
Abstract
Parapharyngeal space (PPS) tumors are relatively rare, accounting for 0.5% to 1% of all head and neck tumors. Among these, pleomorphic adenoma is the most common benign subtype, representing 34% of all PPS tumors. The core therapeutic principle for this lesion is complete tumor resection to reduce the risk of recurrence. Traditional surgical approaches include transcervical and transoral routes. This study presents a case of pleomorphic adenoma located in the parapharyngeal space with extension to the deep lobe of the parotid gland, which was successfully resected by endoscopic-assisted transoral plasma surgery without robotic assistance. This case provides a valuable clinical reference for the minimally invasive management of similar lesions.
Keywords
Case Presentation
A 67-year-old female patient initially presented to Xiaoshan First People’s Hospital and was subsequently transferred to the Second Affiliated Hospital of Zhejiang University in February 2025, before being referred to Hangzhou First People’s Hospital for further treatment. She had a 5-year history of pharyngeal foreign body sensation and was found to have a nasopharyngeal neoplastic protrusion 2 weeks prior to the current visit. No other accompanying symptoms (such as dysphagia, dyspnea, snoring, or nasal obstruction) were reported during clinical inquiry.
The patient had a medical history of hypertension, hyperlipidemia, anxiety disorder, and hypothyroidism, for which she was receiving regular pharmacologic treatment. She had also previously undergone iodine-131 therapy. There was no family history of related diseases.
Physical examination revealed significant bulging of the posterior end of the soft palate and deviation of the uvula to the right, with no obvious tonsillar enlargement (Figure 1A). No masses were palpable in the neck or at the mandibular angle, and no facial paralysis was observed. The patient’s serum tumor markers were within the normal reference range.
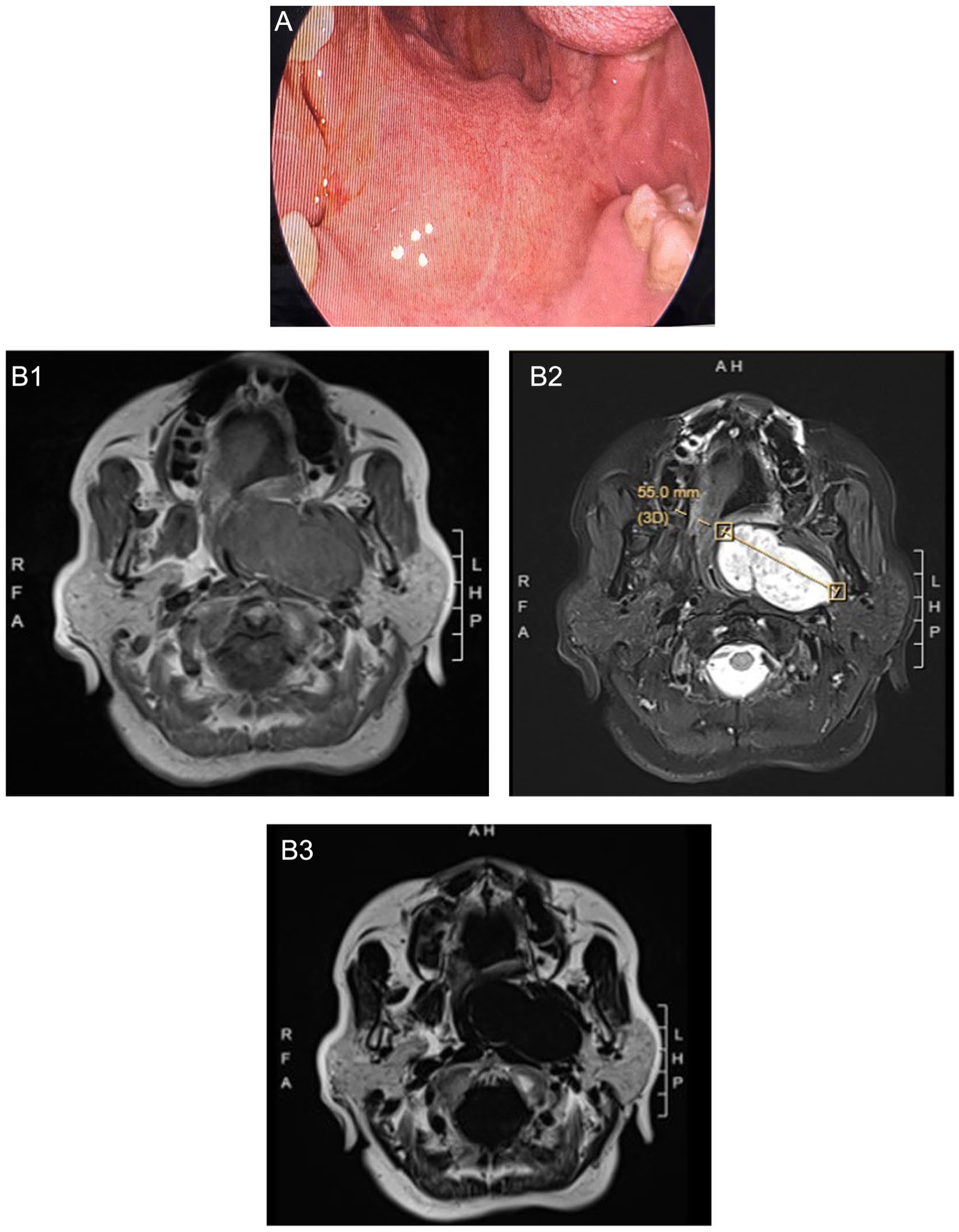
(A) Preoperative oral photo. (B1-B3) Preoperative MRI images. MRI, magnetic resonance imaging.
Nasal endoscopy showed a round neoplasm on the left side of the nasopharynx with a relatively smooth surface. Nasopharyngeal magnetic resonance imaging (MRI) revealed an elliptical abnormal signal in the left parapharyngeal space, which exhibited isointense signal on T1-weighted imaging (T1WI) and mixed hyperintense signal on T2-weighted imaging (T2WI), with clear margins and measuring approximately 57 × 29 × 43 mm. After contrast administration, the lesion showed obvious enhancement with internal septations. The nasopharyngeal cavity was narrowed, and the left pharyngeal recess was significantly compressed and narrowed. The right torus tubarius, pharyngeal recess, and parapharyngeal space appeared normal, with no abnormal signals or postcontrast enhancement. No pathologically enlarged lymph nodes were detected in the bilateral necks within the scanning field. A neurogenic tumor was initially considered the most likely diagnosis (Figure 1B).
Neck computed tomography angiography (CTA) demonstrated that the left nasopharyngeal mass was supplied by the left external carotid artery (Figure 2). No arterial stenosis, aneurysm, or vascular malformation was found in the neck, and the carotid sheath remained intact without tumor involvement. Preoperative identification of the tumor’s vascular supply provided crucial guidance for intraoperative hemostasis.
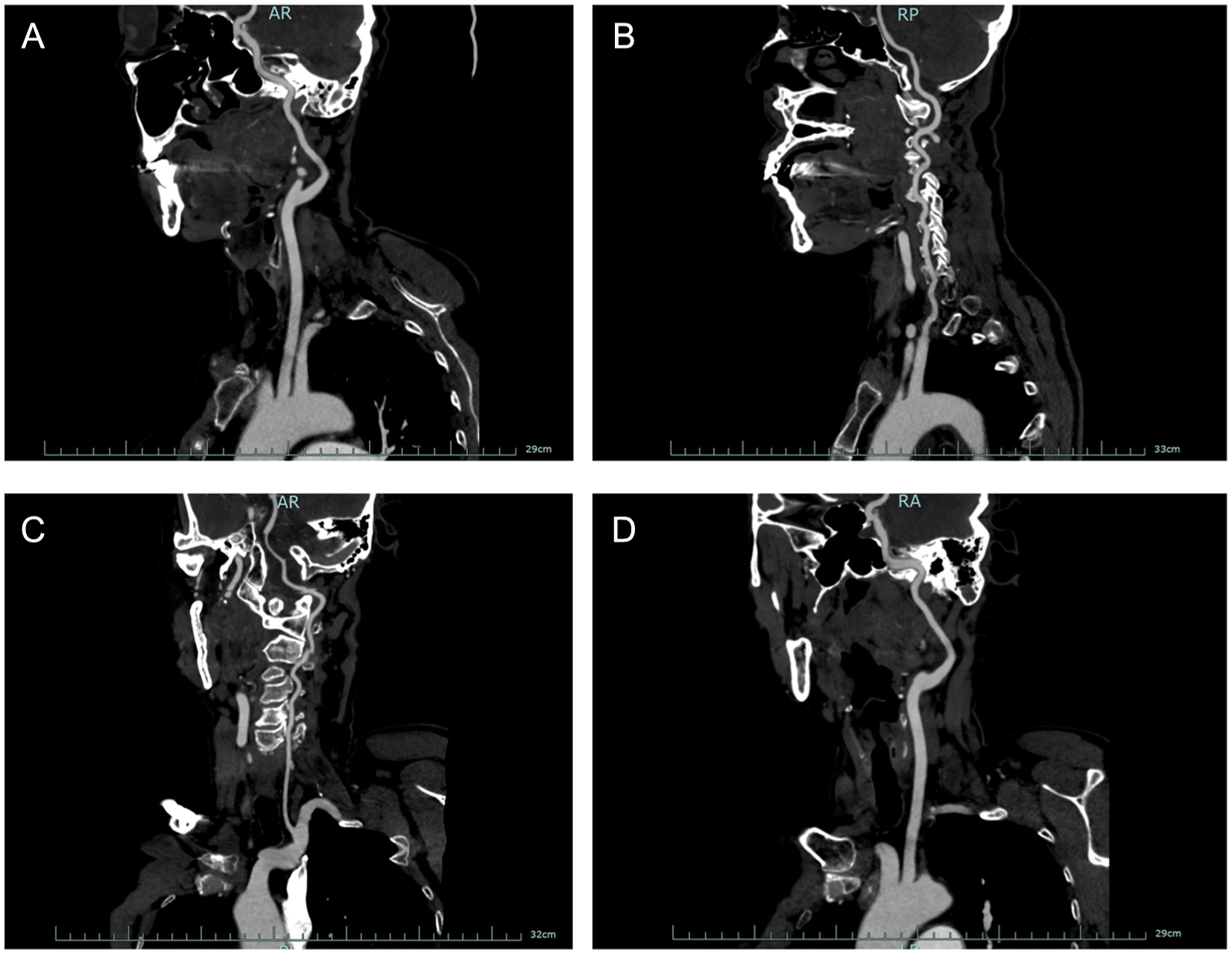
(A-D) Preoperative CTA: The left mass is supplied by the left external carotid artery. CTA, computed tomography angiography.
Based on the patient’s clinical manifestations, medical history, and imaging findings, a preliminary diagnosis of a parapharyngeal space mass (with potential involvement of the deep parotid lobe) was made. Differential diagnosis was required to rule out primary deep parotid gland tumors, which can be distinguished by the preservation of the fat plane between the tumor and the parotid gland on T1-weighted sequences.
Surgical Method
Surgical approaches for parapharyngeal space masses include single or combined transoral, transcervical, transparotid, and transmandibular techniques. In recent years, robotic-assisted transcervical surgical approaches have also been reported in the literature. 1 The patient’s mass was mainly located in the prestyloid space. Although the tumor was large and deeply located, extending inward to the nasopharynx and clivus, it was deemed suitable for a transoral approach. Therefore, the decision was made to perform endoscopic-assisted transoral resection of the parapharyngeal space and skull base lesion under general anesthesia.
Surgical Procedure
Under general anesthesia, a Davis gag was used to retract the upper and lower jaws, exposing the pharyngeal cavity. Under endoscopic guidance, an electrocautery scalpel was used to make a longitudinal incision from the upper pole of the left tonsil to the hard palate. The tumor extended superiorly to the eustachian tube, laterally to the medial pterygoid muscle, and medially in an expansive pattern to the nasopharynx and clivus, with posterior compression of the neurovascular structures in the jugular foramen area.
Given the large size of the tumor, intracapsular debulking was performed first (the tumor contents were pale yellow and lobulated), and a portion of the tissue was sent for frozen section analysis. After debulking, the tumor was completely dissected along the safe margin and capsular plane. Inferiorly, the submandibular gland capsule remained intact without invasion; superiorly, the tensor veli palatini muscle and levator veli palatini muscle were identified; posteriorly, the fascia covering the anterior surface of the internal carotid artery was noted. The lateral root of the tumor capsule was tightly adherent to the deep lobe of the parotid gland, which was incised and separated using a plasma knife, followed by complete removal of the capsule (Figure 3).
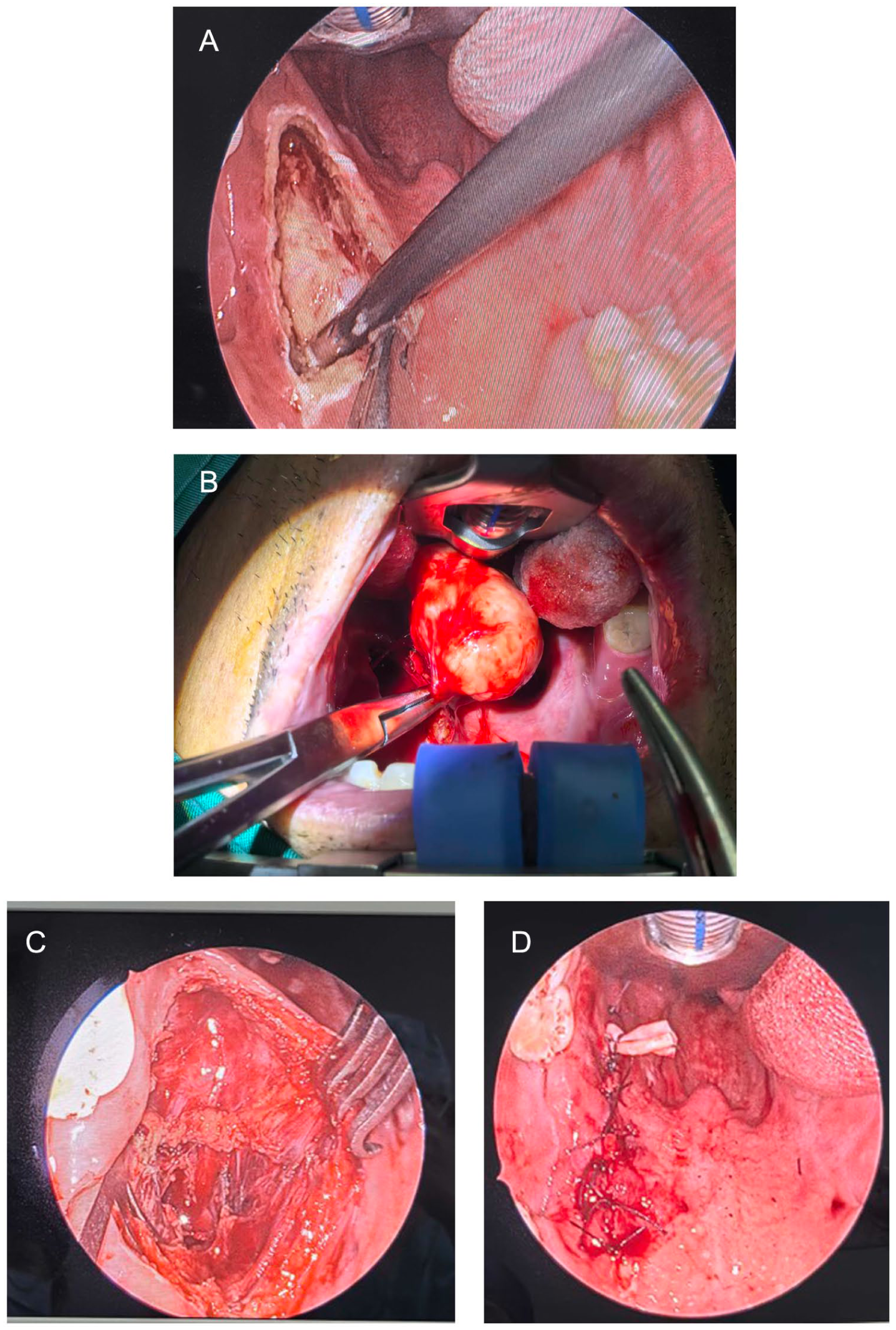
Surgical procedure: (A) Separate the mass with plasm; (B) the tumor is completely peeled off with the capsule; (C) the tumor was completely resected without any residue; (D) postoperative suturing and placement of a drainage tube.
Postoperative Results
The resected specimen measured 6 × 5 × 2 cm. Histopathological and immunohistochemical analyses confirmed a salivary gland epithelial neoplasm, consistent with pleomorphic adenoma accompanied by active myoepithelial proliferation (Figure 4).
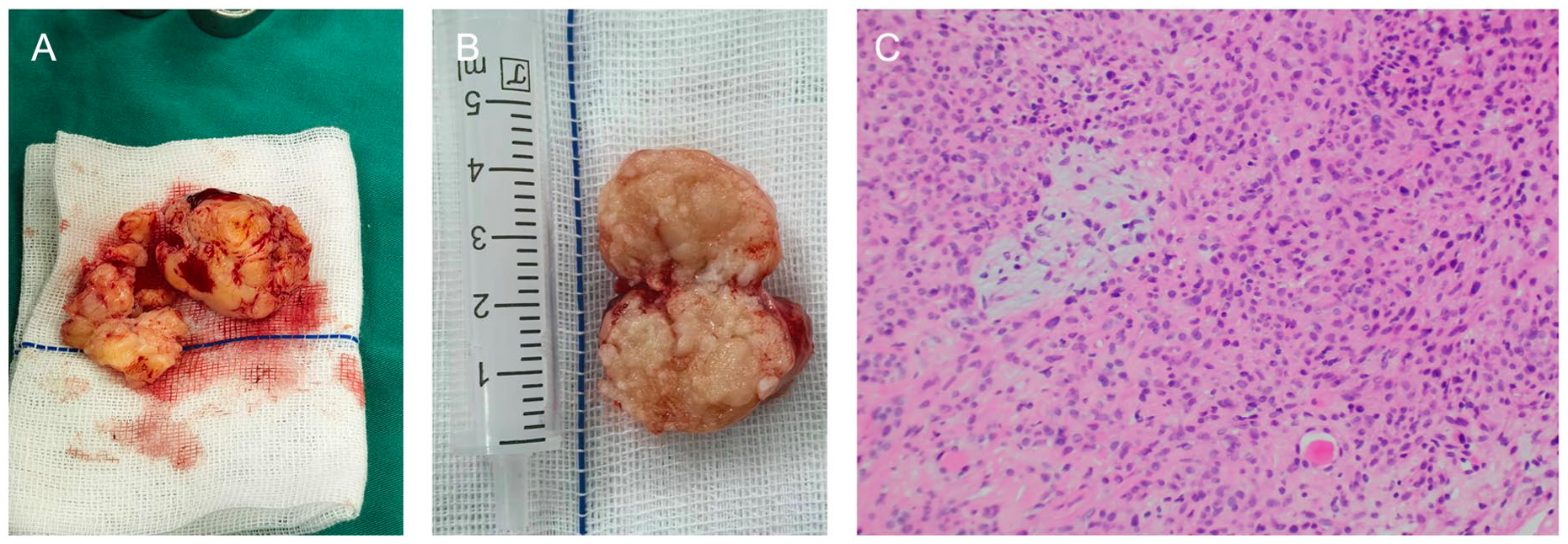
The size of the resected mass was approximately 6 × 5 × 2 cm (A) A is the portion removed during the implementation of capsular cytoreductive surgery. (B, C) Under HE (Hematoxylin-Eosin staining) staining (200× magnification): Findings of the specimen.
The patient had an uneventful postoperative course without complications such as fever, and the surgical incision achieved primary healing. No tumor recurrence was found in the left parotid gland region or nasopharynx. Facial nerve function was preserved at House-Brackmann Grade I, swallowing function remained intact, and the pharyngeal foreign body sensation resolved completely.
At the 2-month postoperative follow-up, parotid gland MRI showed that the left parotid gland had a full morphological appearance without abnormal space-occupying lesions. The parapharyngeal space structure was normal, and no radiological signs of recurrent pleomorphic adenoma in the deep parotid lobe were observed (Figure 5).
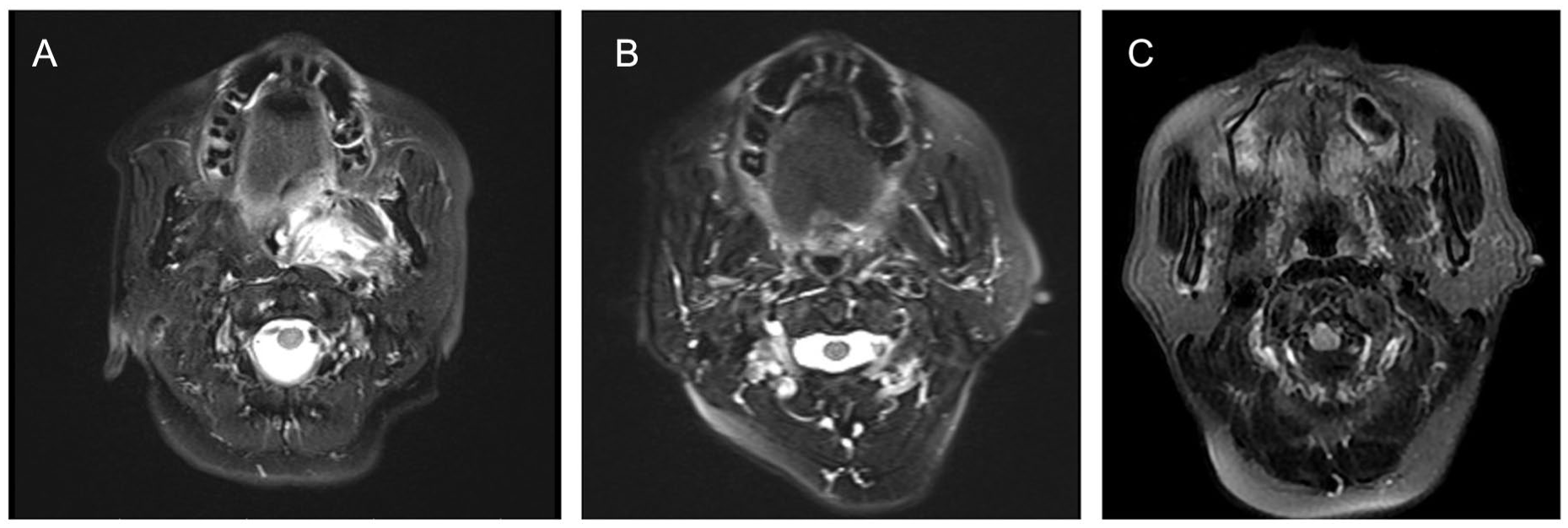
No signs of tumor recurrence were observed. (A) MRI images 1 day after the operation. (B) MRI images 2 months after the operation. (C) MRI images 6 months after the operation. MRI, magnetic resonance imaging.
Discussion
The parapharyngeal space (PPS) is a complex anatomical region of the head and neck (apex at the hyoid superior cornu, base at the skull base),bounded by cervical vertebrae/paravertebral muscles (posterior), pterygomandibular suture (anterior) oropharynx/nasopharynx (medial), and mandibular ramus/deep parotid lobe (lateral). 2 Divided by the styloid process into prestyloid and posterior compartments, the former is the most common site for PPS tumors (predominantly pleomorphic adenomas), while the latter harbors mostly neurogenic tumors, accounting for most nonsalivary PPS neoplasms.3,4 Approximately 80% of PPS tumors are benign.
Surgical approaches for PPS tumors include transcervical, transcervical-parotid, mandibular split, transcervical-mastoid, infratemporal fossa, and transoral approaches. A case series analysis of PPS pleomorphic adenomas 5 showed endoscopic transoral approach is utilized in only 1% to 2%,while open surgical approaches (48%) are more common but carry higher complications (eg, facial nerve injury and residual scarring).5,6 According to relevant studies,1,5,7 -10 the endoscopy-assisted transoral approach confers minimal invasiveness and is indicated for well-defined benign prestyloid lesions,9,11 caution is warranted for the application of this approach in retrostyloid tumors, which are predominantly neurogenic/vascular tumors with frequent carotid artery displacement.
The present patient had a large postsyloid tumor with internal septations, close to deep parotid lobe and compressing jugular foramen. Despite deep location and complexity condition (risk of rupture, neurovascular injury with transoral surgery), endoscopic-assisted transoral approach combined with low-temperature plasma technology was selected to avoid facial nerve injury and scar hyperplasia from transcervical approach. Surgical strategy: intracapsular debulking first, then low-temperature plasma dissection of tumor-parotid adhesion, achieving complete resection without unnecessary parotid sacrifice. The low-temperature plasma system uses high-frequency energy for water evaporation, protein denaturation, and vascular coagulation, offering excellent cutting/hemostatic, minimal thermal diffusion, and reduced electrical neural stimulation. 12
Intraoperative blood loss (5 mL) and hospital stay (4 days)were both less than those of open surgical approaches (7-10 days).7,9 No neurovascular injury observed intra- or postoperatively, confirming the apporach’s flexibility and safety for benign PPS tumors. Transoral robotic surgery is an alternative but limited by high costs ($1.4-2 million), long learning curve, poor cost-effectiveness, and stricter tumor restrictions (higher difficulty for large tumors, risk of delayed capsular rupture). 9 Besides, capsular rupture increases recurrence risk. 13
The patient’s pleomorphic adenoma (6 cm maximum diameter, deep location, parotid adhesion, skull base clivus/jugular foramen compression) was successfully resected via endoscopic transoral+ low-temperature plasma with “intracapsular debulking + precise adhesion dissection.” No recurrence was noted postoperatively, providing valuable clinical evidence for minimally invasive management of complex PPS tumors.
Footnotes
Acknowledgements
The case report was written by Xiaocan Zhu, Hangzhou, China. The contributions of each author are as indicated in the “Author Contributions” section.
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases or series of cases.
Consent to Participate
The patient in this case report has provided written informed consent. The patient confirms and agrees that we can conduct research, publish research, and use his photos and other case data.The signed written informed consent form was documented in the patient’s medical record.
Consent for Publication
The patient is aware and agrees that the article may be published in an open access manner. The signed written informed consent form was documented in the patient’s medical record.
Author Contributions
Concept and design: Xiaocan Zhu, Shihan Qing, Zhiqi Ma.
Acquisition, analysis, and interpretation of data: Xiaocan Zhu, Shihan Qing, Lesi Xie, Siyi Xu.
Drafting of the manuscript: Xiaocan Zhu, Zhiqi Ma.
Critical revision of the manuscript for important intellectual content: Yong Li, Jing Li.
Accountability for all aspects of the work: Huyi Lin, Kexin Liu, Yong Li, Jing Li, Zhiqi Ma, Xiaocan Zhu, Hanqing Shi.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National Key R&D Program of China (2022YFC2504100) and Science and Technology Development Project of Hangzhou (grant. 20241026Y017).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data in this article: images, imaging data, etc., can be obtained by sending an email to: