
Abstract
Middle ear tumors are relatively rare, and among them, the diagnoses of middle ear lesions originating from cartilage-like tissue are even rarer. Use of transcanal endoscopic ear surgery (TEES) has increased in recent years because of its advantages, such as clear visual field and minimally invasive procedure. Here, we report a middle ear mass originating from cartilage-like tissue treated with TEES. A 62-year-old woman presented with progressive right-sided hearing loss. A white mass was revealed through the tympanic membrane, and pure-tone audiometry detected a mean 50.0 dB conductive hearing loss. Computed tomography showed a mass in the tympanic cavity. TEES was performed for diagnosis and treatment. A white translucent tumor was observed intraoperatively, and it was completely resected. Histopathological examination confirmed the diagnosis of a mass originating from degenerated cartilage-like tissue. To the best of our knowledge, this is the first study of a middle ear mass originating from cartilage-like tissue treated with TEES. TEES with its clear visual field and precise techniques was beneficial in treating the middle ear lesions circumscribed in the tympanic cavity.
Introduction
Middle ear tumors are relatively rare. Moreover, their differential diagnoses are varied, and clinical symptoms and laboratory data are not specific. Diagnosis based on preoperative findings of the tympanic membrane or imaging study is difficult; thus, histopathological examination is often required for confirmed diagnosis. Furthermore, middle ear lesions originating from cartilage-like tissue are even rarer, and to our knowledge, there is only one previously published case report. 1
Transcanal endoscopic ear surgery (TEES) is an innovative surgical option that provides access to the tympanic cavity. In recent years, the employment of TEES has increased due to its advantages, including a brighter, larger visual field and minimally invasive procedure.2-7 Generally, non-hemorrhagic lesions localized in the tympanic cavity, such as cholesteatoma or ossicular malformation, are good indications for TEES.7,8 However, there are only few reports of middle ear tumors treated with TEES.
Herein, we present a case of a middle ear mass originating from cartilage-like tissue that was considered a tumor preoperatively and treated with TEES. In this study, TEES was useful, especially in the observation of the lesion extending toward the protympanum and the aditus to the mastoid antrum.
Case report
A 62-year-old woman with no past medical or trauma history visited our department with a complaint of right-sided hearing loss that had slowly worsened over several years. A non-pulsatile white mass was observed through the posterior-superior quadrant of the right tympanic membrane (Figure 1(A)). The patient did not have a history of vertigo, facial nerve palsy, taste disorder, or external ear malformation. Pure-tone audiometry detected that the right-side average hearing level at frequencies of 500, 1000, 2000, and 4000 Hz was 50.0 dB with low-tone conductive hearing loss (Figure 1(B)). Electroneurography of the right side showed 169.3% in the musculus orbicularis oculi and 129.6% in the musculus orbicularis oris in comparison with the left side. Computed tomography (CT) of the right temporal bone identified a well-circumscribed mass with soft-tissue density, measuring 4 × 8 × 9 mm in size, and less hemorrhage. It extended from around the incudomalleolar joint toward the epitympanum and protympanum (Figure 1(E)). The mass showed a few scattered high-density nodules (Figure 1(F)). And it was adjacent to the facial nerve canal, with a thinning area that suggested canal bone loss (Figure 1(G)). The ossicular chain seemed intact. Magnetic resonance imaging (MRI) demonstrated no evidence of cholesteatoma on periodically rotated overlapping parallel lines with an enhanced reconstruction technique (Figure 1(H)). Preoperative and postoperative findings. (A) Appearance of preoperative tympanic membrane. A non-pulsatile white mass was observed through the right tympanic membrane (white arrow). (B) Preoperative pure-tone audiogram. Mean hearing level in the right side was 50.0 dB with low-tone conductive hearing loss. (C) Appearance of postoperative tympanic membrane. There was no evidence of recurrence. (D) Postoperative pure-tone audiogram. There was an improvement in conductive hearing loss in the speaking range and low-tone area. Mean hearing level was 36.3 dB. (E) Preoperative CT of the right temporal bone showed that the mass, with soft-tissue density, is well circumscribed from the epitympanum and the aditus to the mastoid antrum (white arrow, axial image). (F) A few small high-density nodules were observed within the mass (white arrow, axial image). (G) The mass was in contact with the facial nerve canal, which exhibited suspicious signs of bone loss (white arrow, coronal image). (H) Preoperative MRI revealed no evidence of cholesteatomas (axial image).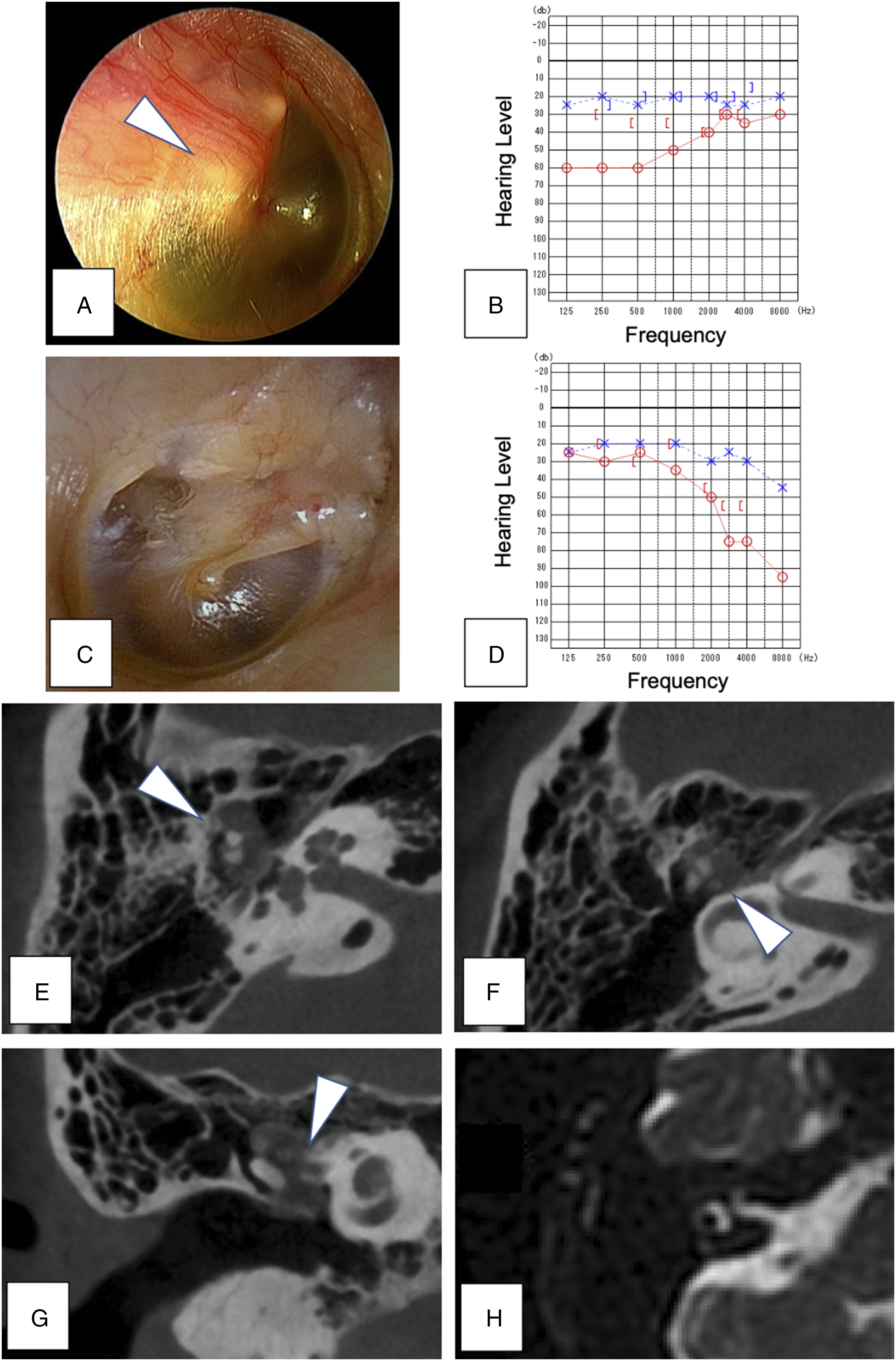
Based on these findings, exploratory tympanotomy and tumor resection with TEES were performed. Elevation of the tympanomeatal flap revealed a smooth, translucent mass, which contained white, firm interspersed nodules. Although the mass was adjacent to the chorda tympani nerve, it could be detached (Figure 2(A)). The mass merged the malleus and incus together and extended to the aditus to the mastoid antrum, the epitympanum, and the protympanum (Figure 2(B)). The mass was extensively bordered by the stapes and the horizontal portion of the facial nerve canal; thus, we proceeded carefully by confirming that there was no material or electrical connection between the mass and facial nerve with a nerve integrity monitor system (NIM-Response®, Medtronic, USA). After identification and dissection of the incudostapedial joint with an angled endoscope, the malleus head and incus were removed. With transcanal attico-antrostomy, we totally resected lesions (Figure 2(C)). After total resection, the presence of any remnants was carefully checked with an angled endoscope (Figure 2(D)). Finally, type IIIc tympanoplasty and scutum plasty were performed with the cartilage of tragus. Intraoperative and histopathological findings. (A) A smooth-translucent mass was observed adjacent to the chorda tympani nerve. (B) The lesion had merged the malleus and incus together. (C) A few white-firm interspersed nodules were visible within the lesion. (D) After resection, the operated site was carefully examined using an angled endoscope. (E) Hematoxylin-eosin (high magnification): degenerated cartilage-like tissue (black arrow) and calcification (white arrow). (F) Hematoxylin-eosin (high magnification): infiltration of inflammatory cells (white arrow) and old hemorrhagic scars (black arrow). (G) Vimentin (mesenchymal tumors, low magnification): positive. (H) AE1/AE3 (epithelial tumors, low magnification): negative. (I) S100 (nervous tumors, low magnification): negative. (J) Ki-67 (cell proliferative ability, low magnification): negative. TF: tympanomeatal flap, ML: mass lesion, CT: chorda tympani nerve, M: malleus, I: incus, N: nodules within the mass, S: stapes, FN: facial nerve. HE: hematoxylin-eosin.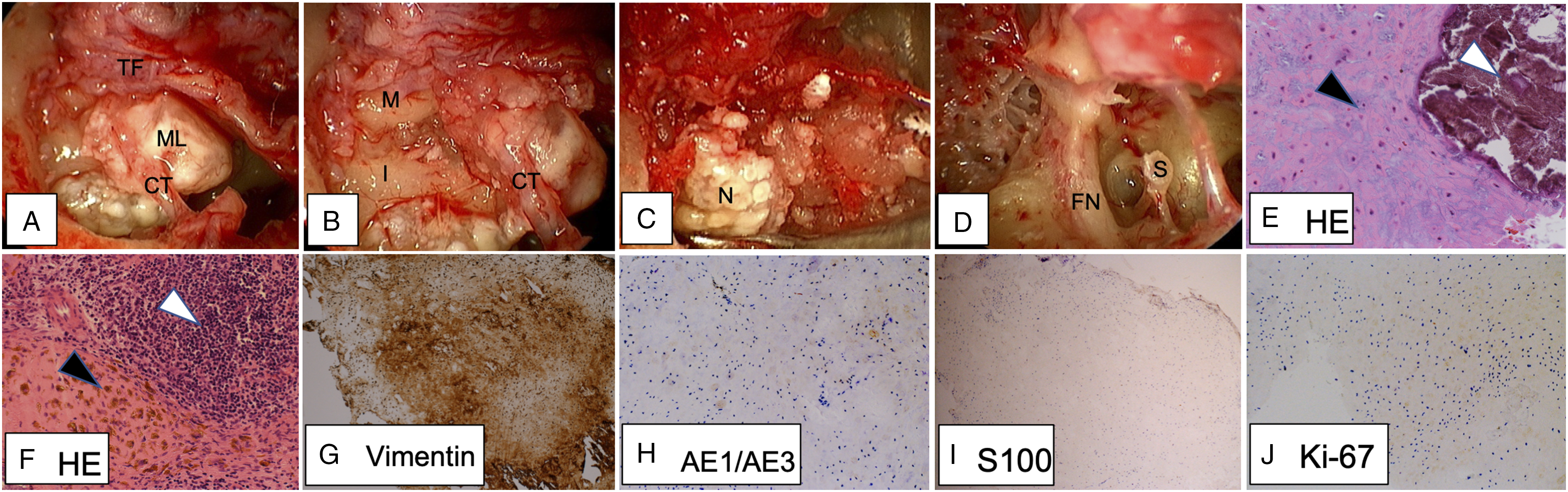
Histopathological examination revealed that the majority of the mass was composed of degenerated cartilage-like tissue along with some bony tissue, crystal-like tissue, inflammatory cell infiltration, and diffuse old hemorrhage (Figure 2(E) and (F)). Immunohistochemical staining was positive for vimentin and negative for AE1/AE3 and S100 (Figure 2(G) to (I)). Collectively, the final diagnosis was not fully defined, but was at least confirmed as a mesenchymal mass that was presumably originated from the cartilage-like tissue. No malignant or neoplastic characteristics were observed, which is compatible with the negative Ki-67 immunostaining (Figure 2(J)).
There was no evidence of recurrence at 1 year postoperatively (Figure 1(C)). Pure-tone audiometry detected an improvement in conductive hearing loss in the speaking range and low-tone area; however, high-tone sensorineural hearing loss was observed (Figure 1(D)). Regular follow-up is necessary for assessing recurrence and hearing changes.
Discussion
Middle ear tumors are relatively rare diseases, and the literature on their diagnosis and management are scarce. The differential diagnosis of middle ear lesions ranges from benign tumors, such as cholesteatomas, schwannomas, paragangliomas, adenomas, and osteomas, to malignant tumors, such as carcinomas and rhabdomyosarcomas. Its clinical symptoms include hearing loss, tinnitus, vertigo, and otorrhea, while malignant tumors often cause bleeding, pain, and facial palsy.3,6,9-12 Preoperative examinations including imaging studies are not specific. Especially, cholesteatomas and osteomas can be differentiated by tympanic membrane findings or imaging studies such as CT, whereas other tumors are difficult to diagnose by only those studies, and required histopathological analysis for a confirmed diagnosis in most patients. In cases of benign tumors, the main treatment is resection.
Furthermore, middle ear lesions originating from cartilage or cartilage-like tissue are even rarer. To the best of our knowledge, there has been only one report of a middle ear cartilaginous mass, which was diagnosed in a 7-year-old boy. 1 In that patient, the mass was accidentally found and initially considered a congenital cholesteatoma. Although surgery was performed, pathological examination revealed the mass to be “degenerated cartilage tissue.” Thus, it was hypothesized that the mass was an “excessive blastemal tissue differentiated into cartilaginous tissue.”
Additionally, a typical example of mass lesions originating from the bone or cartilage as with this case is osteomas. The etiology of middle ear osteomas remains unclear. According to the literature, there are 2 main causes: (1) congenital factors, such as heredity abnormalities,10,13 and (2) acquired factors, such as chronic inflammation including otitis media or trauma.11,12 In this study, the patient had a slow onset after middle age, and pathological evaluation demonstrated inflammation and old hemorrhage. This may suggest that the etiology of this case was that congenital or acquired mass was enlarged and adhered to surrounding tissues due to secondary causes such as infection or bleeding.
Preoperative CT revealed some scattered high-density areas within the mass, which, on further histopathological examination, was considered to be the bone and crystal-like tissue. In the previous literature, the teratomas in other body regions often revealed masses with mixed calcification and cystic areas in CT. 14 However, to our knowledge, there are no studies with similar findings in middle ear teratomas. Whether this imaging finding can help diagnosis for lesions originated from the bone or cartilage remains unclear, and more studies are needed for further understanding and validation.
Pure-tone audiometry at 1 year postoperatively revealed improvement in conductive hearing loss in the low-tone area and speaking range and high-tone sensorineural hearing loss. This may have been due to intraoperative manipulation around the ossicles, especially the dissection of the incudostapedial joint. Fortunately, the patient did not have any complaint of hearing loss, but careful follow-up is necessary.
In our study, the middle ear lesion was resected with TEES. The use of TEES for middle ear disease was first reported in 1993. 15 In recent years, its employment has increased due to its advantages, such as bright and enlarged field of view and minimally invasive procedure.2-7 Although it has been suggested that non-hemorrhagic and well-circumscribed lesions localized in the tympanic cavity, such as cholesteatoma or ossicular malformation, are good indications for TEES, there are few reports of middle ear tumors treated with TEES.7,8 And those reports demonstrated that TEES is useful for treatment of middle ear tumors especially those that are less-hemorrhagic (non-inflammatory) and well circumscribed in the tympanic cavity as in our case.3-6 In our case, use of an endoscope, particularly an angled endoscope, was beneficial for manipulation and observation of the protympanum, tympanic sinus, and mastoid antrum, which often become blind spots of the microscope.
Conclusion
We report a case of a middle ear mass originating from cartilage-like tissue that was completely resected with TEES. Preoperative diagnosis was difficult, and histopathological and immunohistochemical examinations were required for confirmed diagnosis. The presence of scattered high-density areas within the lesions on CT may be used to identify whether the lesion originates from bone or cartilage. In our study, the TEES approach for middle ear lesions circumscribed in the tympanic cavity was favorable due to its clear visual field and precise techniques.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.