. 11 Some authors have linked this pathology to smoking and asthma. 12 The development of these lesions later in life makes a congenital etiology less likely. Our patient presented at the age of 59 with a 2 year history of symptoms, supporting the hypothesis of a non-congenital origin for REAH. 13
Clinically, REAH is most commonly observed on the lateral nasal wall, 5 though other sites, such as the nasopharynx and paranasal sinuses, have also been reported.14,15
Histopathological examination is the gold standard for an accurate diagnosis of REAH. 16 Macroscopically, the lesions tend to be polypoid, with a friable to firm consistency and a yellowish to white coloration. They may also appear edematous or shiny. 17 Microscopically, the lesion consists of a subepithelial glandular proliferation with round to ovoid glands lined by ciliated respiratory epithelium originating from the superficial mucosa. Mucoid metaplasia, with mucoid or amorphous material filling the glandular lumina, has occasionally been observed. 18 The basement membrane is thickened and eosinophilic, with an edematous stroma. 4
Many cases of REAH are identified through biopsy. 3 Despite the characteristic histological features of this entity, distinguishing it from differential diagnoses can be challenging, particularly in cases of small fragmented endoscopic biopsies. 18 Recognizing this diagnosis is crucial, as its definitive treatment is simple excision, unlike other possible diagnoses. Complete excision is curative, offering an excellent prognosis.5,14,19
To date, there is no evidence of recurrence or aggressive behavior in REAH. 15
Conclusion
Respiratory epithelial adenomatoid hamartoma is a rare but benign entity that, despite its indolent nature, poses a considerable diagnostic challenge due to its clinical and radiological similarities with more concerning pathologies. Our case of nasopharyngeal REAH, initially misinterpreted as a possible carcinoma, emphasizes the importance of awareness among clinicians and pathologists to avoid unnecessary invasive treatments.
Histopathological examination remains essential for confirming the diagnosis, as complete surgical excision provides definitive management with an excellent prognosis. To date, there is no evidence of malignant transformation or recurrence after excision. Increased recognition and reporting of REAH, particularly in unusual locations such as the nasopharynx, will aid in refining diagnostic criteria and improving patient management.
Footnotes
Acknowledgements
None.
Authors’ Note
All the authors have read and agreed to the final manuscript.
Ethical Considerations
Our institution Faculty of Medicine of Sousse’s Ethics Committee does not require ethics approval for reporting individual cases or case series since we anonymously reported clinical and imaging information concerning our patient’s case.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Statement of Informed Consent
A written informed consent was obtained from the patient for his anonymized information to be published in this article.
Data Availability
Data will be made available on request