
Abstract
Keywords
Introduction
Pleomorphic adenoma (PA) is a benign salivary gland tumor, it is generally slow-growing and well-circumscribed, it is considered the most common benign salivary gland tumor and is commonly seen in the parotid gland.1-4 In the case of recurrent pleomorphic adenoma, tumors are often located or extend into the parapharyngeal space. 1 The parapharyngeal space is a complex suprahyoid anatomical space, described as an inverted pyramid with the base formed by the skull base and the apex reaching the greater cornu of the hyoid bone. It is lateral to the pharynx and contains 2 compartments, the prestyloid and poststyloid compartment. 5 The differential diagnosis of benign parapharyngeal space (PPS) tumors includes PAs of the salivary glands, which are the most common, followed by paragangliomas and neurogenic tumors. 5 Magnetic resonance imaging (MRI) is considered the method of choice for evaluating PA. 4 Surgical excision remains the best treatment for PPS tumors. Different surgical approaches have been described, including transcervical, transparotid, transoral, infratemporal, and transmandibular alone or in combination. These approaches have been used to resect PPS tumors depending on the size, location, relationship with the surrounding vessels and nerves, and surgeon’s preference. 5 The recommended treatment for recurrent PA included surgical excision, radiation therapy, or a combination of these. 2 Since not all tumors with rupture of the capsule recur, and some recur after adequate surgery, the causes for recurrent PA seem to be multifactorial. 3 Here we present a case of recurrent giant PA that extends to parapharyngeal space after previously limited excision.
Case presentation
A 45-year-old male presented to the otolaryngology clinic with a complaint of a mass on the right side of his neck that he noticed about a year ago with a gradual increase in size. He reported severe dysphagia, particularly with solid foods. He also experienced mild dyspnea and a sensation of a pharyngeal foreign body. The patient had undergone limited surgical excision of a parotid mass diagnosed as a PA 7 years earlier. Before he became aware of the swelling in his neck, he had been asymptomatic for roughly 6 years. No significant weight loss has been noted, and the patient denied any medical history.
On clinical examination, a firm, non-tender, well-circumscribed mass approximately 3 cm in diameter was palpated in the right parotid region precisely on the previous surgical scar. A smaller mass was also medial and inferior to the previous one (Figure 1A). In addition, swelling in the soft palate with reddish overlying mucosa was observed (Figure 1B). No cervical adenopathies were palpated, and all cranial nerves were undamaged. An MRI revealed a massive multi-lobulated deep parotid lobe mass occupying the whole right parapharyngeal space, extending to the skull base upward, pushing the pharynx to the other side. It also caused the posterior dislocation of the vascular-nervous bundle. Beneath the platysma muscle, other masses appeared to be distinct from the main huge mass (Figure 2).

(A) Clinical examination reveals 2 adjacent masses with the previous surgical scar. (B) Right submucosal swelling with reddish mucosa.
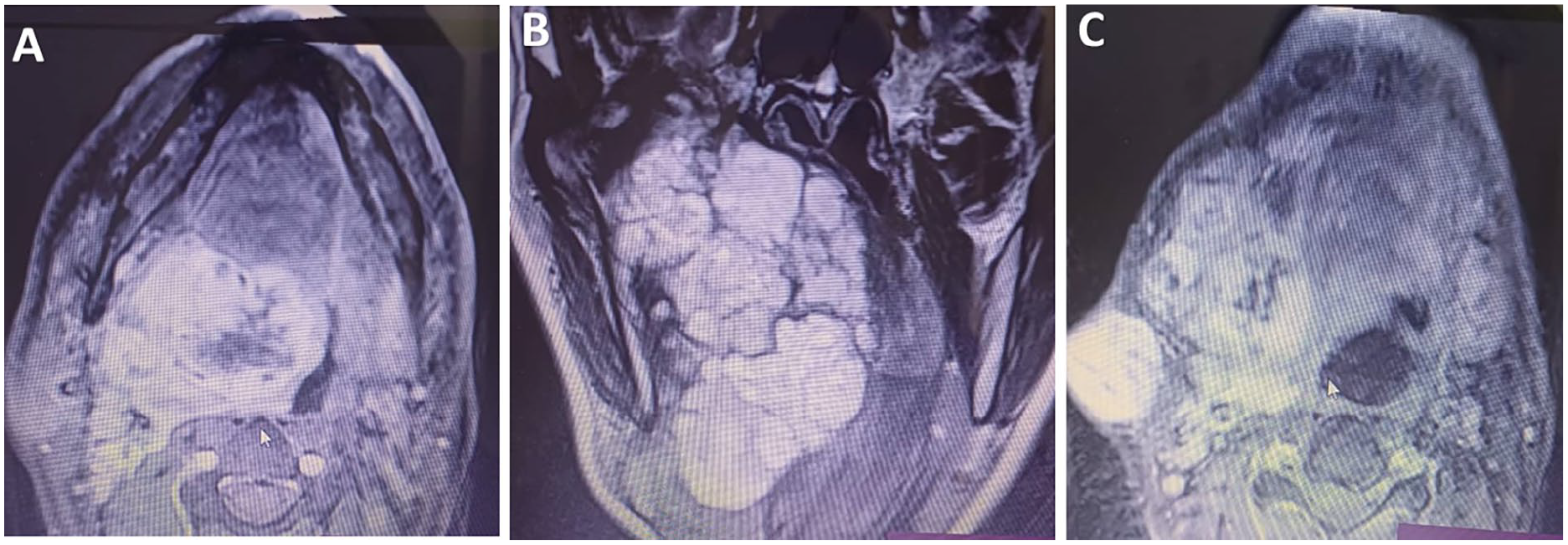
MRI: (A) Axial scan reveals a huge mass in the parapharyngeal space. (B) A coronal scan shows the multi-lobulated appearance of the mass. (C) Subcutaneous independent mass. MRI, magnetic resonance imaging.
Surgical excision was performed by a cervical-transparotid approach combined with a mandibular swing approach to access the complete removal of the mass (Figure 3). A tracheostomy was performed prior to surgery. The superficial parotid lobe was removed with the preservation of the facial nerve. Then, the entire mass along with the deep lobe was extracted from the parapharyngeal space. Small masses that resembled the primary tumor were noted to be attached to the platysma muscle. They were excised, sacrificing part of the platysma and marginal nerve due to intense attachment. Histological examination confirmed the recurrence of PA with clear margins, but focally close to the tumor, approximately 5 mm away. After 7 days, the patient was decannulated and discharged. He was subsequently admitted to radiotherapy.
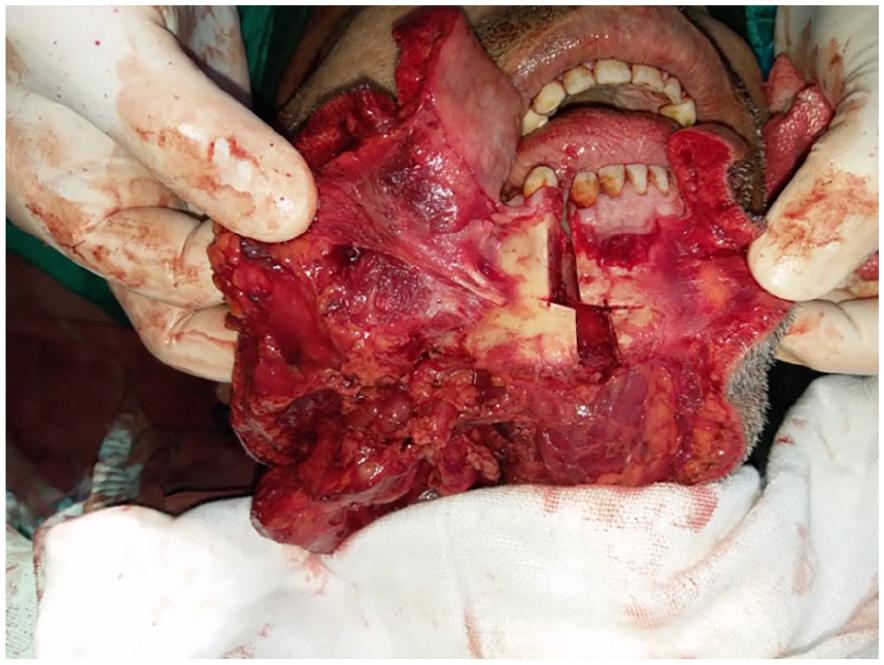
Mandibular osteotomy to full access to the mass.
Discussion
Parapharyngeal space tumors (PPT) are rare, accounting for 0.5% of head and neck neoplasms. Most of these tumors (70%-80%) are benign and 40% to 50% of these originate in the salivary glands, particularly the PA. PA in the PPS can develop de novo or may arise from the deep lobe of the parotid gland and extend into the PPS.8,9 PA is a benign salivary gland tumor composed of proliferating ductal and myoepithelial elements in a variably myxoid to chondroid background stroma which may demonstrate an infinite number of architectural configurations. and due to its slow growth, it can remain undetected for a long time till it exceeds about 3 cm in size.4-8 Although PAs are benign, recurrences are observed in about 5% of all cases after surgery. Recurrence is mainly observed in those cases characterized by the focal absence of the capsule that often envelops the tumors, with microscopic tumor projections into the surrounding parotid tissue, or in cases of capsule rupture occurring during surgical removal of the tumor. Simple enucleation of the tumor may leave these projections behind and thus increase the risk of recurrence. 8 In our case, the patient had undergone a limited surgical excision of his original PA 7 years earlier.
Recurrent PA may present as a solitary mass or may present at many sites as multinodular distinct masses spreading within the previous surgical bed due to the scattering of tumor cells during the surgery as our patient. PPT frequently manifests via medial displacement of the lateral wall of the oropharynx or a growth on the upper neck, and nearly 50% of patients present with a neck mass. In addition to the mass effect, the clinical manifestations of parapharyngeal space tumor include a foreign body sensation in the throat, swallowing difficulties and voice changes, as well as trismus, otological symptoms secondary to Eustachian tube obstruction, and, more rarely, obstructive sleep apnea. The appearance of facial pain or paralysis of the cranial nerves is associated with malignant degeneration.8-11
Computed tomography scans and MRIs are vital tools for PPS tumors. MRI is, actually, the imaging technique of choice for these tumors. Accurate in 95% of cases, it allows delineation of all PPS masses and precise its relationship to the surrounding tissues which helps the surgeon to determine the appropriate approach. Normal anatomy and tumor-fat interface are best studied on T1-weighted sequences, whereas tumor margins and tumor-muscle interface on T2-weighted sequences.6-12
The management of recurrent PA represents a challenge for surgeons, especially in cases with excessive extension to surrounding spaces due to the presence of vital neurovascular elements. The literature advocates various surgical approaches for the excision of PPS tumors, including PA. The intraoral approach, also known as transoral or transpalatal, is useful when a small benign avascular tumor is presented in the oropharynx that does not extend to the styloid process. The transcervical approach is the most frequently used approach for the excision of PPS tumors, large tumors measuring up to 11 cm can be excised successfully. This approach provides direct access to the PPS and gives adequate control over the neurovascular bundle in the neck. A combined transparotid-transcervical approach is useful with tumors in the poststyloid compartment or for those originating from the deep lobe of the parotid gland extending to PPS. Transcervical approaches can also be combined with mandibulotomy in cases of malignant tumors, tumors with vascular origin, and recurrent tumors. In some types of osteotomies, lip-splitting may be required. In these cases, due to damage to the floor of the mouth during the surgery, tracheostomy, and nasogastric tube feeding may be required.10-12 In our case, a transparotid-transcervical approach with median mandibulotomy was used due to the large extension of the tumor which occupies the right parapharyngeal space extending upward to the skull base (with no signs of bony destruction), downward to the submandibular region, with extension along the previous scar reaching the subcutaneous plane. Postoperative radiotherapy may prevent the recurrence of PA; however, clinicians must weigh the risk of recurrence against the complication of cerebral damage and late malignant transformation. 5 In our case, the patient had been admitted to radiotherapy due to the giant size of the tumor which was very close to the clear margin.
Conclusion
Parapharyngeal space tumors, while infrequent, present considerable challenges in clinical management. This case underscores the necessity for meticulous surgical planning and precise excision during the initial treatment of PA to mitigate the risk of recurrence. Such recurrences may complicate subsequent interventions, particularly if tumor extension into the parapharyngeal space occurs. The parapharyngeal region is home to critical neurovascular structures, and inadvertent injury to these components during surgical procedures can lead to significant complications. Therefore, comprehensive preoperative evaluation and judicious surgical strategies are imperative to enhance patient safety and optimize clinical outcomes.
Footnotes
Acknowledgements
The authors are grateful for their colleagues in Al-Mouwasat Hospital in the ENT-HNS department.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Written informed consent was acquired from the patient for publication of this article.