
Abstract
Objective:
This study aimed to identify the risk factors associated with olfactory dysfunction (OD) in patients with chronic rhinosinusitis without nasal polyps (CRSsNP), a prevalent condition where impaired smell significantly reduces quality of life. The goal was to provide insights for improving clinical management strategies.
Methods:
A prospective study was conducted on patients undergoing endoscopic surgery. CRSsNP patients were categorized into an OD group (n = 36) and a normosmic group (n = 36) based on olfactory tests, with 21 septoplasty patients as healthy controls. Demographic and clinical data were analyzed. Logistic regression and receiver operating characteristic (ROC) curves were used to identify independent risk factors and assess their predictive value.
Results:
A total of 93 subjects were included. Comparative analysis revealed no significant differences in age, body mass index, sex, disease duration, smoking history, drinking history, diabetes, or hypertension among the 3 groups. However, the OD group exhibited significantly lower nasal cavity volume and counts of mucosal olfactory marker protein-positive cells (STOMP). Conversely, they had significantly higher sinusitis severity scores (Lund–Mackay CT), nasal endoscopic scores (Lund–Kennedy), interleukin-5 (IL-5) levels, total serum immunoglobulin E (IgE), olfactory detection/recognition thresholds, and olfactory visual analog scale scores. Multivariate analysis confirmed that nasal cavity volume, Lund–Mackay score, Lund–Kennedy score, IL-5, IgE, and STOMP were independent influencing factors for OD. Correlation analysis further supported these findings. The ROC curve analysis validated that all these parameters had significant predictive value for identifying OD, with area under the curve values all >0.6.
Conclusion:
Nasal cavity volume, Lund–Mackay CT score, Lund–Kennedy endoscopy score, IL-5, IgE, and STOMP are significantly and independently associated with OD in CRSsNP patients. These parameters demonstrate efficacy in screening for olfactory abnormalities, enabling early identification and providing a valuable reference for optimizing clinical therapeutic strategies to improve patient outcomes.
Keywords
Introduction
Olfaction is a critical sensory function in the human body, with a broad range of mechanisms that enable comprehensive assessment of hazardous environments, thereby helping individuals avoid dangers, recognize and identify objects, and facilitate social interactions. Olfactory dysfunction (OD) can directly impact patients’ mental health, compromise their quality of life, and in severe cases, even increase mortality. 1 Chronic rhinosinusitis (CRS) has become one of the most common chronic diseases in otorhinolaryngology, primarily characterized by inflammation of the nasal cavity and nasal mucosa. It typically presents with mucopurulent nasal discharge, nasal congestion, and varying degrees of facial pressure or heaviness, as well as hyposmia. 2 According to a study by Chee et al, 3 the prevalence of CRS in the United States can be as high as 12.00%, with estimated annual direct costs reaching up to $11 billion.
Currently, based on the presence or the absence of nasal polyps, CRS is clinically categorized into 2 types, which are CRS with nasal polyps (CRSwNP) and CRS without nasal polyps (CRSsNP). 4 Upon analysis of the type of tissue remodeling, 5 there were some differences in the substance of both, with albumin deposition, pseudocysts, and stromal edema formation as the primary features of tissue remodeling in CRSwNP patients. In contrast, patients with CRSsNP have fibrosis as a key manifestation of tissue remodeling, associated with basement membrane increment and goblet cell deposition. 6 At this stage, the pathogenesis of CRS has not been clarified, and it is usually characterized by chronic inflammation and tissue remodeling of the nasal and sinus mucosa as a common feature. Related scholars have found 7 that there is usually a close correlation between the pathogenesis of CRSsNP and long-term inflammation of the nasal mucosa and impaired barrier function. Among them, the nasal mucosal barrier, as the primary line of defense of the nasal cavity, can not only achieves defense against pathogen invasion and maintain local immune balance but also preserves nasal wetness and olfactory function. 8 OD has become the most common symptom in patients with CRSsNP, and its prevalence can reach between 30% and 80%. 9
A growing body of research focuses on olfactory impairment in patients with CRSsNP. Timely identification of risk factors and implementation of targeted interventions may effectively improve olfactory function and enhance quality of life. Consequently, investigating the risk factors for OD in patients with CRSsNP is crucial for elucidating the underlying pathophysiological mechanisms and generating novel therapeutic approaches. Furthermore, such research provides evidence to inform public health policy-making, promotes the development of strategies for prevention, diagnosis, and management, and ultimately contributes to the reduction of societal health burdens.
Information and Methods
General Information
Patients who underwent endoscopic surgery admitted to the hospital between April 2023 and December 2024 were prospectively selected, among whom patients with reported chronic inflammation but without the presence of nasal polyps were categorized as CRSsNP. They were divided into an OD group (n = 36 cases) and an olfactory normal group (n = 36 cases) according to the olfactory function test. Patients with septoplasty were included as healthy controls, with a total of 21 patients included. The study was approved by the Medical Ethics Committee of Shanghai Xuhui Center Hospital. Patients and their families gave informed consent, and all procedures were conducted in accordance with the ethical standards of the 1964 Declaration of Helsinki and its subsequent amendments.
Inclusion Criteria
(1) Meeting the diagnostic criteria for CRS in Meltzer et al 10 ; (2) no history of nasal and respiratory system procedure; (3) no history of mental illness, good cognitive function, and cooperating with complete study; (4) age ≥18 years, regardless of sex.
Exclusion Criteria
(1) Patients with odontogenic sinusitis or secondary CRS; (2) individuals diagnosed with aspirin-exacerbated respiratory disease; (3) cases complicated by allergic fungal sinusitis, cystic fibrosis, or immunosuppression; (4) subjects with congenital anosmia; (5) individuals with a history of head trauma; (6) patients presenting with neurodegenerative disorders (eg, Alzheimer’s disease or Parkinson’s disease); (7) those with other conditions potentially affecting the olfactory or nasal mucosal contractility, including nasal space-occupying lesions, benign/malignant sinonasal tumors, and severe allergic rhinitis.
Data Collection
Basic information was registered and collected from the patients after admission, including age, body mass index (BMI = weight [kg]/height squared [m2]), sex, course of disease (real course of disease obtained by the physician using scientific communication techniques), history of disease (diabetes patients were in accordance with the diagnostic criteria related to diabetes in the [Cosentino et al 11 ]), hypertension patients were all in accordance with the diagnostic criteria related to hypertension in the (Flack and Adekola 12 ), smoking history (≥100 cigarettes in the past 1 year), and drinking history (≥1 drinking in a single week for 5 consecutive months).
Nasal Cavity Volume Testing
An A1-type acoustic radiometer produced by GM (United Kingdom; Irvine, Scotland, UK) was used, and the patients were tested after sitting still for 20 minutes in a relatively quiet and fixed environment with a room temperature of 20 °C to 22 °C and a humidity of 20% to 80%, in order to reduce the unknown effects caused by external factors on the nasal mucosa. With all patients given the sitting position, an appropriately sized nasal probe was selected to prevent rhinitis deformation and to achieve the adequate sealing of the nasal cavity thereby minimizing measurement error. After completing the above preparations, the patients were instructed to hold their breath for 3 to 5 seconds to try 4 measurements continuously to obtain the nasal cavity volume 2 to 5 cm from the anterior nostril before nasal mucosa contraction.
Sinusitis Severity Score (Lund–Mackay CT)
The severity of sinonasal disease was radiologically assessed using the standardized Lund–Mackay scoring system. 13 This scoring system evaluates bilateral maxillary sinuses, anterior ethmoid sinuses, posterior ethmoid sinuses, sphenoid sinuses, frontal sinuses, and the osteomeatal complex (OMC) based on coronal or axial sinus CT scans. The scoring criteria are as follows: (1) 0 points: complete sinus pneumatization without any mucosal thickening or opacification; (2) 1 point: partial sinus opacification (mucosal thickening or fluid presence without complete sinus obstruction); (3) 2 points: complete sinus opacification (significant mucosal thickening or complete sinus cavity filling with fluid). The scores from both sides were summed to obtain the final score, with a maximum total score of 12 points. Higher scores indicated more severe disease progression in patients.
Nasal Disease Severity Score 14 (Lund–Kennedy)
The Lund–Kennedy scoring was independently performed by 2 rhinologists (both with >5 years of specialized nasal endoscopy training and annual surgical volumes exceeding 200 cases) under standard nasal endoscopy to evaluate mucosal edema, discharge, and scarring. 14 Radiologists were responsible for anatomical imaging and obstruction assessment, while rhinologists focused on mucosal pathology and functional evaluation. All patients underwent axial + coronal high-resolution noncontrast CT scans of the paranasal sinuses. Image interpretation and analysis were conducted by physicians, assessing the maxillary sinus, anterior ethmoid sinuses, posterior ethmoid sinuses, pterygoid sinus, frontal sinus, and OMC. The scoring system was as follows: For sinuses: 0 points (normal), 1 point (partial opacification), 2 points (complete opacification). For OMC: 0 points (no obstruction), 2 points (obstructed).
Laboratory Indicator Tests
All participants underwent fasting venous blood collection (5 mL) from the antecubital region on the morning of the second day post-enrollment. Blood samples were processed using a fully automatic biochemical analyzer (model B03-4821-01, National Medical Device Registration No 20162400242; Siemens Healthcare Diagnostics, Inc (Tarrytown, NY, USA)). Centrifugation was performed at a radius of 8 cm, speed of 3000 rpm for 10 minutes to isolate serum and plasma, which were then stored at −80 °C until analysis. Interleukin-5 (IL-5) was quantified using a Luminex-based multiplex assay kit. Total immunoglobulin E (IgE) in tissues/serum was measured by radioimmunoassay. STOMP in the superior turbinate mucosa: mucosal tissue samples were obtained during endoscopic sinus surgery. Specimens were immediately fixed in 4% formaldehyde to preserve cellular architecture, followed by standardized tissue processing (dehydration, clearing, and paraffin embedding). Paraffin blocks were sectioned at 4 to 5 μm thickness and mounted on slides. Immunohistochemical staining for olfactory marker protein was performed, with positive cells quantified under microscopy at appropriate magnification by trained pathologists.
OT&T Sniff Test
Testing was conducted in a well-ventilated, odor-neutral environment. The examiner held 1 end of odorant-impregnated test strips, dipped them in specific solutions, and presented them ~1 m anterior to the patient’s nasal vestibule for identification. Both detection threshold and recognition threshold were recorded. The OD could be divided into five levels based on the identification threshold, level I: ≤1.0 points, normal OD; level I: >1.0 to 2.5 points, mild decline in olfactory function; level M: >2.5 to 4.0 points, moderate decline in olfactory function; level W: >4.0 to 5.5 points, severe decline in olfactory function; level V: >5.5 points, olfactory loss.
Olfactory Visual Analog Scale Scores
In this study, the olfactory visual analog scale (OVAS) was employed to subjectively assess patient’s olfactory function. This scale consists of a 10 cm horizontal line with anchor descriptors at both ends: left end (0 points): labeled as “no olfactory problems whatsoever”; right end (10 points): labeled as “the most severe olfactory problems imaginable.” Patients were instructed to mark a point on the line based on their subjective perception of olfactory function during the preceding week, indicating the severity of their OD. The distance (in centimeters) from the left endpoint (0 point reference) to the marked position was recorded as the OVAS score (eg, a mark at 5 cm corresponds to 5 points). Higher scores reflect greater self-reported OD severity.
Statistical Treatment
SPSS25.0 (Armonk, New York, USA) statistical software was used to analyze the data, and the count data were expressed as (n) or (n [%]), with the χ2 test adopted for comparison between multiple groups. The measurement data that conformed to normal distribution were expressed as mean ± standard deviation, with the F value test applied for comparison between multiple groups. The measurement data that did not conform to normal distribution were expressed as the median and interquartile spacing (M [P25, P75]), with the Z test used for comparison between multiple groups. P < .05 was regarded as statistically significant. The occurrence of OD was taken as the dependent variable. Nasal cavity volume, Lund–Mackay CT score, Lund–Kennedy nasal endoscopy score, IL-5, IgE, and mucosal olfactory marker protein-positive cell count (STOMP) were taken as the independent variables, with Pearson correlation analysis adopted to analyze the correlation. Differential indicators were analyzed by multifactor Logistic regression analysis, with receiver operating characteristic (ROC) curves taken to analyze the predictive value of each factor.
Results
Comparison of General Information of Patients in Each Group
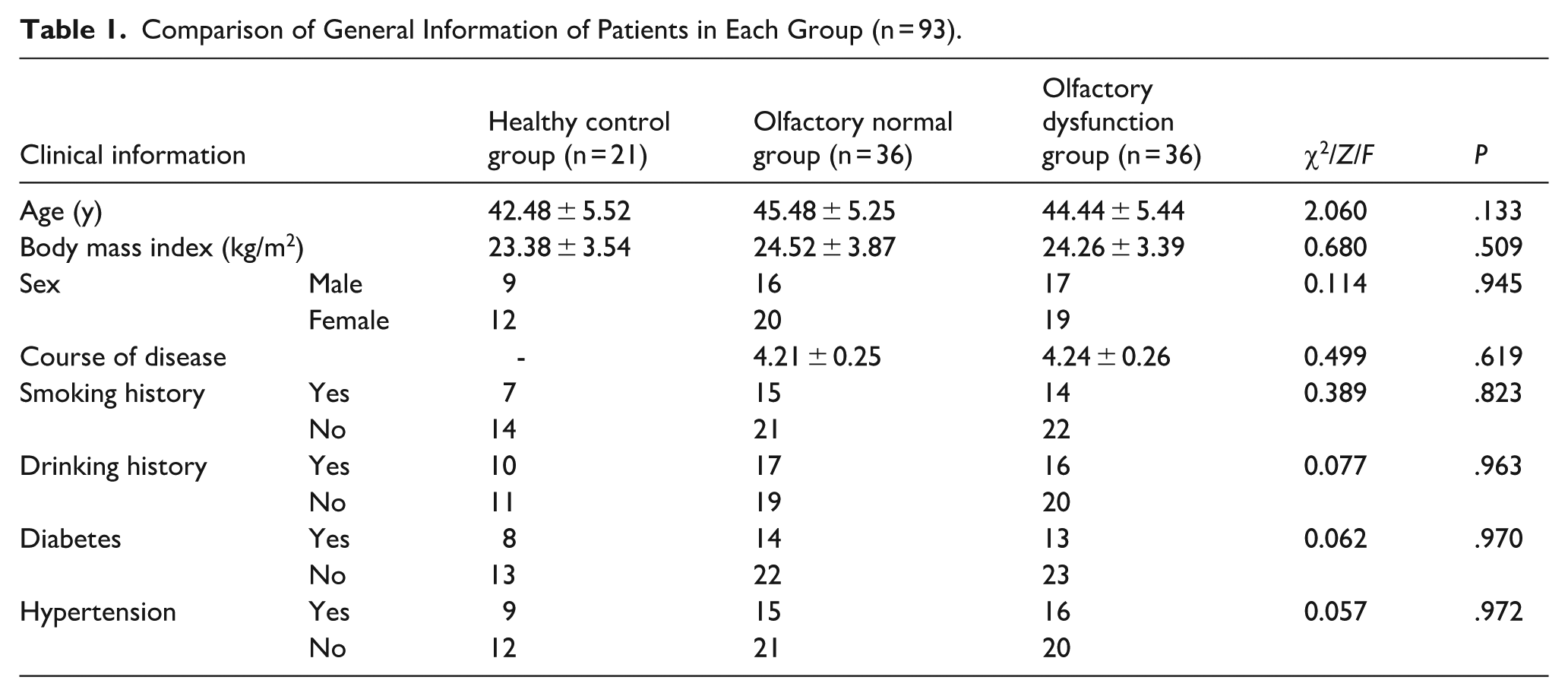
As shown in Table 1, a total of 93 subjects were included in this study. Comparing the general information of age, BMI, sex, course of disease, smoking history, drinking history, diabetes, hypertension in the 3 groups, the results were no statistically significant (all P > .05), suggesting that the groups were comparable.
Comparison of General Information of Patients in Each Group (n = 93).
Comparison of Olfactory Phenotypic Characteristics and Nasal Mucosa Condition of Patients in the 3 Groups
According to the olfactory function tests of the 3 CRSsNP patient groups presented in Table 2, the OD group demonstrated significantly lower nasal cavity volume and STOMP compared to both the healthy control group and the normosmic group. Conversely, this group showed significantly higher Lund-Mackay CT scores, Lund-Kennedy nasal endoscopy scores, IL-5 levels, IgE levels, detection thresholds, recognition thresholds, and OVAS scores than the healthy control groups (P < .05).
Comparison of Olfactory Phenotypic Characteristics and Nasal Mucosa Condition of Patients in the 3 Groups.
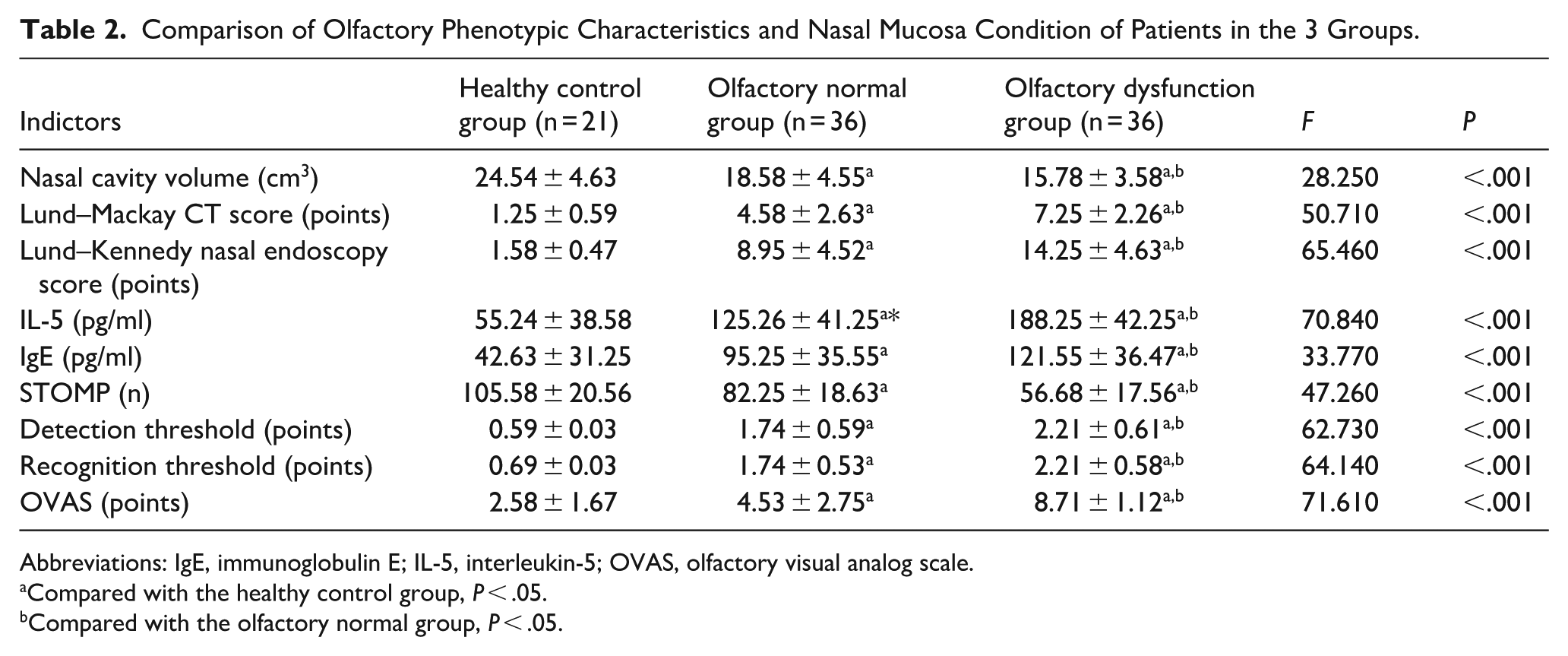
Abbreviations: IgE, immunoglobulin E; IL-5, interleukin-5; OVAS, olfactory visual analog scale.
Compared with the healthy control group, P < .05.
Compared with the olfactory normal group, P < .05.
Correlation Analysis of Olfactory Function Score, Nasal Mucosal Barrier Function, Inflammatory Indicators, and OD
As shown in Figure 1, the Pearson correlation model indicated that Lund–Mackay CT score, Lund–Kennedy nasal endoscopy score, IL-5, IgE, perception threshold, and recognition threshold were positively correlated with OD (r = 0.484, 0.507, 0.608, 0.347, 0.373, and 0.400, respectively, P < .05). Nasal cavity volume and STOMP were negatively correlated with OD (r = −0.328 and −0.582, P < .05).
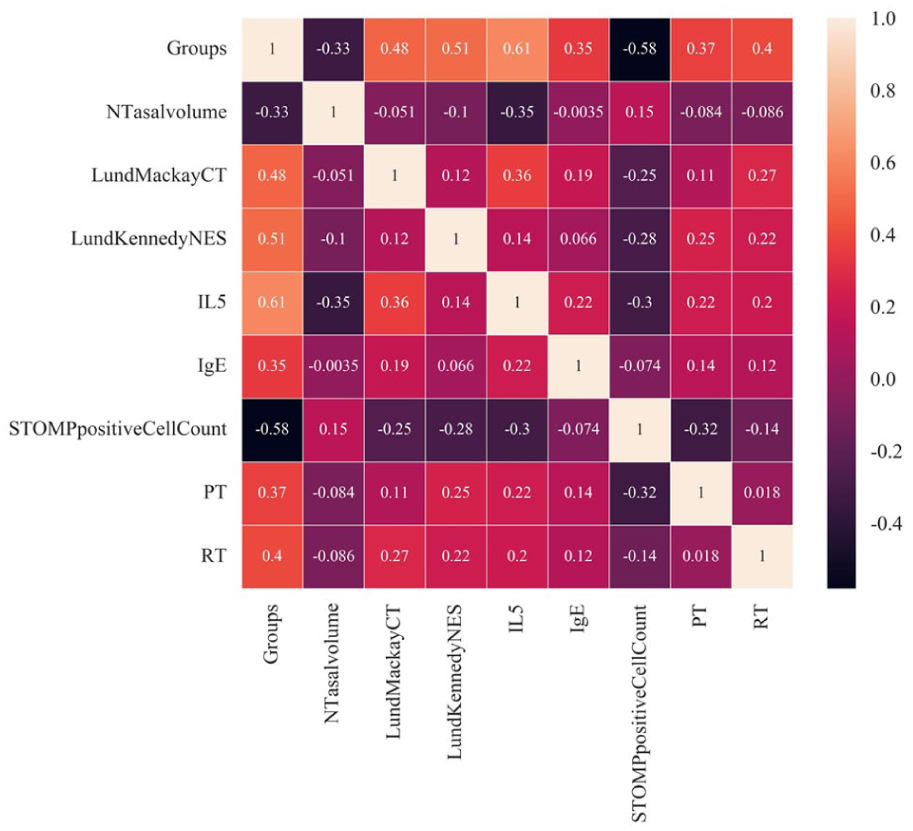
Correlation of nasal cavity volume, Lund–Mackay CT score, Lund–Kennedy nasal endoscopy score, IL-5, IgE, and STOMP between with olfactory dysfunction. IgE, immunoglobulin E; IL-5, interleukin-5.
Univariate and Multifactorial Logistic Regression Analysis Affecting OD
As presented in Table 3, a single factor analysis of nasal cavity volume, Lund–Mackay CT score, Lund–Kennedy nasal endoscopy score, IL-5, IgE, STOMP, detection threshold, and recognition threshold was performed sequentially by Logistic predictive modeling on the patients in the olfactory normal group and OD group. The single factor regression analysis expressed that nasal cavity volume (OR = 0.84, 95% CI = 0.75-0.96, P = .008), Lund–Mackay CT score (OR = 1.55, 95% CI = 1.23-1.95, P < .001), Lund–Kennedy nasal endoscopy score (OR = 1.32, 95% CI = 1.14-1.53, P < .001), IL-5 (OR = 1.04, 95% CI = 1.02-1.05, P < .001), IgE (OR = 1.02, 95% CI = 1.01-1.04, P = .005), STOMP (OR = 0.92, 95% CI = 0.88-0.96, P < .001), detection threshold (OR = 3.71, 95% CI = 1.57-8.77, P < .001), and recognition threshold (OR = 5.17, 95% CI = 1.82-14.65, P < .001) were independent risk factors for OD.
Univariate and Multifactorial Logistic Regression Analysis Affecting Olfactory Dysfunction.
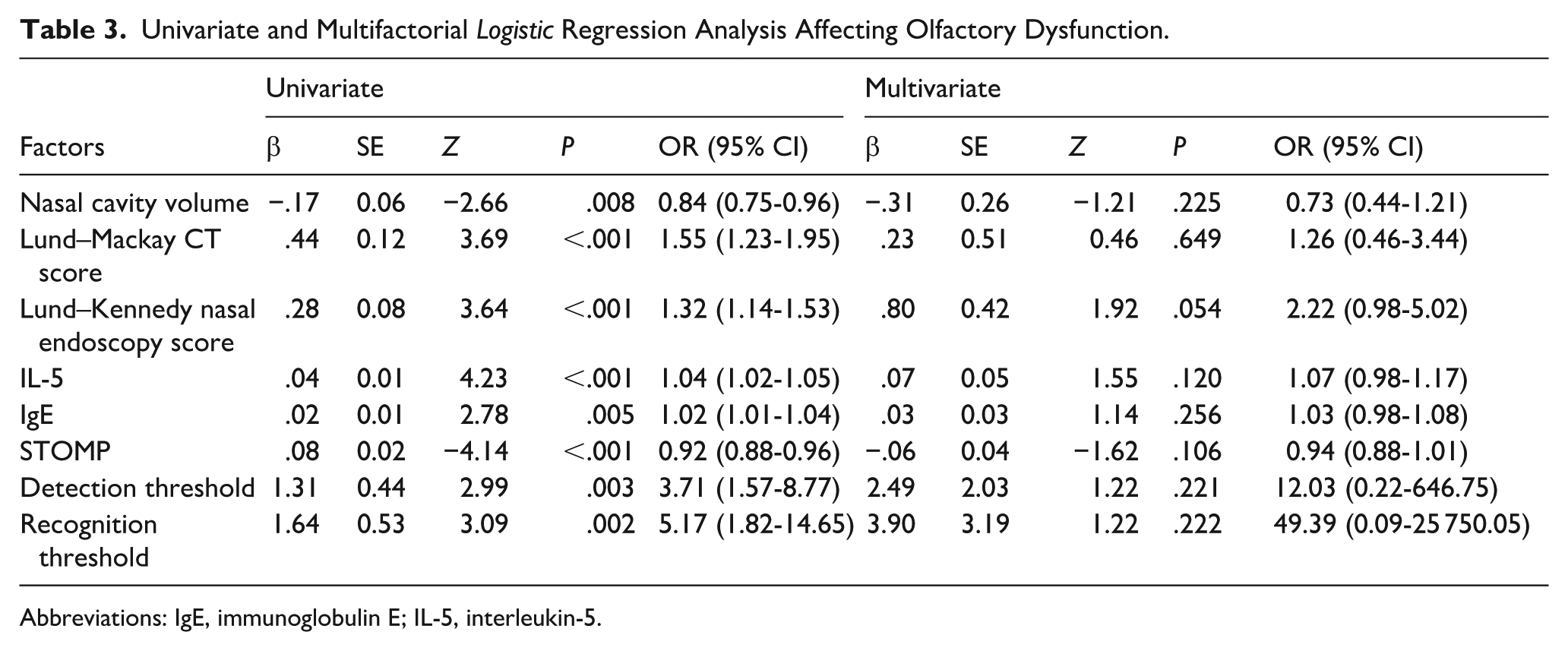
Abbreviations: IgE, immunoglobulin E; IL-5, interleukin-5.
ROC Analysis of Factors Predicting the Occurrence of OD
The ROC curves of patients in the olfactory normal and OD groups indicated that area under the curve (AUC) values of these indexes all >0.6, including nasal cavity volume (AUC = 0.693), Lund–Mackay CT score (AUC = 0.769), Lund–Kennedy nasal endoscopy score (AUC = 0.790), IL-5 (AUC = 0.877), IgE (AUC = 0.707), STOMP (AUC = 0.849), detection threshold (AUC = 0.715), and recognition threshold (AUC = 0.766), thus suggesting that each of the above indexes had a certain degree of predictive value for the occurrence of OD, more details in Figure 2.
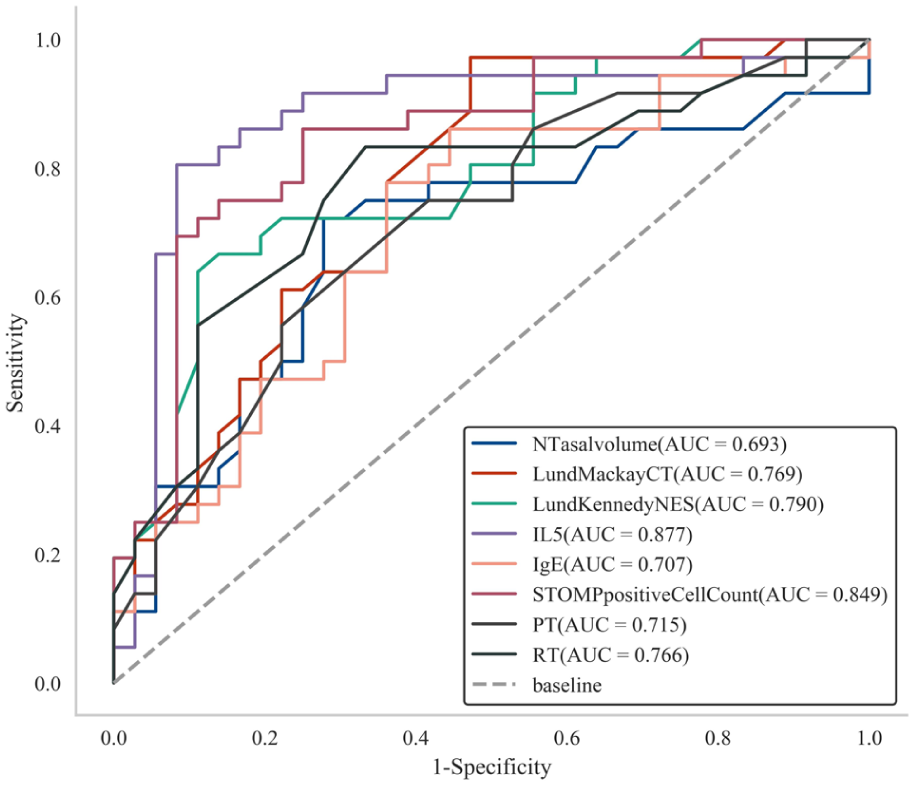
ROC of factors predicting secondary olfactory dysfunction in CRSsNP patients. CRSsNP, chronic rhinosinusitis without nasal polyps; ROC, receiver-operating characteristic.
Discussion
In patients with CRSsNP, the absence of polyps does not preclude the development of OD, which can be initiated by inflammatory processes within the nasal cavity. Previous research has demonstrated 15 that olfactory impairment adversely affects patients’ daily living through multiple mechanisms pathways, with olfactory alterations being associated with nasal structure of OD in CRSsNP. Early identification of contributing factors of CRSsNP could provide valuable guidance for optimizing subsequent clinical management strategies.
This study found that there was a strong correlation between nasal cavity volume and the occurrence of OD in patients with CRSsNP, as an independent influencing factor. Du et al 16 scholars found a significant correlation between nasal cavity volume and OD, further confirming the findings of this study. The reduction of nasal cavity volume can affect the transmission function of olfactory molecules in the nasal cavity, especially the inability of olfactory molecules to reach the olfactory epithelium. Under normal conditions, olfactory molecules are delivered to the olfactory epithelium via nasal airflow, a process, that is, critical to the normal olfactory function. However, when olfactory volume is restricted, olfactory molecules can directly reduce the efficiency of transmission and affect olfactory infection, thus increasing the risk of OD, so it is clinically believed that olfactory perception in CRS patients is usually closely linked to the ideal contractile capacity of the nasal mucosa. This study found that Lund–Mackay CT score was correlated with OD also as an independent risk factor. Ye et al 17 scholars found that higher Lund–Mackay CT scores indicated the presence of more severe OD in patients, which was one of the independent risk factors for poor olfactory prognosis, further confirming the findings of this study. The Lund–Mackay CT score is a scoring system typically used to assess the severity of sinus disease seen on CT imaging in patients with CRS. The score assists physicians in quantifying sinus inflammation specialties and provides targeted support for disease management and treatment outcomes. Related scholars have found 18 that moderate-to-severe sinus lesions (total score of 5 and above) are usually associated with remarkable OD, especially when significant lesions are present in multiple sinus regions (eg, maxillary and ethmoid sinuses), with a higher risk of olfactory loss. If the sinuses are infected and inflamed, especially the maxillary sinus and ethmoid sinus, the cavity is full of inflammatory secretions, which directly cause obstruction of nasal airflow, interfering with the normal entry and conduction of odor molecules, and the obstruction of nasal passages reduces the olfactory epithelial stimulation, thus affecting the olfactory perception. Therefore, improved Lund–Mackay CT scores are positively correlated with OD, and assessment of sinus lesions by CT imaging can provide clinicians with information of expectation in patients with OD. 19
This study found a strong association between the Lund–Kennedy nasal endoscopy score and OD. Mallick et al 20 scholars found certain correlation between Lund–Kennedy nasal endoscopy score and OD, which was consistent with the findings of this study. The Lund–Kennedy nasal endoscopy scoring system assists doctors in determining the degree of lesions on the sinuses and nasal cavity-related structures of patients, mainly through the results of nasal endoscopy. Moreover, doctors are able to assess in detail the inflammation in different areas, thus understanding the severity of the lesions and helping to determine treatment options. Several studies have declared21,22 that there is usually a correlation between higher Lund–Kennedy scores (ie, patients with more severe inflammation) and OD. Lesions of the nasal passages and maxillary sinuses of the nasal cavity, assessed in the Lund–Kennedy scoring system, are directly related to this obstruction, and the blockage of nasal passages restricts the entry of airborne volatile chemicals into the olfactory region, making the OD. Another scholarly study found 23 that lesions in areas with more severe inflammation, such as the middle nasal passage and maxillary sinus, might directly lead to the blockage of airflow, which in turn affected olfactory perception, as assessed by the Lund–Kennedy score. In this study, it was found that the IL-5 index has a correlation with olfactory function as one of the independent risk factors. Shin et al 24 scholars found that elevated levels of IL-5 in sinus tissue were significant in assessing early OD, which was consistent with the findings of this study. IL-5 can enhance chemokines and has a migratory activating effect on eosinophils. IL-5 is a cytokine secreted by T-cells and other immune cells, which are usually closely related to the growth, activation, and recruitment of eosinophils. In patients with CRS, elevated IL-5 indexes can lead to a large number of eosinophil aggregates, which can release a wide range of inflammatory mediators in the nasal cavity and sinuses, resulting in the exacerbation of local inflammation. Meanwhile, IL-5 directly affects OD by regulating the activation of eosinophils and prompting the cells to release inflammatory mediators such as leukotrienes and proteases, which cause local tissue damage and affect the olfactory epithelial structure and function. Another scholar’s study found 25 that IL-5 was not only involved in the recruitment of eosinophils but was also closely related to the activities of other immune cells. The elevation of this indicator might lead to the continuous activation of immune responses in nasal cavity, forming a vicious circle that exacerbated the inflammatory response and OD.
This study found that there was a strong association between IgE and OD. Seah et al 26 scholars found that elevated serum total IgE levels were identified as an independent risk factor for OD. IgE plays an important role in allergic reactions, usually in allergic diseases by binding to allergens, activating mast cells and basophils, and releasing inflammatory mediators such as histamine, leading to local inflammation and tissue damage. In patients with CRS, elevated IgE can exacerbate the allergic inflammatory response, triggering swelling of the nasal cavity and sinuses, resulting in increased secretions and mucosal damage, coupled with the fact that IgE promotes the release of a series of inflammatory mediators, such as histamine, leukotrienes, and cytokines through the activation of mast cells and basophils, which increases chronic inflammation in the nasal cavity and sinuses, jeopardizing the olfactory epithelium, thus leading to impaired olfactory function. 27 Another study found 28 that decreased function of the olfactory epithelium can cause damage, degeneration, and functional decline of the olfactory epithelium, triggering OD. In this study, it was found that the STOMP was correlated with OD as an independent risk factor. Chen et al 29 demonstrated that elevated STOMP levels negatively correlated with olfactory function, corroborating our results. The upper turbinate—a critical anatomical structure lined with olfactory epithelium—contains essential components for olfactory signal transduction (eg, olfactory receptors, adenylate cyclase). Increased STOMP suggests olfactory receptor cell proliferation and heightened activity. However, in CRS, mucosal edema and excessive secretions may obstruct molecules from reaching the olfactory cleft, impairing odor perception despite elevated olfactory marker protein-positive cell counts. 30 This study found that detection threshold and recognition threshold, as the independent risk factors, had certain correlation with OD. The perception threshold is the lowest concentration at which an individual can perceive the odor, below which an odor cannot be identified or detected by the individual. The level of the perception threshold reflects the sensitivity of the olfactory system of patients, with lower thresholds indicating that the patient is able to perceive odors at lower concentrations, and vice versa, indicating that there is a problem with the olfactory system. The recognition threshold is the lowest concentration at which the patient can recognize the type of odor. After detecting an odor, the patient needs a sufficient concentration to determine the nature of the odor, and a lower recognition threshold usually means that the patient can not only detect the odor but also recognize the type of odor; however, a higher recognition threshold suggests the presence of OD. The results of the Pearson correlation model constructed in this article indicated that nasal cavity volume, Lund–Mackay CT score, Lund–Kennedy nasal endoscopy score, IL-5, IgE, STOMP, detection threshold, and recognition threshold were strongly associated with the occurrence of OD in patients with CRSsNP. Through Logistic regression model analysis, it was found that all the above indicators were influential factors in the occurrence of OD in patients with CRSsNP, but P > .05 existed in multifactorial analysis. Multifactorial analysis considered the interrelationships of a number of factors, and there might be complex interactions between certain factors at different stages, which affected the significance of the results. It was possible that there was a certain amount of colinearity among some variables that affected the relationship between multifactors and OD. Meanwhile, small sample sizes might fail to detect smaller differences, resulting in higher P values and higher statistical efficacy in the results of multifactor analysis; thus, larger sample sizes were required.
However, this study has several limitations. First, the sample size was relatively small (36 patients with OD, 36 patients of normal olfaction, and 21 healthy controls) and recruited from a single center, which may affect the reliability and generalizability of the findings. Second, the observation period (April 2023-December 2024) was relatively short, whereas OD typically develops progressively over time, making it challenging to fully evaluate the influence of nasal mucosal barrier damage within this limited timeframe. Although we included nasal cavity volume, Lund–Mackay CT scores, Lund–Kennedy nasal endoscopy scores, IL-5, IgE, and STOMP as predictive variables, other potential factors associated with OD may have been overlooked. Additionally, the use of patient-reported OVAS as the primary olfactory outcome measure introduces 2 key limitations: (1) subjective scoring cannot distinguish between conductive olfactory impairment (eg, nasal obstruction preventing odorants from reaching the olfactory cleft) and sensorineural damage (eg, olfactory neuron apoptosis); (2) psychological state may influence scoring accuracy. These factors suggest that OVAS is better suited as a supplementary quality-of-life metric rather than an absolute measure of olfactory function. While OVAS remains a clinically practical symptom assessment tool, its results may be affected by patient mood, cognitive bias, and verbal expression differences. Future studies should incorporate psychophysical testing and olfactory-evoked potentials to differentiate between perceptual deficits and organic damage. Further improvements in sample size, study design, and long-term follow-up investigations are needed to enhance the accuracy and broader applicability of the findings.
In summary, nasal cavity volume, Lund–Mackay CT score, Lund–Kennedy nasal endoscopy score, IL-5, IgE, STOMP, detection threshold, and recognition threshold demonstrated significant associations with OD in patients with CRSsNP, each of which was identified as an independent influencing factor. The constructed ROC curves effectively facilitated the screening of olfactory impairment and early detection of abnormalities, thereby providing valuable references for optimizing subsequent clinical treatment strategies.
Footnotes
Ethical Considerations
This study was reviewed and approved by the Ethics Committee of Shanghai Xuhui Center Hospital.
Consent to Participate
Written informed consent was obtained from all participants, and all procedures followed the principles of the Declaration of Helsinki.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.