
Abstract

Anterior cervical spine fusion and plate fixation is the procedure of choice when the goal is to gain access to the anterior aspect of the spinal cord and nerve roots. 1 Although upper airway-digestive tract involvement is possible after spine surgery, it is unusual and generally due to visceral perforation and graft displacement, or external compression. 2
The case here presented refers to a 53-year-old Sinhalese man who came to our emergency department because of unremitting and progressive dyspnea associated with odynophagia, pharyngodynia, and a temperature and weight loss; the initial complaints had occurred 2 months earlier. A clinical examination revealed severe inspiratory dyspnea with tirage and cornage, and a flexible trans-nasal fiber endoscopic evaluation documented the presence of a large, smooth, and pinkish endolaryngeal mass. This formation seemed to protrude from the posterior aspect of the hypopharyngeal wall at the level of the epiglottis petiole, and obstructed the airway lumen so that the glottic plane and pyriform sinuses could not be explored (Figure 1A). An emergency tracheotomy was performed under local anesthesia, which led to the recovery of spontaneous breathing. A post-tracheotomy computed tomography (CT) scan of the neck region revealed the presence of a swelling in the posterior hypopharyngeal wall that obliterated both piriform sinuses and seemed to originate from a large bone fragment located about 1.5 cm in front of the body of the fourth cervical vertebra and associated with a surrounding inflammatory reaction. A more precise case history was taken in the presence of a Shinalese interpreter, and the patient reported that, 4 years earlier, he had undergone anterior cervical decompression at levels C3 and C4 with fusion by bone grafting (an iliac crest autograft) and without plate fixation because of a cervical vertebral hernia. Therefore, he underwent high-resolution CT and magnetic resonance (MR) scans of the cervical spine (Figure 1B) that revealed evidence of cage migration in front of the body of the fourth cervical vertebra. The foreign body was surrounded by strongly enhanced soft tissue reaching the posterior hypopharyngeal and laryngeal walls, the possible expression of an inflammatory reaction. Consequently, the patient was started on intravenous broad-spectrum antibiotic therapy with piperacillin + tazobactam 2.25 g 3 times a day, and metronidazolo 500 mg 3 times a day. One day later, the patient vomited a foreign body that proved to be the bone cage used for cervical spine arthrodesis (Figure 1C) and, suspecting the development of a hypopharyngeal fistula, a nihil per os regimen was introduced and a naso-gastric feeding tube was positioned. The CT and MR scans confirmed the presence of a fistulous tract extending from the spine to the right posterior hypopharyngeal wall (Figure 2). The patient also developed fever with increased inflammatory indices, and a peripheral blood culture was positive for multiresistant S. mitis. Consequently, on the basis of an antibiogram, intravenous vancomycin was introduced and led to a clinical improvement documented by a progressive reduction in the volume of laryngeal tumefaction revealed by repeated fiber endoscopic assessments (Figure 3A), and a subjective improvement in breathing. However, the development of impaired renal function meant that vancomycin was stopped and surgical therapy was considered because of the persistence of fever. Ten days after admission, the patient underwent a combined trans-cervical otolaryngological and neurosurgical procedure: no abscess cavity was found, but retro-pharyngeal granulation tissue was discovered at the interface between the prevertebral space and the posterior hypopharyngeal wall. No evident fistulous tracts were detected, but inspection of the spine plane revealed osteomalacia of the residual fourth spinal arch. After consultation with an infectious disease specialist because of the persistence of fever, intravenous meropenem (1 g twice a day) and teicoplanine (400 mg a day) were started and led to a progressive clinical and subjective improvement. Fiber endoscopy showed a further progressive reduction in posterior hypopharyngeal wall swelling (Figure 3B) and a contrast MR scan 7 days after surgery documented the closure of the fistulous tract. The patient was returned to oral feeding and discharged a few days later with a prescription for daily antibiotic administrations on an outpatient basis for 4 weeks. No recurrences had occurred 2 years later (Figure 3C).
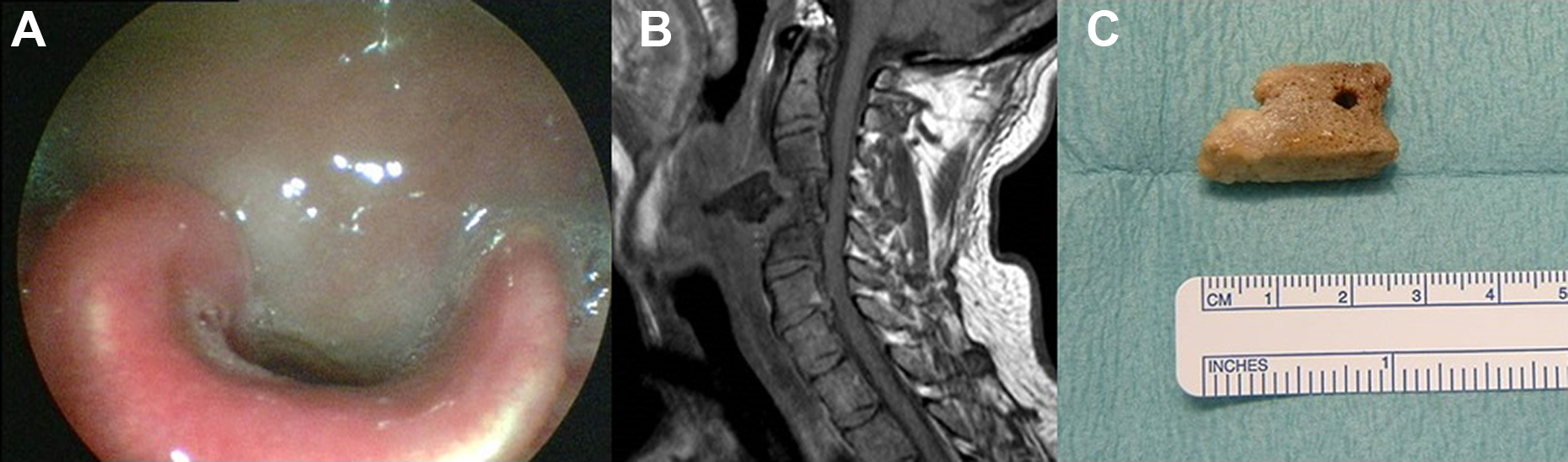
Endoscopic view of a protruding mass completely obstructing the laryngeal lumen (A); MR scan showing cage displacement in front of the body of the fourth cervical vertebra and the surrounding inflammatory tissue (B); the vomited bone cage (C). MR indicates magnetic resonance.
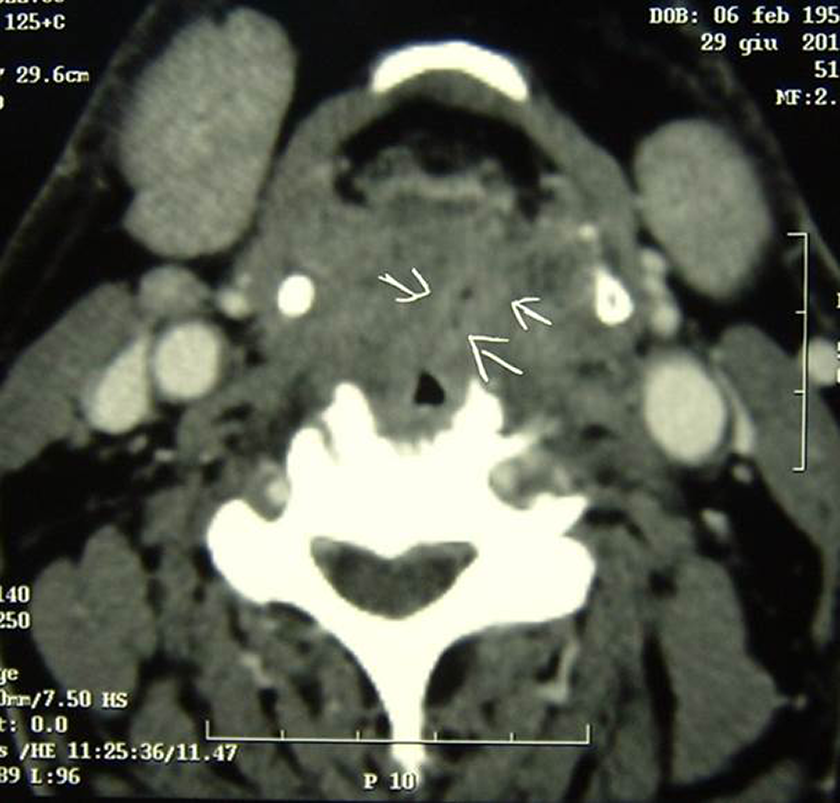
Computed tomography scan showing the presence of a fistulous tract extending from the spine to the right posterior hypopharyngeal wall (white arrows).
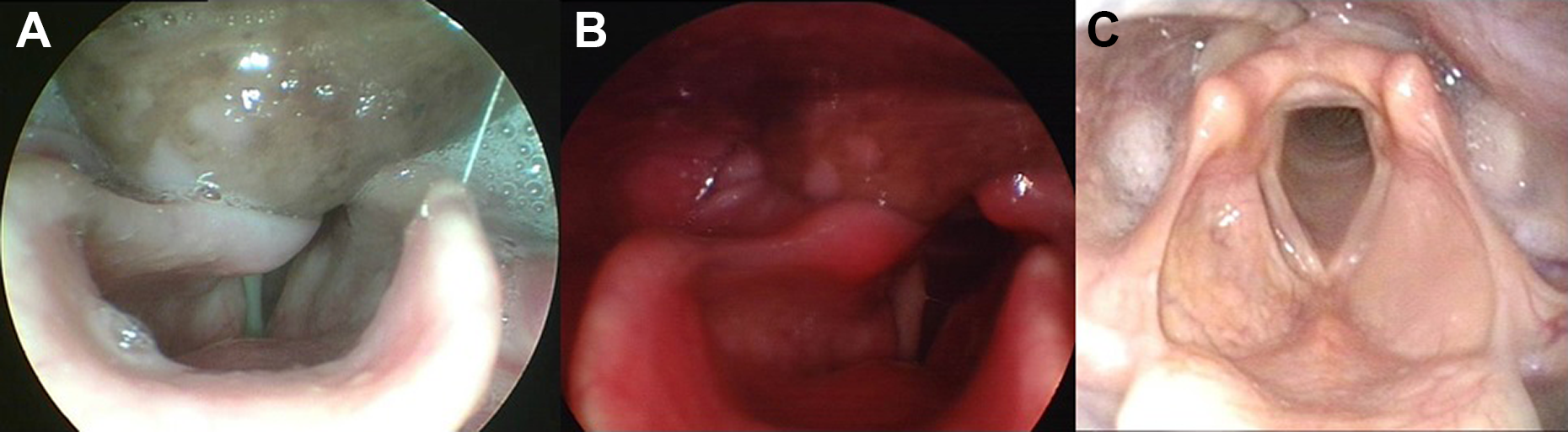
Endoscopic view documenting a slight reduction in the protruding endolaryngeal mass 8 days after admission (A); endoscopic view documenting the significant reduction in the protruding endolaryngeal mass 17 days after admission (B); endoscopic view at the end of the 2 years follow-up period showing complete restitutio ad integrum (C).
Delayed hypopharyngeal and esophageal perforation with bone graft displacement in the digestive tract have previously been reported as infrequent complications after vertebroplasty (<1% of cases) 3 be due to the protrusion and displacement of the autologous bone grafts and abscess formation. 4 Dyspnea after vertebroplasty is extremely unusual and due to laryngeal soft tissue compression by a protruding posterior vertebral abscess or displaced foreign bodies, or may rarely be related to bilateral Recurrent laryngeal nerve palsy. 5 Delayed perforation with late bone graft extrusion and deep neck space infection may be treated by means of enteral feeding, aggressive intravenous antibiotic therapy, and surgical drainage and debridement. However, the management of a small delayed hypopharyngeal and esophageal perforation such as that affecting our patient is still much debated. Some authors recommend surgical management as the first choice because conservative management is associated with the formation of an abscess in 25% to 45% of cases. 6,7 On the other hand, a wait-and-see strategy including adequate systemic antibiotic therapy and parenteral feeding may be effective in the case of small perforations with a well-contained leak and in stable patients without septicemia. 8
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.