
Abstract
Objective:
Carotid body tumors (CBTs) are rare neurogenic tumors that may indirectly affect cardiac autonomic regulation. This study aims to investigate the relationship between tumor size and electrocardiographic (ECG) findings, particularly the corrected QT (QTc) interval.
Methods:
This retrospective study included 21 patients with histologically or radiologically confirmed CBTs treated at a tertiary center between 2021 and 2025. Patients with comorbidities or medications affecting cardiac conduction were excluded. Tumor sizes were measured via contrast-enhanced computed tomography or magnetic resonance imaging. Preoperative ECGs were analyzed for heart rate, P wave, PR, QRS, T wave, and QTc intervals. The correlation between tumor size and ECG parameters was assessed using Spearman’s rank correlation.
Results:
A statistically significant and strong positive correlation was observed between tumor size and QTc interval (r = 0.940, P < .001). No other ECG parameter showed a significant association with tumor size. Tumor size explained 88.36% of the variance in QTc duration (r 2 = 0.8836).
Conclusion:
This study demonstrates a strong correlation between CBT size and QTc prolongation, suggesting vagal overactivity as a possible mechanism. QTc may serve as a noninvasive marker of subclinical autonomic dysregulation in CBT patients. Larger prospective studies are warranted to validate this association and explore its clinical significance.
Introduction
Carotid body paragangliomas, also known as glomus caroticum tumors, are rare, typically benign neuroendocrine neoplasms that originate from paraganglionic tissue located at the carotid bifurcation. These tumors are known for their slow growth and hypervascularity. 1 Although they are generally localized, their anatomical proximity to the carotid sinus and cranial nerves suggests potential influence on autonomic cardiovascular regulation. Prior literature has described cases of bradycardia, hypertension, and arrhythmias in association with paragangliomas, especially those of larger size or functional activity.1,2 However, the correlation between tumor mass and specific electrocardiographic (ECG) parameters has not been systematically explored. This study aims to investigate whether there is a measurable relationship between the size of carotid body tumors (CBTs) and changes in ECG intervals, with a particular focus on the corrected QT (QTc) interval, a marker of ventricular repolarization and arrhythmia risk.
Materials and Methods
Study Design and Ethical Approval
This retrospective study was conducted at Başakşehir Çam and Sakura City Hospital, Istanbul, Turkey. The protocol was approved by the hospital’s ethics committee (approval no: 2025-58; date: February 26, 2025) and complied with the Declaration of Helsinki.
Patients Selection
Patients diagnosed with carotid body paraganglioma between June 2021 and April 2025 were retrospectively reviewed. The inclusion criteria were as follows:
Confirmed diagnosis of CBT based on radiological (computed tomography [CT] angiography or magnetic resonance imaging [MRI]) or histopathological findings.
Availability of a preoperative 12-lead surface ECG taken within 1 month of diagnosis.
Regular sinus rhythm on ECG.
No history of cardiac surgery or structural heart disease.
No concurrent systemic diseases (eg, diabetes, hypertension, and renal insufficiency).
No use of any medications affecting cardiac conduction or autonomic tone (eg, beta-blockers, calcium channel blockers, and antiarrhythmics).
No radiological evidence of altered carotid artery flow on CT angiography.
No associated functional paraganglioma (eg, pheochromocytoma) or other paraganglionic foci.
Tumor located primarily at the carotid bifurcation without deep skull base extension.
These strict selection criteria were adopted to minimize confounding factors that could influence ECG parameters. Patients with arrhythmias, cardiovascular or systemic comorbidities, relevant medication use, functional tumors, extracarotid extension, impaired carotid flow, or incomplete data were excluded. A total of 21 patients who met all inclusion and exclusion criteria were included in the final analysis.
Tumor Size Measurement
Tumor dimensions were evaluated using contrast-enhanced CT and/or MRI obtained during the initial diagnostic workup. All imaging studies were assessed using a calibrated Picture Archiving and Communication System (PACS; Echelon, Fujifilm Healthcare, Tokyo, Japan) workstation, and multiplanar reconstructions were systematically reviewed in axial, coronal, and sagittal planes to ensure comprehensive spatial evaluation.
The maximum and the minimum tumor diameters (in millimeters) were measured by a single radiologist with formal training and clinical experience in head and neck imaging. Measurements were obtained in the plane demonstrating the greatest longitudinal extent of the lesion. In cases where both CT and MRI datasets were available, contrast-enhanced CT images were preferentially utilized, owing to their superior spatial resolution for delineating soft tissue and vascular boundaries.
To ensure methodological consistency, all measurements were performed using standardized window level and width settings, as well as fixed magnification ratios across cases. The radiologist was blinded to all ECG and clinical outcome data to eliminate potential observer bias.
ECG Evaluation
Preoperative 12-lead surface ECGs were recorded using a standard ECG device (Philips TC20 [PACS; IntelliSpace Portal, Philips Healthcare, Best, The Netherlands]) at a paper speed of 25 mm/s and an amplitude of 10 mm/mV, with patients in the supine position. The following parameters were analyzed: heart rate, P wave duration, PR interval, QRS duration, T wave duration, and QTc interval, calculated using Bazett’s formula: QTc = QT/√RR. All ECG measurements were manually performed using digital calipers by a single cardiologist experienced in ECG interpretation. The evaluator was blinded to tumor size and all clinical data to minimize potential measurement bias.
Statistical Analysis
All statistical analyses were performed using IBM SPSS Statistics for Windows, version 22.0 (IBM Corp, Armonk, NY, USA). Continuous variables are presented as mean ± standard deviation, along with their minimum and maximum values. The Shapiro-Wilk test was used to assess the normality of the data distribution. Since the data were not normally distributed, the non-parametric Spearman’s rank correlation test was employed to evaluate the relationship between tumor size and various ECG parameters. A 2-tailed P ≤ .05 was considered statistically significant. In addition, for significant correlations, the coefficient of determination (r 2) was calculated to estimate the proportion of variance in the ECG parameter that could be attributed to tumor size.
Results
A total of 21 patients diagnosed with CBTs were included in the study. Of these, 12 were female and 9 were male. The mean age was 47.81 ± 7.75 years for female patients and 48.7 ± 9.2 years for males (Table 1).
Demographic Data of the Patients.
Abbreviations: N, number of patients; SD, standard deviation.
The tumor diameters ranged from 1.7 to 6 cm (3.4 ± 1.1). ECG parameters were evaluated using preoperative 12-lead surface recordings, and correlations with tumor size were analyzed using Spearman’s rank correlation test (Table 2).
Correlation Analysis Between Tumor Size and ECG Parameters.
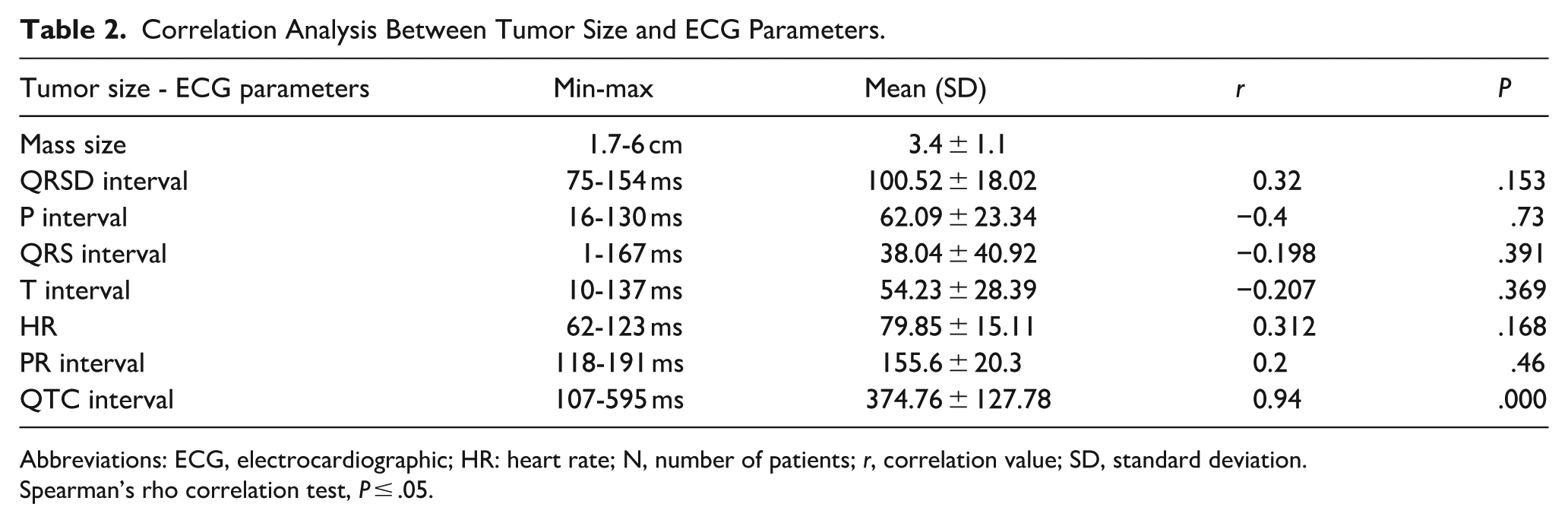
Abbreviations: ECG, electrocardiographic; HR: heart rate; N, number of patients; r, correlation value; SD, standard deviation.
Spearman’s rho correlation test, P ≤ .05.
Among the evaluated parameters, a statistically significant and strong positive correlation was observed between tumor size and QTc interval (r = 0.940, P < .001). This finding suggests that increasing tumor diameter is associated with prolonged ventricular repolarization (Table 2).
The mean QTc interval was 374.76 ± 127.78 ms (range: 107-595 ms), as shown in Table 2. No other ECG parameter exhibited a statistically significant correlation with tumor size. These findings suggest that tumor size does not significantly affect atrioventricular conduction (as reflected by the PR interval), ventricular depolarization duration (QRS interval), or heart rate. The QTc interval was the only ECG parameter to demonstrate a clear and clinically meaningful association with tumor size in this patient group.
The proportion of variance in QTc interval explained by tumor size was calculated as r 2 = 0.8836 (88.36%; Figure 1).
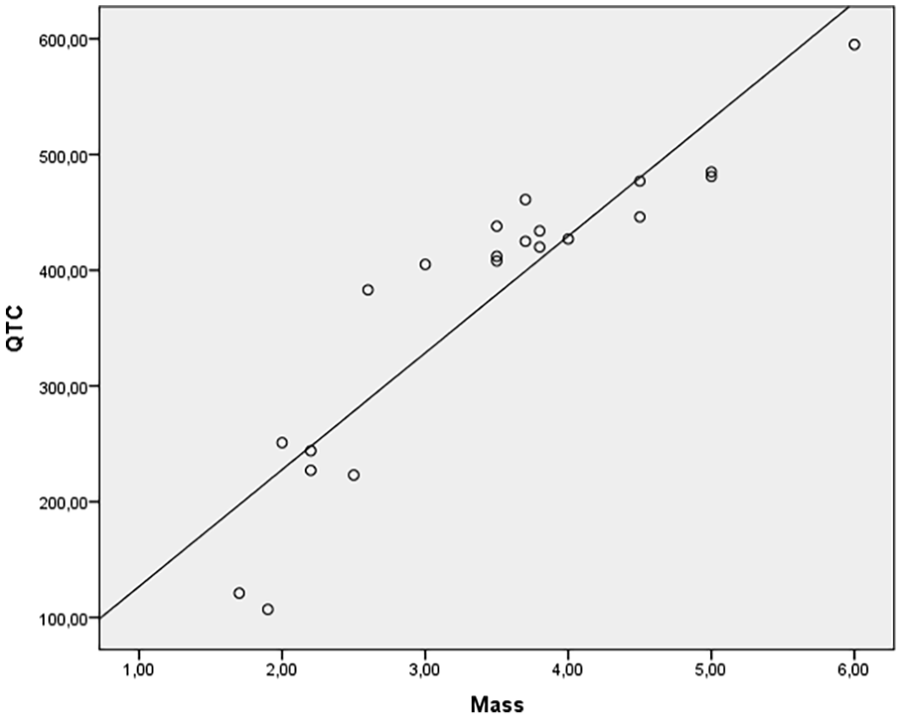
Correlation between tumor size and QTc interval. A strong and statistically significant positive correlation was found (Spearman’s r = 0.940, P ≤ .05). The coefficient of determination (r 2 = 0.8836) indicates that 88.36% of the variance in QTc interval is explained by tumor size. QTc, corrected QT.
Discussion
In our study, we investigated the effects of CBT size on ECG parameters. CBTs are rare neurogenic tumors originating from the chemoreceptive tissue of the carotid body and represent the most common type of paraganglioma in the neck region. 3 They are mostly sporadic and only rarely bilateral. 4 Surgical excision remains the primary and most commonly preferred treatment modality. 5 However, due to their proximity to the carotid artery bifurcation and adjacent cranial nerves, surgery may pose technical challenges. Potential complications include cranial nerve injury, bleeding, and vascular damage. In patients with small, asymptomatic, and slow-growing tumors—especially elderly patients or those with high surgical risk—active surveillance may be considered.5,6 Given the tumor’s anatomical complexity and location, manipulation during surgery is associated with notable morbidity, with complication rates reported between 20% and 27%. 7 Although extremely rare, sudden cardiac arrest may occur intraoperatively, likely due to carotid sinus hypersensitivity. 8
There are no reports in the literature indicating a direct effect of CBTs on cardiac rhythm or ECG findings; however, indirect effects have been demonstrated.7,8 Carotid bodies become activated in hypoxic conditions and can increase heart rate and blood pressure via sympathetic nervous system activation, potentially leading to tachycardia. 9 In individuals who have undergone carotid body resection, the heart rate response to stress conditions such as hypoglycemia is attenuated, indicating a regulatory role in cardiovascular homeostasis. 10 In tumors such as CBT, excessive catecholamine secretion may result in hypertension and tachycardia, which can be reflected on the ECG. 11 Carotid sinus hypersensitivity refers to an exaggerated baroreceptor response to mechanical stimulation, 12 and larger tumors may increase the risk of this complication during surgery.
Previous studies have shown that CBTs can influence ECG findings, yet to date, no research has directly addressed the correlation between tumor size and ECG parameters. Our study represents the first to explore this potential relationship. We identified a strong association between tumor size and QTc interval. This finding may be explained by autonomic modulation, particularly vagal overactivity, which is known to influence cardiac repolarization. Supporting this hypothesis, Schmid et al reported a case of a CBT patient presenting with recurrent syncope, presumably due to carotid sinus hypersensitivity and vagal stimulation. 13 Although QTc prolongation was not measured in that case, the resolution of syncopal episodes following tumor excision suggests a cardiac effect. Our findings provide quantitative electrophysiological evidence for this mechanism.
Duan et al further described a case of cardiac arrest triggered by carotid sinus hypersensitivity during CBT dissection. 14 While their report emphasized mechanical baroreceptor stimulation rather than tumor size, it supports the broader concept that CBTs can exert significant vagally mediated cardiovascular effects. Unlike their case, in our study, a strong positive correlation was observed between glomus caroticum tumor size and QTc prolongation. This finding suggests that the QTc interval may serve as a noninvasive marker reflecting subclinical vagal hyperactivity in patients with CBTs. In particular, significant QTc prolongation in patients with larger tumors may have clinical relevance regarding perioperative cardiac complications.
Prolongation of the QTc interval indicates delayed ventricular repolarization, which may lead to serious clinical outcomes such as torsades de pointes, malignant ventricular arrhythmias, syncope, and sudden cardiac death.15,16 Therefore, careful preoperative evaluation of the QTc interval is essential in patients diagnosed with CBT. Contributing factors that can prolong QTc—such as electrolyte imbalances, bradycardia, or QT-prolonging medications—should be avoided. Considering that vagal tone may increase during surgery, close intraoperative cardiac monitoring and preparedness for resuscitation are crucial. 12
In conclusion, the QTc interval may not only represent an electrophysiological measure but also serve as a helpful parameter for predicting increased cardiovascular risk in CBT patients. Further prospective studies with larger patient cohorts are needed to validate our findings.
Conclusion
The observation that QTc prolongation correlates with lesion size in glomus caroticum tumors suggests that QTc may serve as a valuable electrophysiological marker for identifying patients at increased cardiovascular risk in the perioperative management of CBT. Further large-scale studies are warranted to validate its clinical utility.
Footnotes
ORCID iDs
Ethical Considerations
All procedures performed in studies involving human participants were by the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study protocol was approved by the ethical research committee of the Başakşehir Çam and Sakura City Hospital in Istanbul.
Consent to Participate
Routine informed consent was obtained from all patients before hospitalization, and informed consent from the individuals in the control group was obtained in the study. There is no support source that requires confirmation.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Available.