
Abstract
Objective:
To investigate a minimally invasive treatment method for piriform sinus fistula during infection.
Methods:
A retrospective analysis was performed on children diagnosed with pyriform sinus fistula infection at the Women’s and Children’s Hospital of Qingdao University from January 2022 to December 2024. All patients underwent ultrasound-guided puncture combined with endoscopic low-temperature plasma closure of the internal fistula. Successful treatment was defined as complete fistula closure following a single hospitalization and surgical procedure.
Results:
A total of 14 children (7 males and 7 females) were included, of whom 12 had left-sided lesions and 2 had right-sided lesions. In all 14 cases, the internal fistula scar in the piriform sinus healed well, exhibiting only slight mucosal edema. MRI findings showed significant reductions in cystic cavity size and relief of airway compression. Fiberoptic laryngoscopy confirmed closure of the internal fistula without evident tissue swelling. Postoperative dysphagia occurred in 4 patients but resolved gradually within 1 week. No complications related to recurrent or superior laryngeal nerve injuries, such as hoarseness or cough, were observed. During a follow-up period of 6 to 24 months, 1 patient experienced relapse, while the remaining patients exhibited no swelling or symptoms of respiratory compression.
Conclusion:
Ultrasound-guided puncture combined with endoscopic low-temperature plasma closure is an effective, minimally invasive, and safe approach for the treatment of infected piriform sinus fistula. This method can serve as a minimally invasive therapeutic option during active infection.
Introduction
Congenital piriform sinus fistula (CPSF) is a rare lesion originating from abnormal embryonic development of the third and fourth branchial clefts, predominantly affecting children. Its primary clinical manifestations are recurrent neck abscesses and acute suppurative thyroiditis. 1 Traditional treatment involves complete fistula excision via an external cervical approach during the stable inflammatory phase. During the acute infection phase, conservative treatment, including active anti-infection therapy and abscess drainage, is usually adopted.2,3 However, the external cervical approach is associated with considerable trauma, surgical complexity, numerous complications, and esthetically unfavorable neck scars.2,3 Recent technological advancements have led to the development of minimally invasive treatments, including endoscopic electric cauterization, chemical cauterization, and CO2 laser cauterization, for CPSF during stable inflammation. Due to their minimally invasive, safe, and effective nature, these methods have gradually gained acceptance.4,5 However, electric cauterization and CO2 laser cauterization generate temperatures between 400 °C and 1000 °C, causing significant thermal injury to adjacent tissues and potentially injuring the superior or recurrent laryngeal nerves. Additionally, chemical cauterization with agents like chloracetic acid poses difficulties in controlling cauterization depth and area, often necessitating multiple procedures and potentially resulting in esophageal stenosis. Few studies have reported using endoscopic low-temperature plasma for minimally invasive treatment of CPSF during the infection phase in children. This study retrospectively analyzed 14 cases of CPSF treated at our hospital from 2022 to 2025 using ultrasound-guided puncture combined with endoscopic low-temperature plasma cauterization to close the internal fistula during infection. The clinical efficacy of this method was assessed to provide a new therapeutic reference for pediatric CPSF treatment.
Data and Methods
Clinical Data
A total of 14 patients diagnosed with piriform sinus fistula and treated at our hospital from January 2022 to December 2024 were retrospectively analyzed. Patients comprised 12 cases of the sinus type and 2 cases of the fistula type. Patient ages ranged from 1 to 15 years, with a median age of 5 years. Seven patients were male and 7 were female. All patients had received antibiotic therapy before surgery but had not undergone any previous surgical intervention (Figure 1).

Left neck swelling.
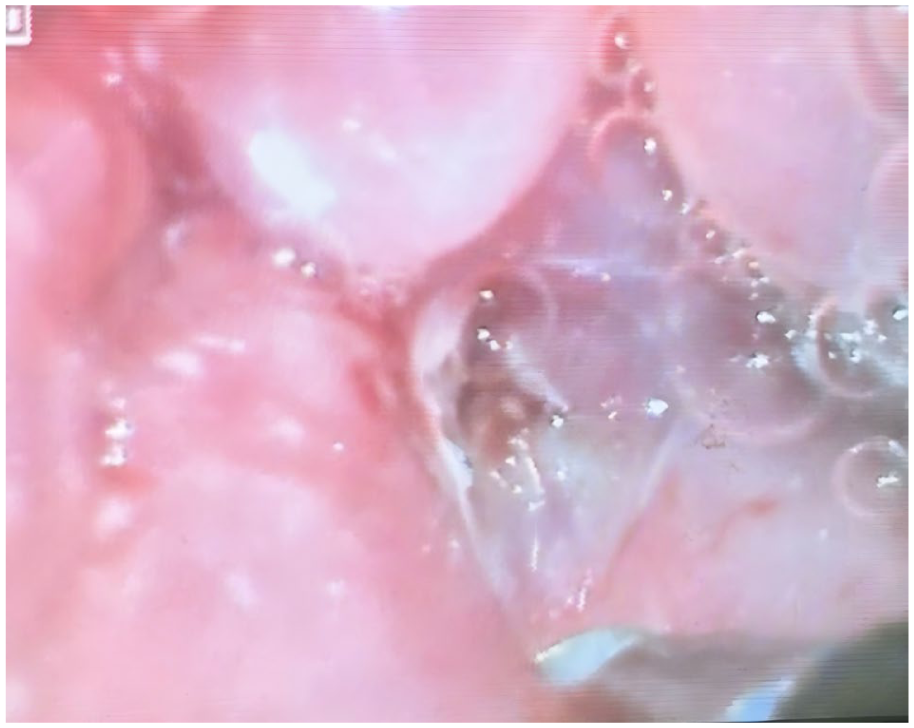
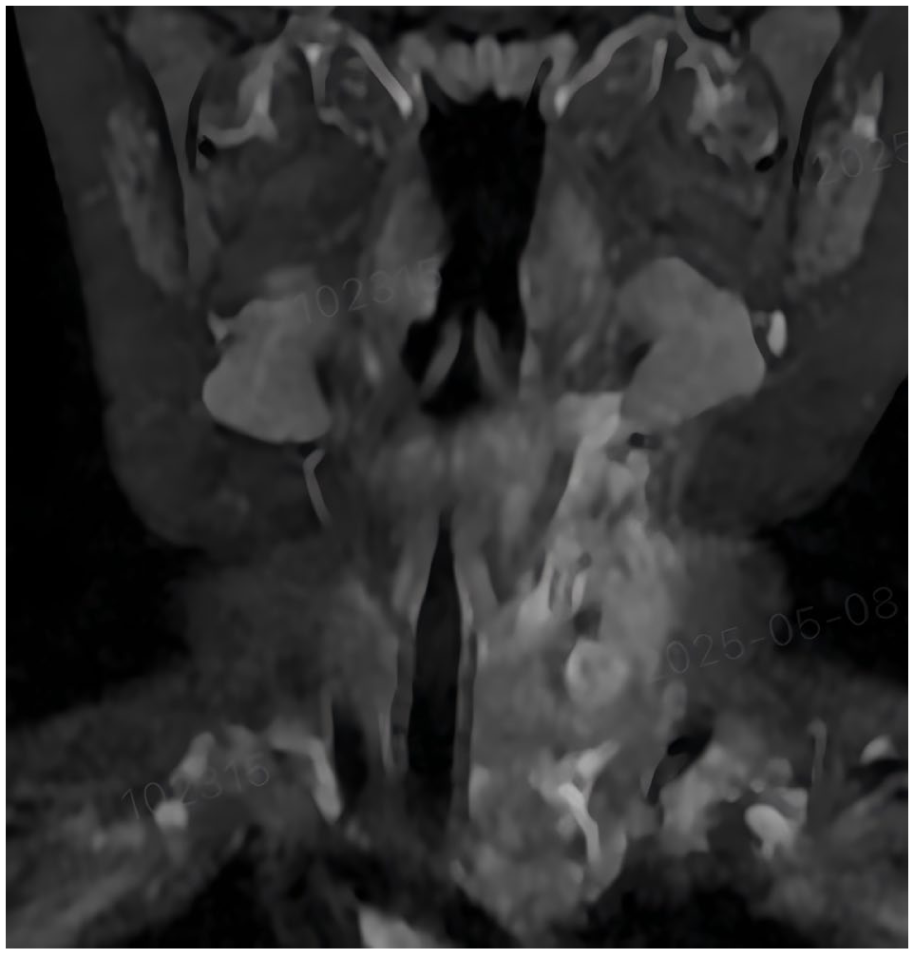
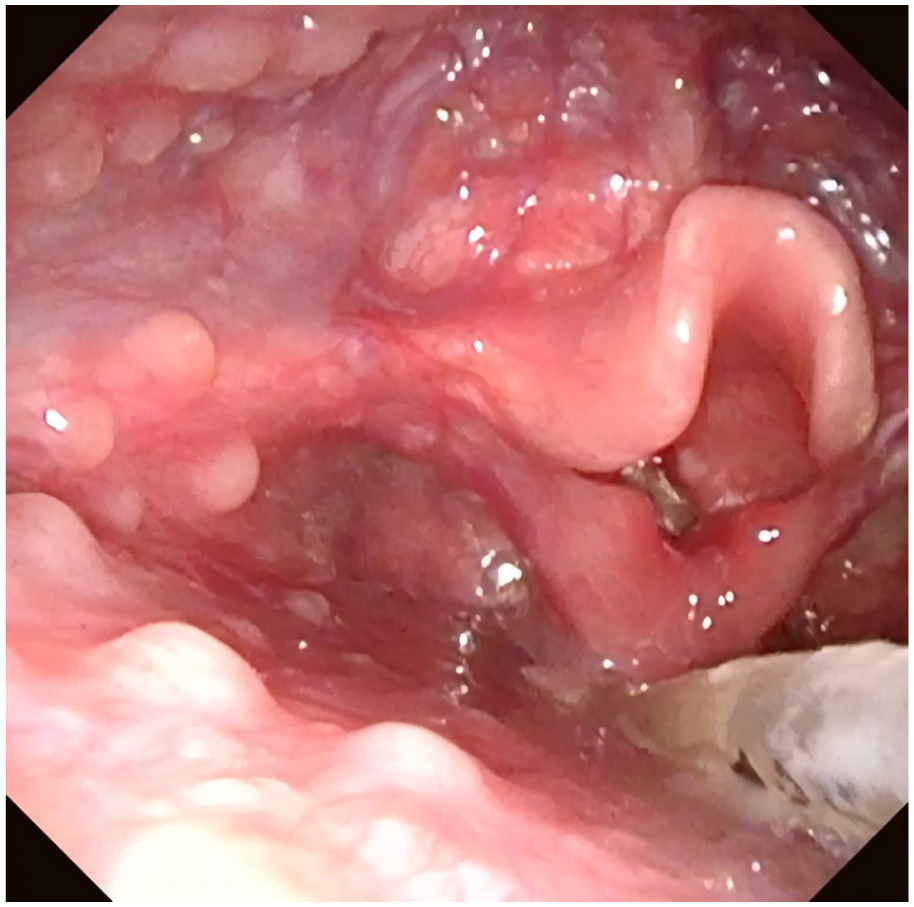
All patients underwent preoperative neck imaging and fiberoptic laryngoscopy. MRI plain scans confirmed piriform sinus fistula in 6 cases (Figure 2), while ultrasound examination confirmed the diagnosis in 10 cases. Fiberoptic laryngoscopy revealed swelling in the piriform fossa (Figure 3) or internal fistula formation in 4 cases (Figure 4). All patients received initial treatment at our hospital, undergoing ultrasound-guided puncture combined with endoscopic low-temperature plasma closure of the internal fistula. The internal fistula was located on the left side in 12 patients and on the right side in 2 patients. Among these, there were 12 sinus-type cases, 2 fistula-type cases, and no cyst-type cases (Table 1).
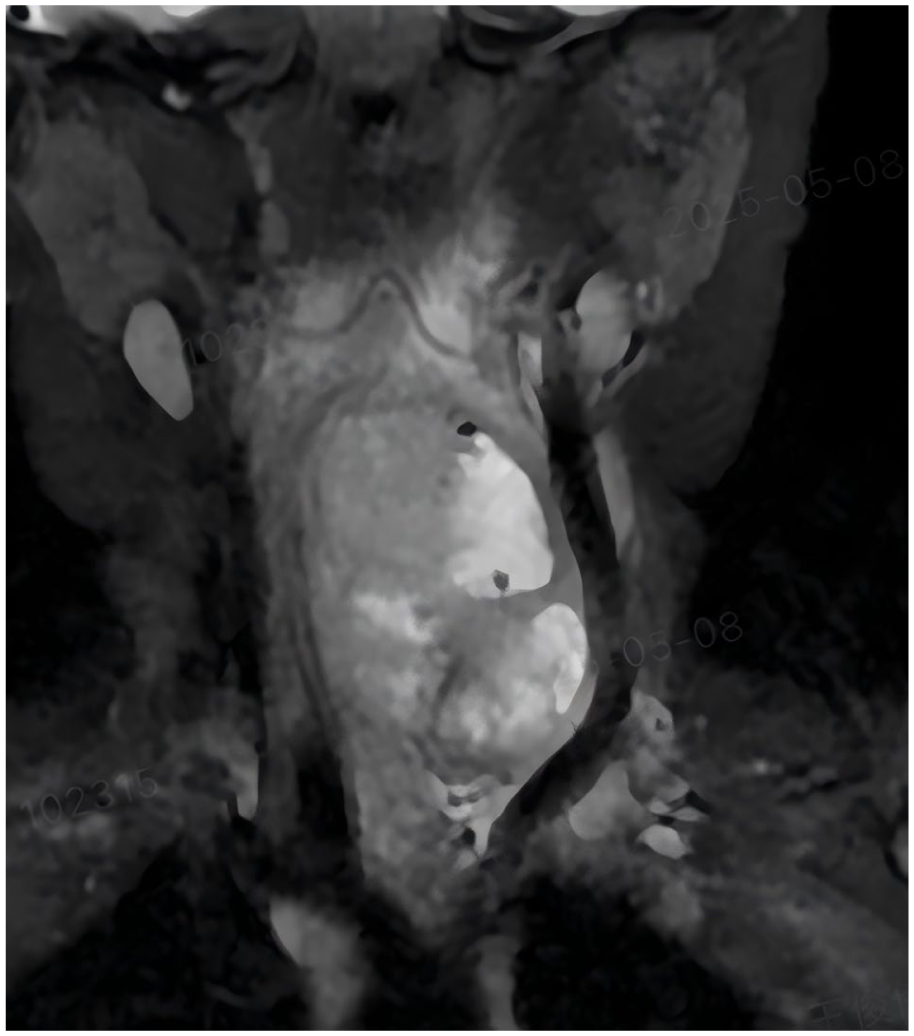
MRI appearances.
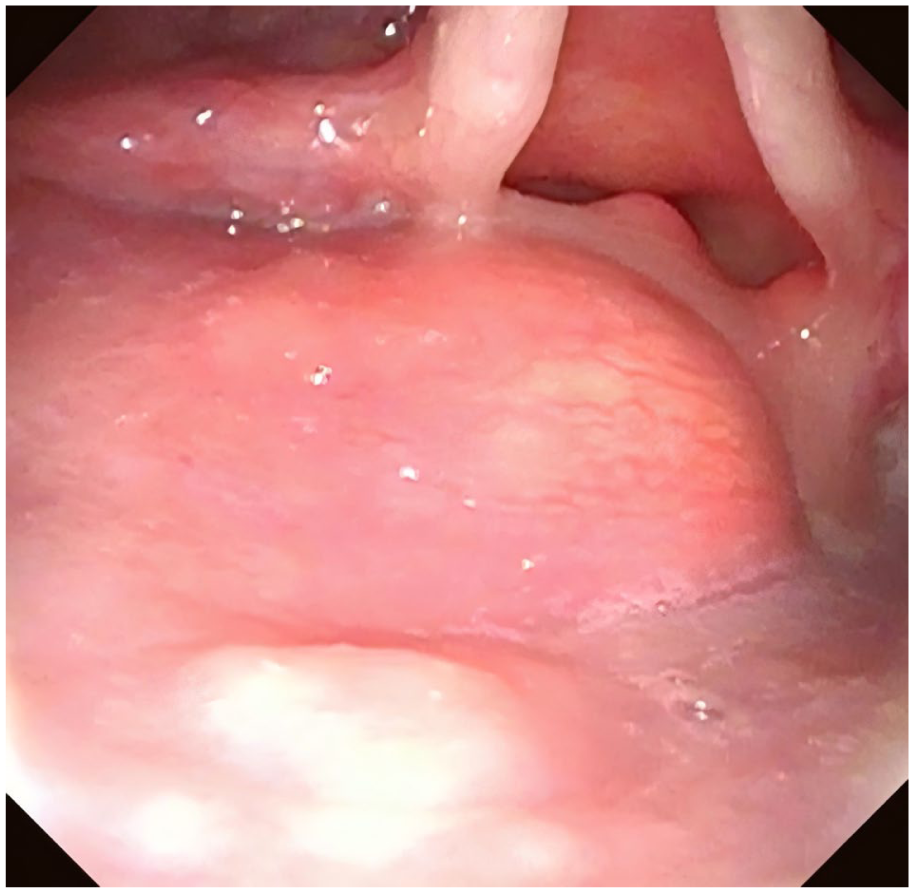
Fiber laryngoscope examination.
Basic Clinical Data of 14 Patients With CPSF (Cases).
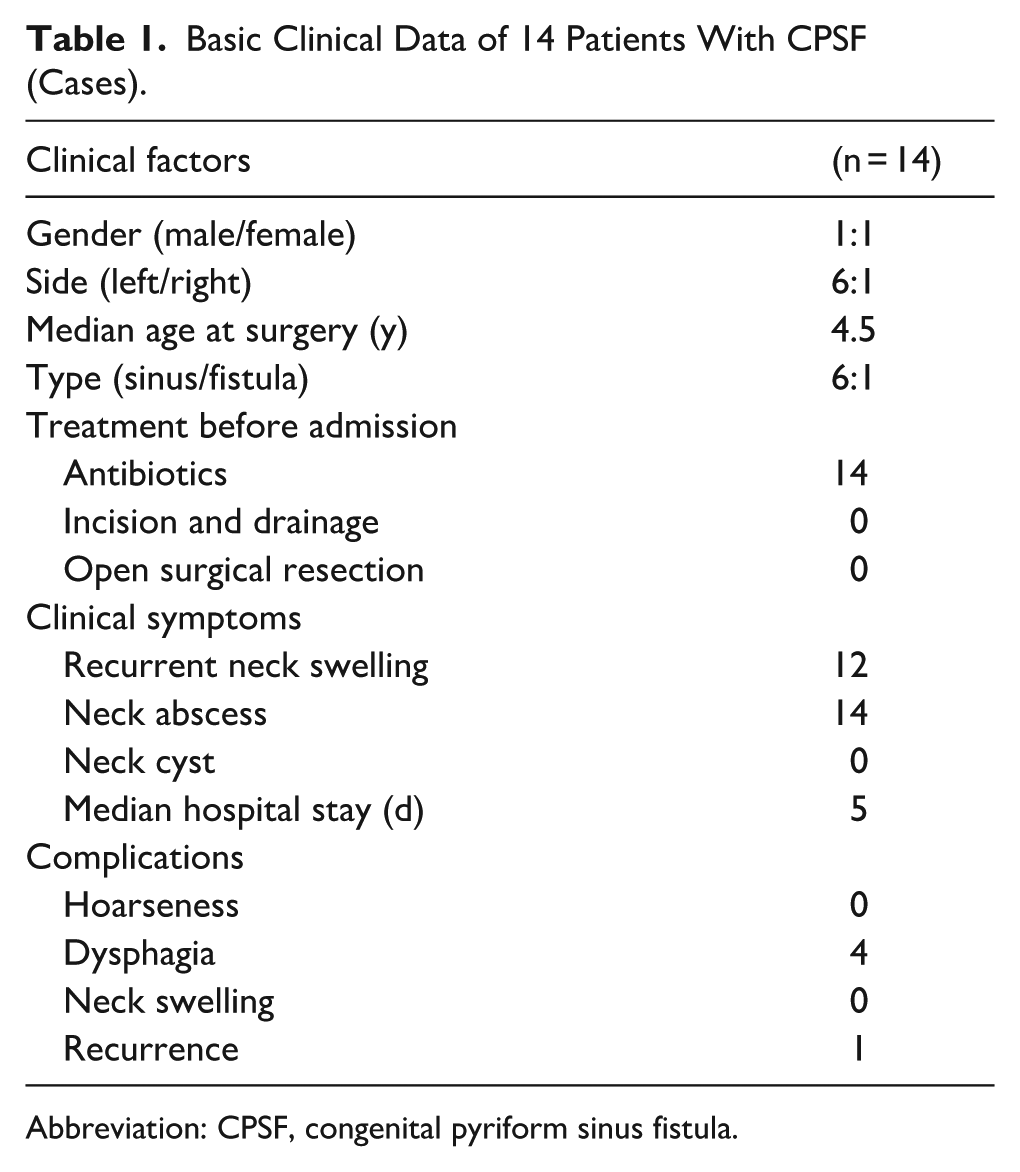
Abbreviation: CPSF, congenital pyriform sinus fistula.
Surgical Methods
Following admission, vital signs were monitored, oxygen therapy was administered, and antibiotics were initiated for all patients. Initially, a drainage tube (22 G single-lumen deep vein puncture catheter) was inserted under ultrasound guidance (Figure 5). The aspirated fluid appeared thin and beige. The indwelling drainage tube enabled repeated fluid drainage and cyst irrigation. After 3 to 5 days, drainage volume decreased, and neck swelling gradually resolved. Subsequently, endoscopic low-temperature plasma cauterization of the internal fistula in the piriform fossa was performed under general anesthesia. Bilateral piriform fossae were examined endoscopically. After identification of the internal fistula (Figure 4), normal saline was repeatedly injected through the drainage tube until the fluid draining from the internal orifice appeared clear. A low-temperature plasma probe was then inserted 1 cm into the internal fistula, and thorough cauterization was performed from the inside outward. Each cauterization lasted 1 to 2 seconds and was repeated 2 to 3 times until the surrounding mucosa turned white, indicating complete closure of the internal fistula (Figure 6). Following adequate hemostasis, no active bleeding was observed. Nasogastric tube feeding was provided for 1 week postoperatively. The neck drainage tube was removed after 2 to 3 days, once daily drainage volume fell below 2 mL.
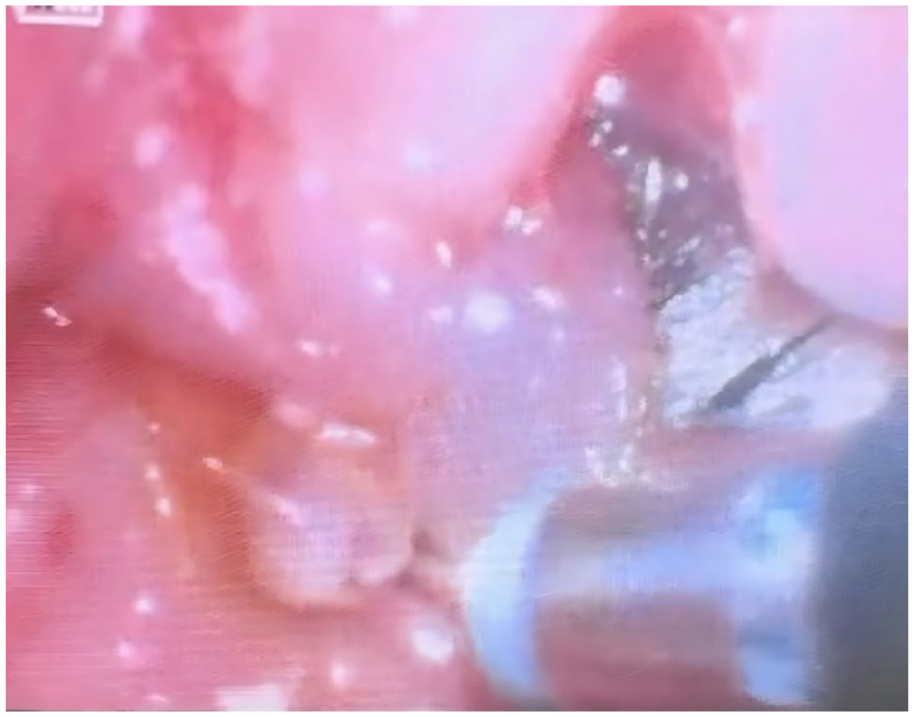
Identification of the internal fistula.
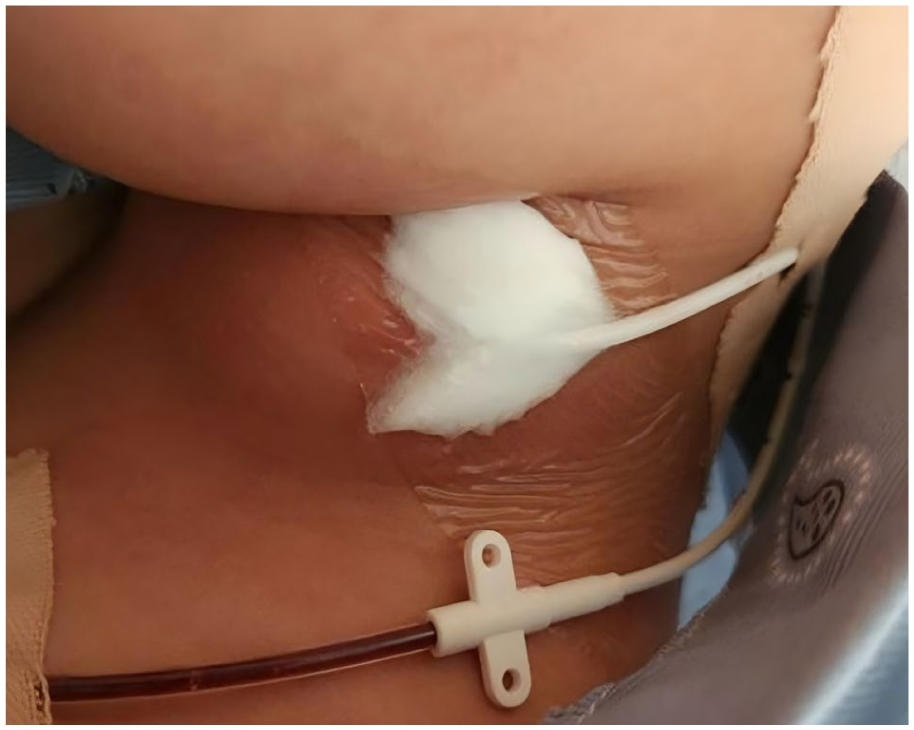
22 G single-lumen deep vein puncture catheter.
Complete closure of the internal fistula.
Results
The average operation time was 40 ± 14.94 minutes (range: 20-60 minutes). The average hospital stay was 12.57 ± 1.87 days (range: 9-15 days). Antibiotic therapy was continued for 1 week postoperatively. After 1 week of nasogastric tube feeding, repeat fiberoptic laryngoscopy showed good scar formation at the piriform fossa fistula site with mild mucosal edema in all 14 patients. Subsequently, the gastric tube was removed, and oral feeding resumed. Follow-up MRI indicated significantly reduced cystic cavity size and relief of airway compression (Figure 7). Repeat fiberoptic laryngoscopy demonstrated complete closure of the internal fistula without obvious tissue swelling (Figure 8). Four patients experienced postoperative dysphagia, which gradually resolved within 1 week. No complications, such as injury to the recurrent or superior laryngeal nerves, hoarseness, or cough, were observed. During the follow-up period of 6 to 24 months, 1 patient experienced relapse, while the remaining patients exhibited no swelling or airway compression symptoms.
Postoperative MRI appearances.
Postoperative fiber laryngoscope examination.
Discussion
CPSF is an extremely rare congenital malformation originating from branchial clefts, accounting for ~2% to 10% of all branchial cleft anomalies. 6 Approximately 93% to 97% of CPSF cases occur on the left side, potentially due to the elongated and complex anatomical pathway of the left fistula and asymmetric vascular development. 7 CPSF predominantly occurs in children, accounting for ~80% of cases, with no significant gender differences. In this study, the male-to-female ratio was 1:1. 8 Among the 14 patients included, 12 cases (85.71%) had left-sided lesions, slightly lower than previously reported, which may be attributed to the small sample size. CPSF is classified into 3 types: cyst, sinus tract, and fistula, with the sinus tract type being most common. The cyst type primarily occurs in fetuses or newborns. 7 This study included 12 sinus-type and 2 fistula-type cases, consistent with previous reports.
Due to the low incidence of CPSF, the absence of specific clinical symptoms during noninfectious periods, atypical imaging features, and limited clinician familiarity with this condition, the rates of misdiagnosis and posttreatment recurrence remain high. Upper respiratory tract infections may facilitate bacterial entry through the fistula, leading to acute infection. Early clinical symptoms include painful neck masses, recurrent fever, or acute suppurative thyroiditis, occasionally accompanied by diffuse neck swelling. 9 In later stages, neck abscesses may develop. Following incision and drainage, recurrence or persistent fistula formation frequently occurs. Antibiotic therapy and abscess drainage alone are insufficient for effectively curing piriform sinus fistula.
The 14 children included in this study were transferred from other departments due to ineffective antibiotic treatment. Initial diagnoses included left-sided neck abscess (9 cases), acute thyroiditis (3 cases), thyroid abscess (1 case), and infected cystic neck mass (1 case). As CPSF often terminates at or traverses the upper pole of the lateral thyroid lobe, inflammation readily spreads to the thyroid gland, resulting in abscess formation. Clinical manifestations include recurrent deep neck infections or persistent suppurative thyroiditis. In this study, 4 children initially presented with acute thyroiditis or thyroid abscess. Therefore, CPSF should be suspected in children presenting with recurrent anterior neck swelling or acute thyroiditis, especially when symptoms occur on the left side.
CPSF must be differentiated from various other neck diseases due to its nonspecific clinical presentation. When presenting as a cystic neck mass, it should be distinguished from lymphangioma, cystic teratoma, esophageal cyst, cervical thymic cyst, laryngocele, and bronchogenic cyst. When presenting as inflammatory neck swelling, CPSF should be differentiated from first and second branchial cleft anomalies, thyroglossal duct fistula, cervical lymphadenitis, acute suppurative thyroiditis, cervical cellulitis, epidermoid cyst infection, cervical tuberculosis, foreign-body infection, infections originating from tonsillar, pharyngeal, or odontogenic sources, and thyroid cysts.10 -12
Advances in imaging techniques have improved the diagnostic accuracy of CPSF. For children with suspected CPSF, ultrasound, esophageal barium swallow, neck MRI, and fiberoptic laryngoscopy are recommended examinations.13 -17 Fiberoptic laryngoscopy identifying the fistula within the piriform fossa is the gold standard for diagnosing CPSF; however, the need for general anesthesia limits its widespread use. 18 Detection of the internal fistula is challenging, as it may be obscured by mucosal folds or edema. Therefore, pronounced edema in the piriform fossa strongly suggests CPSF. In this study, fiberoptic laryngoscopy identified internal fistulas in 4 cases (28.57%). Consequently, fiberoptic laryngoscopy performed under general anesthesia is the preferred diagnostic method for children highly suspected of having CPSF.
Ultrasound imaging can reveal deep neck soft tissue infections and clarify the relationship between the infected region and thyroid gland, although it may easily lead to misdiagnosis as a common soft tissue infection of the neck. In this study, ultrasound correctly identified CPSF in 10 cases (83.33%). Esophageal barium swallow typically demonstrates a thin, tubular filling defect in the affected piriform fossa, although cooperation from infants is often limited. 19 Only 3 patients underwent this examination, which yielded negative results due to fistula obstruction caused by edema during acute infection. Therefore, radiographic evaluation is recommended during stable inflammatory periods. Computed tomography (CT) imaging typically reveals a shallow or absent piriform fossa on the affected side. Infections involving the ipsilateral thyroid gland may show air-containing spaces. In this study, CT correctly identified 8 cases (57.14%), making it an effective complementary examination when barium swallow results are negative. 20 MRI typically demonstrates low-signal infectious lesions and abscesses involving the thyroid gland posterior to the thyroid cartilage on T2-weighted images. 21 However, due to its high cost and difficulties in obtaining patient cooperation, MRI is not recommended as the primary diagnostic method for CPSF. Considering their noninvasive nature, minimal radiation exposure, repeatability, and good patient compliance, ultrasound and/or MRI are recommended examinations.
Studies have indicated that Streptococci or viridans streptococci are the predominant pathogens in pediatric patients with infected piriform sinus fistula. In contrast, common pathogens in adults include Klebsiella pneumoniae, possibly due to differences in immunity between children and adults. 22 In this study, bacterial cultures were obtained from all patients, and viridans streptococci were identified in 3 cases. Therefore, once an abscess has formed, prompt puncture and drainage should be performed, and appropriate antibiotics are selected based on culture results.
During the acute infection phase of CPSF, traditional management typically involves intensive antibiotic therapy to control the infection. If an abscess develops, incision and drainage are performed, followed by open surgical excision after infection resolution.7,18 During incision and drainage of an abscess, a relatively long surgical incision is typically required in the neck. Following the procedure, the open wound necessitates daily irrigation and dressing changes, which can compromise patient comfort. Moreover, after infection control is achieved, further wound healing is required before an open fistulectomy can be performed. Open surgery is time-consuming, often involves extensive tissue dissection, increases the risk of nerve injury, and results in noticeable scarring in the neck. In this study, ultrasound-guided puncture and drainage were employed as an alternative to conventional incision and drainage. Under real-time ultrasound guidance, this technique allows for precise localization and drainage of abscesses or fluid collections associated with pyriform sinus fistula, thereby minimizing damage to surrounding tissues. After catheter placement, the cavity can be irrigated, and negative-pressure suction can be applied to facilitate pus evacuation. Given its potentially less invasive nature, this approach may reduce postoperative pain, bleeding, and infection risk, promote faster recovery, and effectively lower the incidence of iatrogenic infection. 23 Previous studies have reported an open-surgery failure rate of 15% and a complication rate of 6%, with the most common complications being vocal cord paralysis, salivary fistula, and infection.2,3
In 1998, Jordan et al first reported endoscopic electrocautery treatment for CPSF without recurrence or complications during an 18 month follow-up period. 24 Subsequently, numerous studies have explored other endoscopic treatments, including laser cauterization, chemical cauterization, fibrin glue bonding, and suturing. Due to their simplicity, high success rates, fewer complications, and absence of neck scars, these techniques have become preferred methods for CPSF management.4,5 Nevertheless, electrocautery and CO2 laser methods generate temperatures ranging from 400 °C to 1000 °C, causing significant thermal damage to surrounding tissues and potential injury to the superior and recurrent laryngeal nerves. Additionally, laser procedures carry fire risks. 25 Chemical cauterization using agents such as trichloroacetic acid poses challenges in controlling cauterization depth and extent, frequently requires repeated treatments, and carries risks of postoperative esophageal stenosis and transient hoarseness. 26
Historically, a stable inflammatory phase was considered essential prior to endoscopic treatment. 3 However, given the recurrent and unpredictable nature of CPSF episodes and limitations of current endoscopic techniques, there is an urgent need to develop safer, simpler, and more feasible minimally invasive approaches during acute infection episodes. Low-temperature plasma, a novel energy-based platform, operates at lower temperatures than conventional electrocautery, resulting in less collateral tissue damage. Moreover, this equipment is widely accessible and has gained broad clinical acceptance.
Low-temperature plasma cauterization destroys the internal fistula and adjacent mucosa, resulting in scar formation, adhesion, and closure. This procedure prevents pharyngeal secretions and pathogens from the upper respiratory and digestive tracts from entering the fistula, thus reducing infection risk. Several studies have compared the one-time fistula closure rates during acute infection versus stable inflammatory periods. Closure rates were 100% during the acute infection period and 98% during the stable inflammatory phase, with no statistically significant difference between the 2 periods. These findings provide theoretical support for performing internal fistula closure during acute infection.18,27,28 Although some researchers have recommended simultaneous endoscopic closure of the internal fistula with abscess drainage, identifying the internal fistula endoscopically during acute or subacute infection phases of CPSF remains challenging. 29 Therefore, this study employed catheterization, wherein saline injection into the cavity facilitated locating the internal fistula. In this study, 14 children with acute CPSF infections underwent ultrasound-guided puncture and catheterization. After drainage for 3 to 5 days, endoscopic low-temperature plasma radiofrequency ablation was performed under general anesthesia to close the internal fistula. Nasal feeding was continued for 1 week postoperatively, and continuous neck drainage was maintained without negative pressure. The mean operation time was 40 ± 14.94 minutes. The longest operation time was 60 minutes in early cases due to varying surgical proficiency, while subsequent operations averaged 20 minutes, significantly shorter than the mean duration reported by Pan et al. 30 After 1 week of nasogastric feeding, the neck was maintained under nonnegative pressure continuous drainage. When drainage output was <2 mL, the drainage tube was removed, and antibiotics were administered for 1 week. The mean hospitalization duration was 12.57 ± 1.87 days, slightly longer than that reported for open surgery, primarily due to postoperative drainage and nasogastric feeding requirements following low-temperature plasma ablation. However, this extended hospitalization did not reflect increased surgical trauma. Neck swelling completely subsided within 4 weeks, and only 1 patient experienced recurrence during 6 to 24 months of follow-up. All patients experienced mild postoperative neck pain, and 4 patients reported transient dysphagia, which resolved within 1 week. The operation times of these 4 patients were 60, 60, 55, and 55 minutes, suggesting that dysphagia may be associated with longer procedures and limited operator experience. These results demonstrate the effectiveness and feasibility of ultrasound-guided catheterization combined with endoscopic low-temperature plasma radiofrequency ablation for the treatment of acute CPSF infections. Based on our findings, ultrasound-guided catheter drainage combined with endoscopic low-temperature plasma radiofrequency ablation for fistula closure is more suitable for patients with pyriform sinus fistula accompanied by abscess formation who require urgent drainage but are ineligible for open surgery, as well as for those with high esthetic demands.
The criteria for successful CPSF treatment included the absence of neck pain or swallowing discomfort on the affected side and confirmation of internal fistula closure via fiberoptic laryngoscopy at 1 and 3 months postoperatively. Based on these criteria, recurrence occurred in 1 case (7.14%) following low-temperature ablation. The failure was attributed to incomplete cauterization of the sinus mucosa due to limitations in the direction and angle of the fistula, leading to remucosalization and sinus reformation. To minimize recurrence risk, several points should be considered: (1) during endoscopic plasma ablation, the probe should be inserted deeply to the base of the fistula (typically more than 1 cm) to ensure thorough cauterization of the entire mucosal lining, although exact cauterization depth may be challenging to estimate, particularly in children. (2) Because mucosal healing takes ~7 days postablation, all children in this study were maintained on a nasogastric feeding regimen for 1 week after surgery. (3) Residual fistulas after treatment may cause secondary infections, particularly if residual sinus tracts persist near the thyroid gland.
In summary, for children with acute CPSF infection and intact neck skin, especially those with limited mouth opening or restricted endoscopic visibility, ultrasound-guided puncture, and catheter drainage combined with endoscopic low-temperature plasma radiofrequency ablation are recommended. Low-temperature plasma ablation has proven effective for treating CPSF during the acute infection stage. It offers advantages such as minimal invasiveness, repeatability, wide age applicability, good clinical compliance, and fewer treatment sessions for young children. However, this study is limited by its small sample size and short follow-up duration. Therefore, larger multicenter studies with extended follow-up periods are required to validate these findings.
Footnotes
Ethical Considerations
The studies involving human participants were reviewed and approved by the ethics committee of Qingdao Women and Children’s Hospital.
Consent to Participate
The patient’s legal guardian provided written informed consent to participate in this study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Supported by Qingdao Key Medical and Health Discipline Project.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.