
Abstract
We describe a novel and safe use of existing instrumentation in the removal of select foreign bodies in the upper aerodigestive tract to minimize health-care costs. A retrospective review of 4 cases involving visualized upper aerodigestive tract foreign bodies were identified via flexible laryngoscopy and extracted under local anesthesia from 2016 to 2018. All 4 patients were not in any airway distress and underwent successful removal of the foreign body, which included 2 fishbones, a sewing pin, and a wire bristle with a maxillary Heuwieser or giraffe instrument under flexible laryngoscopy visualizing using local anesthesia without complications. No foreign bodies were dislodged. The use of a maxillary Heuwieser and flexible laryngoscopy visualization is safe, allows for removal of otherwise difficult to reach foreign bodies at the bedside, improving patient comfort, obviates the need for general anesthesia to the patient, and minimizes health-care costs.
Introduction
Fish bones have classically been the most common foreign bodies that gets lodged in the pharynx. In recent years, the incidence of other foreign bodies in the pharynx has been rising, particularly the wire bristle. 1 One retrospective review identified 8% of all upper aerodigestive foreign bodies involved the throat with a bedside successful removal rate of 67%. 2 In cases when extraction is not possible using traditional bedside techniques, patients often require general anesthesia for operative exploration and removal. To date, there have been no reports of sinus instruments utilized for removal of throat foreign bodies.
Methods
The University of Rochester institutional review board approved this study. Retrospective review of case series involving visualized upper aerodigestive tract foreign bodies and 4 cases of foreign bodies lodged in the base of tongue were identified via flexible laryngoscopy and extracted under local anesthesia from 2016 to 2018. Success rates and complications including failure to extract or dislodgement of the foreign body were reviewed.
Results
Four adult patients were identified to have a foreign body visualized on flexible laryngoscopy. All 4 patients presented immediately to the emergency department following foreign body ingestion were not in any airway distress and underwent successful removal of the foreign body, which included 2 fishbones, a sewing pin, and a wire bristle. All patients tolerated the procedure without excessive gag reflex or complications (see Figure 1).
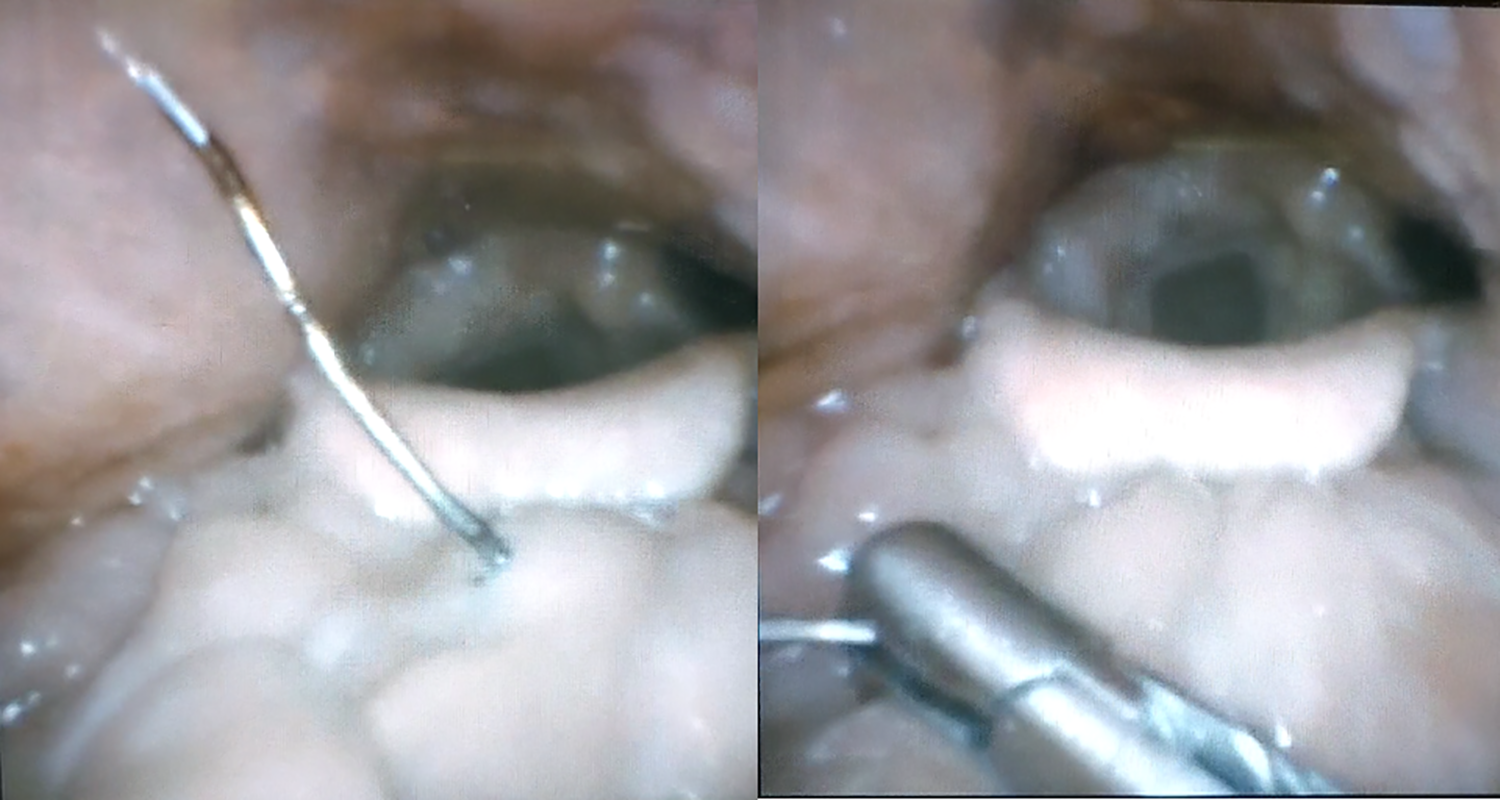
(Left) Flexible nasendoscopy reveals wire bristle embedded in base of tongue, (right) removal under nasoendoscopy with front-to-back nonbiting giraffe.
Technique
Flexible nasendoscopy is used first to identify foreign body location. If visualized, the described technique can be attempted. The nose is topicalized with oxymetazoline and 2% lidocaine spray followed by 2% lidocaine soaked pledgets bilaterally. The aerodigestive tract is then topicalized with 3 mL of 2% lidocaine nebulized over 10 minutes. The pledgets are removed and the flexible nasendoscope is positioned to visualize the foreign body on the screen. The surgeon utilizes an assistant to stabilize the endoscope, retracts the tongue with a gauze, and uses either a maxillary Heuwieser or 90-degree side-to-side nonbiting giraffe (Karl Storz, El Segundo, California) to remove the foreign body (see supplemental video).
Discussion
Historically, removal of foreign body involved utilizing a laryngeal mirror or direct laryngoscopy with patient in intubation position. In 1990s, flexible gastroscopes and nasendoscopes with working channels were described in the use of removal of foreign bodies, however the ability for the patient to tolerate these was limited due to the discomfort associated with the larger caliber endoscopes. 3,4 The flexible nasendoscopy guided removal of fish bones was described in 1995 by Koay and Herdman, 5 where the eyepiece was stabilized by an assistant and the surgeon removes the visualized foreign body using Magill forceps following topical spray of anesthetic to the throat.
Several advancements in different subspecialties over past decades allow further refinement of foreign body removal. Major advances such as smartphone mounts and video towers now allow for bedside video flexible nasendoscopy routinely. The use of nebulized local anesthetic has been described in the removal of fish bones in the oropharynx and is a common technique utilized in awake fiberoptic intubation. The topical application of local anesthetic via nebulization with adequate anesthetic application to the nose is an important technique for successful transoral injection laryngoplasty. When utilized appropriately, it can minimize the patient gag reflex and allow for better tolerance of foreign body removal in difficult areas such as the oropharynx. Advances in sinus surgery in the past 2 decades have led to the development of a host of specialized tools for manipulation of tissue in difficult to reach areas such as the frontal and floor of the maxillary sinuses. These instruments are small in profile and contoured to reach beyond the base of tongue to the piriform sinuses without contact to the surfaces of the oropharynx that can elicit a gag reflex. Varied closure patterns of the graspers allow for facile removal of the foreign bodies in any orientation (Figure 2).
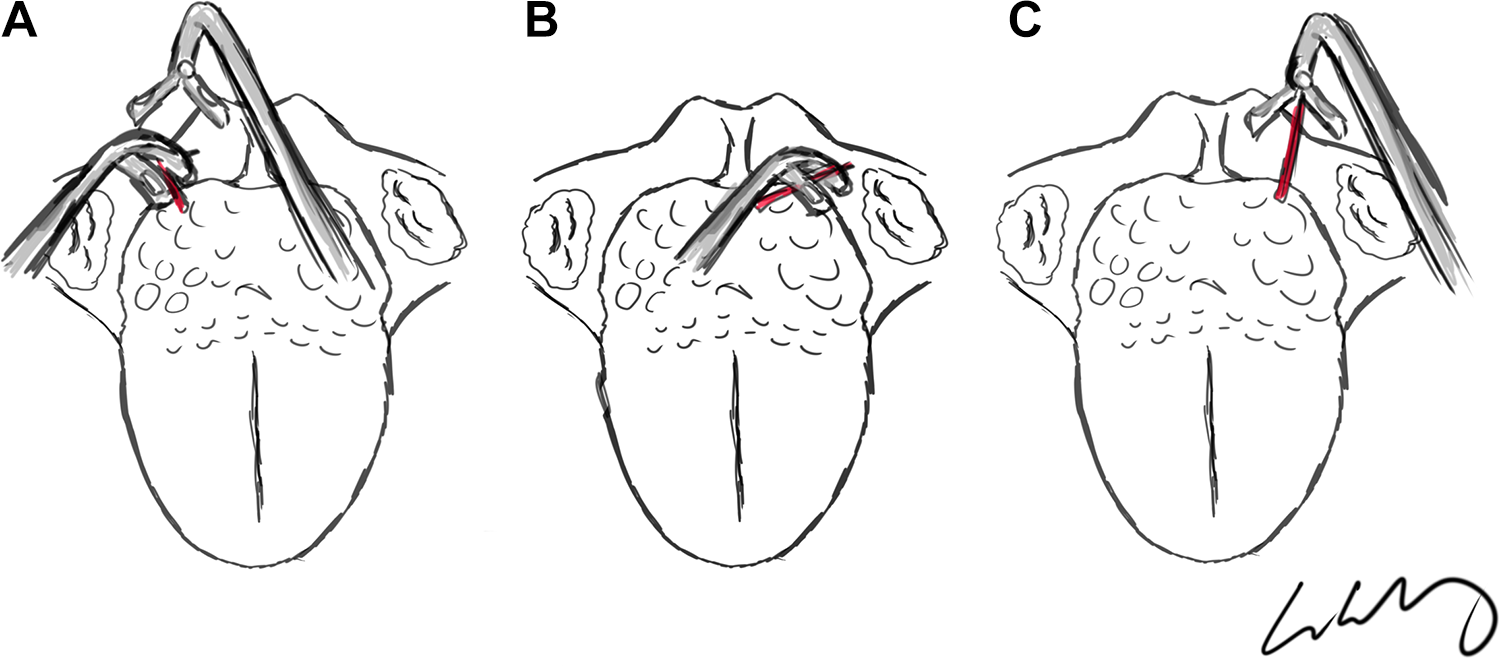
A, Only tip of foreign body visible, amenable to either Heuwieser or side-to-side giraffe. B, Horizontally oriented, most accessible by Heuwieser. C, vertically oriented, most accessible by side-to-side nonbiting giraffe.
Several factors in general practice can make existing techniques difficult to implement. While flexible laryngoscopy is commonplace, channeled flexible endoscopes may not be available in some practice settings for foreign body removal. In contrast, sinus instruments are a routine part of general otolaryngology practice. There is a significant size and articulation advantage to use of sinus instruments. A comparison of the sizes of commonly used instruments including St. Clair-Thompson forceps and Magill forceps compared to sinus instruments is shown in Figure 3; the articulating joint of the mentioned forceps is at the handle and thus the shaft opens when attempting to grab foreign bodies, an issue that is not present with sinus instruments.
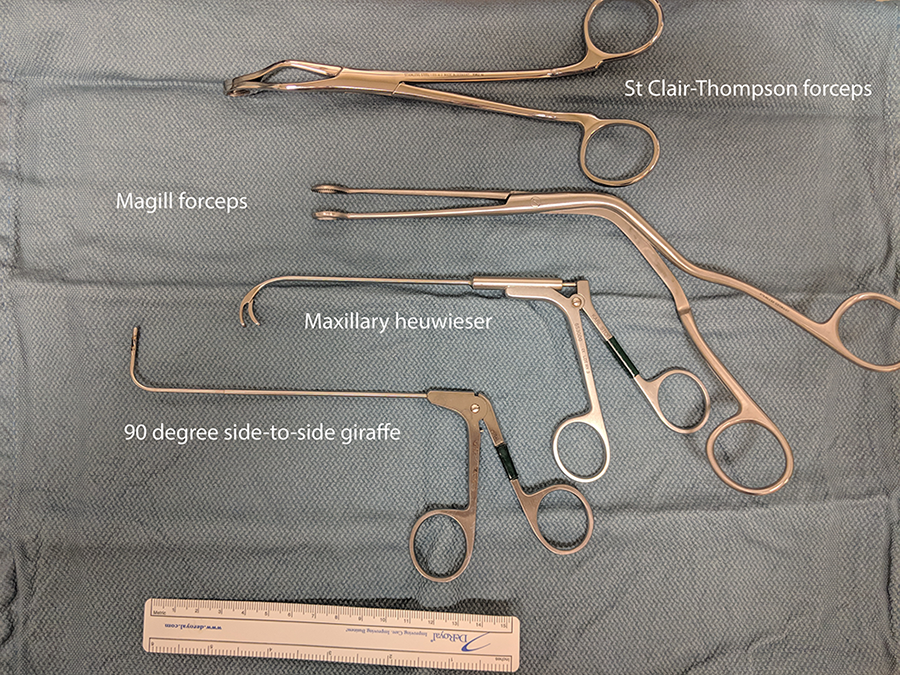
Comparison of traditional forceps to maxillary Heuwieser and side-to-side giraffe. The articulation of the forceps widens the shaft of the forceps when opening as demonstrated, not seen with sinus instruments.
Our report contributes to the refinement of existing foreign body removal techniques described by Koay and Herdman by integrating the newer technologies employed in different subspecialties of rhinology and laryngology. 5 These can improve patient comfort during removal and may allow for removal of otherwise difficult to access foreign bodies in the oropharynx that would necessitate general anesthesia and direct laryngoscopy. Avoiding the need to go to the operating room in visualized foreign bodies has many advantages including minimizing delay in removal and potentially losing visualization of a migrating fish bone, decreasing the overall health-care cost, and eliminating exposing the patient to the risks of general anesthesia.
Conclusions
The use of sinus instruments in conjunction with flexible laryngoscopy visualization is safe, allows for removal of otherwise difficult to reach foreign bodies at the bedside. This obviates the need for general anesthesia to the patient and minimizes health-care costs.
Footnotes
Authors’ Note
Poster presentation at ABEA of the Combined Otolaryngology Spring Meeting May 1-5, 2019; Austin, Texas.
Acknowledgments
The authors appreciate Dr Paul Alain Lambert’s assistance in the making of the supplemental video. The sample footage was recorded in a safe, controlled fashion and the research subject (W.W.) was not subjected to risk of foreign body aspiration.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.