
Abstract
This report describes an atypical presentation of cryptococcal meningitis (CM) in a 51 year-old HIV-negative male with diabetes, hypertension, and psoriasis. The patient presented with a 10 day history of subacute headache, vomiting, and fever, followed by the abrupt onset of profound bilateral sensorineural hearing loss (SNHL), ataxia, diplopia, anosmia, ageusia, drowsiness, meningismus, absent gag reflex, and bilateral abducens palsy. Brain MRI revealed inflammatory changes involving the sellar diaphragm, thalamus, and pituitary stalk. Cerebrospinal fluid analysis confirmed CM (pleocytosis, elevated protein, hypoglycorrhachia, opening pressure >60 cmH2O, positive cryptococcal antigen), with negative HIV and malignancy screens. Audiometry confirmed profound bilateral SNHL. Treatment included intravenous liposomal amphotericin B followed by high-dose oral fluconazole, augmented by serial therapeutic lumbar punctures for intracranial pressure (ICP) control. Partial hearing recovery was observed at 1 month follow-up. This case highlights that sudden bilateral SNHL—rarely the dominant initial manifestation—can herald CM even in hosts without overt immunosuppression, posing significant diagnostic challenges. The constellation of profound SNHL, multiple cranial neuropathies (including VIII), cerebellar signs, and markedly-elevated ICP strongly implicates retrocochlear pathology, likely resulting from meningeal inflammation, direct vestibulocochlear nerve invasion, and/or neural compression. Critically, timely-antifungal therapy combined with aggressive ICP reduction facilitated neurological recovery, demonstrating potential reversibility and avoiding premature cochlear implantation. Clinicians should consider CM in patients presenting with acute bilateral audiovestibular dysfunction accompanied by cranial neuropathies or elevated ICP, particularly with subacute prodromal symptoms. This case underscores the essential role of concurrent ICP-directed management alongside antifungals to optimize neurological outcomes, including hearing recovery.
Keywords
Introduction
Cryptococcal meningitis (CM), caused primarily by Cryptococcus neoformans, represents a significant opportunistic infection of the central nervous system, particularly in immunocompromised individuals such as those with HIV/AIDS, diabetes mellitus, or chronic steroid use. 1 While classically presenting with subacute symptoms such as headache, fever, and meningismus, its neurological complications can be diverse and devastating.1,2 Sensorineural hearing loss (SNHL) is an uncommon recognized complication of CM, yet it rarely dominates the clinical presentation at onset.1,2 The pathophysiology of SNHL in CM involves retrocochlear damage from direct fungal invasion of the vestibulocochlear nerve, meningeal infiltration, or elevated intracranial pressure (ICP) causing compression.1,3,4 Unlike bacterial meningitis—where labyrinthitis ossificans necessitates urgent cochlear implantation (CI)—CM rarely induces cochlear fibrosis, and hearing loss may exhibit partial or complete reversibility with timely-antifungal therapy and ICP management.1,4 However, profound bilateral deafness as a presenting or early complication remains exceptionally rare, particularly in immunocompetent hosts.3,5
Here, we present a case of CM in an HIV-negative patient with multiple comorbidities, whose clinical course was marked by sudden, profound bilateral deafness preceding formal diagnosis. This case underscores the diagnostic challenges of CM when atypical symptoms predominate and highlights the potential for hearing recovery despite severe initial deficits. It further emphasizes the critical role of ICP control in mitigating neurological sequelae.4,6
Case Presentation
A 51 year-old male with underlying diabetes mellitus, hypertension, and psoriasis presented to the neurology department with a 10 day history of gradual-onset severe headache, vomiting, and fever, preceded by a recent upper respiratory tract infection. On hospital day 7, he developed sudden-onset bilateral deafness accompanied by ataxia, diplopia, anosmia, and ageusia. Clinical examination revealed drowsiness, positive meningeal signs, absent gag reflex, and bilateral abducens nerve palsy. Brain MRI demonstrated regular hypointense thickening with mild enhancement on T1-weighted sequences involving the sellar diaphragm, thalamus, and pituitary stalk, suggesting inflammatory sequelae; the remainder was unremarkable (Figure 1). Cerebrospinal fluid analysis showed pleocytosis (400 WBCs/μL), elevated protein (117 mg/dL), hypoglycorrhachia (36 mg/dL), op = 60 cmH2O, and positive Cryptococcus antigen, and HIV was negative. Audiometry confirmed profound bilateral SNHL (Figure 2), while oncological investigations were negative. A diagnosis of CM was established, prompting treatment with intravenous liposomal amphotericin B (350 mg/day for 2 weeks) followed by oral fluconazole (800 mg/day for 8 weeks) and repeated lumbar punctures (LPs) for monitoring ICP. The patient was discharged after 2 months with improved meningeal/cerebellar signs on maintenance fluconazole (200 mg daily for 6 months). One-month follow-up documented partial hearing recovery (Figure 3).
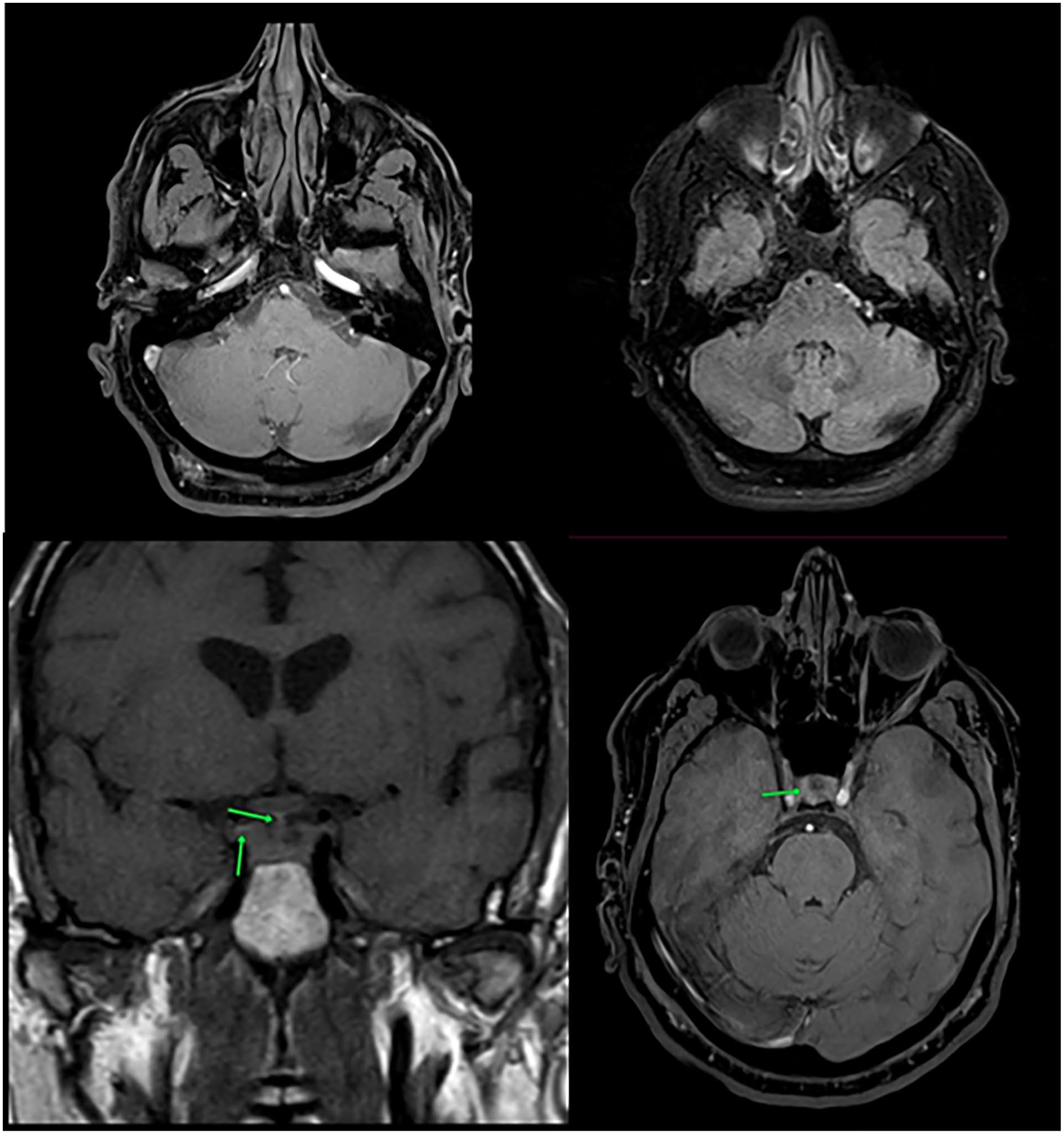
Brain MRI demonstrated regular thickening with mild enhancement on T1-weighted sequences involving the sellar diaphragm and pituitary stalk, suggesting inflammatory sequelae (arrow).
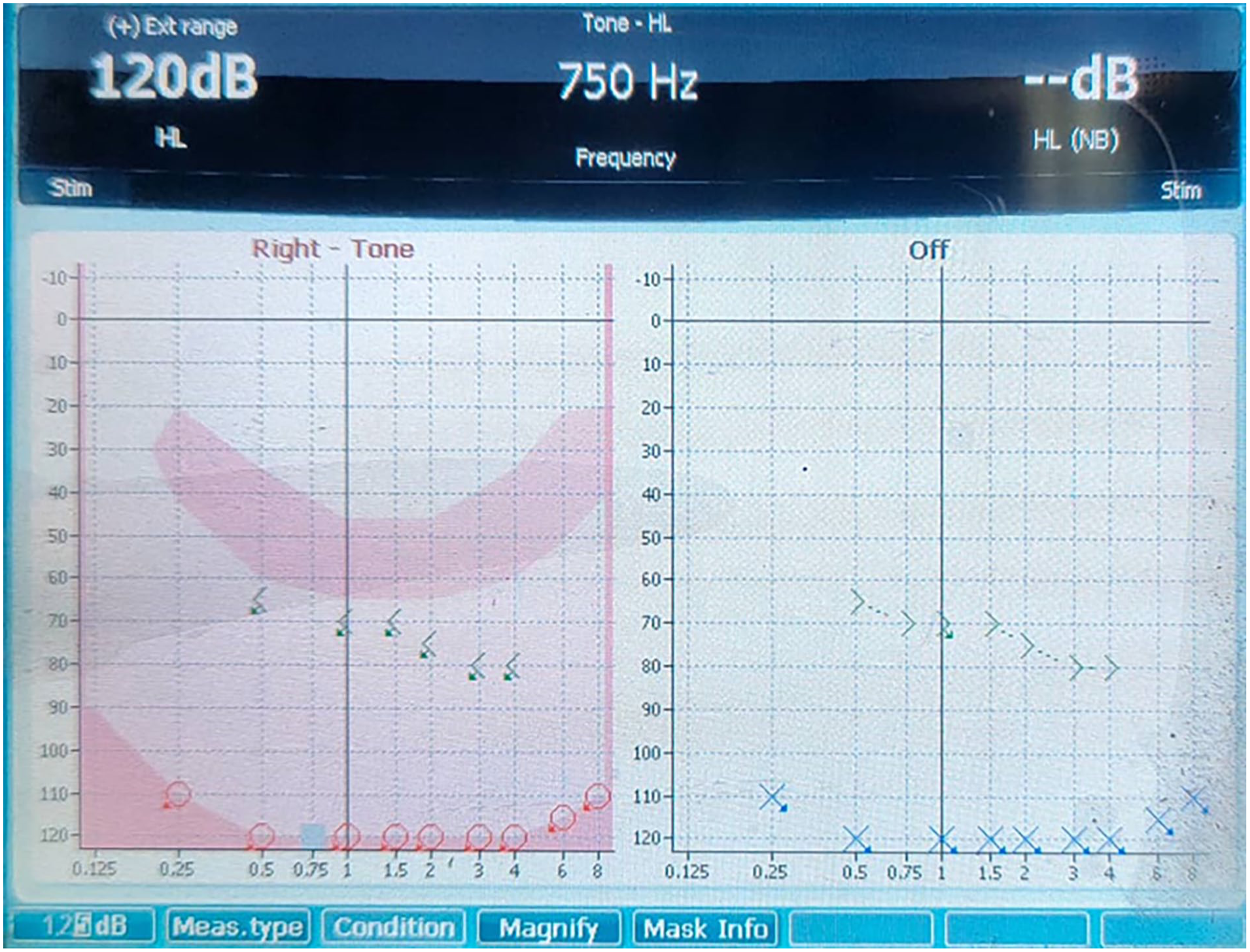
Pure-tone audiogram at the time of diagnosis shows bilateral profound hearing loss.

Audiogram after 1 month shows improvement.
Discussion
This case illustrates several critical aspects of CM, notably the dramatic presentation with sudden, profound bilateral SNHL preceding definitive diagnosis in an immunocompetent host. While SNHL is a recognized complication of CM—it is rarely the dominant initial symptom, posing significant diagnostic challenges.1,2,5 Our patient’s rapid evolution from headache/vomiting to complete deafness, cranial neuropathies (abducens palsy, absent gag reflex), and cerebellar signs underscores CM’s capacity for multifocal neurological injury, often mimicking other conditions like stroke or autoimmune encephalitis.3,4
The pathophysiology of SNHL in CM remains debated, but evidence strongly implicates retrocochlear involvement. Histopathological studies consistently demonstrate cryptococcal infiltration of the cochlear nerve, spiral ganglion cells, or internal auditory canal, with relative sparing of the organ of Corti.1,6,7 This aligns with our patient’s preserved otoacoustic emissions (OAEs) despite profound deafness—indicating intact outer hair cell function—and absent auditory brainstem responses (ABRs), signifying neural pathway disruption.1,5,7 Elevated ICP (>60 cmH2O in our case) likely compounded neural injury via the compression of the vestibulocochlear nerve or ischemia.1,4,5 Notably, MRI in our patient showed no cochlear fibrosis or ossification, distinguishing CM from bacterial meningitis where labyrinthitis ossificans necessitates urgent CI.2,5
Hearing recovery potential is a key distinction from bacterial meningitis. While initial deficits can be profound and bilateral (as here), partial or even complete reversal is possible with timely-antifungal therapy and aggressive ICP control.2,4 -6 The normalization of OAEs in our patient likely predicted this favorable trajectory.2,5 Recovery mechanisms may include the following: (1) Reduced meningeal inflammation and ICP lowering alleviate neural compromise.4,5 (2) Cryptococcal toxins or edema may cause transient conduction block without axonal destruction.1,2 (3) Antifungals clear direct nerve invasion.1,6 Serial therapeutic LPs were pivotal in our management, correlating with clinical improvement. This reinforces that ICP control—not just antifungals—is critical for mitigating neurological sequelae, including SNHL and vision loss.4 -6
Diagnostic pitfalls in this case warrant emphasis. The subacute headache phase (10 days) initially obscured CM, while sudden deafness was misattributed to idiopathic causes. CM should be suspected in any patient with subacute headache plus: 1) Unexplained cranial neuropathies (especially VIII).1,3 (2) SNHL with retrocochlear features (absent ABRs + preserved OAEs).2,5 (3) Immunosuppression (even mild, eg, diabetes).1,3 LP with cryptococcal antigen testing remains diagnostic gold standard; delaying it risks irreversible deficits.1,3,4
Therapeutic implications arise from CM’s unique SNHL profile: (1) CI decisions: Unlike bacterial meningitis, cochlear ossification is rare in CM.2,5 CI can be deferred for 3 to 6 months to allow potential recovery, particularly if OAEs are present.2,5 (2) Steroid caution: Empiric steroids for “idiopathic” sudden SNHL may worsen occult cryptococcal infection.1,7 (3) ICP-first approach: Serial LPs/shunting is nonnegotiable for SNHL/vision recovery, even with adequate antifungals.4 -6
Our case aligns with emerging evidence that CM can present with prominent otovestibular symptoms even in immunocompetent hosts, often as the heralding sign. 8 This atypical presentation can lead to critical diagnostic delays, as the initial focus may mistakenly be on idiopathic sudden SNHL. A high index of suspicion is therefore paramount in patients presenting with acute bilateral audiovestibular dysfunction, particularly when accompanied by other subtle neurological signs, to ensure timely LP and antigen testing. 9
The pathophysiological mechanism appears to be predominantly retrocochlear, as evidenced by the common finding of internal auditory canal enhancement on MRI, which correlates strongly with the degree of hearing loss. 10 This radiographic finding suggests inflammatory involvement of the nerve itself, either from direct fungal invasion or, more likely, from a robust postinfectious inflammatory response within the confined bony canal. This distinguishes CM from bacterial meningitis, where cochlear fibrosis is more common, and underscores the potential for neural recovery with appropriate management. 10
The potential for hearing recovery, even after profound loss, is a critical prognostic feature that must guide management decisions. Unlike bacterial meningitis, cochlear ossification is rare, allowing for a period of observation while administering aggressive antifungal and ICP-directed therapy before considering CI. 8 The observed recovery, often partial but functionally significant, reinforces that the primary injury is often to neural conduction rather than permanent cochlear destruction, highlighting the importance of serial audiometric monitoring.9,10
Sudden bilateral SNHL, though atypical, can herald CM—especially in hosts with subtle immunocompromise. Our case underscores that: (1) Retrocochlear injury predominates, often sparing the cochlea itself. (2) Recovery is possible with ICP control and antifungals, avoiding rushed CI. (3) OAEs are prognostic and should be routine in audiometric assessment.
Heightened suspicion for CM in acute audiovestibular presentations enables earlier intervention, optimizing neurological outcomes.
Conclusion
This case highlights that sudden, profound bilateral SNHL, though atypical, can be the heralding manifestation of CM, even in patients without overt immunosuppression. The clinical presentation, associated cranial neuropathies, and elevated ICP strongly suggest retrocochlear pathology, likely stemming from meningeal inflammation, direct nerve invasion, and neural compression. The observed partial hearing recovery following timely-antifungal therapy and aggressive ICP reduction via serial LPs underscores the potential for neurological reversibility. This emphasizes the critical need to consider CM in acute audiovestibular presentations and the nonnegotiable role of concurrent ICP-directed therapy alongside antifungals to optimize outcomes, including hearing recovery and avoidance of premature CI.
Footnotes
Ethical Considerations
Our institution does not require ethics approval for reporting individual cases.
Consent for Publication
Written informed consent was obtained from the patient for publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the author or corresponding author upon reasonable request.