
Abstract
Objective:
The differences in the outcomes between the totally endoscopic approach and the traditional microscopic approach remain unclear for limited attic cholesteatomas. This systematic review and meta-analysis aim to compare the outcomes of the endoscopic approach and the microscopic approach for the management of cholesteatoma limited to the attic.
Data Sources:
Searches were performed using PubMed, Cochrane Library, Web of Science, Clinical Trials, and Google Scholar.
Review Methods:
This review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis Protocol 2020 guidelines. Studies were included based on predefined eligibility criteria and assessed for quality using the revised Cochrane risk-of-bias 2 tool and the Methodological Index for Non-Randomized Studies criteria. The primary outcomes for this review were audiological outcomes, healing time, operating time, middle ear structures visibility index (MESVI), postoperative complications, and long-term outcomes.
Results:
Seven studies with a total of 539 patients (541 operated ears) were included. The endoscopic group had a statistically significantly higher MESVI (Z = 23.205, P < .0001). The overall effect showed less postoperative pain among patients undergoing the endoscopic technique (Z = −6.942, P = .000). No statistically significant difference between both groups was found in terms of healing time, operating time, postoperative complications and audiological outcome.
Conclusion:
The endoscopic approach for the management of cholesteatoma limited to the attic region has some advantages compared to the microscopic approach, namely in terms of better middle ear structures visibility and less postoperative pain. Future research conducted with high-quality comparative prospective studies is needed to further compare both surgical approaches and confirm the advantages of the endoscopic approach.
Introduction
Cholesteatoma is an abnormal growth within the middle ear formed by keratinizing squamous epithelium. It usually destroys the ossicles and results in several complications.1 -3 Cholesteatoma can be classified according to its site of origin into 3 types: attic cholesteatoma, tensa cholesteatoma, and sinus cholesteatoma, which is considered an important factor in the determination of the surgical procedure and prognosis.3,4 In addition, the European Academy of Otology and Neurotology and the Japan Otological Society (EAONO/JOS) published a joint consensus in 2016 on the definition, classification, and staging of cholesteatoma. EAONO/JOS classified cholesteatoma into 4 stages, stage I: Cholesteatoma localized to the attic; stage II: Cholesteatoma involving 2 or more sites; stage III: Cholesteatoma with extracranial extension; and stage IV: Cholesteatoma with intracranial extension. 5
Traditionally, middle ear cholesteatoma surgery is performed under a microscope with a transcanal or retroauricular approach.2,6 In cases of attic cholesteatoma, the majority of surgeons favor the retroauricular approach (canal wall-up tympanoplasty + mastoidectomy) to perform epi-tympanotomy and eliminate the disease from the attic and middle ear. 6 However, it is difficult to view possible hidden lesions in the anterior epitympanic recess and tympanic sinus using a microscope alone, which can possibly lead to residual disease and recurrence. 7 For the past 2 decades, endoscopes have come a long way in the field of otology. Endoscopes offer multiple advantages due to the minimally invasive technique and improved visualization. 8 Initially, endoscopes were used as an adjunct to the traditional microscopic approach to improve visualization and access to hidden areas and unveil residual cholesteatoma during surgery. With time, their utility evolved to help in the dissection of cholesteatoma in areas difficult to reach by a microscope only.8,9 Nowadays, various authors propose the use of transcanal totally endoscopic ear surgeries as a safe and effective surgical approach for middle ear cholesteatoma.10 -13 Even though endoscopes provide better access and visualization of hidden areas, they have various limitations, including the lack of stereopsis, being a single-handed technique, and the need for prolonged training.2,7,14
Utilizing the endoscope for the treatment of middle ear cholesteatoma either by performing totally endoscopic ear surgery or microscopic surgery assisted by the use of endoscopy has been proven by various authors to significantly decrease the incidence of residual lesions as well as recurrence rate.15 -17 Yet, the differences in the outcomes between the totally endoscopic approach and the traditional microscopic approach remain unclear, especially for limited attic cholesteatomas. As such, this systematic review and meta-analysis aims to compare the outcomes of the endoscopic approach and the microscopic approach for the management of cholesteatoma limited to the attic.
Materials and Methods
Search Strategy
The systematic review adhered to the updated Preferred Reporting Items for Systematic Reviews and Meta-Analysis Protocol (PRISMA-P) 2020 statement. 18 The search was conducted on March 23, 2024, using 4 main databases: MEDLINE, Web of Science, Google Scholar, and PubMed. Only full-text articles available in English were included in our search. Moreover, our search was performed using the Boolean search technique with the following keywords: (attic cholesteatoma OR cholesteatoma OR middle ear cholesteatoma OR limited cholesteatoma) AND (endoscopic OR endoscope OR transcanal) AND (microscopic OR open OR microscopy). The relevance of studies included in the reference list was also assessed manually. Only comparative studies published in the English language that evaluated and compared the outcomes of endoscopic and microscopic techniques for the management of limited attic cholesteatoma were selected for further evaluation. The protocol for this study was registered in the International Prospective Register of Systematic Reviews with the registration number: CRD42024535930.
Inclusion and Exclusion Criteria
Studies were included in this review if they met the following inclusion criteria: (1) compared the outcomes of endoscopic and microscopic techniques in cases of limited attic cholesteatoma with at least 10 patients and no age limitation; (2) clear definitions of the endoscopic and microscopic approaches; (3) clearly defined outcomes such as healing time, and air-bone gap closure; (4) clear definition of the attic cholesteatoma as confirmed by Computed tomography (CT) scan.
Animal studies, abstracts, letters, editorials, reviews, and expert opinions were excluded. Studies were excluded for several reasons to maintain the integrity and consistency of our analysis. Some lacked the necessary outcome measures or did not address the objectives relevant to our review, making them unsuitable for meaningful comparison. Others had methodological inconsistencies, such as differences in population selection, intervention type, or outcome assessment, which were not aligned with our inclusion criteria. In addition, a number of studies were excluded due to the unavailability of full texts, despite multiple efforts to obtain them. Without access to the complete methodology and results, these studies could not be reliably assessed for inclusion.
Study Selection
Two reviewers independently screened the titles and abstracts of the identified articles using the search strategy against the eligibility criteria. Duplicate studies and irrelevant studies were excluded. Full-text reviews of eligibility were then performed for all remaining articles by the same 2 independent reviewers. Any disagreements regarding uncertainty were resolved through discussion with a third senior reviewer. The senior author approved all selected articles for inclusion.
Data Extraction
Using a standardized data extraction form, data were drawn by 3 authors and re-evaluated by 2 separate authors, and discrepancies were resolved through discussion and consultation with the senior author. The extracted data included the first author, publication year, study design, study population, number of patients, follow-up period, preoperative and intraoperative findings, operating time, MESVI, postoperative pain, postoperative complications such as taste sensation abnormalities and vertigo, audiological outcome, healing time, and long-term outcomes.
Quality Assessment
The revised Cochrane risk-of-bias 2 tool (RoB 2) was used to evaluate the quality of randomized controlled trials (RCTs). 19 The Methodological Index for Non-Randomized Studies (MINORS) was used to assess the quality of nonrandomized studies, including cohort, case-control, and comparative observational studies. 20 The MINORS criteria consist of 12 items scored as: 0 (not reported), 1 (reported but inadequate), 2 (reported and adequate) with a total maximum score of 24. 20 Two authors independently conducted the risk-of-bias assessment, and disagreements were resolved by consensus after consultation with the senior author.
Meta-Analysis and Data Synthesis
Separate meta-analyses were conducted for binary and continuous outcomes. As multiple study designs were included (it may lead to the methodological variability across studies), the random-effects model using the DerSimonian and Laird method was applied. Heterogeneity was summarized using the estimate of between-study variance (tau-squared), and the proportion of variability in effect estimates due to between-study heterogeneity was summarized using I-squared statistic (I2). Inverse variance methods were used for continuous outcomes, and Mantel-Hanzel method was used for binary outcomes. If the standard deviation was missing, we estimated it using the “t” distribution. A 95% prediction interval for the random-effects model was calculated if at least 3 studies were available in a meta-analysis. For continuous outcomes, the pooled mean difference (MD) was calculated and reported with 95% confidence intervals (CIs), and for binary data, we calculated the pooled odds ratio (OR) and 95% CIs using the same methodology. Publication bias was not assessed as the total number of studies in a given meta-analysis was <10. Subgroup analyses (such as by study design) were not performed due to the limited number of studies. All analyses were performed using Stata v18·0 (Stata Corp, College Station, TX, USA). A P < .05 was considered statistically significant for overall and subgroup effects.
Results
Review of Existing Literature
The electronic research initially yielded a sum of 9987 citations. After excluding the duplicates, a tally of 9740 records remained. Following an extensive and rigorous title and abstract screening, a total of 9 articles were obtained for full-text analysis, out of which only 7 met our inclusion criteria and were relevant to our objective.1 -3,6,14,21,22 Figure 1 shows the PRISMA flowchart that demonstrates the screening process.
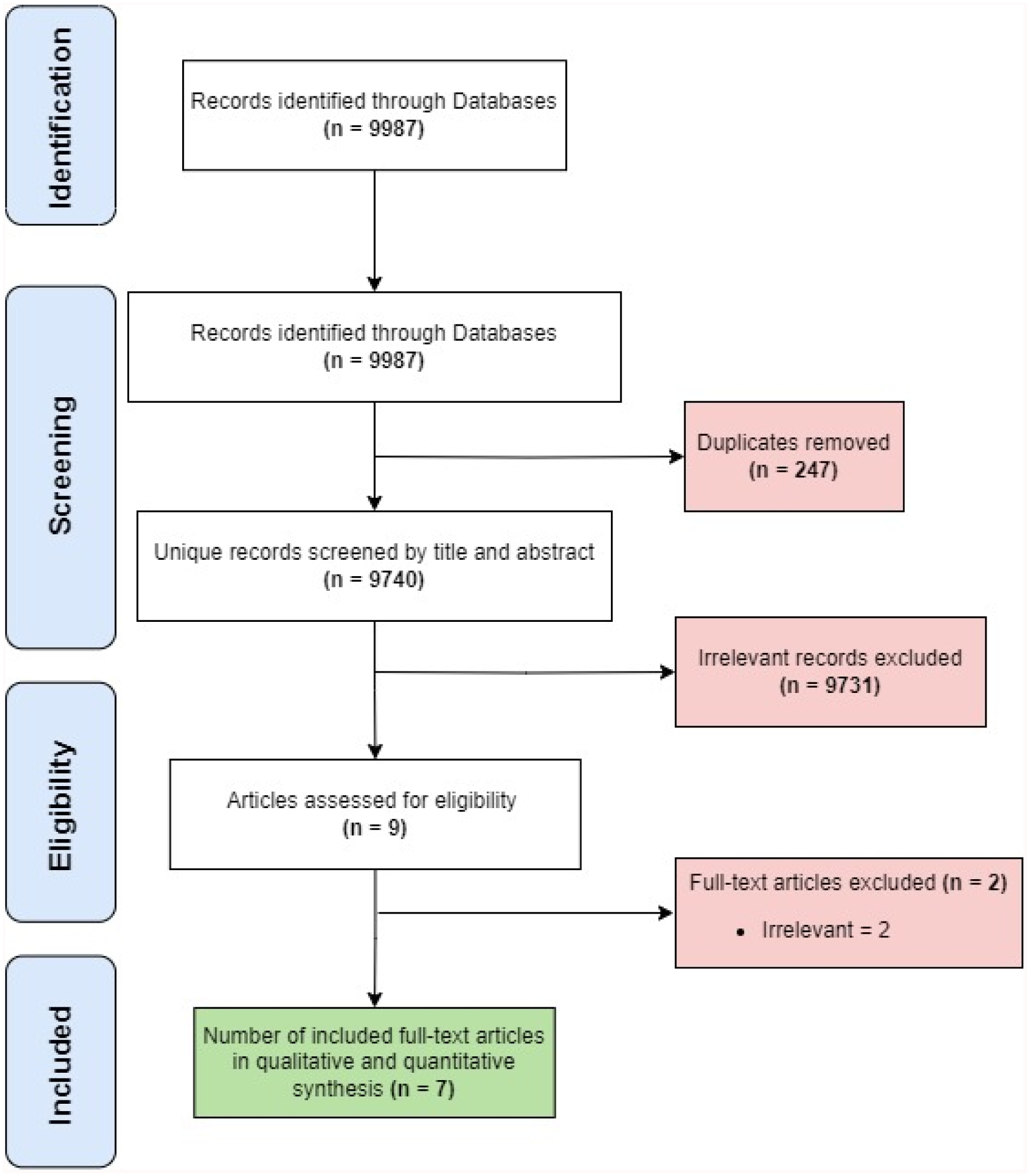
PRISMA flowchart of literature search and review. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analysis.
Characteristics of Included Studies
In total, we included 7 studies that compared the outcomes of endoscopic and microscopic management of attic cholesteatoma. Three of the studies included were RCTs, in which participants were randomly assigned into 2 groups: one undergoing the endoscopic approach and the other undergoing the microscopic technique.1,6,21 Moreover, 3 studies were conducted prospectively. In these studies, patients were divided randomly between the groups and were followed postoperatively.3,14,22 Lastly, 1 retrospective study was included. 2 A total of 539 patients (541 operated ears) were included. A summary of the included studies and the baseline characteristics of their patients is demonstrated in Table 1. Preoperative and intraoperative findings are reported in (Supplementary Table 1).
Characteristics of the Included Studies and Baseline Characteristics of Enrolled Patients.
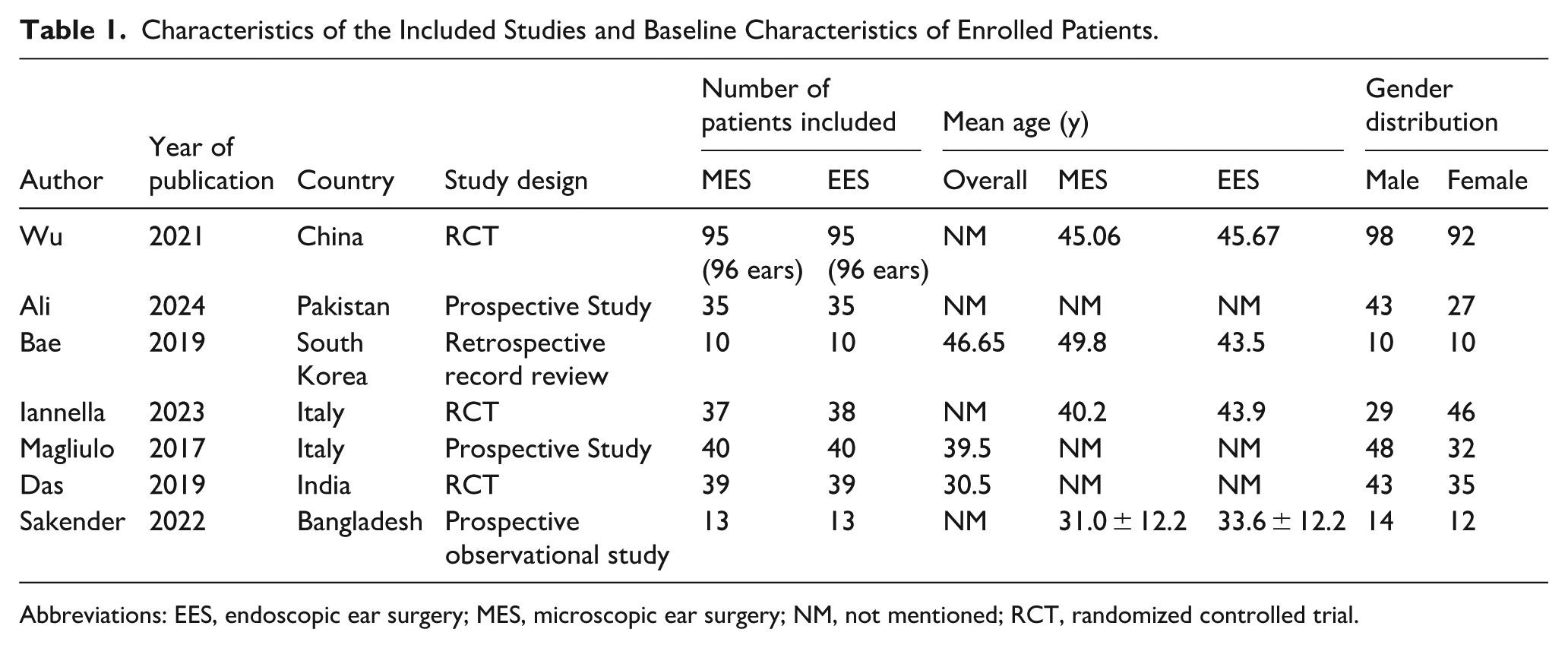
Abbreviations: EES, endoscopic ear surgery; MES, microscopic ear surgery; NM, not mentioned; RCT, randomized controlled trial.
Quality of Included Studies
The 3 included RCTs1,6,21 were subjected to the RoB 2 for quality assessment (Supplementary Table 2). 19 The overall risk of bias for the 3 studies was low risk. The other 4 included studies were subjected to quality assessment using the MINORS criteria, and the mean total score was 18.75 (14-21). 20 All 4 studies were of moderate to good quality (Supplementary Table 3).
Outcomes
Operating Time
Operating time was assessed by 5 studies, 4 of them reported statistical significance. Wu et al noted that the microscopic group on average consumed 105.833 ± 14.19 minutes, while the endoscopic group consumed 93.75 ± 9.97 minutes (P < .05). 1 Similarly, Das et al found that the microscopic group had a higher average than that of the endoscopic group, 143.4 ± 9.97 and 122.833 ± 16.69 minutes, respectively (P < .05). 21 On the other hand, Ali et al and Magliulo and Iannella reported longer operating time in the endoscopic groups. In their study, Ali et al reported that the microscopic group averaged 69.8 ± 8.48 minutes while the endoscopic group averaged 87.7 ± 11.7 minutes (P < .0001). 14 Likewise, Magliulo and Iannella reported that the endoscopic group needed 87.8 ± 11.9 minutes on average, and the microscopic group needed 69.7 ± 8.49 minutes one average (P < .0001). 22 Bae et al and Iannella et al reported no statistical difference in the operating time between both groups.2,6 Details of the operating time are reported in Supplementary Table 4. There was a high degree of heterogeneity among the studies with I2 value of 97.6% (MD = 1.122, 95% CI = −13.687 to 15.930, I2 :97.6%, P < .0001; Figure 2). The pooled analysis for overall effect showed no statistically significant difference in the surgical duration among both groups (Z = 0.148, P = .882).
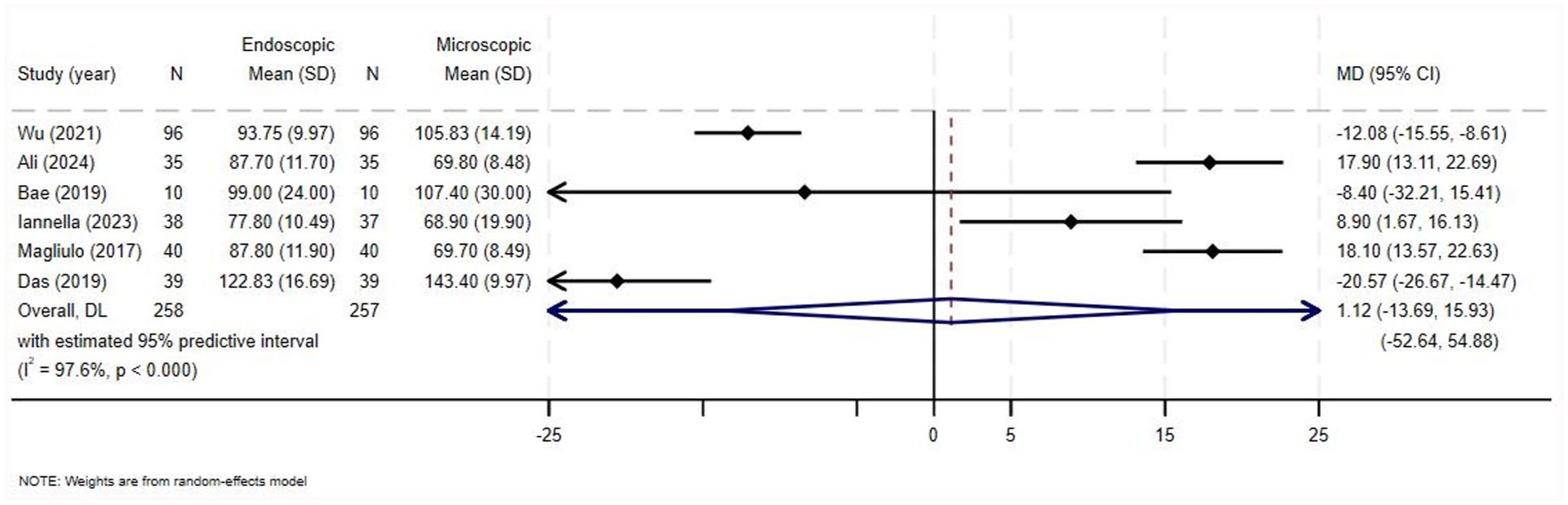
Forest plot for operating time.
Middle Ear Structure Visibility
Middle ear structure visibility was only assessed by 2 articles using the MESVI,1,21 which collectively included 270 patients. Wu et al reported that the median MESVI in the microscopic group was 4 (range 3-8) in comparison to the endoscopic group, which had a higher median score of 8 (range 3-10), with a statistically significant difference (P < .05). 1 Similarly, Das et al reported a statistically higher median in the endoscopic group compared to the microscopic group, 8 (range 3-10) and 4 (range 3-8), respectively (P < .0001; Supplementary Table 5). 21 No heterogeneity among the included studies was noted (MD = 3.59, 95% 3.29-3.90, I2 = 0%, P = .468; Figure 3). The pooled analysis for the overall effect showed that MESVI was higher in the endoscopic group compared to the microscopic group (Z = 23.205, P < .0001).
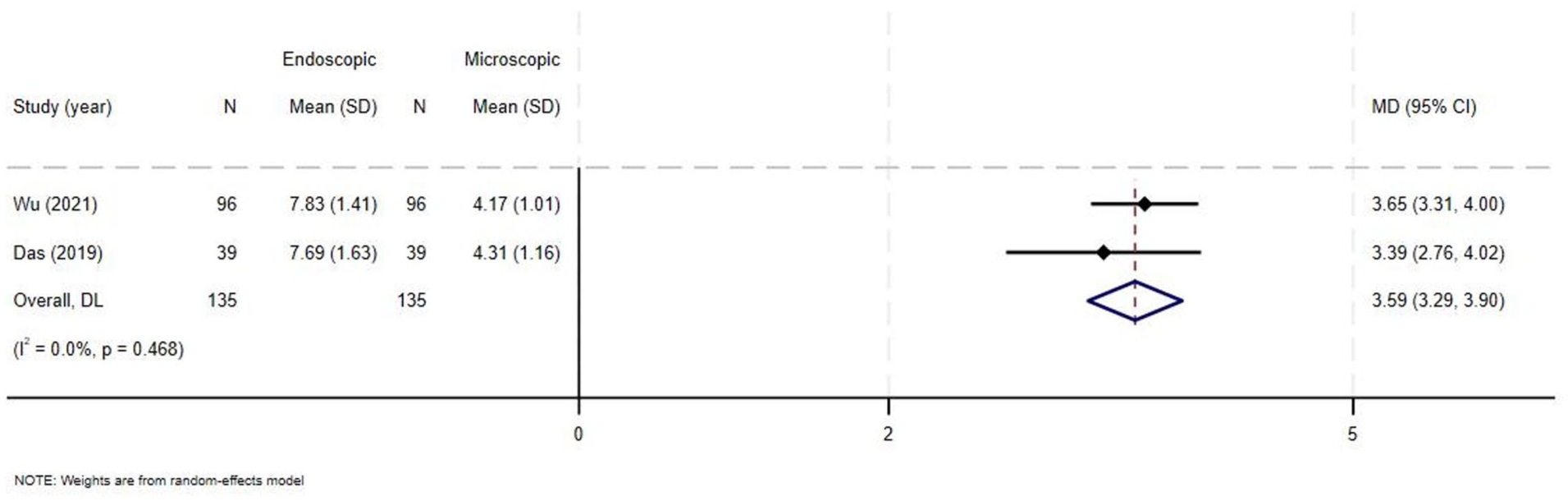
Forest plot for middle ear structure visibility.
Postoperative Taste Sensation Abnormalities
Postoperative taste sensation abnormalities were evaluated by 5 studies, collectively including 443 ears, and all were included in the meta-analysis.1,3,6,14,22 Ali et al, Iannella et al, and Magliulo and Iannella reported a higher percentage of postoperative taste sensation abnormalities occurring in the microscopic group compared to the endoscopic group, while Wu et al and Sakender and Rahaman reported a higher percentage in the endoscopic group. However, none of the studies reported statistically significant differences (Supplementary Table 6). No heterogeneity of the OR was noted among the included studies (OR = 0.77, 95% CI = 0.48-1.23, I2 = 0%, P = .650; Figure 4). The pooled analysis for overall effect showed no statistically significant difference among both groups (Z = −1.093, P = .274).
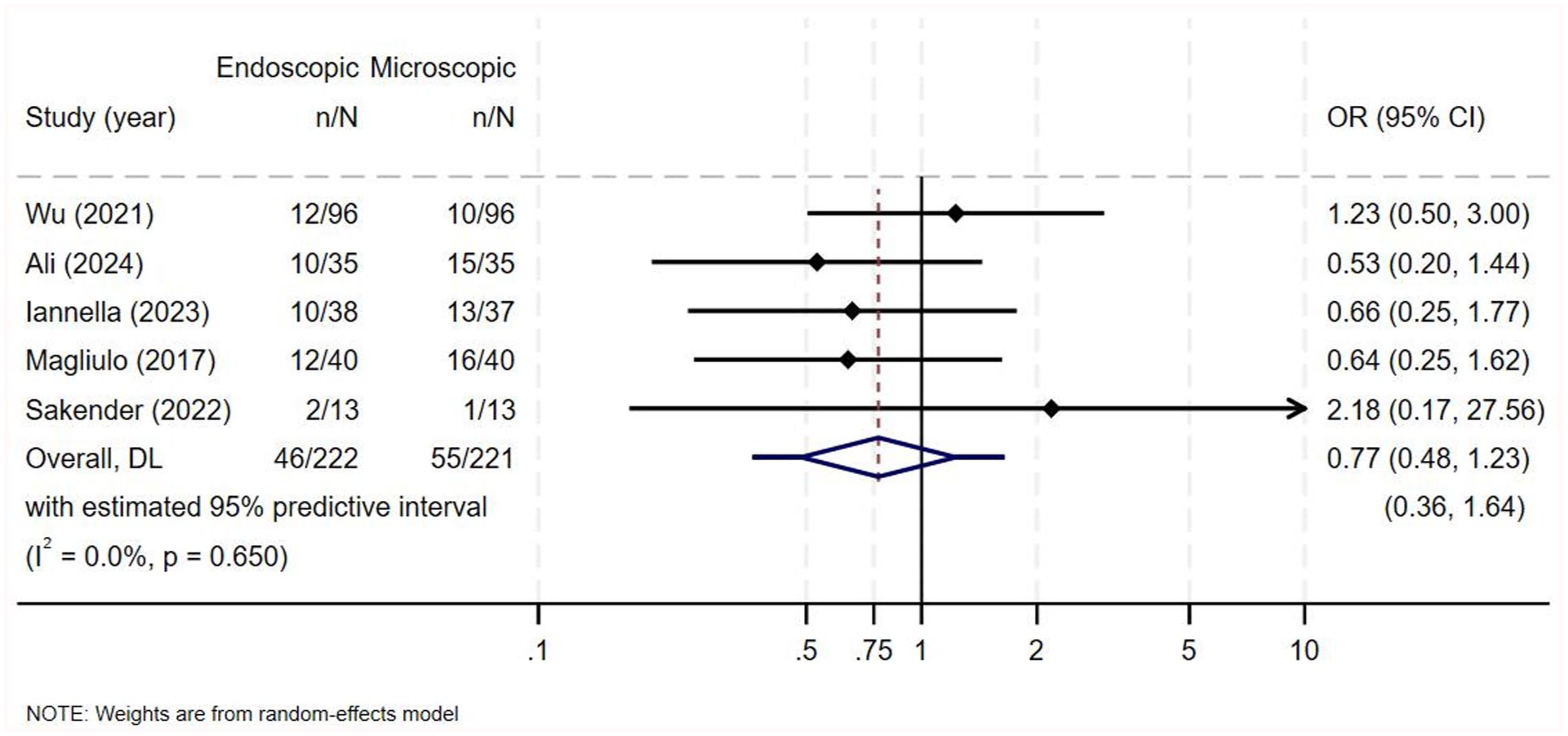
Forest plot for taste sensation abnormalities.
Postoperative Vertigo/Dizziness
Postoperative vertigo/dizziness was evaluated in 6 of the included studies.1,3,6,14,21,22 However, in their RCT, Das et al only mentioned that no significant difference was found between the 2 groups in terms of postoperative vertigo without mentioning the number of patients affected. 21 Consequently, that study was excluded from the meta-analysis. The meta-analysis included 443 ears from 5 studies.1,3,6,14,22 All of the included studies reported a higher percentage of patients experiencing postoperative vertigo/dizziness in the microscopic group compared to the endoscopic group. Nevertheless, none of the studies reported statistically significant differences (Supplementary Table 7). No heterogeneity of the OR was noted among the included studies (OR = 0.545, 95% CI = 0.276-1.075, I2 = 0%, P = .723; Figure 5). The pooled analysis for overall effect showed no statistically significant difference among both groups (Z = −1.752, P = .080).
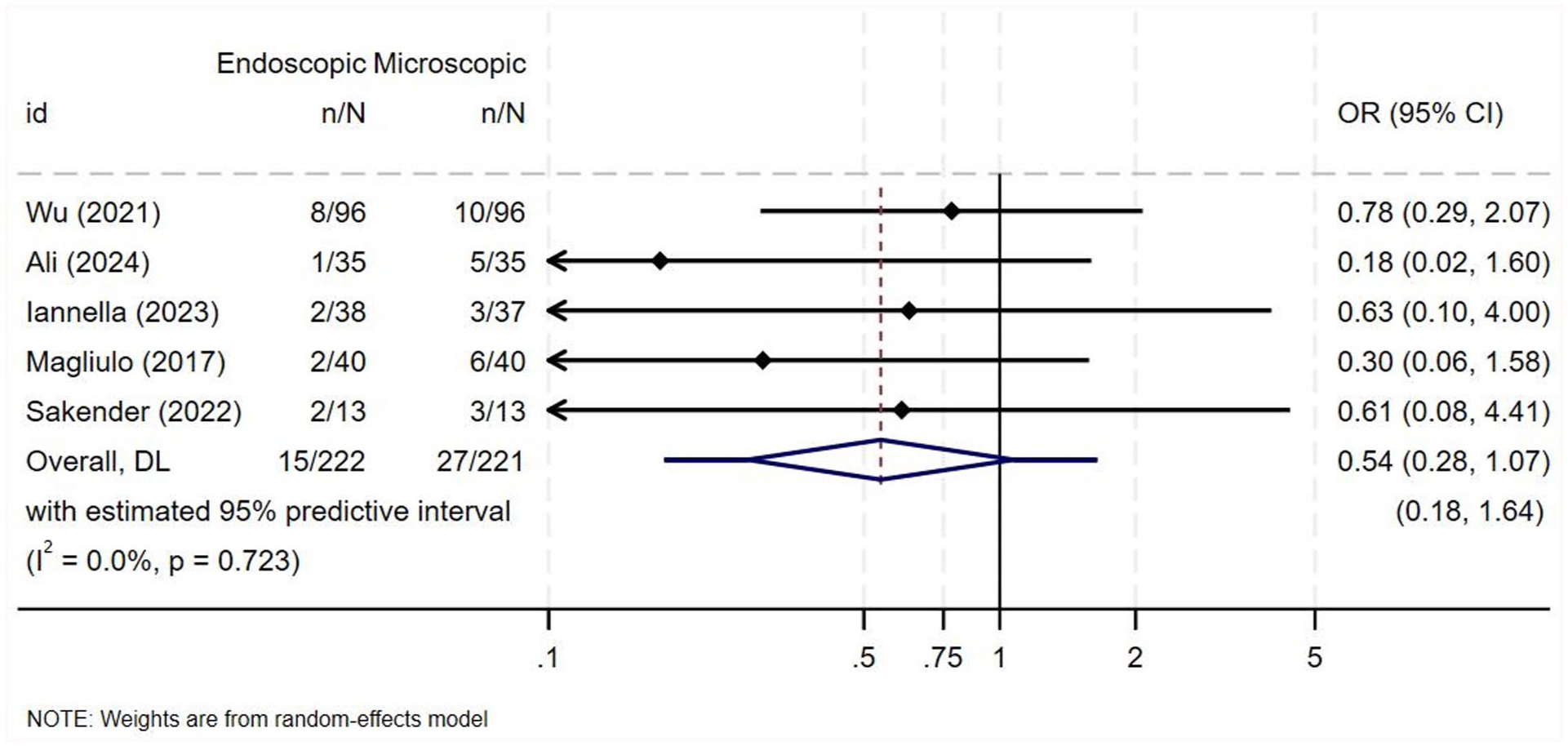
Forest plot for postoperative vertigo and dizziness.
Average Healing Time
Healing time was given as the mean with standard deviation in 4 studies, which collectively included data on 417 ears, all of which were incorporated into the quantitative analysis.1,6,14,22 Wu et al and Iannella et al reported similar results among both groups without a statistically significant difference.1,6 In contrast, Ali et al and Magliulo and Iannella reported that the healing time was significantly shorter among patients in the endoscopic group as compared to the microscopic group14,22 (Supplementary Table 8). There was a high degree of heterogeneity among the studies (MD = −5.185, 95% CI = −12.280 to 1.911, I2 = 93.4%, P < .0001; Figure 6). The pooled analysis for overall effect showed no statistically significant difference in the average healing time among both groups (Z = −1.432, P = .152).
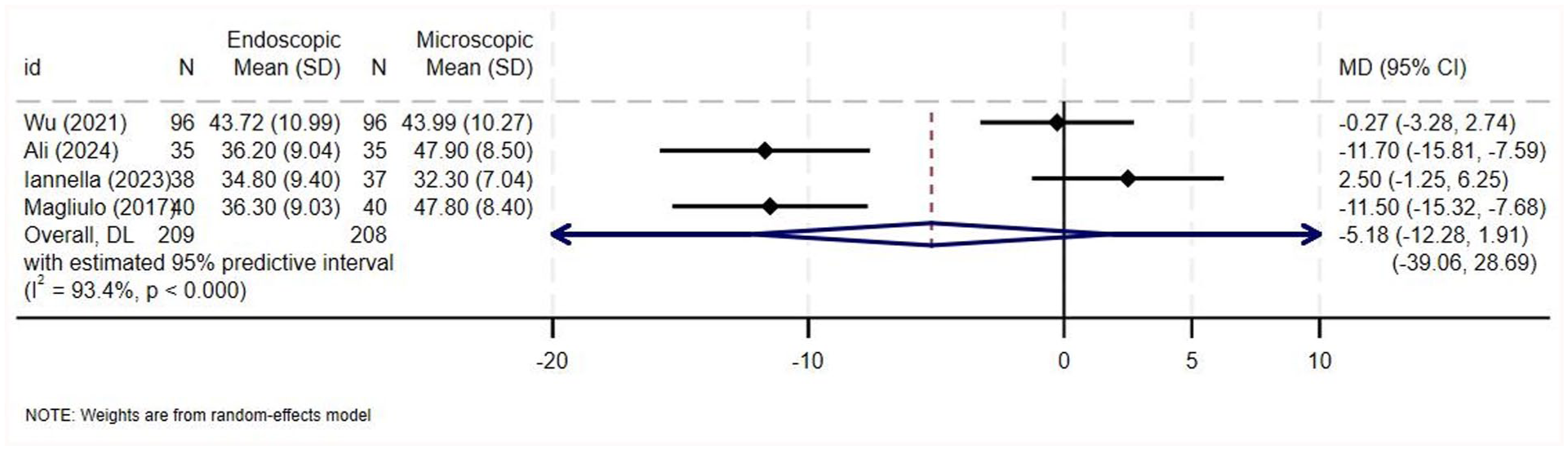
Forest plot for healing time.
Hearing Outcome
All 7 included studies evaluated the hearing outcomes in terms of air-bone gap closure and/or postoperative air-conduction thresholds.1 -3,6,14,21,22 All of the included studies reported no significant difference in the audiological outcome between both surgical approaches.1 -3,6,14,21,22 Three studies provided data on the audiological outcome as air-bone gap closure and were thus included in the quantitative analysis (238 ears).1 -3 Data on air-bone gap closure from 238 ears across the 3 studies is demonstrated in Supplementary Table 9. There was weak heterogeneity among the studies (MD = −0.028, 95% CI = −0.767 to 0.712, I2 = 25.2%, P = .262; Figure 7). The pooled analysis for overall effect showed no statistically significant difference among both groups (Z = −0.073, P = .941).
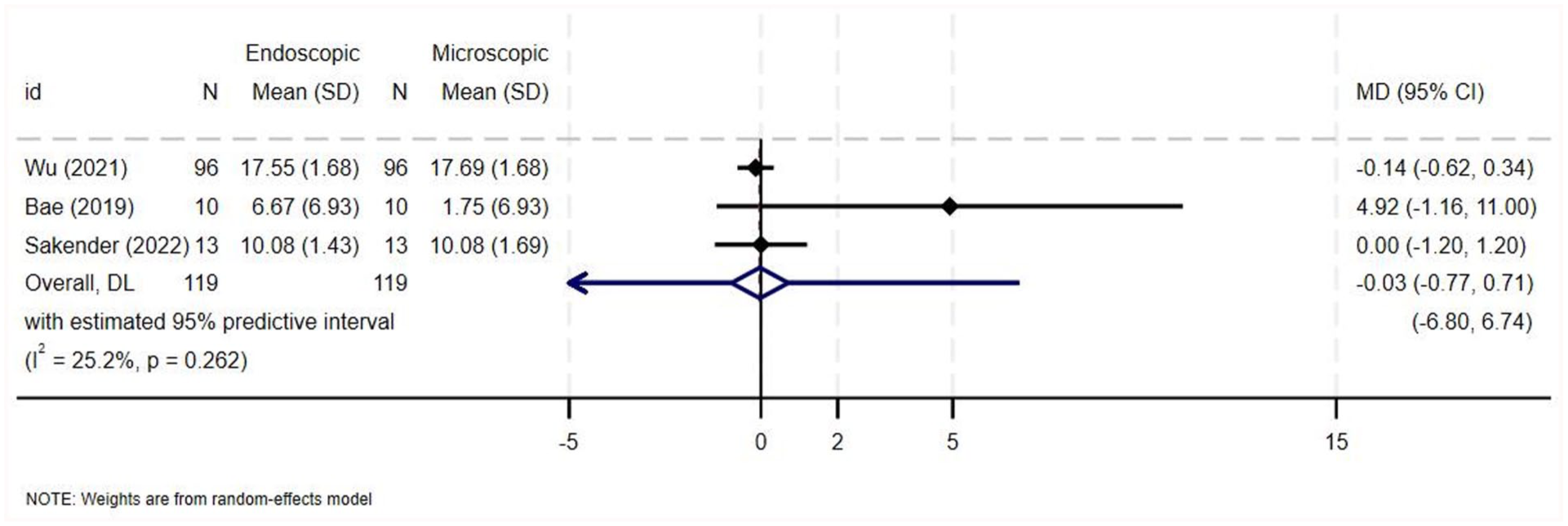
Forest plot for air-bone gap closure.
Postoperative Pain
Data pertaining to postoperative pain were reported by 6 studies. Four out of the 6 studies assessed pain only using a patient report-based classification that classified pain using 3 grades: almost no pain, mild pain requiring no analgesics, and pain requiring analgesic drugs.3,6,14,22 One study by Wu et al used the same classification, in addition to a numerical rating scale at 6 hours postoperatively. 1 Das et al, on the other hand, only used the numerical rating scale at 6 hours postoperatively. 21 All 6 studies demonstrated a higher number of patients with postoperative pain requiring analgesics and/or a higher pain score in the microscopic groups, as demonstrated in Supplementary Table 10. Five out of the 6 studies reported that the higher proportion of pain in the microscopic groups was statistically significant,1,3,14,21,22 while Iannella et al reported that the difference was not statistically significant. 6 In terms of the number of patients requiring analgesia postoperatively, there was moderate heterogeneity among the studies (OR = 0.10, 95% CI = 0.03-0.41, I2 = 53%, P = .074; Figure 8) and the pooled analysis for overall effect revealed higher postoperative pain among patients in the microscopic group (Z = −3.207, P = .001). In terms of the postoperative pain on a numerical rating scale, there was a high degree of heterogeneity among the studies (MD = −2.075, 95% CI = −2.661 to −1.489, I2 = 76.7%, P = .038; Figure 9) and the pooled analysis for overall effect revealed higher postoperative pain among patients in the microscopic group (Z = −6.942, P = .000).
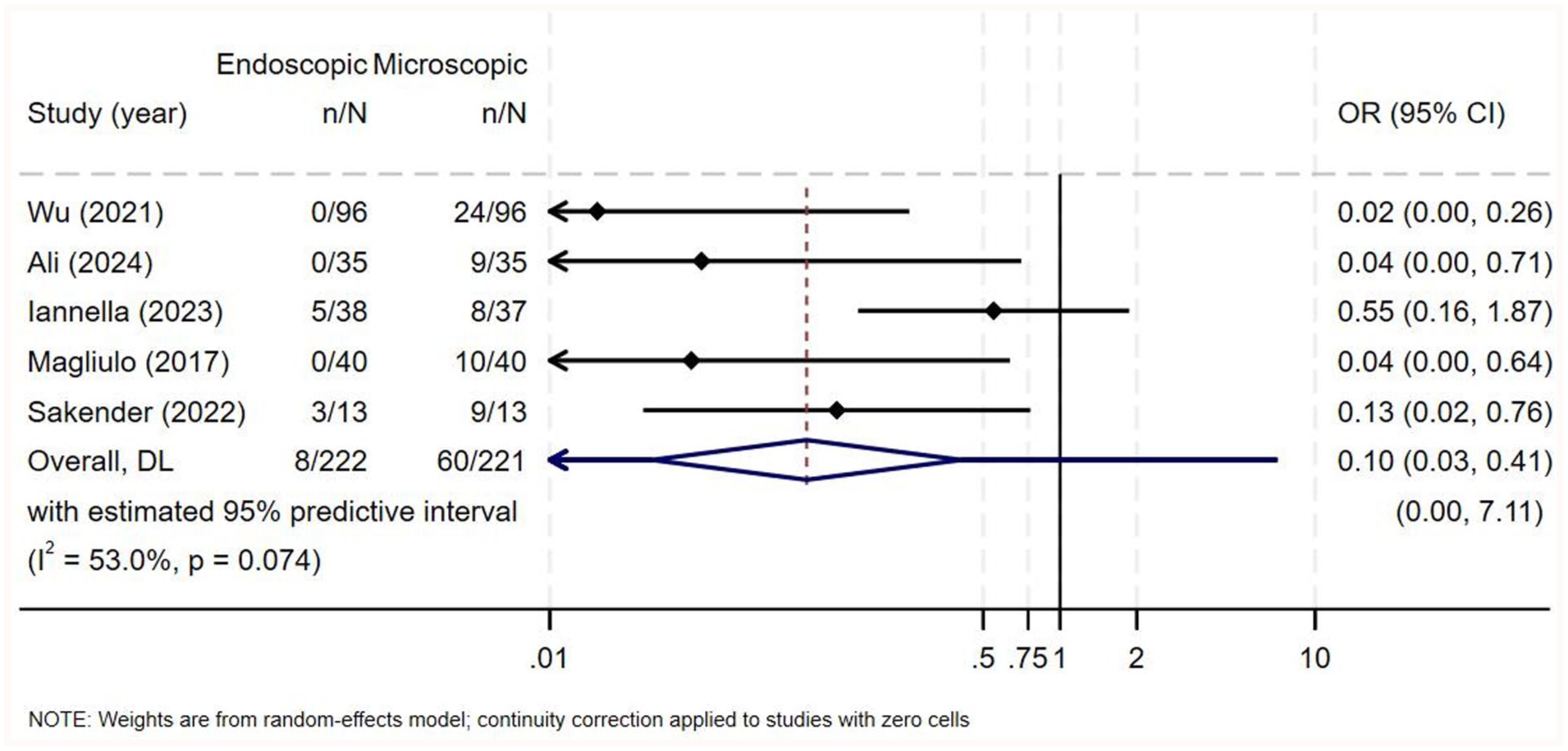
Forest plot for postoperative pain (number of events requiring analgesics).
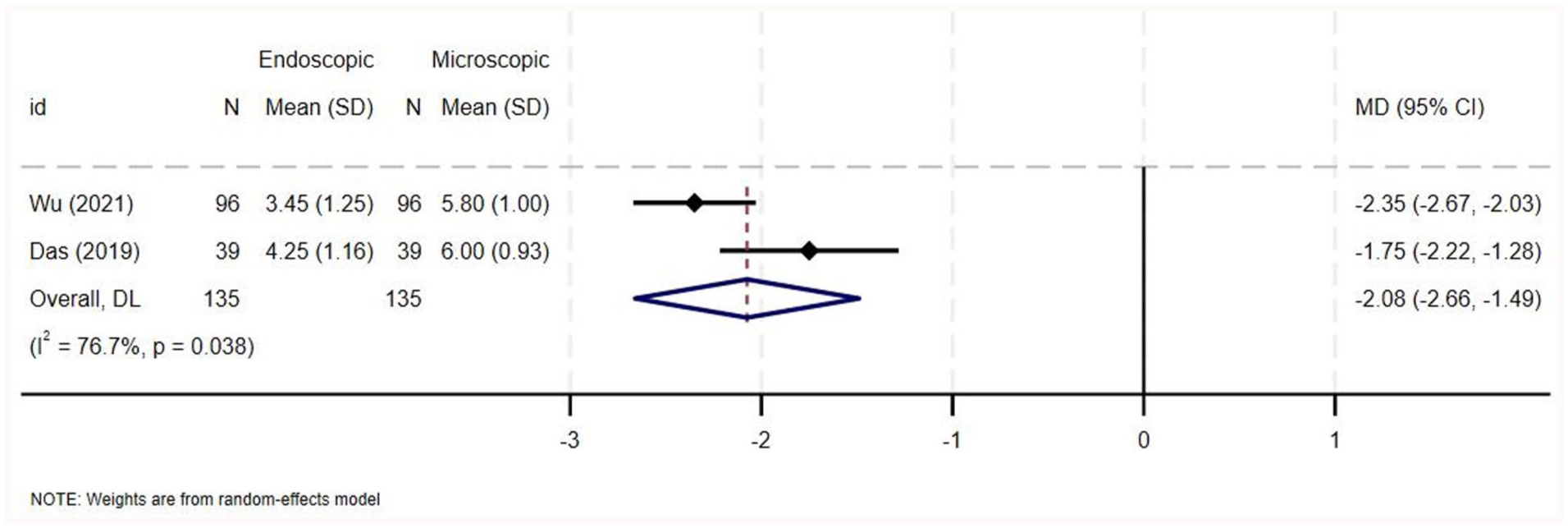
Forest plot for postoperative pain (pain score on a numerical scale).
Long-Term Outcomes
Six out of the 7 studies provided data on disease recurrence.1,2,6,14,21,22 Four out of the 6 studies reported no disease recurrence in either group during their follow-up periods.2,6,14,22 Wu et al reported 4 cases of recurrence in the patients who underwent the endoscopic approach and 5 cases of recurrence in the microscopic group. 1 Das et al reported 1 case in the endoscopic group and 2 cases in the microscopic group. 21 All 6 studies reported that there was no statistically significant difference in the recurrence rate between both groups (Supplementary Table 11).
Two out of the 7 studies provided data on residual disease.2,22 Both studies reported no residual disease in both groups without a statistically significant difference both groups (Supplementary Table 11).
Two out of the 7 studies provided data on other long-term outcomes, namely displacement of cartilage, perforation, and retraction pocket formation.1,21 Displacement of cartilage and retraction pocket formation occurred more commonly in the microscopic group in both studies.1,21 Perforation occurred more commonly in the microscopic group in the study by Wu et al, 1 while it occurred in 1 patient in each group in the study by Das et al. 21 None of the differences between both groups in the occurrence of these complications was statistically significant (Supplementary Table 11).
Discussion
The main principle of the surgical management of middle ear cholesteatoma is extensive disease removal as well as reconstruction of hearing. Essential factors for successful surgical and patient-related outcomes include preservation of normal mucociliary function, clearance of the ventilation pathway of the middle ear and mastoid and improved hearing outcome. Thus, the principal disadvantage of the conventional microscopic approach is the visualization of hidden areas.8,16,17,23,24 Initially, endoscopes were used as an adjunct to overcome this drawback. 24 Nowadays, it has become more widely popular among otologists to perform totally endoscopic ear surgery in type I tympanoplasty and stapes surgery with comparable results to microscopic ear surgery.25,26 Yet, the question remains of whether totally endoscopic ear surgery could replace microscopic ear surgery for the management of middle ear cholesteatoma limited to the attic. This systematic review and meta-analysis were performed for the purpose of assessing and comparing the structural, functional, and quality of life outcomes between the microscopic and endoscopic approaches for the management of middle ear cholesteatoma limited to the attic.
Middle ear structure visibility was assessed objectively using the MESVI in 2 RCTs.1,21 The pooled analysis for the overall effect showed that the endoscopic group had a greater MESVI than the microscopic group. This indicates that endoscopic approach is preferable in terms of improved visualization and assessment of concealed areas.1,21 Enhancing visualization has a major impact on important outcomes, such as the rate of disease recurrence and residual disease. It also affects the ability to visualize structures from multiple perspectives and the willingness to sacrifice additional bone. This finding is consistent with other previous studies, which demonstrated that endoscopic approach has a superior advantage in regard to visualization of the middle ear structures.8,16,17
The analysis of disease recurrence data is particularly important, as it directly speaks to the long-term efficacy of the 2 surgical approaches. Factors that affect the structural outcome leading to disease recurrence and/or residual disease include incomplete disease removal, failure to clear the middle ear ventilation pathway, and excessive mucosal damage.24,27 -29 The majority of included studies (4 out of 6) reported no disease recurrence in either the microscopic or endoscopic groups during follow-up.2,6,14,22 This is an encouraging finding, suggesting both techniques can achieve durable disease control. The 2 remaining studies that reported some recurrence found no statistically significant difference in recurrence rates between the groups.1,21 Likewise, the included studies that provided data on residual disease reported no cases in either group.2,22 These consistent findings across the majority of studies strengthen the conclusion that the surgical approach does not have a significant impact on the risk of disease recurrence and residual disease in limited attic cholesteatoma, despite the potential advantages often attributed to the endoscopic technique.
Hearing improvement is an essential functional outcome and an important measure for the efficacy of the surgical technique. Studies have shown that ossicular preservation is higher in the endoscopic approach with 42% compared to 10% in the microscopic approach.2,30,31 The endoscopic approach has the advantage of improved visualization of the ossicular chain and the preservation of normal mastoid air cells, which leads to better hearing outcomes. 24 Nevertheless, the findings of audiological outcomes in our systematic review, such as air-bone gap closure and postoperative air-conduction thresholds, present a clear and consistent picture. All 7 studies reported no significant difference between the microscopic and endoscopic approaches.1 -3,6,14,21,22 The quantitative analysis, including data of postoperative air-bone gap closure from 238 ears across 3 studies, further corroborated this finding.1 -3 The pooled analysis for the overall effect demonstrated a statistically nonsignificant difference in average air-bone gap closure between the 2 techniques.1 -3 These results suggest that both approaches are equally effective in achieving optimal postoperative audiological outcomes.
As the endoscopic technique is minimally invasive, it aligns with the goal of achieving less postoperative pain, decreased length of hospital stay, faster recovery, and earlier return to daily routine. Moreover, there is no need for a head shave, mastoid bandage, or a visible post-aural scar, leading to a better cosmetic outcome.32 -35 In comparison with the endoscopic approach, the microscopic approach demonstrated a higher incidence of postoperative pain requiring the use of analgesia and a higher pain score. This difference was statistically significant in 5 out of the 6 studies, with only Iannella et al finding it to be nonsignificant.1,3,6,14,21,22 The reason for this finding is that endoscopic procedures are less invasive with minimal tissue dissection and a transcanal approach, causing less tissue trauma than microscopic procedures, which involve larger skin incisions and greater tissue manipulation. A similar finding was presented by Choi et al, who found that the endoscopic group had significantly lower pain levels 1 day after surgery than the microscopic group, which could be attributed to the external incision and the external auditory canal bone drilling in the microscopic approach. 36 The evidence on postoperative healing time presents a nuanced picture. While Wu et al and Iannella et al found comparable average healing durations between the approaches, Ali et al and Magliulo and Iannella reported significantly shorter healing times with the endoscopic technique.1,6,14,22 The high heterogeneity (I2 = 93.4%) suggests that the healing process may be influenced by a complex interplay of factors, including surgical expertise, patient characteristics, and postoperative management. The pooled analysis for the overall effect did not identify a statistically significant difference in average healing time between the 2 approaches. This unexpected finding indicates that the surgical approach may not be the primary driver of postoperative healing outcomes, highlighting the multifactorial nature of the healing process.
Wu et al and Das et al reported that the microscopic approach had longer average operating times compared to the endoscopic approach, while Ali et al and Magliulo and Iannella found the opposite, with the endoscopic approach taking longer.1,14,21,22 The high heterogeneity observed (I2 = 97.6%) suggests significant variability in factors influencing operating time, such as surgeon experience, surgical technique, patient characteristics, and procedural details. 1 Importantly, the pooled analysis for the overall effect did not find a statistically significant difference in surgical duration between the microscopic and endoscopic groups. This indicates that the operating time may not be a key differentiating factor between the 2 approaches, possibly due to the learning curve associated with each technique and the complexity of the procedures.
Complications after cholesteatoma surgery are generally considered few and rare. We identified discrepancies between the included studies on the postoperative taste abnormalities; however, none of these studies found any statistical significance.1,3,6,14,22 The fact that neither of the approaches clearly outperforms the other in terms of taste results indicates that both approaches can be used safely without significantly affecting this crucial functional outcome. Regarding postoperative vertigo, our findings indicated that none of the studies showed statistically significant differences, even though a higher percentage of patients in the microscopic group than in the endoscopic group experienced postoperative vertigo or dizziness.1,3,6,14,22 Nevertheless, this should raise our concern that, despite the statistical insignificance, a microscopic approach may actually increase the possibility of developing a vestibular complication. As a result, a clinical evaluation and the vestibular background of the patient should always be taken into consideration.
Our findings of improved middle ear visibility and reduced postoperative pain with the endoscopic approach are consistent with the existing literature. Previous meta-analyses have similarly reported lower recurrence and residual rates, as well as reduced postoperative discomfort with endoscopic surgery, while showing no significant differences in graft uptake, audiological outcomes, or operative times compared to microscopic techniques. Together, these results support the growing evidence that endoscopy offers specific advantages, particularly in visualization and patient comfort, without compromising surgical efficacy.7,24
Strengths and Limitations
Despite the variability in the study designs, all the included studies offered direct comparisons of the outcomes between both surgical approaches. The findings of this systematic review and meta-analysis provide valuable insights into the comparative outcomes of endoscopic and microscopic management of attic cholesteatoma.
The limitations of this study include the small sample size of the included studies, potentially leading to limited statistical power and the inability to detect small differences between the 2 techniques. In addition, the data gathering process may have been affected by confounding variables, such as variations in surgical experience, patient characteristics, and follow-up durations across the included studies. Most studies were conducted by authors who are endoscopic surgeons who performed total endoscopic surgeries and compared the results to the microscopic approach, possibly leading to inherent reporting bias. Furthermore, the high heterogeneity observed in operative and healing times (I² > 90%) can likely be attributed to several factors. One key source is the variation in surgical techniques across studies—particularly the use of single-handed versus bimanual endoscopic approaches, which can significantly impact operative efficiency and precision. Additionally, differences in surgeon experience and the learning curve associated with endoscopic techniques may have contributed to the variability, as procedures performed during the early adoption phase may take longer and result in slower healing. These factors collectively contribute to the substantial heterogeneity observed and highlight the need for more standardized reporting and technique descriptions in future studies. Also, the follow-up periods in the included studies were generally inadequate for assessing long-term outcomes. This limits the ability to draw conclusions about recurrence rates and delayed complications, which are crucial in evaluating the long-term efficacy of cholesteatoma surgery. The lack of studies with follow-up beyond 5 years is a notable limitation and highlights the need for future research with extended follow-up to provide more robust outcome data.
Recommendations
With appropriate training and skill with the endoscopic technique, it is the preferred approach for cholesteatoma limited to the attic region, considering the definite advantages it offers. Based on the findings and limitations of this review, we recommend conducting larger, well-designed, and comparative prospective studies to further investigate the comparative outcomes of endoscopic and microscopic management of attic cholesteatoma. These studies should aim to control for potential confounding variables and employ standardized outcome measures to provide more robust and reliable evidence to guide clinical practice.
Conclusion
The endoscopic approach for the management of cholesteatoma limited to the attic region has some advantages compared to the microscopic approach, namely in terms of better middle ear structures visibility and less postoperative pain. No significant differences between both approaches were noted in terms of residual disease and disease recurrence. Likewise, no significant differences in the operation time, average healing time, and audiological outcome between both approaches were found. Future research conducted with high-quality comparative prospective studies is needed to further compare both surgical approaches and confirm the advantages of the endoscopic approach.
Supplemental Material
sj-docx-1-ear-10.1177_01455613251391550 – Supplemental material for Comparison of Endoscopic and Microscopic Management of Attic Cholesteatoma: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-ear-10.1177_01455613251391550 for Comparison of Endoscopic and Microscopic Management of Attic Cholesteatoma: A Systematic Review and Meta-Analysis by Hassan Alalawi, Mohammed Bahabri, Marwah Alqathmi, Kholoud Alsiwed, Abdullah F. Alharbi, Maha Ahmed Alzahrani, Abdulmajeed Alhindi, Ramesh Vishwakarma and Hosam A. Amoodi in Ear, Nose & Throat Journal
Supplemental Material
sj-docx-2-ear-10.1177_01455613251391550 – Supplemental material for Comparison of Endoscopic and Microscopic Management of Attic Cholesteatoma: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-2-ear-10.1177_01455613251391550 for Comparison of Endoscopic and Microscopic Management of Attic Cholesteatoma: A Systematic Review and Meta-Analysis by Hassan Alalawi, Mohammed Bahabri, Marwah Alqathmi, Kholoud Alsiwed, Abdullah F. Alharbi, Maha Ahmed Alzahrani, Abdulmajeed Alhindi, Ramesh Vishwakarma and Hosam A. Amoodi in Ear, Nose & Throat Journal
Supplemental Material
sj-docx-3-ear-10.1177_01455613251391550 – Supplemental material for Comparison of Endoscopic and Microscopic Management of Attic Cholesteatoma: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-3-ear-10.1177_01455613251391550 for Comparison of Endoscopic and Microscopic Management of Attic Cholesteatoma: A Systematic Review and Meta-Analysis by Hassan Alalawi, Mohammed Bahabri, Marwah Alqathmi, Kholoud Alsiwed, Abdullah F. Alharbi, Maha Ahmed Alzahrani, Abdulmajeed Alhindi, Ramesh Vishwakarma and Hosam A. Amoodi in Ear, Nose & Throat Journal
Footnotes
Acknowledgements
We would like to express our sincere gratitude to Dr Anas S. Alyazidi for his assistance with this research project.
Ethical Considerations
Ethics approval from the institutional review board was not required for this study, as it is a systematic review of previously published data.
Author Contributions
H.A., M.B., and H.A.A. contributed to the study concept and design. H.A., M.B., M.A.A., K.A., and A.F.A. contributed to data search, analysis, and interpretation. R.V. contributed to study design and statistical analysis of the data. All authors contributed to manuscript drafting. H.A., M.A.A., and H.A.A. contributed to the critical revision of the manuscript. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The relevant data of this study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.