
Abstract
Endoscopic examination of the nasal cavity is an integral part of the assessment of patients with chronic rhinosinusitis. However, the benefit gained by performing endoscopy with respect to the patient’s medical condition has not been completely assessed. We conducted a prospective cohort in an academic medical center. Thirty-nine patients diagnosed with chronic rhinosinusitis, without polyps, whose ailment was managed conservatively with no surgical intervention. All patients underwent nasal endoscopy, a computed tomography (CT) scan rated for Lund-MacKay score, and completed a sino nasal outcome test (SNOT)-20 questionnaire. This same evaluation was repeated 6 weeks following medical treatment. The CT scan and SNOT-20 questionnaire were independent parameters to evaluate the endoscopy score in each nasal passage. Thirty-nine (28 females) patients completed the follow-up period. A total of 156 endoscopic evaluations were performed, in which 74 nasal cavities were found to have significant pathology and 82 were either normal or displayed mild pathology. The correlation with the Lund-MacKay score was poor with a positive predictive value of 68.9% (31.1% false positive and 28% false negative). However, while looking at the SNOT-20 score, corrected for repeated measures, a higher endoscopy score was associated with a higher SNOT-20 score (odds ratio = 3.53, 95% confidence interval = 1.54-8.09, P = .003). Patients with higher endoscopy scores had a greater probability for exhibiting severe symptoms. However, we could not demonstrate a strong correlation between nasal endoscopy findings and CT scan scores. Therefore, with respect to patients with chronic rhinosinusitis without polyps, nasal endoscopy could be utilized as a beneficial objective tool.
Introduction
Chronic rhinosinusitis (CRS) is a frequent cause of otolaryngology clinic visits. 1 Its economic burden in the United States alone is enormous and estimated to be ∼$22 billion a year. 2 Patients’ complaints are focused mostly on nasal congestion, facial pain, cough, and overall decline in their life quality. 3 Patients’ evaluation is based on history, physical examination, and imaging. Nasal endoscopy is one aspect of the sinonasal assessment during the clinic visit and preoperative evaluation; however, its role and necessity have not been completely verified, especially when the patient has no polyps. In a systematic review done by Wuister et al, computed tomography (CT) scan was suggested to be unnecessary for diagnostic purposes in case of positive findings using nasal endoscopy; however, negative endoscopy findings were not able to rule out CRS. 4 Therefore, the aim of this study was to evaluate nasal endoscopy as a diagnostic tool in CRS without nasal polyps (CRSsNP).
Patients and Methods
Ethical Considerations
The local institutional review board approved the study. The trial was registered at the clinical trials website (NCT00335309). Informed consent was obtained from all individual participants included in the study.
Design
The study was designed as a prospective cohort. We enrolled patients 18 to 80 years of age who were diagnosed clinically with CRSsNP, and confirmed by CT scan, and presented to our medical center. We excluded patients with previous sinonasal intervention or trauma, patients who were found to have polyps on physical examination, those who were suspected of having rhinosinusitis of dental origin, and immune suppressed patients as well as patients who had been treated for possible sinusitis prior to their evaluation. Patients allergic to penicillin were excluded as well as all patients were administered the same penicillin-based treatment.
Procedures
After signing an informed consent form, each patient underwent a thorough nasal endoscopic evaluation by a single rhinologist (T.M.), after which a validated Hebrew version SNOT-20 5 form was completed and a sinus CT scan was performed. Patients with cultures of bacteria resistant to Augmentin were excluded as well as patients with atopic disease background. A unified treatment protocol was applied to all patients of regular dose Augmentin for 14 days. Nasal decongestants (oxymetazoline 0.1%) were given for 4 days, with nasal steroids (fluticasone propionate 50 μg) for an additional 6 weeks. Six weeks later, each patient attended a follow-up visit, which included repeated evaluations.
In order to correlate the SNOT-20 score with the endoscopy score, we created a model in which the total SNOT-20 score was the dependent variable (low SNOT-20 score ≤40 and high SNOT-20 score ≥40) and the endoscopy score was the independent variable. In this model, we took into consideration the affected side only, since we speculated that the affected side would be the reason for the subjective effect on the patient.
Nasal Endoscopy Score
Based on the Lund-Kennedy endoscopic staging system, 6 each patient underwent a nasal endoscopic evaluation upon enrollment and, once again, 6 weeks following treatment. The endoscopic score was based on the sum of 2 parameters, nasal discharge and mucosal status. Normal nasal discharge was scored 0, clear discharge was scored 1, and pus was scored 2. Normal-looking mucosa was scored 0, hypertrophy without erythema was scored 1, and hypertrophy with erythema was scored 2. The score range was 0 to 4, whereby a score of 0 points was best and 4 points reflected a poor nasal endoscopic status.
Computed Tomography Scan Score
Each patient’s baseline and follow-up CT scans were evaluated and scored according to the Lund-MacKay scoring system 7 by 2 independent rhinologists (N.U., R.C.K.). The scoring results were tested for agreement and scan scores with substantial disagreement were discussed to finalize the correct score. Eventually, the mean Lund MacKay score was calculated for each patient. In order to simplify our measurements, we divided the CT scan Lund-MacKay score into better (0-4) and worse (5-24) versus the endoscopy score, better (0-1) and worse (2-4).
Statistical Analysis
Statistical analysis was conducted using SPSS version 18 software and SAS version 9.2. First, we considered the CT scan as the reference standard followed by the SNOT-20 results. Each nasal cavity’s endoscopic examination was measured independently, for each nasal passage, on baseline and follow-up examinations. The continuous variables were presented by mean and standard deviation. The categorical variables were presented in percentages. Chi-square test was used for the categorical variables and an independent t test for the continuous variables. Repeated-measures analysis was used to determine whether any change occurred in SNOT scores over time (pre, post, and late post) and between groups. Comparisons between each 2 time points were made using paired t test with Bonferroni correction. The mixed linear model was used to examine whether a difference exists in the mean CT scan score values between the 2 time points (pre and post) while controlling for repeated measures. The generalized estimating equation method (SAS procedure GENMOD) was used to ascertain endoscopy change and CT scan score over time, controlling for repeated measures. A P value <.05 was considered statistically significant.
Results
Patient Demographics
Thirty-nine (72% females) patients were enrolled and completed the follow-up period of 6 weeks. Demographics, symptoms and signs, endoscopic score, SNOT-20, and CT scan scores are outlined in Table 1.
Patient Demographics, Symptoms and Signs, Endoscopic Score, SNOT-20 Score, and CT Scan Score.
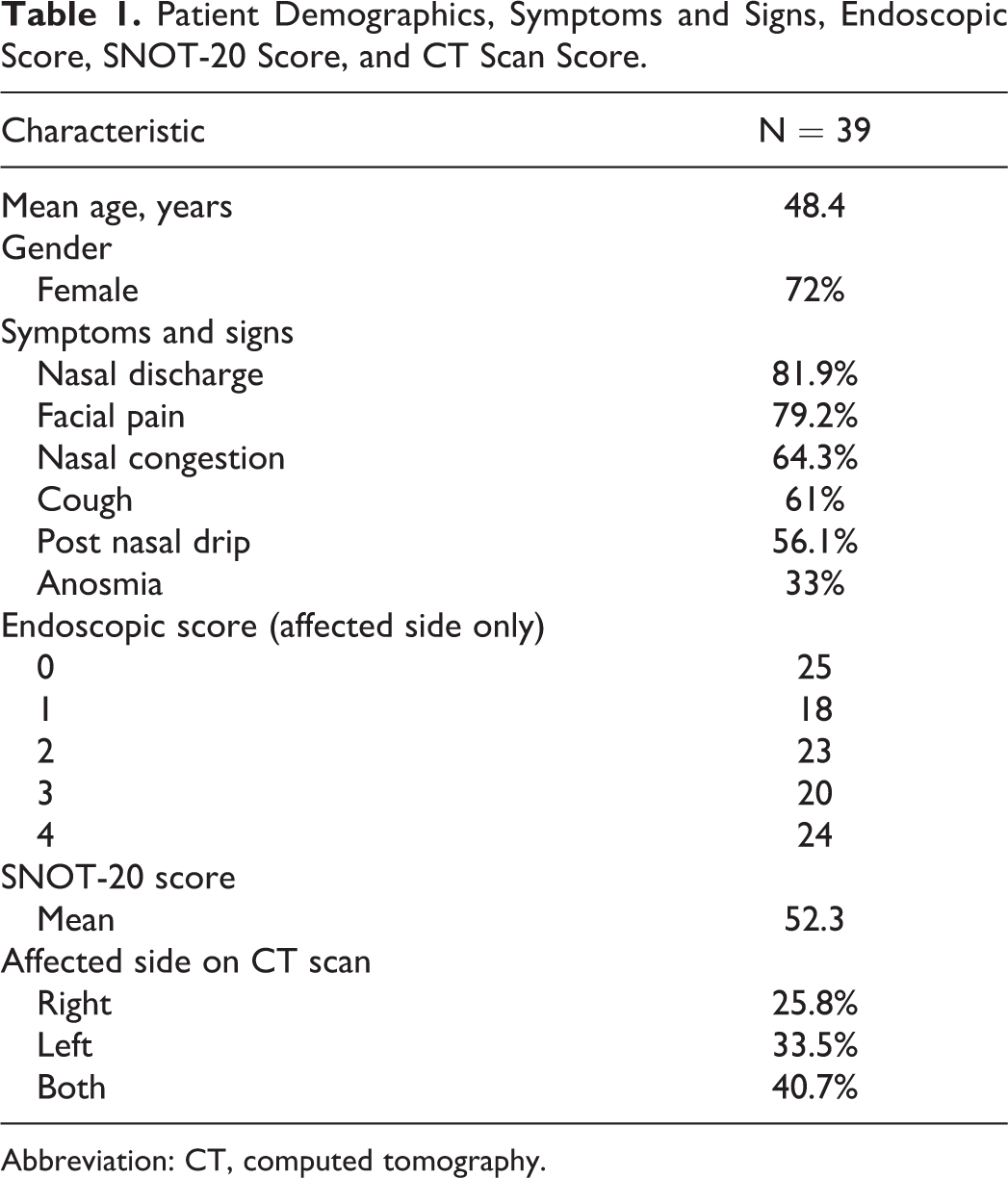
Abbreviation: CT, computed tomography.
Computed Tomography
In order to find the sensitivity, specificity, and positive predictive value of the nasal endoscopy score versus the CT scan score as a reference, we divided these parameters into 2 groups, better and worse (Table 2). The positive predictive value was 68.9% with false positive of 31.1% and false negative of 28%. Using the GENMOD procedure, we found an intercept equal to −1.22 (95% confidence interval [CI]: −1.5 to −0.91), showing no statistically significant agreement of the CT score and the endoscopy score results.
Computed Tomography Scan Lund-MacKay Score Versus Endoscopy Score.
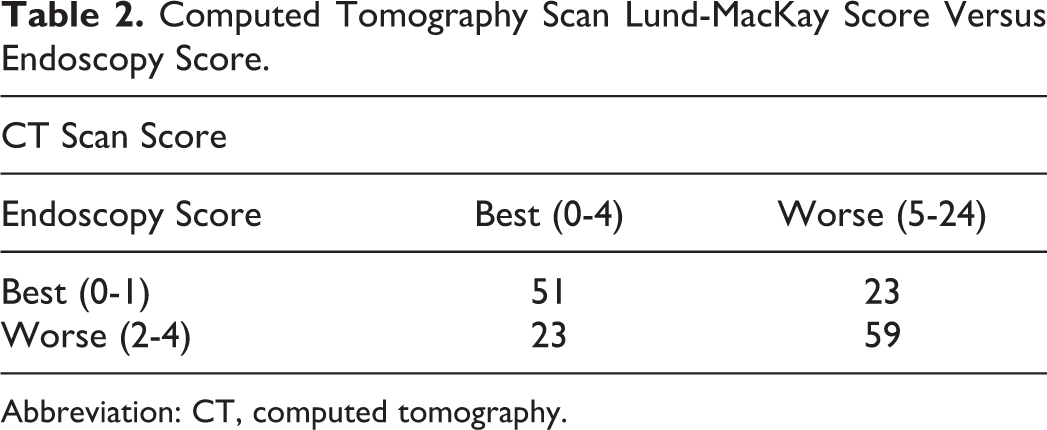
Abbreviation: CT, computed tomography.
SNOT-20
In order to look for a correlation between the nasal endoscopy and the SNOT-20 score, the affected sides were considered (Figure 1). In patients with both sinonasal cavities involved, we calculated an average score of both sides. The correlation was found to be statistically significant (P < .0001). Figure 2 represents the SNOT-20 score dependent on the endoscopy severity score; in other words, the worse the endoscopy score, the worse the individual patient’s life quality. The group that displayed a total score of 1 on the nasal endoscopy (18 nasal passages; odds ratio [OR] = 1.46, 95% CI: 0.39-5.4) did not correlate with its SNOT-20 score. However, for the higher nasal endoscopy score groups, the results were significant: score of 2 group (23 nasal passages), OR = 3.01, 95% CI: 1.35 to 6.72, score of 3 group (20 nasal passages), OR = 3.09, 95% CI: 1.23 to 7.77, and score of 4 group (24 nasal passages), OR = 3.53, 95% CI: 1.54 to 8.09.
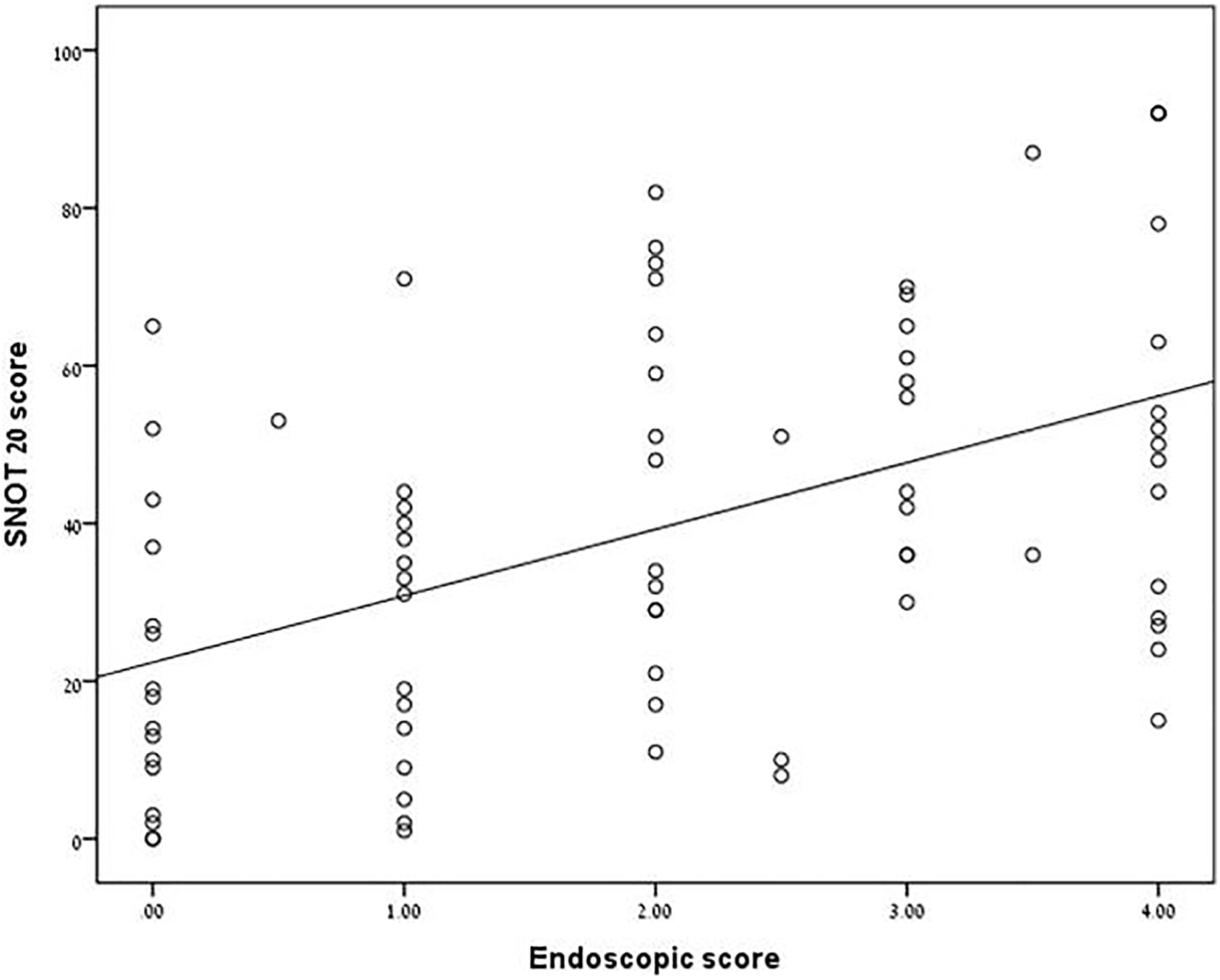
Correlation between nasal endoscopy score and SNOT-20 score. We used the Pearson correlation coefficient, r = 0.47, N = 78 (before and after treatment), P < .0001.
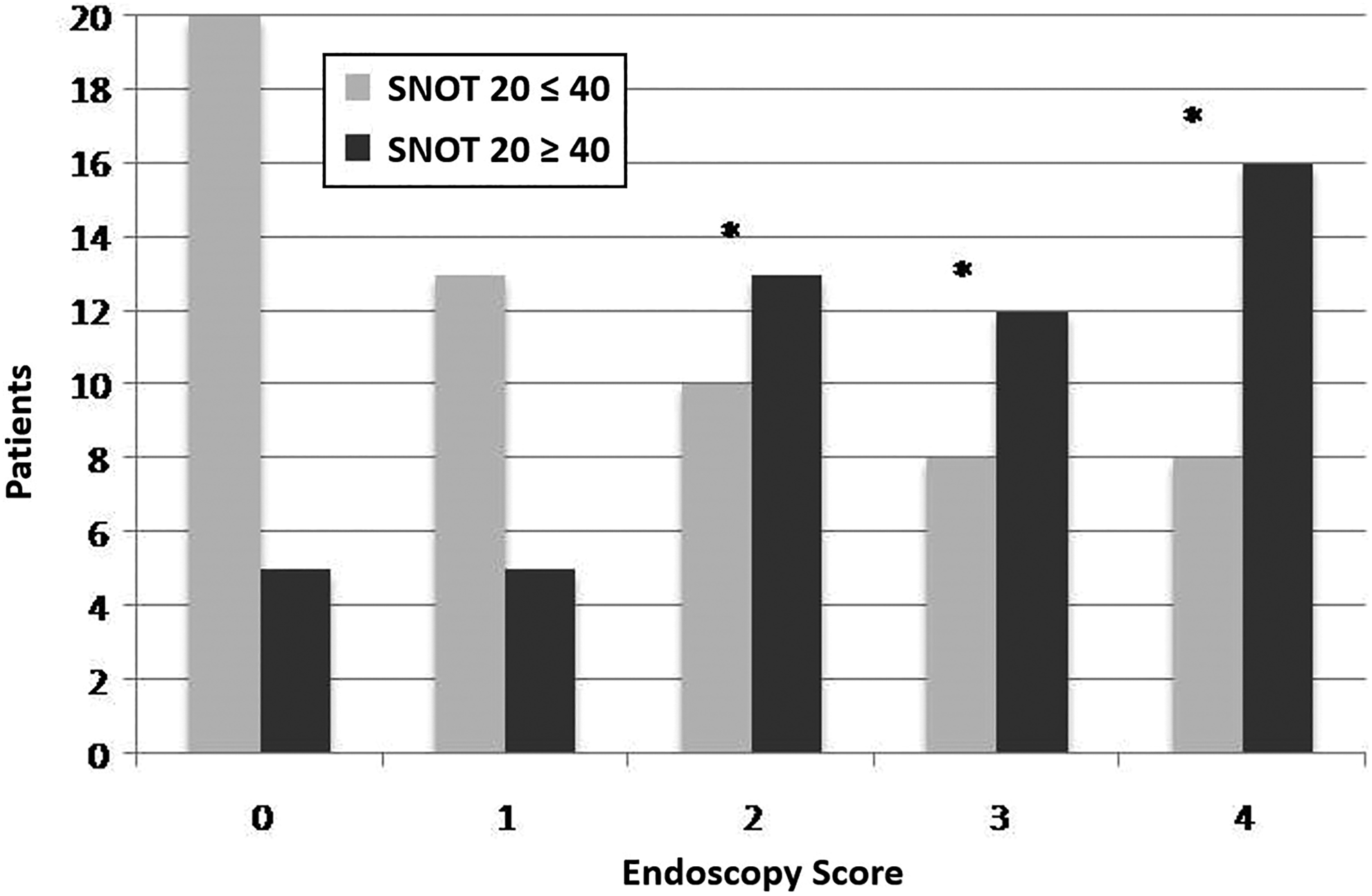
SNOT-20 score dependent on endoscopy score severity. SNOT = SNOT-20. *Statistical significance.
Looking at SNOT-20 as the dependent parameter and CT scan as the independent one, we found a strong correlation in the higher Lund-MacKay score: 5 to 9 score, OR = 2.25, 95% CI: 1.35 to 3.75, P = .002, 10 to 24 score, OR = 2.52, 95% CI: 1.40 to 4.57, P = .002.
Discussion
Nasal endoscopy is an inseparable part of the clinical assessment of patients with CRS. In this prospective study, focusing selectively on patients with CRSsNP, we were able to show a strong correlation of nasal endoscopy findings with patients’ subjective parameters presented here using the SNOT-20 quality-of-life questionnaire. This association between physical examination findings and patients’ well-being is stronger than its association with CT scores.
Diagnosis of CRS is based on both subjective and objective measures including endoscopic findings and CT scan. 8 Anosmia is considered to be a reliable predictor for CRS diagnosis, even in the absence of polyps. 9 Computed tomography scan is considered the gold standard, with respect to the diagnosis of CRS, and is the most common investigative tool in CRS assessment. 10 However, utilizing CT to confirm the diagnosis of CRS might be misleading at times as well. Several studies failed to show a valid correlation between CRS symptoms and severity on the basis of CT scores. 11 –13 Specifically, a weak correlation was found between quality-of-life questionnaires, including the SNOT-20, and CT-scan in patients with CRSsNP. 14 Agius and Stankiewicz et al, however, showed that patients subjectively diagnosed with CRS exhibited a strong correlation with CT scan findings. 15,16
Nasal endoscopy has an added value over anterior rhinoscopy. Adding nasal endoscopy was found to improve CRS diagnosis in patients presenting with the adequate criteria, whether or not they had nasal polyps, improving the odds from 1.1 to 4.6. 17 In this study, we were able to show that nasal endoscopy in patients with CRSsNP correlates well with the subjective assessment while leaving the CT scan as an ancillary investigation, especially when findings are positive with respect to nasal mucosal status and the presence of pus. In a study of 125 patients with CRS, endoscopy was able to confirm the diagnosis but could not, in the inverse situation, rule it out; the specificity of endoscopy was 100% and the sensitivity 24%. With this high specificity, the presence of mucopurulent discharge during endoscopy becomes a strong argument in favor of antibiotic treatment and culture sampling. 18
Our findings are different from other studies showing no correlation of endoscopic findings with other factors; Koskinen at al looked at differentiating CRSsNP and allergic rhinitis patients and found endoscopy not useful. 19 Feng et al examined different chronic nasal conditions in 150 asthmatic patients and did not find a difference in the Lund-Kennedy endoscopic score; however, they did find the nasal symptoms score in correlation with endoscopy score. 20 The usefulness of nasal endoscopy in these studies was low; however, different pathologies were evaluated there while the group in the current study was more homogenous and that may allow a better evaluation of nasal endoscopy as a tool.
Although we studied a relatively small sampling of patients, we were able to demonstrate a statistically significant correlation between nasal endoscopy during physical examination and the patients’ subjective status. We were investigating specifically a selective group of patients with CRS who had no nasal polyps for whom we formulated a unified management strategy and follow-up without surgical intervention, thus aiming for consistent methodology. In accordance with other studies, we were able to show that utilization of the CT scan during patients’ assessment should be used in refractory cases or when a surgical intervention is considered, especially when endoscopic findings are substantial and are compatible with patients’ complaints. A normal nasal endoscopy in a patient who may have underlying CRS (false negative) supports the role of CT if there is high clinical suspicion. While imaging plays a central role in CRS management, it is secondary to a thorough, attentive patient interview for obtaining medical history and symptoms and to a physical examination that includes a nasal endoscopy.
Conclusions
Nasal endoscopy is an important part of the evaluation of patients with CRSsNP. A high SNOT-20 score is in agreement with poor endoscopic findings. However, we could not demonstrate a strong correlation between nasal endoscopy and CT scan scores. Therefore, with respect to patients with CRSsNP, positive nasal endoscopy could be utilized as a beneficial, objective tool that facilitates an appropriate management plan, as long as surgical intervention is not considered, or complications are not suspected.
Footnotes
Acknowledgments
The authors wish to thank Mrs Tobie Kuritsky and Migal-CBR for editorial assistance.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.