
Abstract
Introduction:
Schwannomas are rare, typically benign tumors arising from Schwann cells. Parapharyngeal space tumors account for only about 0.5% of all head and neck neoplasms, with schwannomas representing ~31% of these. Among these, schwannomas originating from the cervical sympathetic chain (CSC) are particularly rare but clinically important. These tumors grow slowly and often present with vague symptoms such as mild dysphagia, which delays diagnosis. Imaging techniques such as computed tomography (CT) and magnetic resonance imaging aid evaluation. This report presents a rare CSC schwannoma case and reviews 54 others to highlight diagnostic and clinical features.
Case Presentation:
A 44-year-old Arab female presented with a 4-month history of mild dysphagia and right-sided throat discomfort. Physical examination revealed a smooth, non-tender submucosal bulge along the right lateral pharyngeal wall. Contrast-enhanced CT demonstrated a well-circumscribed, homogeneously enhancing mass in the right paravertebral space, displacing the carotid sheath—radiologically consistent with a schwannoma. The tumor was excised via a transcervical approach and found intraoperatively to originate from the CSC. Histopathology confirmed a benign schwannoma. Postoperatively, the patient developed first-bite syndrome (FBS), managed conservatively with gradual symptom improvement. At 6-month follow-up, she remained asymptomatic with no evidence of recurrence.
Conclusion:
Parapharyngeal schwannomas are rare neurogenic tumors that often present with vague symptoms, delaying diagnosis. CSC schwannomas, though uncommon, carry a high risk of postoperative complications such as FBS and Horner’s syndrome. Accurate imaging, early recognition, and multidisciplinary planning are essential for safe surgical resection and optimal patient outcomes. This case, alongside our literature review, emphasizes the importance of correlating tumor origin with clinical behavior and postoperative sequelae.
Keywords
Introduction
Schwannoma, also referred to as neurilemmoma, is a rare and typically benign neurogenic tumor originating from Schwann cells, a specialized type of glial cell involved in nerve sheath formation. 1 Tumors arising in the parapharyngeal space (PPS) are themselves uncommon, accounting for ~0.5% of all head and neck neoplasms, with schwannomas being the most frequently encountered subtype within this region (constituting ~31% of PPS tumors).2,3 While PPS schwannomas primarily derive from neurogenic tissues, their precise etiology remains unclear, and they characteristically demonstrate indolent, slow-growing behavior. 3 Patients often present with non-specific clinical symptoms such as dysphagia or chronic nasal obstruction, which can delay diagnosis. 3
Imaging modalities such as computed tomography (CT) and magnetic resonance imaging (MRI) are essential for evaluation, typically revealing well-circumscribed, homogeneously enhancing soft-tissue masses. 3 The cornerstone of treatment is complete surgical excision, followed by histopathological confirmation to establish the diagnosis. 4 Within the spectrum of neurogenic tumors in the PPS, schwannomas originating from the cervical sympathetic chain (CSC) represent a rare but clinically important subset. 5
Herein, we report a unique case of a schwannoma arising from the CSC in a middle-aged female who initially presented with mild dysphagia. In light of the tumor’s rarity and diagnostic challenges, we performed a review of 54 previously published cases of parapharyngeal schwannomas. Our analysis focused on clinical presentations, tumor origins, complication rates according to nerve involvement, and morphologic characteristics. By incorporating our current case as the 55th, this study provides a broader understanding of the clinical spectrum and reinforces the significance of considering CSC schwannomas in the differential diagnosis of PPS masses.
Case Presentation
A 44-year-old Arab female with no significant past medical or surgical history presented to the otolaryngology clinic with a 4-month history of right-sided throat discomfort and mild dysphagia. She denied odynophagia, weight loss, voice changes, or respiratory symptoms. There was no history of trauma, radiation exposure, or familial neurocutaneous syndromes.
Physical examination revealed a smooth, non-tender submucosal bulge along the right lateral pharyngeal wall, with mild medial displacement of the right tonsillar pillar. No mucosal erythema, ulceration, or exophytic lesions were observed. Neurological assessment revealed intact cranial nerves (CN) IX, X, and XII bilaterally, and cervical palpation showed no palpable neck masses or lymphadenopathy.
Due to the suspected pharyngeal tumor, the patient underwent contrast-enhanced axial CT of the neck. Imaging revealed a well-defined soft-tissue mass with benign features centered in the right paravertebral space, extending anteromedially into the lateral pharyngeal space, corresponding to the clinically observed pharyngeal bulge. The lesion caused anterolateral displacement of the carotid sheath as a single unit and maintained preserved blood flow to the carotid arteries. It also abutted the vertebral artery without signs of vascular invasion or luminal narrowing. The mass exhibited homogeneous enhancement, without central necrosis or calcifications, consistent with the radiological features of a schwannoma (Figure 1).
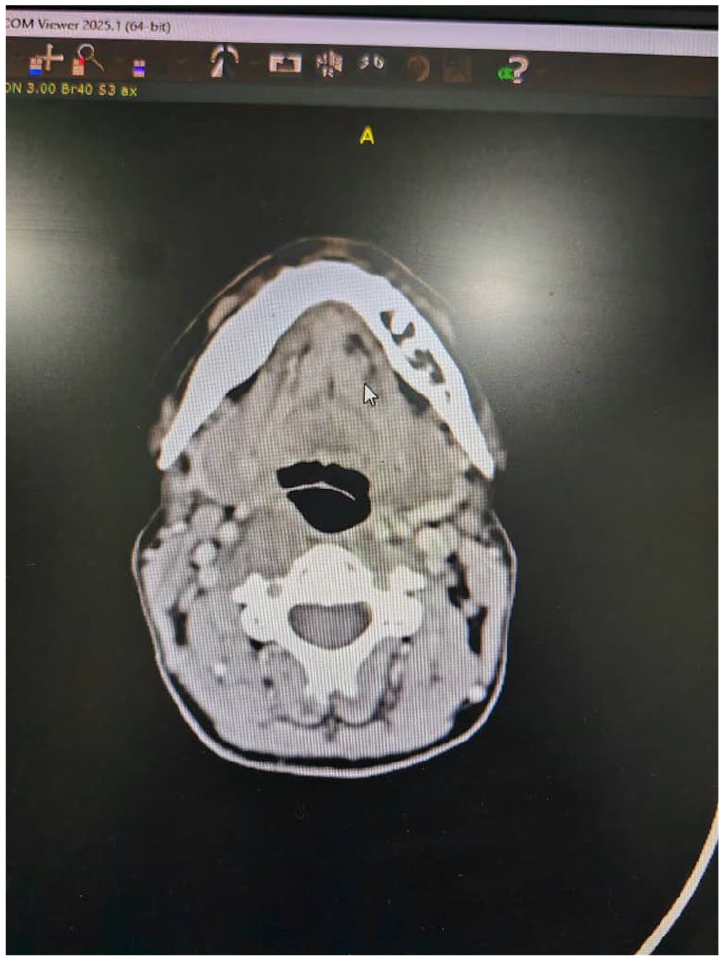
CT scan demonstrates a mass within the paravertebral space, directly abutting the vertebral artery and displacing the carotid sheath laterally. CT, computed tomography.
Following multidisciplinary discussion involving otolaryngology, neurosurgery, and radiology teams, a transcervical lateral approach was selected to avoid mandibulotomy, given the tumor’s accessibility and encapsulation. Intraoperatively, the tumor was identified deep to the sternocleidomastoid muscle, surrounded by a thin fibrous capsule. It was found to originate from the CSC, from which it was meticulously dissected using microsurgical techniques, with preservation of surrounding neurovascular structures including the vertebral artery (Figures 2 and 3).
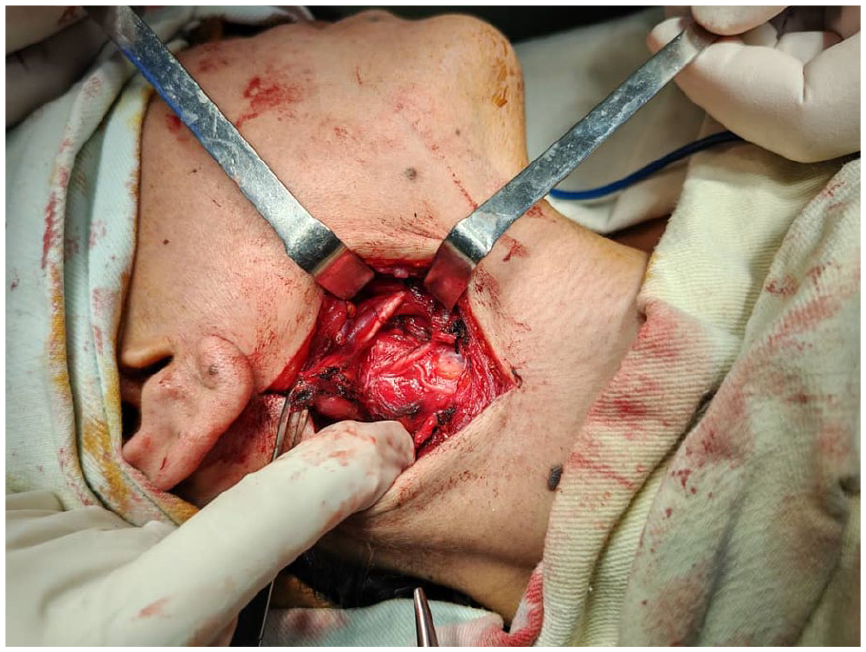
Intraoperative view showing a well-encapsulated parapharyngeal mass being meticulously dissected via a transcervical approach. The tumor is visualized deep to the sternocleidomastoid muscle, adjacent to the carotid sheath and vertebral artery.
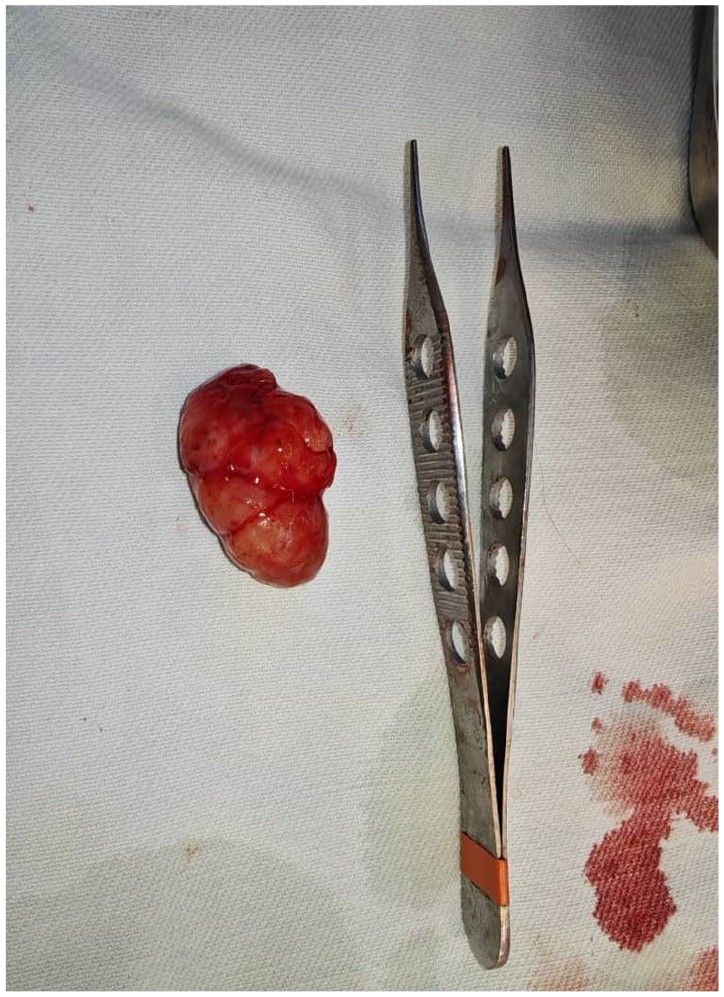
A small, round, well-circumscribed cervical mass measuring ≈2 cm in diameter, surgically excised and encapsulated by a thin fibrous capsule. The cut surface appeared gray-white with firm-to-rubbery consistency and a homogeneous, glistening appearance, showing no areas of necrosis or gross hemorrhage.
Frozen section analysis confirmed a benign spindle-cell neoplasm with no evidence of malignancy. Final histopathology revealed a well-encapsulated benign schwannoma composed of Antoni A areas with palisading nuclei forming Verocay bodies, and less cellular Antoni B areas with loose myxoid stroma. No atypical mitotic activity, necrosis, or tissue invasion was observed (Figure 4).
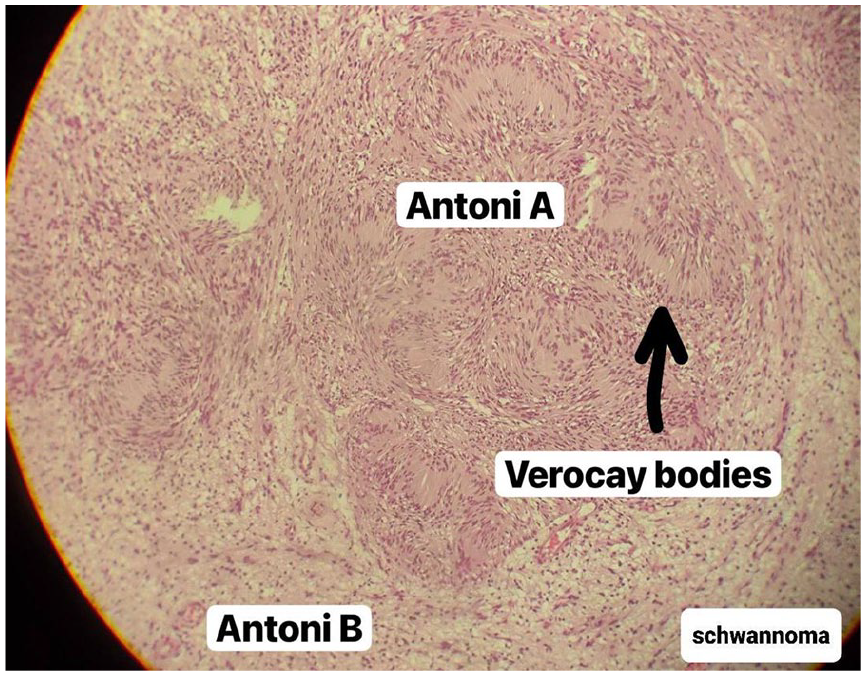
Photomicrograph of a schwannoma (H&E stain, ×100), demonstrating characteristic Antoni A and Antoni B areas. Verocay bodies are visible within the Antoni A region, formed by palisading of spindle cells around acellular zones.
The postoperative course was initially uneventful, with resolution of dysphagia within 4 weeks. However, within the first postoperative week, the patient reported the sudden onset of sharp, localized pain in the right submandibular region at the initiation of each meal—a clinical picture consistent with first-bite syndrome (FBS). This was attributed to iatrogenic disruption of postganglionic sympathetic fibers innervating the parotid gland during tumor dissection. Conservative management with reassurance and dietary modifications was initiated, resulting in gradual improvement in symptoms over the following weeks.
At 6-month follow-up, the patient remained asymptomatic with no radiological evidence of residual or recurrent disease on surveillance MRI. The long-term plan includes annual clinical evaluation for 5 years, given the low recurrence risk (<5% for encapsulated schwannomas).
Discussion
Parapharyngeal schwannomas were first described as distinct neurogenic tumors of the head and neck in early anatomical and surgical literature, though systematic characterization remains limited due to their rarity. Representing ~0.5% to 1% of all head and neck neoplasms, schwannomas in the PPS most commonly arise from the vagus nerve but may also originate from other cranial or peripheral nerves, including the CSC, hypoglossal nerve, and mandibular division of the trigeminal nerve.5-7 These tumors typically present in adults as slow-growing, often asymptomatic neck masses, although larger lesions can cause compressive symptoms such as dysphagia, odynophagia, or CN deficits. Radiologically, PPS schwannomas often appear as well-circumscribed, homogeneously enhancing masses on CT or MRI, but preoperative identification of the precise nerve of origin is frequently challenging.6,8
In our review of English-language case reports published between 1979 and 2025 using the keyword “parapharyngeal schwannoma,” we identified 54 documented cases, which we analyzed for patient demographics, tumor origin, clinical symptoms, radiologic features, complications, and management strategies. Including our present case, a total of 55 cases were reviewed.
The mean age at presentation was 38.0 ± 16 years (range: 5-75 years), with a female predominance (59%, n = 32/54). The most common nerves of origin were the vagus nerve (27%, n = 15/55), CSC (18%, n = 10/55), and hypoglossal nerve (13%, n = 7/55). Less common origins included the glossopharyngeal, mandibular (V3), lingual, and trigeminal nerves.
Radiologic assessment, primarily using MRI, showed well-circumscribed, encapsulated, T2-hyperintense lesions. However, several cases were misdiagnosed preoperatively, especially those originating from the CSC. These tumors often displaced the carotid sheath anteriorly—mimicking parotid tumors or carotid body paragangliomas—but did not produce the characteristic splaying of the internal and external carotid arteries seen in carotid body tumors, leading to diagnostic confusion.
Clinical manifestations included dysphagia (most common), lower CN palsies (IX-XII), and FBS—the latter being particularly associated with postoperative sympathetic denervation. Complications were reported in 81.8% (n = 45/55) of the cases, with the highest rates seen in schwannomas of the mandibular nerve, glossopharyngeal, and hypoglossal origins. Tumors originating from the CSC exhibited a 90.9% complication rate (10 out of 11 cases, including the present case), with Horner’s syndrome and FBS being the most characteristic findings. In our case, postoperative FBS further supported the tumor’s sympathetic origin.
Surgical resection was the primary treatment in nearly all cases. A transcervical approach was the most commonly used, although some cases required mandibulotomy or skull base access depending on size and location. Nerve-sparing techniques were often attempted, though complete preservation was not always feasible.
Our present case represents the 55th documented parapharyngeal schwannoma, and is unique in its confirmed origin from the CSC, intraoperatively dissected free from the vertebral artery and surrounding structures. Postoperative FBS, managed conservatively, retrospectively supported the sympathetic origin. This case highlights both the diagnostic challenges and the specific complication profile associated with sympathetic chain schwannomas, reinforcing the importance of high clinical suspicion and multidisciplinary planning in managing PPS tumors (Table 1 and Figures 5–7).
A Summary of Discussion Results.
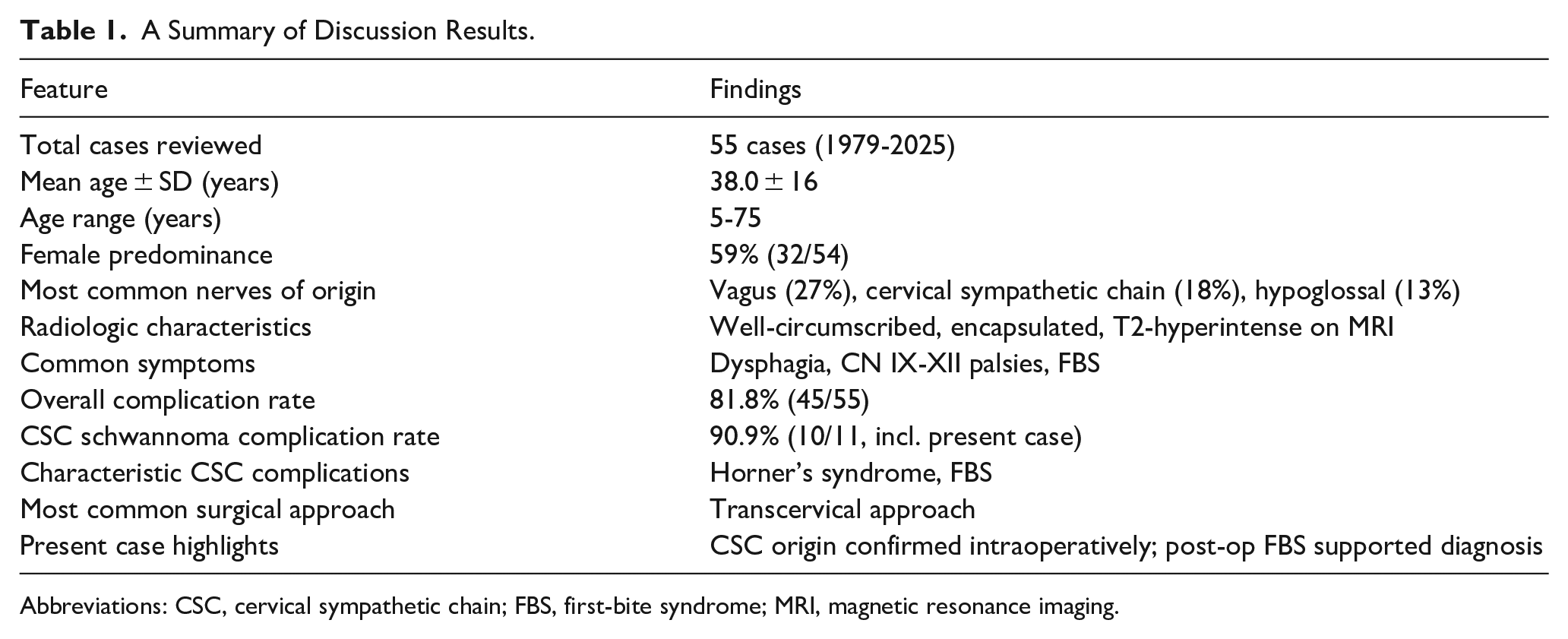
Abbreviations: CSC, cervical sympathetic chain; FBS, first-bite syndrome; MRI, magnetic resonance imaging.
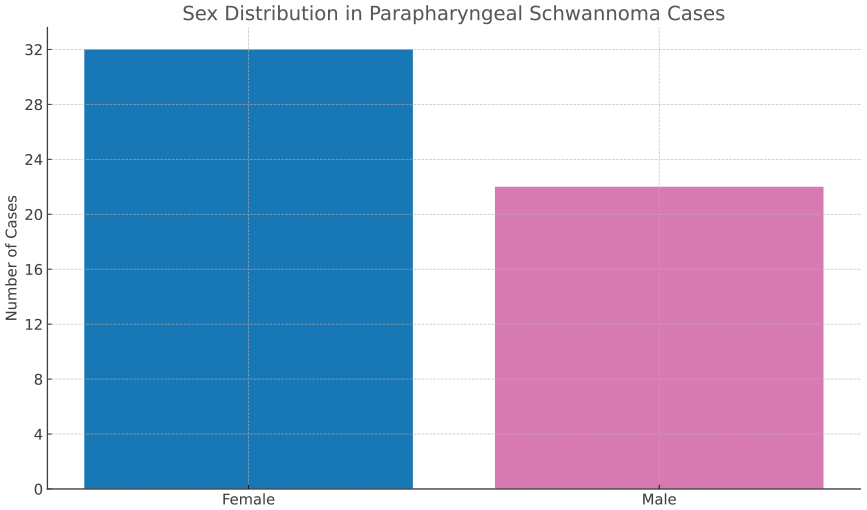
Sex distribution among 55 reported cases of parapharyngeal schwannoma. A female predominance was noted, with 59% (n = 32) of cases occurring in women, 38% (n = 21) in men, and 1 unspecified.
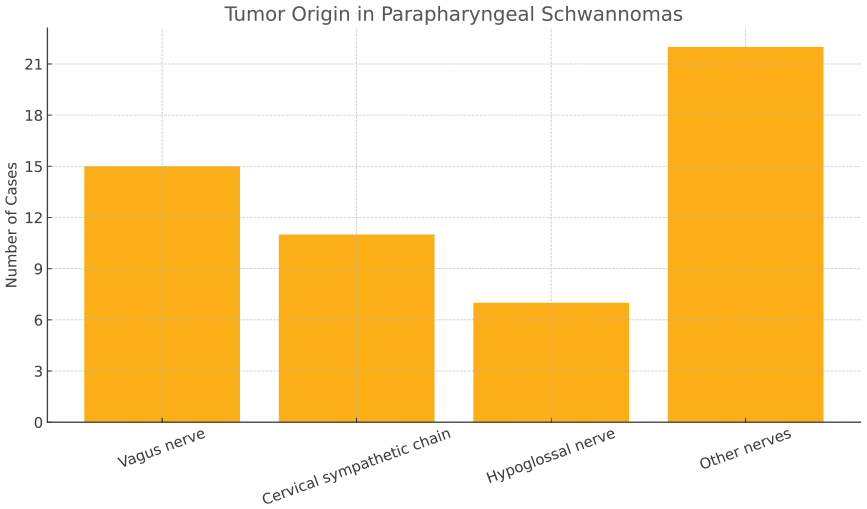
Tumor origin distribution in parapharyngeal schwannomas (n = 55). The vagus nerve was the most common origin (27%), followed by the cervical sympathetic chain (18%) and hypoglossal nerve (13%). Less frequent origins included the glossopharyngeal, mandibular (V3), lingual, and trigeminal nerves.
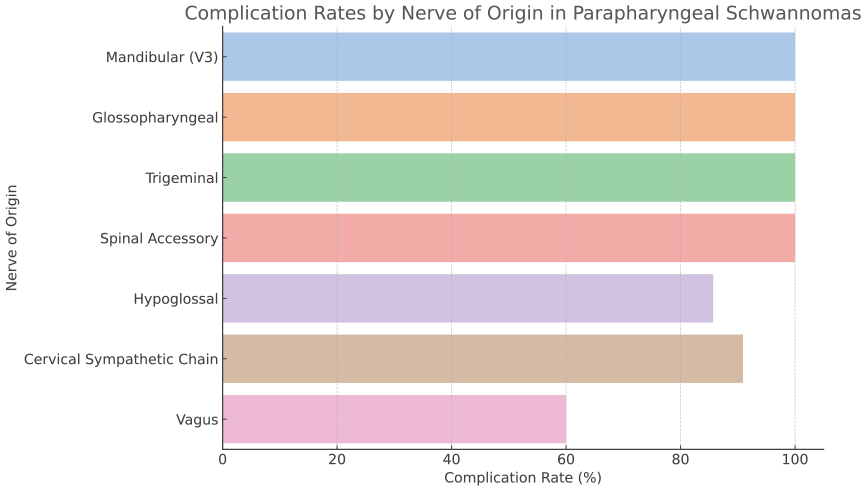
Postoperative complication rates by tumor origin. The highest complication rates were seen in schwannomas arising from the mandibular (V3), glossopharyngeal, and trigeminal nerves (100%), followed by the cervical sympathetic chain (90.9%), hypoglossal nerve (85.7%), and vagus nerve (60%).
PPS schwannomas are rare neurogenic tumors that often pose diagnostic challenges due to their deep anatomical location and subtle or absent clinical symptoms. Mild dysphagia may be the only presenting complaint when the mass compresses adjacent structures, highlighting the need for heightened clinical awareness. Radiologic imaging—particularly contrast-enhanced CT and MRI—plays a pivotal role in characterizing these lesions and planning surgical intervention. Complete surgical excision remains the definitive treatment, with outcomes depending on tumor size, nerve of origin, and intraoperative findings.
This case underscores the importance of including parapharyngeal schwannomas in the differential diagnosis of patients with vague pharyngeal symptoms, such as throat discomfort or mild dysphagia. Early recognition and appropriate imaging can facilitate timely intervention, minimize complications, and improve long-term outcomes, particularly when tumors originate from critical neurovascular structures such as the CSC.
Footnotes
Ethical Considerations
This case was conducted in accordance with the Declaration of Helsinki. Ethical approval was not required as per institutional policy for retrospective case reports.
Consent for Publication
Written informed consent for publication of this case and accompanying images was obtained from the patient.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analyzed during this case report are included in this published article. No additional data are available.