
Abstract
Objectives:
The inconspicuous location and nonspecific symptoms of pharyngeal foreign bodies (FBs) can lead to diagnostic challenges and suboptimal outcomes. This retrospective cohort study aimed to investigate the endoscopic characteristics of pharyngeal FBs to provide guidance for clinical diagnosis and management.
Methods:
Patients with a chief complaint of FB sensation in the pharynx who underwent flexible fiberoptic endoscopy were included. The χ² test was used to compare FB incidence between anatomical regions; association analysis was used to identify factors associated with an FB sensation.
Results:
Of the 460 patients included in the study, FB were confirmed in 190 patients (41%). The root of the tongue (46.84%) and lower poles of the tonsils (18.95%) were the most frequent hypopharyngeal and oropharyngeal sites, respectively. Juvenile patients exhibited a higher incidence of oropharyngeal FB. Additionally, 29 patients (10.7% of patients with an FB sensation) had pharyngeal injury without FB; injuries occurred significantly more frequently in the hypopharynx (21/29, 72.41%) than in the oropharynx (8/29, 27.59%).
Conclusions:
Pharyngeal FBs occur more frequently in younger patients and at the root of the tongue. Hypopharyngeal injury is a likely cause of FB sensation in patients with no FB detected on endoscopy.
Introduction
Pharyngeal foreign bodies (FBs) are a common problem encountered in ear, nose, and throat clinics, often resulting in a sore pharynx, with discomfort being the most pronounced during swallowing. Complications can occur if FBs are not handled properly or in a timely manner. FB lodgment can cause airway obstruction or swallowing dysfunction. Moreover, sharp or abrasive FBs can cause trauma to the mucosal lining of the pharynx, leading to bleeding, infection, and perforation. Furthermore, secondary complications may occur, including chronic inflammation and formation of granulomas or fistulas.1,2 However, the hidden location of FBs in the pharynx combined with imprecise patient symptoms often leads to challenges in clinical diagnosis and treatment, resulting in reduced case management efficiency. Currently, pharyngeal FBs are removed via conventional laryngoscopy or flexible fiberoptic endoscopy. A flexible fiberoptic endoscope offers advantages such as simplicity of operation, a clear field of view, and precise localization, which enhance the diagnostic and treatment efficacy for pharyngeal FBs. In addition, the flexibility and magnification provided by the fiberoptic endoscope allow easy access to various parts of the pharynx and provide a clear field, respectively. This improves detection of concealed or small FBs and provides real-time visual guidance to remove the FB without additional trauma or complications. 3 This study aimed to clarify the clinical characteristics of patients with pharyngeal FBs who underwent flexible fiber optic endoscopy to help guide the clinical diagnosis and treatment.
Patients and Methods
Patients
This retrospective review included patients with a chief complaint of FB sensation in the pharynx who underwent flexible fiberoptic endoscopy at the Shandong Provincial Hospital Ear, Nose, and Throat clinic between March 2022 and March 2023. The inclusion criteria were as follows: (1) history of FB sensation in the throat after swallowing food that persisted until presentation; (2) duration of symptoms ≤1 week; (3) no obvious FB observed on indirect laryngoscopy; (4) flexible fiberoptic endoscopic examination was performed. Based on the endoscopic findings, patients with FB sensation were divided into the FB and non-FB groups. All endoscopic procedures were performed by otolaryngologists.
Instruments
A Visera Elite Video System (OTV-S190; Olympus, Dongjing, Japan), endoscopic camera system (MATRIX HD3; XION, Dongjing, Japan), and disposable biopsy forceps (AMHBFA1.8x1200; Anrei, Hangzhou, China) were used.
Anesthesia Methods
Local anesthesia was administered to all patients before examination. A combination of 1% tetracaine with 1 mL/mg epinephrine was sprayed into the nasal cavity using a nasal spray device. Subsequently, 1% tetracaine was loaded onto another spray device and sprayed into the pharynx.
Examination Methods
The patient was seated, and a flexible fiberoptic endoscope was inserted through the more spacious nostril. If the patient had extremely-narrow nasal passages, which prevented the passage of the flexible fiberoptic endoscope, the patient was asked to bite on a mouth prop, and the endoscope was inserted into the pharynx through the oral cavity. Various parts of the pharynx were carefully examined, focusing on the side where the patient complained of pain or an FB sensation. Suspicious areas were examined multiple times.
Upon discovering an FB, the assistant inserted the biopsy forceps into the pharynx through a channel in the flexible fiberoptic endoscope. First, the distance and the angle between the flexible fiberoptic endoscope, forceps, and the FB were adjusted. Next, the FB was carefully grasped without any damage to the surrounding mucosal tissues. Finally, depending on the size of the FB, it was slowly removed using the flexible fiberoptic endoscope through the mouth or nose.
Statistics Analysis
The χ2 test and Fisher’s exact test were used to compare clinical characteristics between patients with and without FB. Additionally, association analysis was performed to investigate the correlation between the FB location (hypopharynx or oropharynx) and sex, age, and side of the FB. Statistical significance was set at P < .05. Data analysis was performed using SPSS Statistics for Windows, version 26.0 (IBM Corp, Armonk, NY, USA).
Results
Patients Characteristics
A total of 460 patients (232 [50.43%] women and 228 [49.57%] men) met the inclusion criteria. The mean ± standard deviation age was 34 ± 16 years, with the range of 2 to 86 years old. Based on the endoscopic findings, 190 (41%) patients were diagnosed with pharyngeal FBs.
Characteristic of Patients with FB
Among patients with FBs, 95 were women (50%) and 95 were men (50%). Patients’ age showed a normal distribution with 30 (15.79%) juveniles (age <18 years), 101 (53.16%) young adults (age, 18-39 years), 47 (24.74%) middle-aged adults (age, 40-59 years), and 12 (6.32%) older adults (age ≥60 years; Figure 1A). FBs were predominantly found in the hypopharynx and oropharynx. Within the hypopharynx, the most common anatomical regions were the root of the tongue (89 patients, 46.84%) and the vallecula epiglottica (19 patients, 10%). In the oropharynx, FBs were frequently found at the lower and upper poles of the tonsils (36 patients, 18.95%, and 28 patients, 14.74%, respectively; Figure 1B). FBs were mostly detected on the left and right sides of the pharynx (94.21%), and only 5.78% were detected in the middle part (Figure 1C). The distribution of FBs according to anatomical regions is shown in Figure 2.
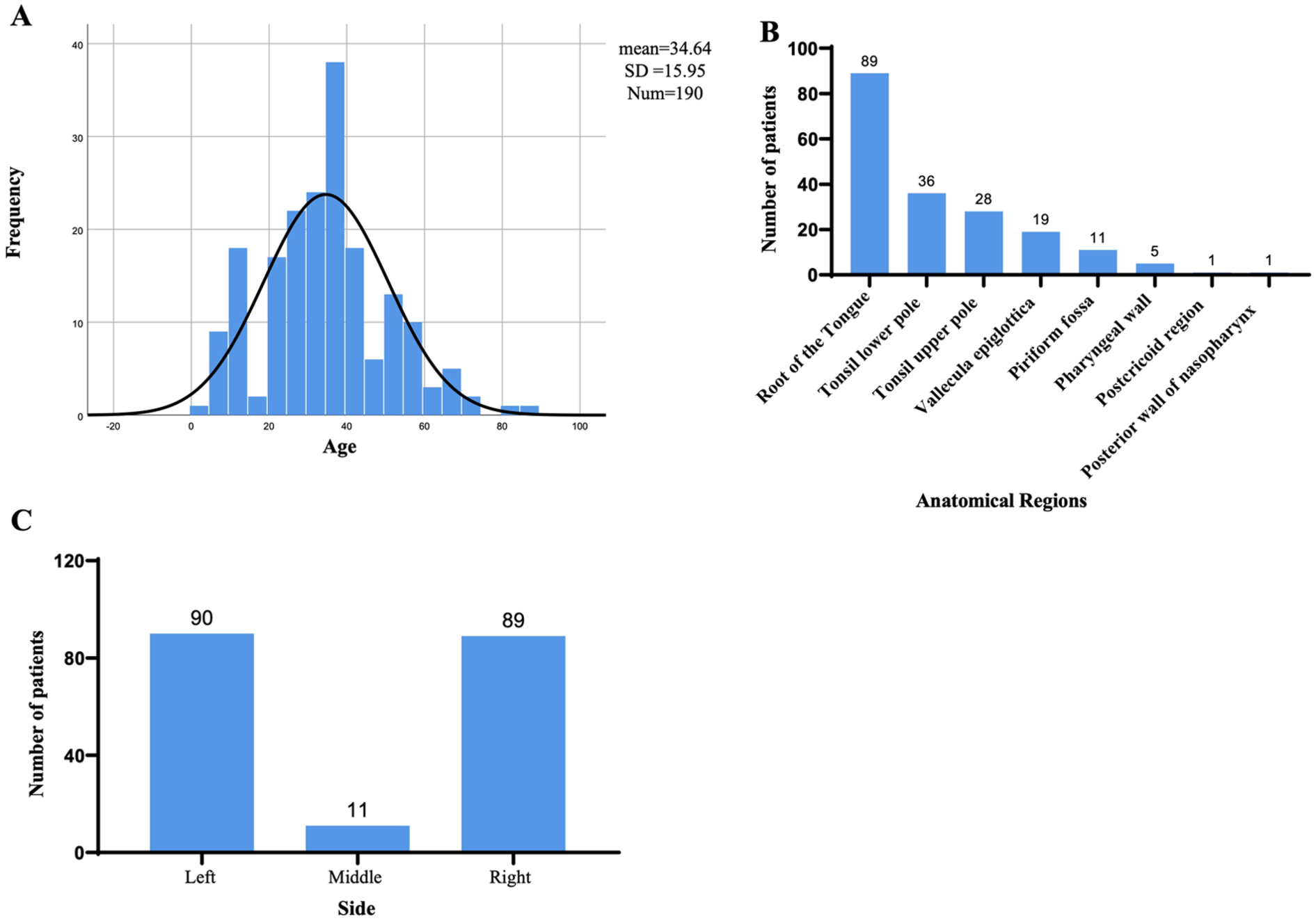
Details of patients with foreign body found in pharynx. (A) Histogram of the frequency distribution of patients ages. (B) Distribution of anatomical regions where foreign body were located in the pharynx. (C) Different sides of foreign body in pharynx.
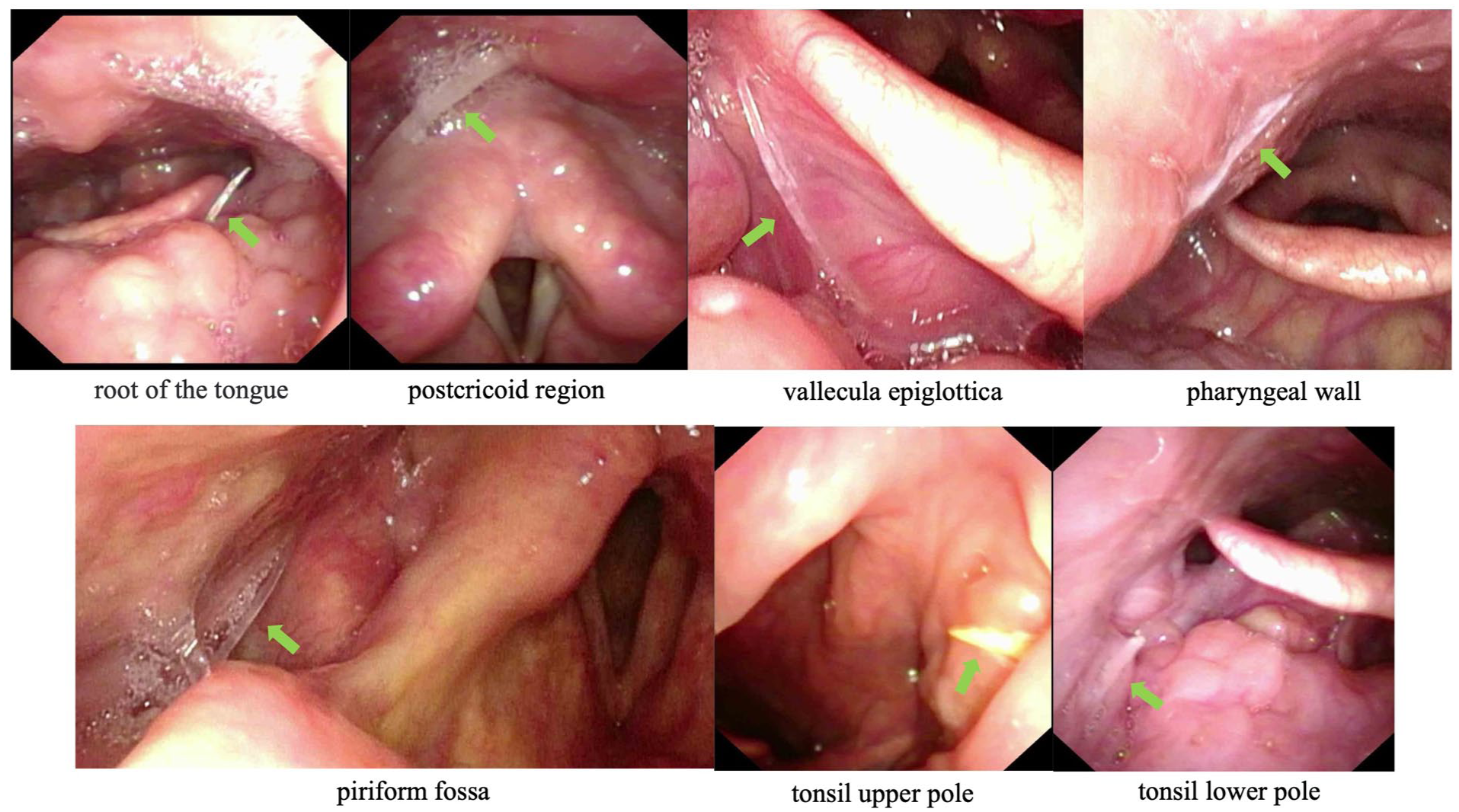
Visualization illustrating the spatial distribution of foreign body lodging sites observed during flexible fiberoptic endoscope.
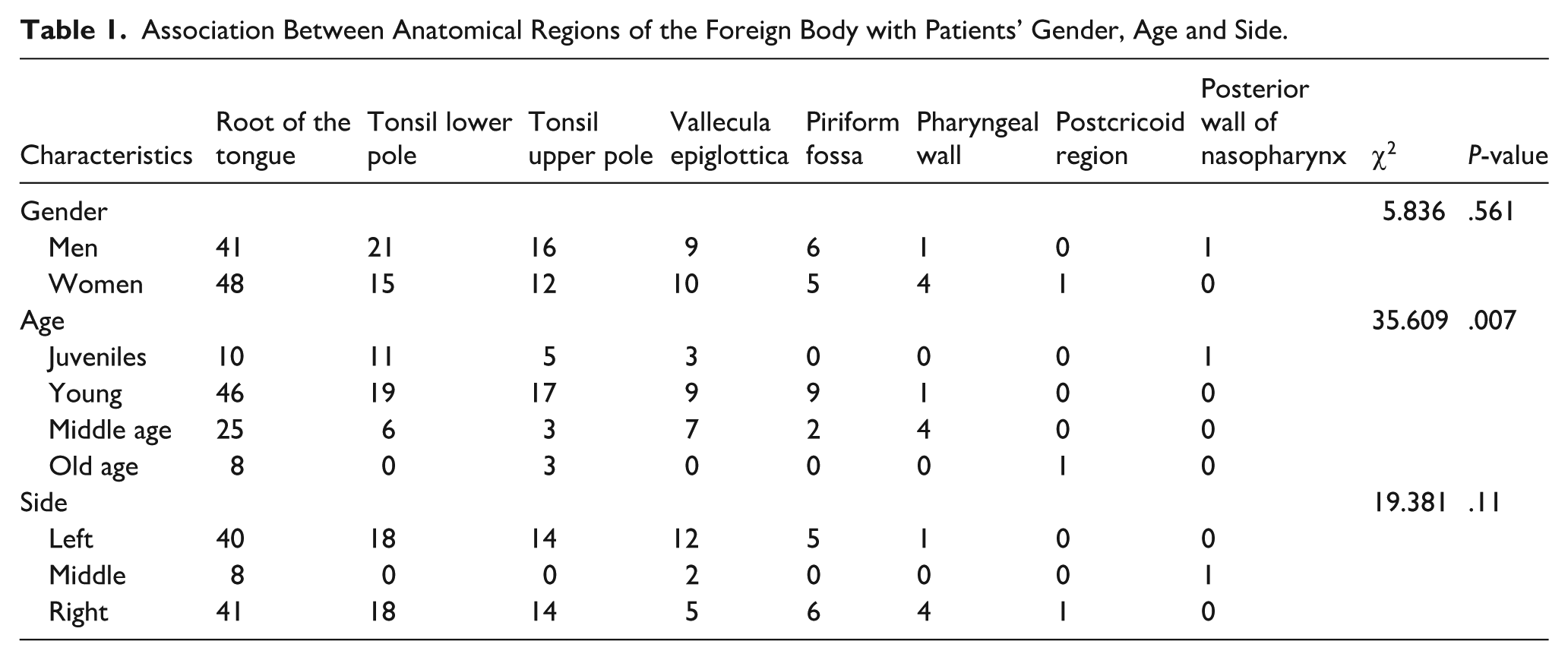
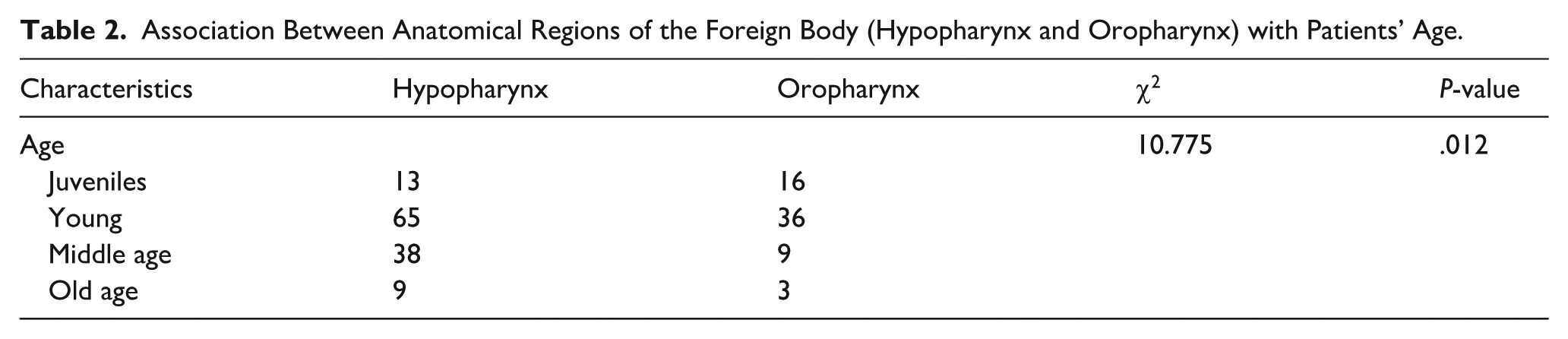
Association analysis revealed no significant correlation between the anatomical position of the FB and the side and patient’s sex (P > .05; Table 1). However, FB were more likely to occur in the oropharynx of juvenile patients and in the hypopharynx of other age groups (P < .05; Table 2).
Association Between Anatomical Regions of the Foreign Body with Patients’ Gender, Age and Side.
Association Between Anatomical Regions of the Foreign Body (Hypopharynx and Oropharynx) with Patients’ Age.
Characteristic of Patients Without FB
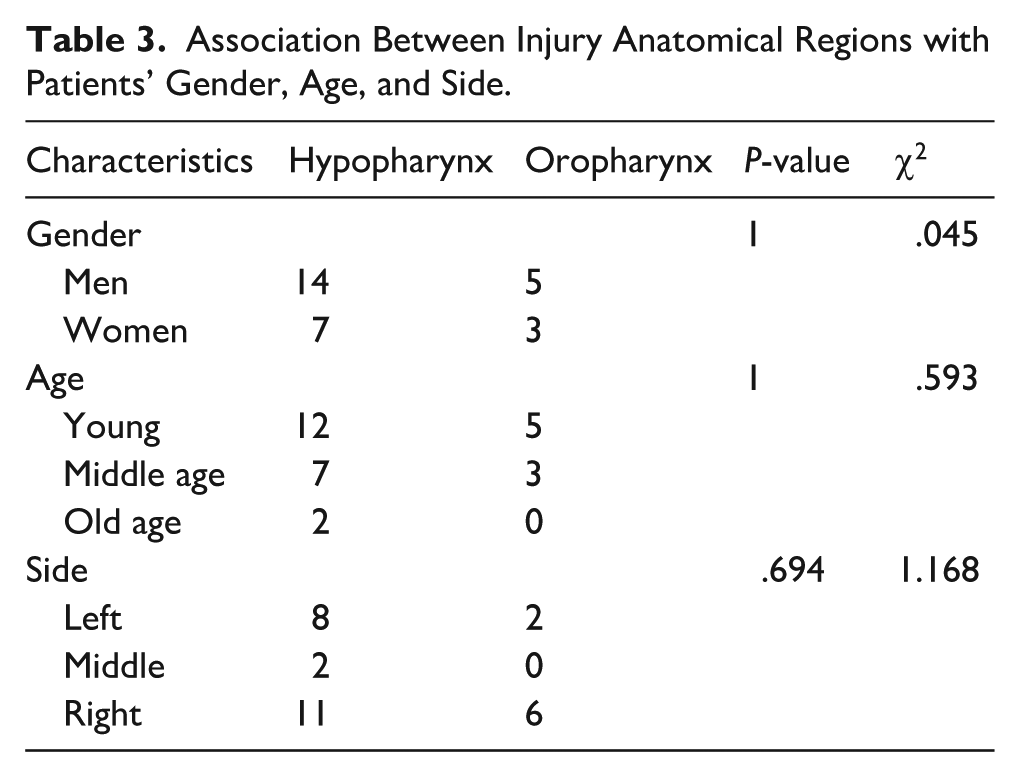
Among patients with an FB sensation, no FB was detected on endoscopy in 270 patients (137 [50.7%] women and 133 [49.3%] men). Of these, 45 (16.67%), 138 (51.11%), 65 (24.07%), and 22 (8.15%) patients were juvenile (age <18 years), young adults (18-39 years), middle-aged adults (40-59 years), and older adults (≥60 years), respectively. Age and sex distribution were not significantly different between patients with and without FBs. Among the 270 patients, 29 (10.7%) were diagnosed with pharyngeal injury using flexible fiberoptic endoscopy, including 19 men (65.51%) and 10 women (34.49%) comprising 17, 10, and 2 young, middle-aged, and older adults, respectively (Figure 3A). Injuries were frequently observed in the tonsils (24.13%), posterior hypopharyngeal wall (20.69%), postcricoid region (17.24%), arytenoid area (13.79%), and other areas (24.15%; Figure 3B). The injuries included ulcers, hyperemia, and edema, of which 21 (72.41%) and 8 (27.59%) were observed in the hypopharynx and oropharynx, respectively. No significant correlation was observed between the anatomical regions of injury and sex, age, or side (P > .05; Table 3).
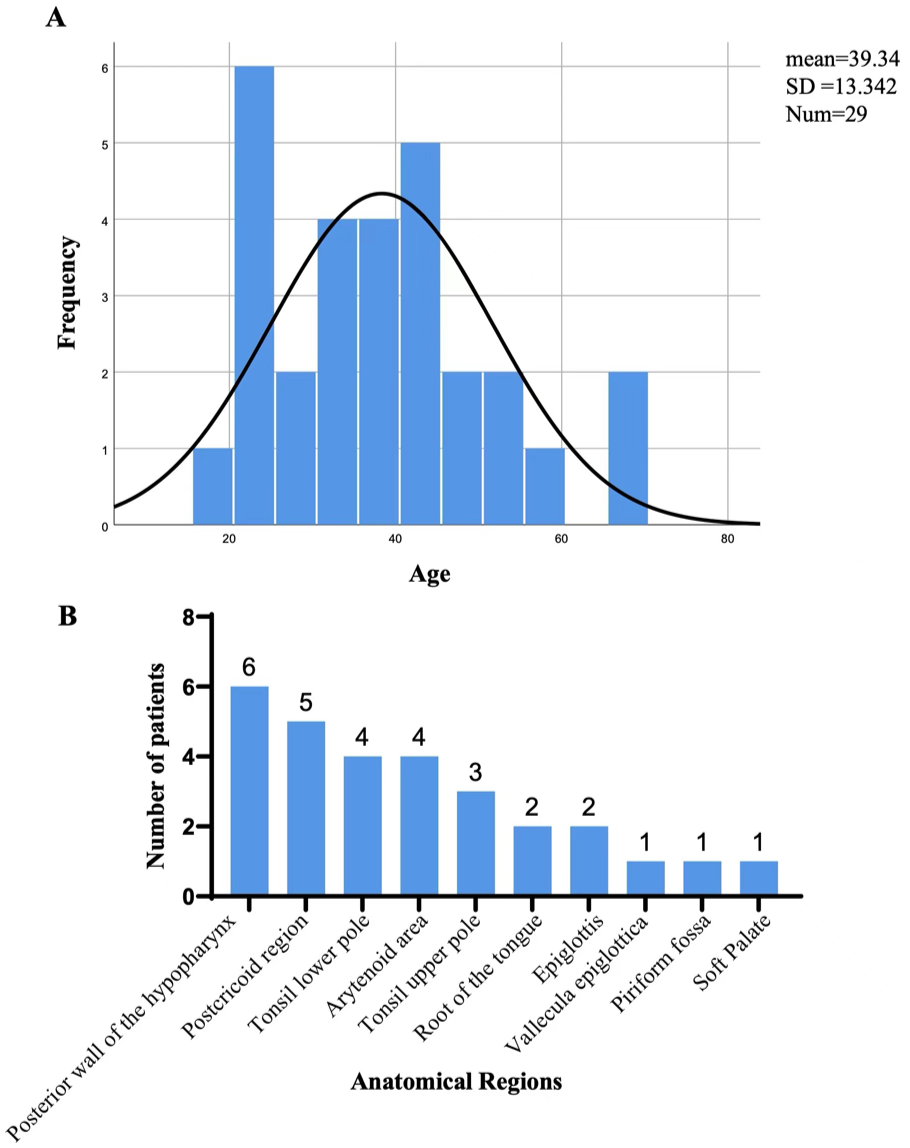
Details of patients without foreign body found in pharynx. (A) Histogram of the frequency distribution of patients ages. (B) Anatomical regions where injuries occurred in pharynx.
Association Between Injury Anatomical Regions with Patients’ Gender, Age, and Side.
Discussion
Pharyngeal FBs are a common problem encountered in ear, nose, and throat clinics. The anatomy of the pharynx is intricate, featuring uneven surfaces that can readily harbor FB in areas such as the tonsils, root of the tongue, vallecula epiglottica, piriform fossa, and other locations, making detection challenging. 4 Moreover, the pharynx is richly innervated, primarily by the pharyngeal nerve plexus located in the posterior pharyngeal wall, which includes the glossopharyngeal, vagus, and maxillary nerves. Therefore, small FBs can cause considerable discomfort or pain. 5
Timely removal of pharyngeal FBs is crucial. Small FBs may cause minor discomfort such as a feeling of pricking or an FB sensation. Compared with larger FBs, smaller FBs are more difficult to detect, leading to prolonged retention. However, the longer the delay in extraction, the more challenging the removal process, and Huang et al reported that FB retention >24 h was the main risk factor for complications in children aged <10 years. 6 FB retention for longer duration may lead to a series of complications, such as FB penetration of the retropharyngeal space and embedding in the upper digestive tract. 7 Furthermore, large FBs may penetrate the esophageal wall, resulting in serious complications such as retropharyngeal or prevertebral abscess, tracheoesophageal fistula, mediastinitis, septicemia, or shock.8 -11 Although large FBs are more easily detected, their complications are more dangerous and may occasionally be life-threatening. In some cases, FB ingestion may lead to pharyngoesophageal perforation, carotid artery rupture, aortoesophageal fistula, and deep neck space infections.12,13 Accurate localization and early removal of FB are crucial for controlling complications. Compared with indirect laryngoscopy, flexible fiberoptic endoscopy is a safe, effective, and well-tolerated diagnostic tool for pharyngeal FB and is widely accepted and recommended worldwide. 6
In this study, FB were confirmed in only 41% patients presenting to the clinic with a chief complaint of an FB sensation in the pharynx. In a retrospective cohort study of adult patients with a chief complaint of FB sensation in the pharynx, larynx, or esophagus presenting to urban academic hospitals, FBs were visualized in 13/27 (48.15%) patients, 14 which was similar to that in our study. The exact cause of the FB sensation remains unclear. Among the 270 patients in whom no FBs were detected in this study, 29 exhibited mucosal injuries that could have contributed to the FB sensation in the pharynx. Moreover, FBs causing discomfort may have been removed spontaneously or passed into the esophagus. 15 Several recent studies have reported a link between FB sensation and conditions such as laryngopharyngeal reflux, gastroesophageal reflux disease, nonspecific esophageal motility disorder, psychological conditions, upper respiratory inflammation and tumors, thyroid disease, and cervical heterotopic gastric mucosa.16 -18
This is the first study to evaluate the association between FB location and clinical features. In this study, the incidence of FBs was higher in the oropharynx than in the hypopharynx. Specifically, the major anatomical sites of FB were the root of the tongue, tonsils, and vallecula epiglottica. These results align with those of the study conducted by the Department of Otolaryngology of Nanjing Drum Tower Hospital, in which the most common sites of pharyngeal FB were the root of the tongue (42.29%), vallecula epiglottica (19.40%), and tonsils. 5 The epiglottis is connected to the root of the tongue, forming a peculiar funnel-shaped anatomical structure that is predisposed to FB lodgment. 19 In addition, FBs are more likely to be concealed at the superior and inferior poles of the tonsils in patients with tonsillar hypertrophy. 20 In this study, the incidence of FB in different locations was not different between the sexes or sides. Furthermore, in young patients, FB were more likely to occur in the oropharynx, possibly because of the physiological tonsillar hypertrophy in children and increased susceptibility to FB entrapment. 21 Therefore, more attention should be paid to the oropharyngeal region when treating young children with pharyngeal FB sensations.
In conclusion, pharyngeal FBs are more likely to occur in younger patients and at the root of the tongue. In patients with no FB detected on flexible fiberoptic endoscopy, hypopharyngeal injury, especially in the posterior hypopharyngeal walls, is a more likely cause of FB sensation. A comprehensive evaluation can enhance the diagnostic and therapeutic efficiency of flexible fiberoptic endoscopy for pharyngeal FBs.
Footnotes
Acknowledgements
Author Contributions
Chao Jiang designed the study and supervised the research work. Changzhen Wu, Ye Li, and Lei Guo collected the data. Yongming Pan and Jing Li analyzed the data. Yongming Pan wrote the manuscript, and Butuo Li revised it.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the National Natural Science Foundation of China (Grant number 82203198) and the Natural Science Foundation of Shandong Province (Grant number ZR2022QH023).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.