
Abstract
Objectives:
Endoscopy has become routinely used in middle ear surgery. The aim of this study is to analyze where this tool may complement the traditional microscopic approach. This is a retrospective study done in single tertiary hospital.
Methods:
We reviewed 342 middle ear/petrous bone surgical procedures performed between 2005 and 2015. Only cases in which both microscopic and endoscope-assisted techniques were used have been included. Sixty-six patients received this double-technique surgery: 51 (77.2%) had middle ear/mastoid and petrous bone cholesteatomas (46 middle ear and mastoid and 5 acquired/congenital petrous bone cholesteatomas), 5 (7.5%) had glomus tympanicum tumors (GTT), 4 (6%) had an ossicular chain dislocation, 3 (4.5%) had purulent chronic otitis media, 2 (3%) had tympanosclerosis, and 1 (1.5%) had an ossicular chain malformation.
Results:
The endoscope was helpful to remove disease remnants not accessible by microscope in 41 (62%) of the cases; 37 (90%) were cholesteatomas, 3 (7%) were GTT, and only 1 (3%) was an open tympanosclerosis. In the remaining 25 (37.8%) cases, the endoscope was useful only to visualize the cavity since the microscope had already been successful in removing the entire lesion.
Conclusions:
The endoscopy can add valuable information and support to the usual microscope approach alone. The consensus of a single best technique does not yet exist, but the physician should choose the best modality or combination of modalities in order to cure the patient and prevent any possible complications or recurrence of the pathology.
Introduction
The microscope was introduced to middle and inner ear surgery in the 1950s, but endoscopy entered into the surgical routine more recently. At first, the endoscope was used as a complementary tool to the microscope to inspect the surgical field1,2 and later it started to be applied as the main magnification tool 3 for the entire surgical procedure. From 2004, we integrated the use of the microscope and the endoscope in order to obtain the optimal results of reducing the invasiveness into the middle ear and petrous bone surgery. 4
The aim of this study is to define in which cases the 2 methods may be applied. We propose a decision tree that will guide the otology surgeon in choosing the best approach to the middle ear and the petrous bone pathologies, taking into consideration both localization and extent of the disease.
Patients and Methods
We reviewed 344 middle ear and petrous bone surgical procedures performed between 2004 and 2015. The inclusion criteria of this study, approved by Humanitas Clinical and Research Hospital Ethical Committee, were pathologies operated on by use of both microscope and endoscope-assisted techniques. Of all, 66 (28 men and 38 women) patients received this double-technique surgery. Of these, 51 (77.2%) had middle ear/mastoid and petrous bone cholesteatomas (46 middle ear and mastoid cholesteatomas and 5 acquired/congenital petrous bone cholesteatomas), 5 (7.35%) had glomus tympanicum tumors (GTT), 4 (5.88%) had ossicular chain dislocation, 3 (4.41%) had purulent chronic otitis media, 2 (2.94%) had tympanosclerosis, and 1 (1.47%) had an ossicular chain malformation.
Microendoscopic evaluation of the affected ear, high-resolution computed tomography, magnetic resonance (MR) of the temporal bones (only for petrous bone cholesteatoma cases), and pure-tone audiometry (PTA) were included in the preoperative assessment. Pure-tone audiometry evaluated changes in hearing levels at 250, 500, 1000, 2000, 4000, and 8000 Hz. bone as well as air conduction. The air–bone gap was higher than 15 dB in all of the cases except one which was only 5dB.
All procedures were performed under general anesthesia and began with the microscopic approach (Leica M400, Wetzlar; Germany). Only when the visual field of the microscope was insufficient to inspect the field and/or treat the disease, we shifted to the endoscope (3 mm 30° rod for the middle ear and 30° 4 mm rod for the petrous bone) with high definition camera and Xenon light (Karl Storz, Tutlingen; Germany).
In the middle ear cases, a bone conduction evaluation of each patient was performed to verify the preservation of hearing function the day after surgery and prior to discharge. Follow-up examinations by microendoscopic visualization of the external auditory canal and tympanic membrane, and PTA tests were performed at 2, 6, 12, and 18th month post operatively. Then, yearly examinations continued to be performed for all the middle ear cases. Also, in cases of petrous bone cholesteatomas, MR of the petrous bone was performed at 6, 12, 18 months postoperatively and then yearly thereafter as follow-up protocol.
Results
The endoscope was helpful to remove disease remnants not accessible by microscope alone in 41 (62.1%) cases. Of these, 37 (90%) were cholesteatoma cases, 3 (7%) were GTT cases, and only 1 (3%) was an open tympanosclerosis. In the remaining 25 (37.8%) cases, the endoscope was useful only to visualize the cavity since the microscope had already been successful in removing the entire lesion. In our series, one patient who was affected by an acquired petrous bone cholesteatoma surrounding the Fallopian canal had a postsurgical facial nerve palsy (House-Brackmann grade III) lasting around 1 year and resolving spontaneously. One patient had bouts of benign paroxysmal positional vertigo successfully treated with Semont maneuvers. Two patients experienced cholesteatoma recurrence. Of these, one was related to a petrous bone cholesteatoma that recurred at 18 months. The second, a 4-year-old female, received 3 microendoscopic surgeries for a massive and invasive cholesteatoma involving the mastoid and middle ear space. The first procedure took place in 2011. Then, in 2014, she was reoperated twice due to residual cholesteatoma within the fenestral area the first time, and in the hypotympanum and facial recess the second. This patient was noted to be disease free at 5 year follow-up. As the usefulness of the endoscope is linked to the anatomical position of the cholesteatoma, we have summarized the anatomical regions of the lesions in the cases where the endoscope was used (Table 1). In these region, the endoscope allowed to detect and remove the pathological tissue avoiding the extensive drilling and helping the reconstruction phase and results.
Anatomical Regions Where the Endoscope Was Used.
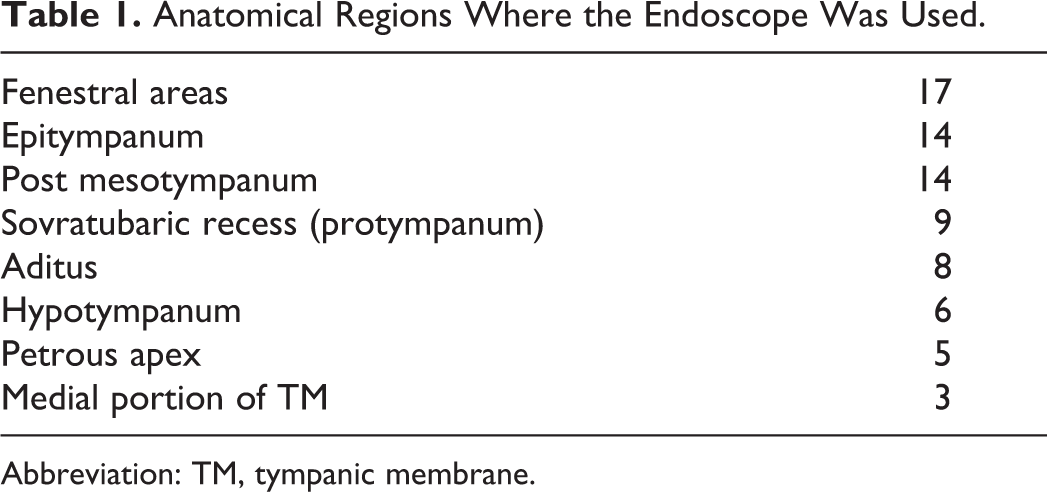
Abbreviation: TM, tympanic membrane.
Discussion
Over the last few decades, several authors,3-10 have shown that both microscopic and endoscopic techniques have advantages and drawbacks. We believe that the otosurgeon should understand these features and adopt the appropriate technique in each step of the surgery to reduce invasiveness without compromising optimal results. Furthermore, the anatomy of the middle ear structures should be protected, auditory function preserved, and operating times kept as short as possible with consequent reduction in length of admission and therefore cost. We have thus performed both microscopic and endoscopic middle ear surgery, and have refused any a priori tool-exclusive surgical procedure, be it microscope or endoscope, in cases where the extent of the disease requires the combined technique.
For cholesteatoma surgery, the pathology where the endoscope is most helpful, the microscopic endaural and transmeatal approaches alone may not be sufficient and the endoscope was used to complete the removal from the fenestral area, tympanic recess, and in all the cases in which the complete visualization of the aditus was not possible as in the presence of small epitympanum lesions. In these limited cases, the endoscope allows one to complete the work through the same natural corridor (external acoustic canal) without the need to perform mastoidectomy. For petrous bone cholesteatoma treatment, the ability to use the small corridor between the internal carotid artery, the posterior cranial fossa dura and the internal acoustic canal allows for a good visualization of the petrous apex. The longer operating time needed was compensated by the limited drilling for the petrosectomy.
Tarabichi,3,6 Migirov, 9 and Marchioni 10 showed all the advantages of the endoscope, and used it to perform all their surgical procedures of the middle ear cavity. Also, they stated the true advantages of this tool: seeing middle ear structures highly magnified, operating through the external ear canal with no retroarticular skin incision, being able to see pathological remnants even “around the corner” thanks to the endoscopes’ angled visual field, the absence of traumatic effect on healthy mastoid process bone, and reduced hospital stay with consequent cost reductions. However, the authors do acknowledge that the endoscope does not solve every problems. Some of these difficulties include difficulty of single-handed surgery, which requires experience and training, the distortion of the wide-angle view which causes loss of perception in the middle ear, the pseudo mini-invasiveness of the technique, and in the presence of a narrow external acoustic canal where this technique is not feasible. Lastly, by endoscopy, it is not possible to treat extended mastoid cholesteatomas.
The term minimally invasive surgery (MIS) of the middle ear by means of an exclusively endoscopic technique is perhaps misleading due to the fact that frequently, the tympanic membrane is detached from its natural position, and functional anatomy of the hearing system may be impaired. Minimally invasive surgery is a concept that not only involves the treatment by way of a small skin incision or through a natural opening. If a skin incision is used, it should to be minimal, of course, but to preserve and respect as much as possible the anatomy and function of the organ treated is more important. On the other hand, in a pure endoscopic approach, in order to have the proper surgical space, the detachment of the tympanic membrane from the handle of the malleus (destroying the so called stria malleolaris) is needed. This surely causes scar tissue formation that could worsens the physiologic transmission of movements of the tympano-ossicular chain, as studied and described by De Greef.11,12 It is important to remember that all of the structures present in the middle ear, namely, ossicles, ligaments, tendons, and membrane, are linked to each other by a very sharp and delicate balance, which must be preserved as much as possible in order to avoid even minimal conductive hearing loss.
Even so, also time and costs must be considered. Nowadays, it is common for hospitals to underline the importance of finding the most advantageous time/cost-quality ratio. In middle ear surgery, cost is related to the type of surgery planned, the hospital stay, and the cost of disposable materials used. There is a direct proportionality of the invasiveness of a surgery to the length of admission and cost. Therefore, a minimally invasive procedure should correlate to lower costs and shorter hospital stay in comparison to a more invasive approach.
Based on this group of patients, we propose the question: But are we absolutely sure that some of the procedures couldn’t be done by MIS using the microscope alone? In our experience, we are used to performing the myringoplasty endaurally (Figure 1): it is our preferred method if the canal is not too narrow or tortuous.
Completely endaural microscopic tympanoplasty (myringoplasty + ossiculoplasty).
In a narrow canal, it is not feasible to complete a microscopic approach but also, exclusive endoscopic use, could be very difficult if not impossible. In this situation, the retroauricolar approach with canal calibration becomes the only possibility. Moreover, the mastoid extension of the cholesteatoma requires extensive bone drilling which, in our opinion, results faster and easier bimanually and if possible using also the microscope. Here we underline that, in exclusively endoscopic endomeatal surgery, the surgical time is relatively longer and consequently so is the postsurgical hospital stay. In our series, patients were discharged at postoperative day 1, but for simple procedure, like endomeatal myringoplasty, the patient was discharged the day of surgery. Of course, in the case of combined microendoscopic approach, the helpfulness and usefulness of the endoscope obviously prolongs the surgical time, this is the price to invest to avoid further revision surgeries.
In 1993, Thomassin 1 introduced the concept of the usefulness of the endoscope in canal wall up (CWU) tympanoplasty that suffer of higher percentage of residual disease respect the canal wall down (CWD) 13 . He demonstrated that the cholestateoma recurrence rate dropped from 47% to 6% when using endoscopes during CWU procedures. In our experience, there were 2 cases of recurrences out of 66 patients. In both cases, the endoscope was used both for removing pathologic residual as well as for visualization of the cavity for visual verification of a disease free field which the microscope is not able to see. Anyway, the pathology recurred all the same. In these recurrences, we do not believe that the reason was in the technique itself but most probably in the anatomical complexity of the middle ear that may easily hide a pathologic lesion.
Therefore, we agree with Badr-el-Dine, 14 who states that incorporating the endoscope into the surgical armamentarium contributes to the (almost) complete removal of the pathology. Still in his study as in ours, it is obvious that, despite the introduction of the endoscope in conjunction with the operating microscope, 100% disease eradication of the pathology cannot yet be achieved.
Five out of 43 operated cases were found to have petrous bone cholesteatomas. These are growing in the petrous bone and can be primitive (congenital) or acquired from an extension of a middle ear cholesteatomas. 15 We treated the petrous bone cholesteatoma with partial petrosectomy using both microscope and endoscope in order to reduce the extent of bone drilling and to avoid, if at all possible, to manipulate the facial nerve. In these cases, the endoscope allowed us to achieve complete removal the cholesteatomas located in the petrous apex without performing facial nerve rerouting, reducing to almost zero the side effects due to its mobilization giving us control of the internal carotid artery for optimal removal of the pathology from its medial wall while respecting the nerve associated with the internal acoustic canal and the dura of the posterior and middle cranial fossa.
The only case of facial palsy we encountered (House Brackmann grade III) resolved in less than 12 months and was related to the cholesteatoma matrix surrounding the tympanic and mastoid tract of the nerve that required its manipulation for the removal and here is likely where the deficit arose. For this reason, we do not suggest to approach a petrous bone cholesteatoma endoscopically if the Falloppian canal is involved. It is preferable to opt for the more extensive microscopic approach to manage the facial nerve while obtaining the radical removal of the disease. By the virtue of the combined use of microscope and endoscope, we achieved the complete removal of these pathologies in 41 (95.3%) of 43 patients with associated long-term disease-free endoscopic evidence at follow-up.
The fenestral area, mostly for the round one, as well as the hidden parts of the epitympanum, the posterior mesotympanum and the hypotympanum, the endoscopic better visualization 16 allowed us to a complete removal of the choelstaetoma matrix without any further drilling need. In the cases of petrous bone cholesteatoma, the endoscope gave us the opportunity to control the petrous apex without the facial nerve repositioning which is burdened by temporary facial nerve paralysis. Few cases of hidden cholesteatoma matrix on the medial surface of the tympanic membrane not directly noticeable by the microscope, the endoscope allowed to remove the pathology without detaching the stria malleolararis preserving the functional anatomical integrity of the tympanomalleolar complex.
We believe that in planning a cholesteatoma surgery, we need to keep in mind which areas are involved and which of them will be accessible only by the endoscope versus requiring the need of different approaches using other instruments. In Figure 2, we propose an algorithm to aid in this decision.
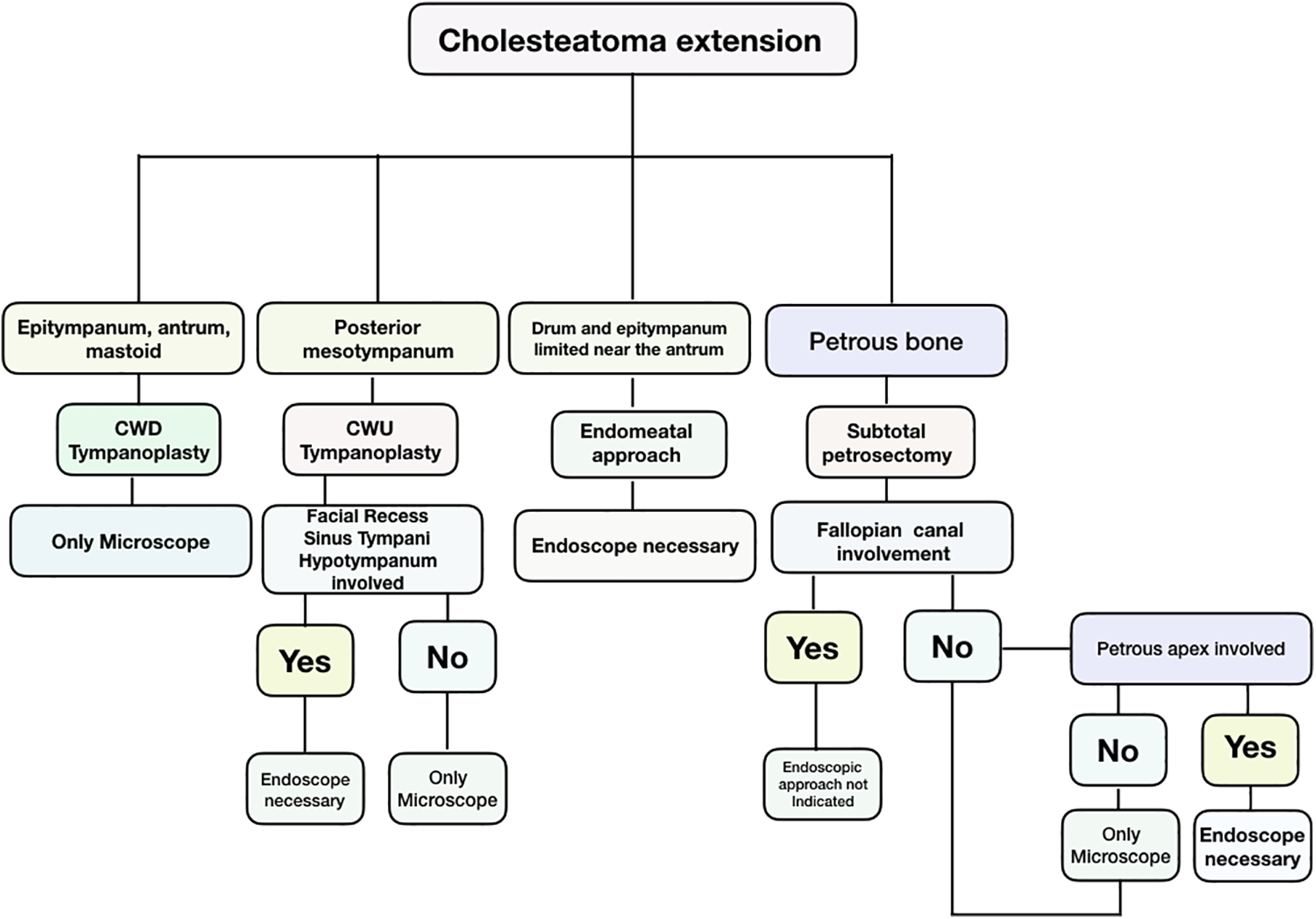
Algorithm for choosing the best approach for middle ear/petrous bone cholesteatomas.
Conclusions
Our experience allows us to indicate the use of the endoscope in cholesteatoma surgery. First, in those cases where it is limited to the drum or with a short extension near the aditus. Second, as complementary tool to complete the surgery in the blind areas of the drum to the microscope. Lastly, to operate the regions, like the petrous apex, which are not easily reached without an extensive dismantling of the petrous bone.
Otosurgeons understand that both microscope and endoscope have advantages and drawbacks. The advantages of the microscope are stereoscopic vision, the possibility of 2-hand surgery, visual conservation of the real anatomy of the middle ear. On the other hand, the most important drawback being the inability to see “around the corner.” The endoscope allows us to see “around the corner” but inevitably, the endoscope does not allow us to perform 2-hand surgery slowing down the procedure. The distortion of the anatomy and the bloodless field needed are the main features that the surgeon must take into consideration.
In our humble opinion, these 2 tools perfectly complement one another. The otosurgeon should be taught to practice the microscopic skills just as the endoscopic ones. The endoscopic practice should be directed not only to improve mono-manual skills but also to understand how the visualization of the anatomy of the middle ear changes when using the microscope and the endoscope, respectively. This concept is of utmost importance because anatomic knowledge is imperative during the surgical practice, above all when its visualization is so tool dependent.
In conclusion, the otosurgeon must have a thorough understanding of the pros and cons of both microscopic and endoscopic technique but more importantly be able to apply that knowledge to decide which tool, or combination of tools, to use. It is imperative that the surgical planning process include consideration of anatomical positioning of the lesion, feasibility of access with chosen technique while striving for the least invasive surgery without compromising complete resection whenever possible. We discourage the a priori use of any individual technique but hope to lead surgeons into planning for cases on an individual bases considering all of the options available to them to achieve the best result.
Footnotes
Acknowledgments
The authors would like to thank: Dr Muaaz Tarabichi for his critical revision, Mrs Daniela Bley Sebastiani for the manuscript syntax revision.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.