
Abstract
Objective:
This study aimed to analyze the efficacy of different doses and forms of corticosteroids in the treatment of postinfectious olfactory dysfunction and to specify the factors related to the curative effects.
Methods:
The medical records of patients diagnosed with postinfectious olfactory dysfunction from January 2018 to May 2019 were reviewed. All patients received different doses of oral corticosteroids for 12 days or inhaled corticosteroids for 1 month.
Results:
A review of the records of 43 patients showed that the mean follow-up time was 6.66 months, and the overall effective rate of treatment was 48.8%. Postinfectious olfactory dysfunction exhibited distinct seasonality, with the highest incidence in March. The curative effect was significantly related to the olfactory discrimination threshold at the first consultation (P = .022), but not significantly associated with age (P = .325), sex (P = .924), duration of disease (P = .526), follow-up time (P = .489), or treatment program (P = .330).
Conclusions:
Different doses and forms of corticosteroids showed no significant difference in the therapeutic effect on postinfectious olfactory dysfunction. The olfactory discrimination threshold at the first consultation was the most important factor influencing the prognosis.
Keywords
Introduction
As an important sensation of the human body, olfaction plays a key role in assisting identification, warning of danger, increasing appetite, and affecting emotions. Normal olfactory function allows people to instinctively chase delicious food and avoid food poisoning. Firefighters, laboratory workers, and other professionals can identify hazardous environments through olfaction. In addition, people enjoy the aroma of tea and mellow wine and different flavors of coffee through the sense of smell. Olfactory dysfunction seriously affects the quality of life, leading to loss of appetite and weight, as well as mental anxiety and depression. 1
Olfactory impairment is a common phenomenon. Large-scale global epidemiological surveys have shown that the incidence of olfactory disorders reaches 19% in Sweden (among patients older than 20 years), 22% in Germany (among patients aged 25-75 years), and 24% in the United States (among patients aged 53-97 years). 2 The most conservative estimates in Europe and America indicate that the incidence of olfactory disorders affecting life exceeds 5%. 3 Studies have shown that the most common causes of olfactory disorders are upper respiratory tract virus infections (18%-45%), nasal and sinus inflammatory diseases (7%-56%), head trauma (8%-20%), drugs or poisons exposure (2%-6%), and hereditary factors (0%-4%). 4 Among them, viral upper respiratory infection is one of the main causes of olfactory disturbance.
The treatment of postinfectious olfactory dysfunction is very limited. 3 At present, the most common therapy is olfactory training. 5,6 The application of other treatments, such as caroverine, zinc preparations, vitamin A, vitamin E, minocycline, and acupuncture, is controversial. 7 However, short-term systemic and/or topical steroid use may be an exception, as some studies have reported that corticosteroids are beneficial for postinfectious olfactory dysfunction. 8 -11 Treatment using systemic corticosteroids may involve the risks of metabolic disorders, gastrointestinal ulcers, elevated blood pressure, and the femoral head necrosis. Patients with underlying diseases are at greater risk. The best type and course of corticosteroid need to be further explored.
Previous studies demonstrated the effect of corticosteroid therapy but did not analyze in detail the effects of sex, age, degree of injury, treatment type, and other related factors on postinfectious olfactory dysfunction. 9,10,12 In this study, 43 patients were examined after a complete follow-up. The influence of various related factors on the curative effect was analyzed. Key influencing factors were explored in the hope of accurately evaluating the prognosis of olfactory disorders after corticosteroid use and guiding the treatment.
Methods
Patients with olfactory disorders admitted to the Second Affiliated hospital of Zhejiang University from January 2018 to May 2019 were included. Patients medical information, including sex, age, time of onset, degree of olfactory loss, manifestations (hyposmia, anosmia, olfactory intolerance, phantosmia, and parosmia), and possible causes (postinfectious olfactory dysfunction, rhinosinusitis, trauma, neurodegenerative disease, chemical exposure, etc), were collected. The sex development and family history were recorded if the patient was suspected of having a hereditary olfactory disorder.
All patients underwent nasal endoscopy and magnetic resonance imaging (MRI) of the olfactory pathway. Magnetic resonance imaging scanning was performed on a GE Sigma VHi Excite 3.0T scanner using the head quadrature coil. After the 3-plane positioning scan, coronary T1-weighted imaging (T1WI) and T2-weighted imaging (T2WI) were conducted perpendicular to the anterior cranial fossa. An inverted recovery sequence was used for T1WI. Then, the sagittal T2WI scan of the olfactory bulb (layer thickness 3 mm and spacing 0 mm) was obtained based on the 3-plane positioning image and the coronal image.
All participants had a clear history of upper respiratory tract infection. The olfactory disturbance did not improve at least 1 week after the symptoms such as nasal congestion and runny nose subsided. Nasal sinusitis and other lesions were excluded by physical and endoscopic examinations and imaging (sinus computed tomography and MRI). Other causes of olfactory disorders were ruled out, and the disorder was diagnosed with postinfectious olfactory dysfunction. The coronavirus disease 2019 (COVID-19) outbreak did not occur until the end of the study. Therefore, this study did not include patients with COVID-19.
All patients underwent a subjective olfactory test at the first visit and after the last treatment. The olfactory detection threshold and the recognition threshold were determined using the T&T olfactory meter (Japan’s First Drug Industry Co., Ltd). This instrument was commonly used for patients having smell disorders in Asia, and the results were correlated well with the University of Pennsylvania Smell Identification Test. 13 The test was carried out following the instructions on the olfactory meter, and the average recognition threshold of 5 olfactory elements was calculated to determine the degree of olfactory loss. Olfactory function was assessed according to the following scoring criteria: normal (<1.0), mildly decreased (1.1 ≤ 2.5), moderately decreased (2.6 ≤ 4.0), severely decreased (4.1 ≤ 5.5), and complete loss (>5.5). All patients were asked to close their eyes during the test to reduce the learning effect of repeated testing.
The patients were treated with 3 regimens: (1) oral methylprednisolone, 40 mg for 3 days, 20 mg for 3 days, and 8 mg for 6 days; (2) oral methylprednisolone, 20 mg for 3 days, 10 mg for 3 days, and 4 mg for 6 days; and (3) inhaled budesonide atomization suspension (AstraZeneca Trading Co., Ltd), atomized with an air compression nebulizer, for 4 weeks, 2 mg in the first 2 weeks and reduced to 1 mg in the last 2 weeks. At the same time, as proposed by Hummel et al, all patients received olfactory training for 12 weeks. 3
A repeated T&T subjective olfactory test was performed after the treatment. The curative effect was evaluated according to the comparison of the average T&T recognition threshold before and after the treatment. Normal posttreatment threshold was defined as cured; posttreatment threshold decreased by 1 point was defined as improved; posttreatment threshold decreased by 2 points or more, which did not reach the normal range, was defined as significantly improved; and posttreatment threshold decreased less than 1 point, with or without falling, was defined as invalid. Patients were followed up in the outpatient clinic every 4 weeks to observe and record any adverse reactions during the treatment period.
SAS 9.4 software was used for statistical analysis. The treatment plan was divided into 3 groups, and the dependent variable was a disordered categorical variable. Numerical variables with normal distribution were expressed as mean ± standard deviation, and analysis of variance was used for the comparisons. Non-normally distributed numerical variables were expressed as median (interquartile range), and a rank-sum test with a completely random design was used for multisample comparison. Categorical variables were described using the R × C contingency table, and χ2 and Fisher exact probability tests were used for statistical analysis. The α level of the statistical test was set to .05.
Results
A total of 43 patients completed treatments and follow-ups, including 31 (72.1%) female and 12 (27.9%) male patients. Patients had an average age of 46.44 ± 12.98 years (21-72 years), and an average disease duration of 6.87 months (0.1-48 months). The mean follow-up time was 6.66 (1-18) months. There was a lack of olfactory perception (≥5.6) in 24 patients, 7 had mildly decreased smell (1.1-2.5), 6 had moderately decreased smell (2.6-4.0), and 6 had severely decreased sense of smell (4.1-5.5). Further, 1 patient developed olfactory intolerance, 1 had parosmia, and 2 had phantosmia (all tastes were irritating). The overall effective rate was 48.9% (21/43 patients). Significant improvements were seen in 7 (16.3%) patients after the treatment, and 14 (32.6%) cases improved to a certain degree. In addition, the treatment was ineffective in 22 (51.1%) patients, among which 3 (7.0%) cases showed a temporary improve in olfactory sensation. Post-viral olfactory dysfunction exhibited obvious seasonal variation, with the highest incidence in March, followed by February and January (Figure 1).
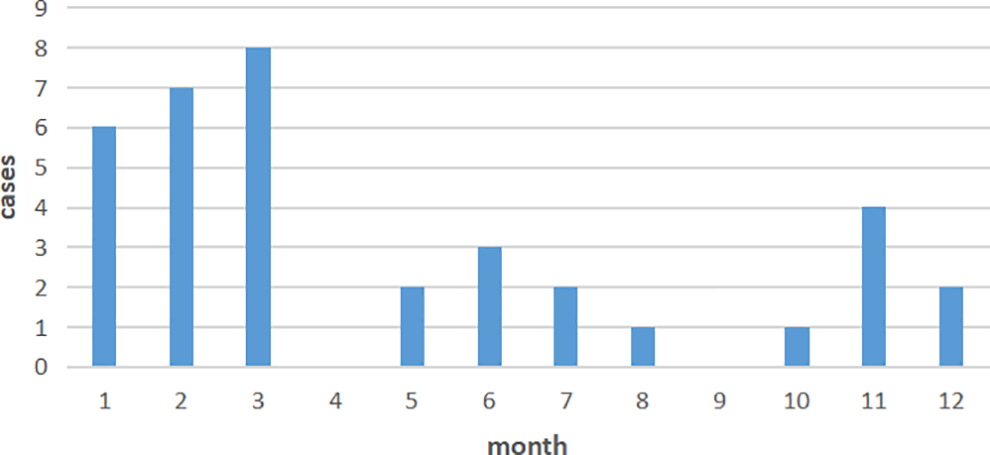
Seasonal incidence of postinfectious olfactory dysfunction.
The demographic data of 3 different treatment groups were compared. No significant differences were found in terms of disease onset age, duration of disease, and follow-up time. Notably, more female and anosmia patients were assigned to group 1. The effective rate of 3 treatment regimens was also compared. Still, no significant difference was found, as shown in Table 1.
Comparison of Clinical Characteristics of 3 Different Treatment Regimen Groups.a
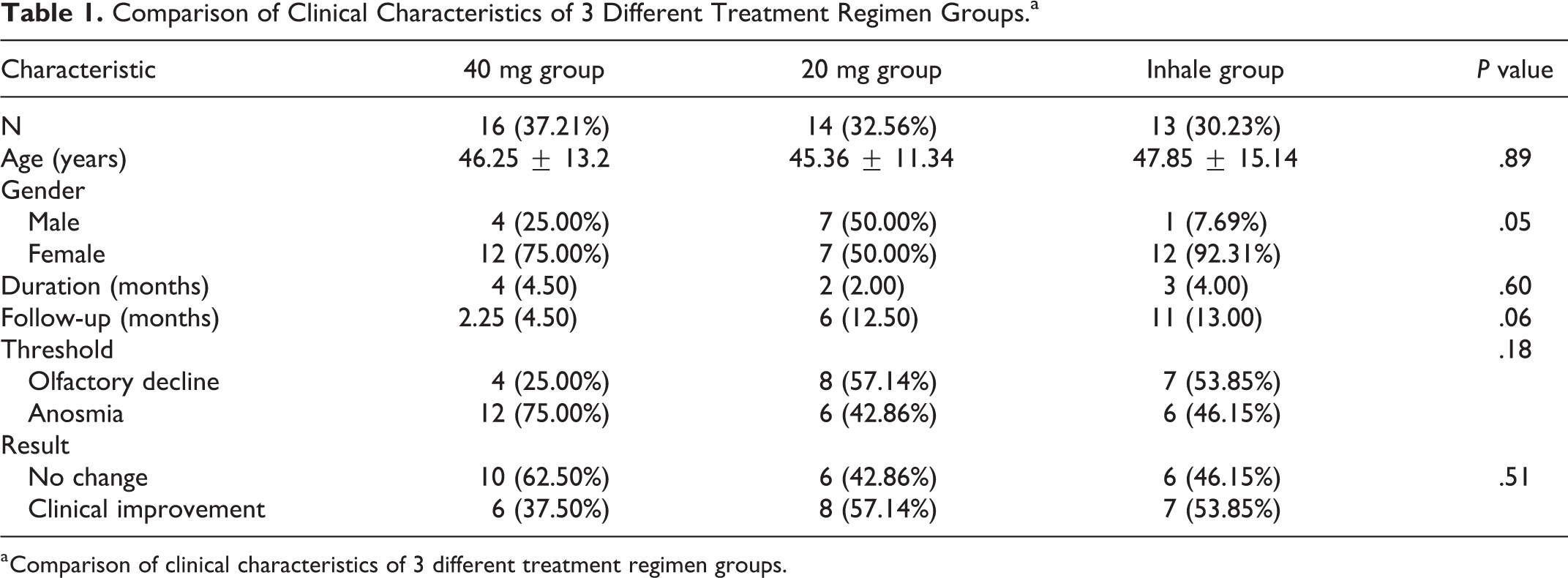
a Comparison of clinical characteristics of 3 different treatment regimen groups.
There was no significant difference in disease onset age, duration of disease, follow-up time, sex, and treatment program when comparing the effective with the ineffective treatment group (Table 2). Regarding the threshold of olfactory discrimination at the first consultation, 24 patients experienced complete olfactory dysfunction, and the treatment was effective in 8 (33.3%) patients. Moreover, 19 cases had incomplete olfactory dysfunction, and the treatment was effective in 13 patients (68.4%; P < .05, Table 2).
Comparison of Clinical Characteristics Between the Effective and Ineffective Treatment Group.a
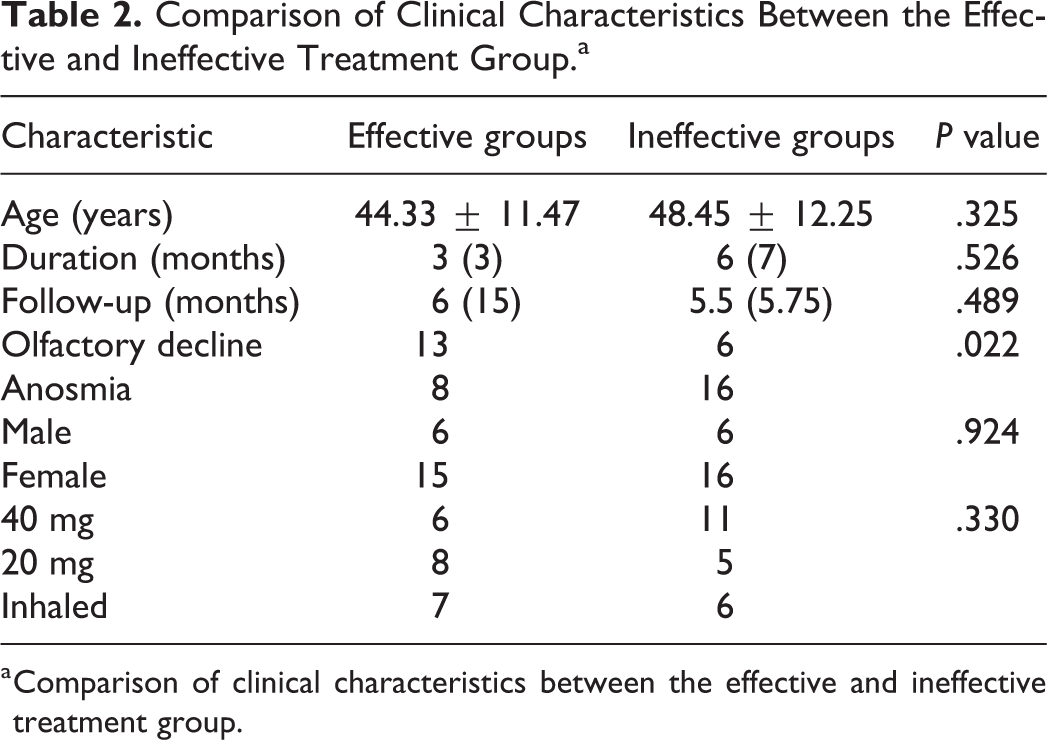
a Comparison of clinical characteristics between the effective and ineffective treatment group.
One patient had facial flushing, 1 had headache, 1 had a poor appetite, 1 had knee pain, and 1 had a dry nasal cavity. All cases showed improvements after discontinuing the drug.
Discussion
This study involved 43 patients with postinfectious olfactory impairment, accounting for about one-fifth of all patients with olfactory disorders during the same period, second only to patients with inflammatory diseases. The findings suggested that infection was an important cause of olfactory disorders. Literature reports have suggested that the incidence of postinfectious olfactory dysfunction is seasonal. Konstantinidis et al reported that postinfectious olfactory dysfunction exhibited seasonality with a peak in March, and the possible pathogenic factors were influenza and parainfluenza viruses (type III). 14 The current study also found that the incidence was highest in March, followed by February and January, which might be related to the low temperature in Hangzhou and the prevalence of upper respiratory tract infections in these 3 months.
The male-to-female ratio in terms of prevalence was 1.0:2.6, suggesting that the female olfactory system was more susceptible to upper respiratory tract infections, which was consistent with other reports. Tian et al reported that the male-to-female prevalence ratio was 1.0:2.3 in 141 patients with olfactory disorders following upper respiratory tract infection. 15 In this study, about half of the patients who lost olfactory sensation had a history of upper respiratory tract infection, indicating that the upper respiratory tract virus exerted a more serious impact on the olfactory system. The average duration of the study was 6.87 months, probably because the onset of olfactory disorders was not obvious. Some patients did not notice the onset of the disease, and only realized olfactory disturbance after encountering a strong smell for a long time. Few doctors carried out the diagnosis and treatment of olfactory disorders. Some patients in this study were referred multiple times, which prolonged the consultation time. The average follow-up time in this study was 6.66 months. Short-term follow-up might confuse accurate treatment effects, whereas a mean follow-up of more than 1 year might result in a high loss rate in China.
The effective rate in this study was slightly lower than that in other studies, which might be related to the higher proportion of olfactory loss in this study. Cavazzana et al reported an average of 1.94 years of follow-up for 791 patients with postinfectious olfactory disorders. They found that age, odor threshold, odor discrimination, and odor identification score at the first visit were significant predictors of the extent of change. The percentage of patients with anosmia and hyposmia who exhibited clinically significant improvement was 46% and 35%, respectively. 16 Dai et al reported that hyposmia patients had a higher recovery rate than patients with anosmia. 17
Whether the dose or form of corticosteroid influences the treatment effect is still controversial. In this study, no difference among 3 treatment groups was found, indicating that different dosages and formulations had no effect on the recovery rate of postinfectious olfactory dysfunction. The small sample size of this study might affect the results, highlighting the need for large sample data to support the findings. However, if this conclusion held true, low-dose oral corticosteroid or inhaled corticosteroid therapy could be considered for patients with an olfactory loss to avoid the side effects of large doses despite the small benefits. Only 3 patients had obvious discomfort after oral corticosteroid administration in this study, which was relieved after reducing the dose. It has been suggested that the side effects of corticosteroid therapy are controllable if low doses are used.
The statistical analysis found that the efficacy was not linked with disease onset age, duration of disease, follow-up time, sex, and treatment plan, but closely related to the threshold of olfactory discrimination at the first consultation. The olfactory disorder is an abnormal neurological change. Persons with olfactory loss have more nerve damage, and the effect of corticosteroid therapy is poor. This is similar to sudden deafness. The difference is that the course of disease has nothing to do with the treatment effect, which cannot be explained at present. One possibility is that olfactory epithelial and nerve cells have a strong regeneration capacity and a great recovery potential and are less influenced by time.
One limitation of this study was the lack of a strict control group, which made it difficult to explain whether the patient’s recovery was spontaneous or the result of treatment. However, in China, it was difficult to do this if patients did not receive any medication but were required to be followed up regularly. After analyzing the patient’s data, it was found that the average disease duration was 6.87 months. Twenty-four (55.8%) patients still lost their sense of smell completely, and other patients had no obvious spontaneous improvement in recent follow-ups, indicating that the patient’s olfaction had entered a plateau. The later improvement was more likely to be the effect of treatment. Another limitation was the small sample size of this study. The study had a large heterogeneity with regard to the follow-up time in different groups. Although the thresholds of the 3 groups were not statistically different, the proportion of patients with anosmia in the methylprednisolone 40 mg group was higher than that in the other 2 groups, which affected the analysis of the results. Hence, the causality could not be determined.
Despite the aforementioned shortcomings, it was one of the few studies in the field investigating the effect of steroids and showing that oral steroids were not superior to topical steroids when looking for recovery. Since the COVID-19 pandemic, many controversial issues have been reported on the use of steroids. The latest research has shown that the olfactory dysfunction of patients with COVID-19 has a high rate of self-healing, but the evidence supporting systemic steroid treatment of olfactory dysfunction caused by COVID-19 is lacking. 18,19 Although this study did not include patients with COVID-19, the group of cases comprised of patients infected with the virus. The conclusions of this study may also suit patients with COVID-19 and olfactory dysfunction, and we should not ignore the side effects of steroids, even for short courses.
Conclusions
The dosage and formulation of corticosteroid did not significantly affect its therapeutic effects on postinfectious olfactory dysfunction. The threshold of olfactory discrimination at the first consultation was the most important factor influencing the prognosis.
Supplemental Material
Supplemental Material, sj-pdf-1-ear-10.1177_01455613211040368 - Treatment of Postinfectious Olfactory Dysfunction Using Corticosteroids
Supplemental Material, sj-pdf-1-ear-10.1177_01455613211040368 for Treatment of Postinfectious Olfactory Dysfunction Using Corticosteroids by Hong-Gang Duan, Fang Ji and Mao-Xiao Yan in Ear, Nose & Throat Journal
Supplemental Material
Supplemental Material, sj-pdf-2-ear-10.1177_01455613211040368 - Treatment of Postinfectious Olfactory Dysfunction Using Corticosteroids
Supplemental Material, sj-pdf-2-ear-10.1177_01455613211040368 for Treatment of Postinfectious Olfactory Dysfunction Using Corticosteroids by Hong-Gang Duan, Fang Ji and Mao-Xiao Yan in Ear, Nose & Throat Journal
Footnotes
Authors’ Note
All procedures performed in studies were in accordance with the ethical standards of the institution or practice at which the studies were conducted (Ethics Committee of 2nd Affiliated Hospital, College of Medicine, Zhejiang University, 2020-215). Informed consent was obtained from all individual participants included in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the grant from the Zhejiang Provincial Natural Science Foundation of China(No.LY18H160006).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.