
Abstract
Primary giant cell tumor of soft tissue (GCT-ST) is a rare entity that is considered the soft tissue equivalent of giant cell tumor of bone. It most commonly arises in soft tissues of the trunk and extremities, with occurrence in the head and neck being extremely rare. We report a case of GCT-ST of the carotid body, the first report of a tumor of this kind arising from this site in the neck. Giant cell tumor of soft tissue is generally considered a benign tumor with low malignant potential; thus, surgical excision is usually curative. However, due to the location and invasive nature of this patient’s tumor, complete excision was not possible. We discuss the implication of this for long-term management of this patient, as well as similarities and differences in clinical presentation, histology, and biological behavior between this case and previously reported cases of GCT-ST.
Introduction
Giant cell tumor of soft tissue (GCT-ST) is a rare and unusual tumor named for its histological and clinical similarities to giant cell tumor of bone. Despite its often benign clinical course, with moderate rate of recurrence and low rate of metastasis, the limited data on GCT-ST lend itself to a relatively small pool of information regarding clinical presentation, diagnosis, treatment, and outcomes. 1 –4 Furthermore, given its predilection for soft tissues of the extremities and trunk, the majority of data on GCT-ST is derived from cases arising from these locations. 1 –3,5,6 To date, only 6 cases of GCT-ST of the neck have been reported in the medical literature. 3,4,6 –11 There have been no reported cases of GCT-ST arising from the carotid body. We aim to add to the current body of literature on this unique tumor by reporting a case of GCT-ST of the carotid body, the first report of a tumor of this kind arising from this site.
Case Report
A 41-year-old woman was referred to our outpatient clinic for evaluation of a left neck mass. The patient reported that she first noticed swelling in her neck 3 months prior to her presentation. A computed tomography scan ordered by her primary care physician revealed a possible left neck mass versus enlarged lymph node (Figure 1 and 2). She was subsequently referred to an outside otolaryngologist, at which time incisional biopsy was performed and revealed a GCT-ST. It was at this point that the patient was referred to our clinic.

Sagittal computed tomography scan of the neck with contrast demonstrating the giant cell tumor measuring 4.55 cm.
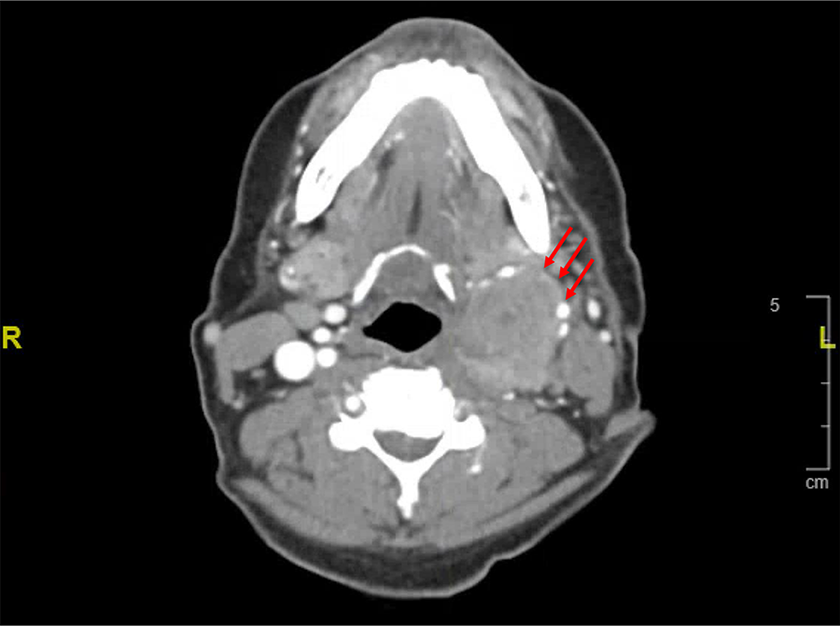
Axial computed tomography scan of the neck with contrast demonstrating the 2.95 cm × 3.61 cm giant cell tumor (red arrows).
Her medical history was unremarkable including any history of head or neck radiation. Other than a feeling of left fullness, she was asymptomatic. Physical examination revealed a 4-cm well-circumscribed, fixed left level II neck mass affixed to the sternocleidomastoid muscle, with a well-healed, overlying scar from the prior open biopsy. Magnetic resonance imaging of the neck revealed a 4.2-cm left neck mass extending superiorly from the level of the angle of the mandible to inferiorly to the left superior aspect of the left thyroid lobe (Figure 3). The mass was found to be lateral to the left carotid artery with anterior displacement of the vessels at the carotid bifurcation. Imaging also showed enlarged left level II and III and right retropharyngeal lymph nodes.
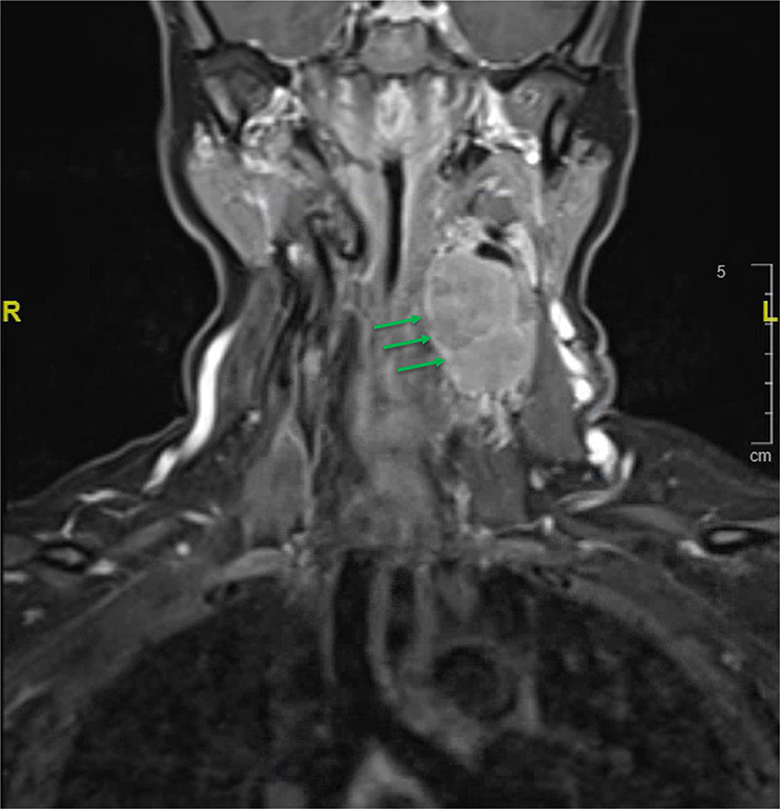
Sagittal T1 magnetic resonance imaging of the neck demonstrating neck mass (green arrows).
The patient was presented to the head and neck multidisciplinary tumor board with the recommendation to undergo surgical resection of the disease as well as ipsilateral neck dissection given the adjacent cervical lymphadenopathy noted on preoperative imaging studies. The mass was found to be fixed to the sternocleidomastoid muscle as well as the greater auricular nerve and external jugular vein. Portions of the structures required sacrifice in order to allow for improved margin control. The mass was found to be dumbbell in shape and emanate from the bifurcation of the left common carotid artery, and the bulk of the mass was found to be deep to this. Below the carotid bifurcation, the mass was fixed to the posterior aspect of the carotid body with extension to the paraspinous musculature. Due to extensive encasement by the mass of the left carotid artery and internal jugular vein, the internal jugular vein was sacrificed while attempting to gain negative margins. Despite hours of meticulous dissection, the tumor was found to be unresectable from the posterior aspect of the left carotid artery and vagus nerve. The vagus nerve was encased 360° by the tumor above and below the carotid bifurcation and thus required sacrifice in order to ensure removal of the tumor without carotid rupture. At the end of the procedure, nearly all of the tumor had been removed save for a sheet of tumor that could not be safely separated from the carotid artery due to risk of rupture. The risk of en bloc resection of the carotid artery with vascular bypass was felt to be greater than the benefit of complete tumor and margin clearance in this situation given the benign histology of this type of tumor. Following this resection, a left suprahyoid neck dissection was performed given the adjacent cervical lymphadenopathy noted on preoperative imaging studies.
At the patient’s 2-week postoperative follow-up visit, the patient complained of a left eyelid droop and hoarse voice. The patient was found to have paralytic ptosis of the left eyelid, likely due to sympathetic nerve injury during surgery, as well as left vocal fold paralysis due to the known sacrifice of the left vagus nerve during surgery. The patient was represented at our institution’s multidisciplinary head and neck tumor conference and the consensus was to recommend radiation therapy. Given the known residual tumor along the carotid body, recurrence was felt to occur at some point in the future, and the likelihood of negative margins with future reoperation was felt to be unlikely.
The differential for this tumor included carotid body tumor (also known as cervical paraganglioma), giant cell tumor of tendon sheath (also known as pigmented villonodular synovitis), and soft tissue sarcoma. 1 –3 Definitive histopathology from the excised mass was found to be consistent with GCT-ST. Microscopically, the mass consisted of round to ovoid mononuclear cells interspersed with numerous multinucleated osteoclast-like giant cells (Figure 4). The nuclei of the giant cells were found to be similar to those of the mononuclear cells and slightly irregular, often with a single distinct nucleolus present in each nucleus (Figure 5). Both the mononuclear cells and multinucleated giant cells displayed abundant eosinophilic cytoplasm and clusters of foamy macrophages were found suggesting regressive change (Figure 6). Immunohistochemical staining of the tumor cells was positive for CD68 and CD163, with the mononuclear cells being more strongly reactive for CD68 and the multinucleated giant cells more strongly reactive for CD163. Scattered cells stained positive for S-100 and SMA. Immunostains for p63 and CD1a were negative.
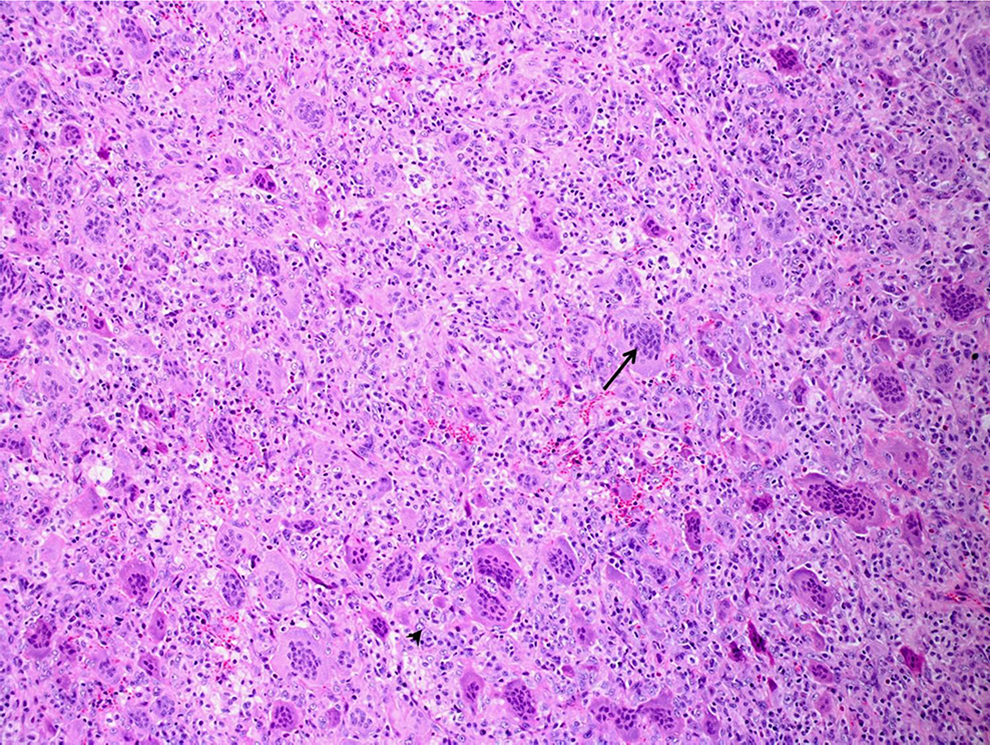
Giant cell tumor of soft tissue. Numerous evenly distributed osteoclast-like giant cells (arrow) admixed with round to oval mononuclear cells (arrowhead; H&E, ×100).
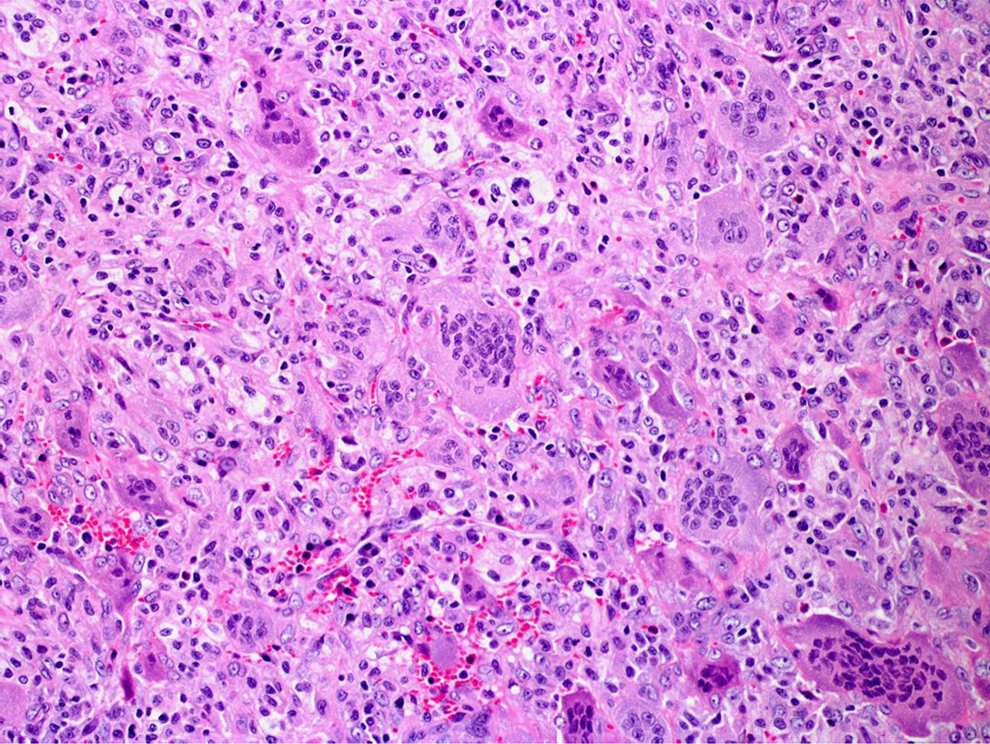
Giant cell tumor of soft tissue. The nuclear features of the mononuclear cells and giant cells are similar. There is no severe nuclear atypia (H&E, ×200).
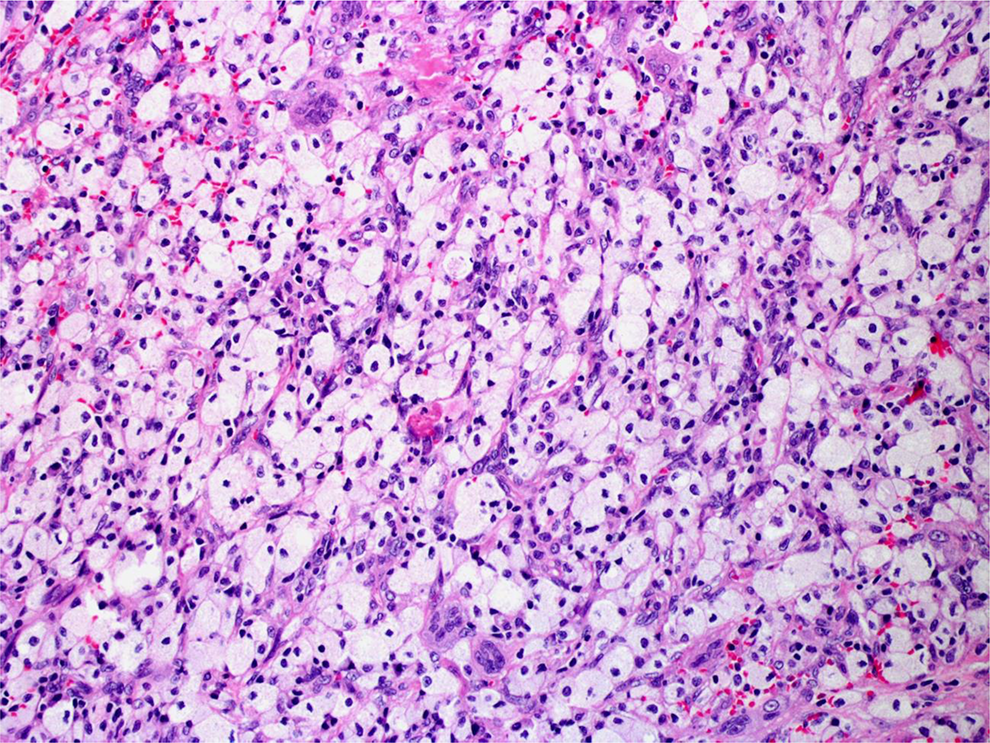
Giant cell tumor of soft tissue. Some areas show clusters of foamy macrophages reflecting regressive change (H&E, ×200).
Discussion
Primary GCT-ST is an unusual tumor that most commonly arises from the superficial or deep soft tissues of the extremities, followed by the trunk and rarely the head and neck. 1 It was first described in 1972 by Salm and Sissons, who refined the diagnostic criteria to include only those tumors of soft tissue containing osteoclastic giant cells similar to those encountered in giant cell tumor of bone, thereby classifying GCT-ST as a clinical entity distinct from other, albeit similar, soft tissue lesions. 3,12 That same year, Guccion and Enzinger published a report which further described the hallmark histological findings of the tumor in addition to its clinical and pathological characteristics. 3,5
Since then, GCT-ST has come to be known as the soft tissue counterpart of giant cell tumor of bone. It frequently presents as a painless mass of a few months’ duration with a predilection for superficial soft tissues of the extremities. 1,2 Histology is notable for the presence of multinucleated osteoclastic giant cells distributed evenly among mononuclear cells, typically histiocytes. Immunohistochemical staining of the multinucleated giant cells shows strong positive reactivity for CD68. 1 –3,5,6,12 Although vascular invasion is common, rates of local recurrence are moderate and metastasis, usually to the lungs, is rare. 1 –4 Treatment is complete surgical excision with wide margins. 1 –3
Reports of primary GCT-ST arising from the neck remain exceedingly rare and thus much of what is known about this tumor is based on its occurrence in the extremities and trunk. We report a case of GCT-ST of the carotid body, a case that is unique both due to its location and because it is the first report of GCT-ST arising from vasculature. In addition to being the first report of its kind, this case also serves to highlight similarities and differences to previously reported cases of GCT-ST.
Although the presentation and histological and immunohistochemical findings in our case were consistent with previously reported cases of GCT-ST, the novel location presented a challenge with regard to treatment. Given its proximity to cranial nerves and the extracranial arterial system, surgical management of GCT-ST of the carotid body is technically challenging compared to GCT-ST located in the extremities or in previously reported regions of the head and neck. Thus, excision with adequate margins, which is generally considered curative for this nonmalignant tumor, may not be achievable, as was the case with this patient. Given the extent of carotid artery involvement, the tumor was unable to be removed in its entirety. As a result, our patient will require close surveillance for recurrence, as the potential for local recurrence may be higher than with tumors that are completely excised. In addition, the portion of the tumor that was left behind will need to be treated with radiation therapy, a treatment option with limited data on outcomes with regard to GCT-ST. Thus, this case represents a unique treatment course compared to previously reported cases of GCT-ST of the head and neck. Further, due to the invasion by this tumor of critical neurovasculature of the neck, excision required sacrifice of several structures, including the left vagus nerve. Thus, the postoperative course for our patient is distinct from that seen with previously reported cases of GCT-ST of the neck, which may in turn have differing implications for long-term management.
Giant cell tumor of soft tissue is a rare and generally benign lesion, most commonly arise in the soft tissues of the trunk and extremities, with rare occurrences in the head and neck. We present the first report of a patient with GCT-ST of the carotid body. Giant cell tumor of soft tissue should be considered in the differential of patients presenting with a carotid body mass given its invasive nature and potential for local recurrence when it arises in this location, both of which in turn have implications for the treatment options and postoperative course of a patient with this tumor.
Footnotes
Authors’ Note
This study was conducted at Cooper University Hospital, Department of Surgery at 1 Cooper Plaza, Camden, New Jersey.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.