
Abstract
Objective:
Ectopic thyroid carcinoma is rare. We present an exceptionally rare case of primary retropharyngeal ectopic papillary thyroid carcinoma (PTC) coexisting with an orthotopic thyroid goiter, aiming to enhance clinical awareness of this condition and to emphasize the importance of comprehensive management of both the ectopic lesion and the orthotopic thyroid.
Methods:
Case report and literature review.
Results:
A 29-year-old male with a 3-year history of pharyngeal foreign body sensation underwent laryngoscopy and noncontrast CT/MRI, revealing a 2.0 × 3.5 cm left retropharyngeal mass. The mass was confirmed as papillary carcinoma via transoral excision. Postoperative contrast-enhanced CT identified metastatic-level VI lymphadenopathy, prompting total thyroidectomy with central neck dissection. Histopathology verified ectopic PTC with central node metastasis (1/20 nodes). Orthotopic thyroid exhibited nodular goiter without malignancy. No recurrence was observed during 36 months of follow-up.
Conclusions:
This case highlights retropharyngeal ectopic PTC’s diagnostic complexity in a patient with orthotopic thyroid gland. Management of ectopic thyroid carcinoma may be guided by thyroid carcinoma guidelines, given its rarity. Total thyroidectomy is recommended to exclude concurrent thyroid malignancy and enable thyroglobulin-based surveillance.
Keywords
Introduction
Thyroid ectopia, defined as functioning thyroid tissue located outside the thyroid gland’s usual anatomical position, results from failed caudal migration during embryogenesis.1-3 Ectopic thyroid tissue is typically found along the normal path of thyroid gland descent, from the foramen cecum at the base of the tongue to the sternal notch, with lingual locations being the most common.1,3,4 Neoplastic and nonneoplastic lesions (thyroiditis, thyroid nodules, and goiter) can occur in the ectopic thyroid tissue,1,5,6 but carcinoma is exceptionally rare.7,8 There is no consensus or established guidelines due to the rarity of the condition.
The retropharyngeal space, anatomically separate from the normal descent path, has not previously been reported as a site of ectopic thyroid carcinoma. Here, we present a rare and complex case involving ectopic papillary thyroid carcinoma in the retropharyngeal space with left cervical lymph node metastasis alongside orthotopic thyroid goiter. The management of orthotopic thyroid tissue in ectopic thyroid carcinoma patients is controversial, and we further propose management strategies for it.
Case Presentation
A 29-year-old male presented with progressive pharyngeal foreign body sensation over 3 years, accompanied by intermittent dysphagia. He denied any significant past medical history, including thyroid-related diseases, head-and-neck surgeries, and radiation exposure. Laryngoscopy identified a smooth submucosal mass on the left posterior pharyngeal wall, with preserved vocal cord mobility and normal epiglottic morphology. Neck computed tomography (CT) and magnetic resonance imaging (MRI) revealed a mass in the left retropharyngeal space with a diameter of 2.0 × 3.5 cm (Figure 1). Thyroid ultrasound showed a colloid nodule (TI-RADS 2) in the right lobe, with an unremarkable left lobe and no significant cervical lymphadenopathy.
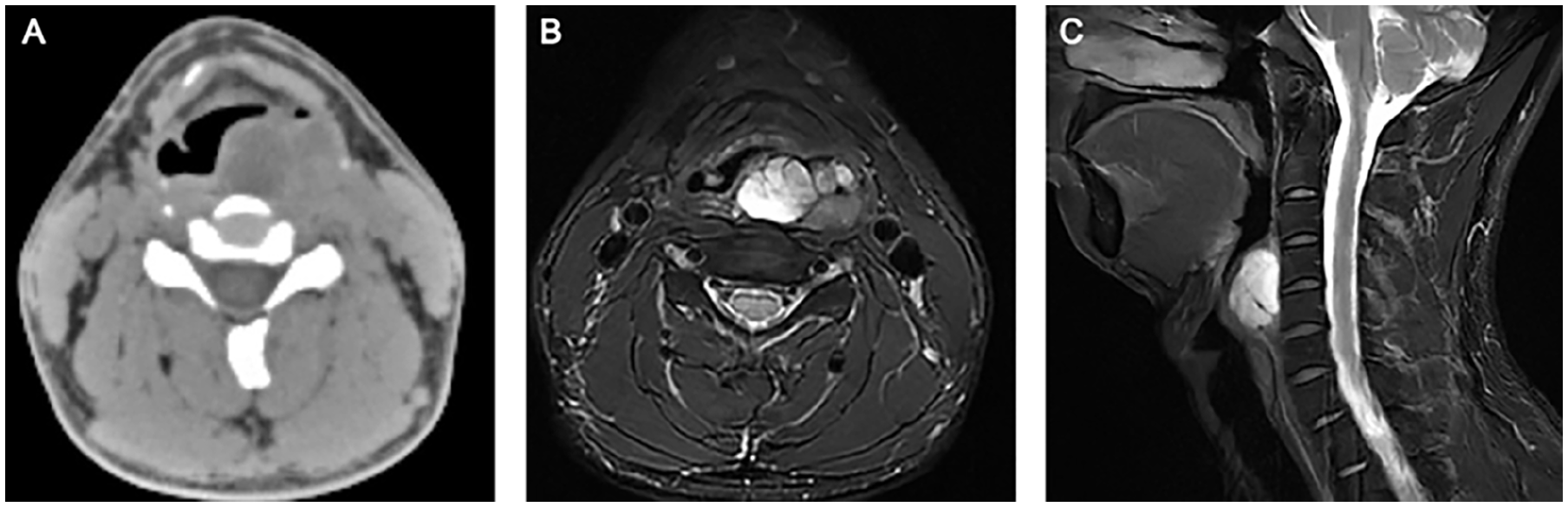
Axial CT (A) demonstrated a mass in the left retropharyngeal space, showing a complex cystic-solid lesion with heterogeneous attenuation. Axial T2-weighted MRI (B) and sagittal T2-weighted MRI (C) showed a left retropharyngeal mass with multinodular hypointense septations and heterogeneous signal, predominantly T2 hyperintense.
The patient underwent transoral CO₂ laser microsurgery (Figure 2), revealing a well-capsulated, lobulated mass (3.5 × 3.0 cm) in the left retropharyngeal space near the pyriform fossa. The lesion, located deep to the muscular layer, was completely excised. Intraoperative frozen section analysis suggested a benign fibrohyperplastic nodule with cystic changes and inflammatory infiltrates. However, definitive histopathology, however, revealed classic papillary thyroid carcinoma (1.5 × 1.3 cm) exhibiting capsular invasion. Immunohistochemistry confirmed thyroid differentiation (TTF-1+, thyroglobulin+, calcitonin−) with BRAF V600E positivity (VE1+), further supported by molecular evidence of BRAF c.1799T >A mutation.
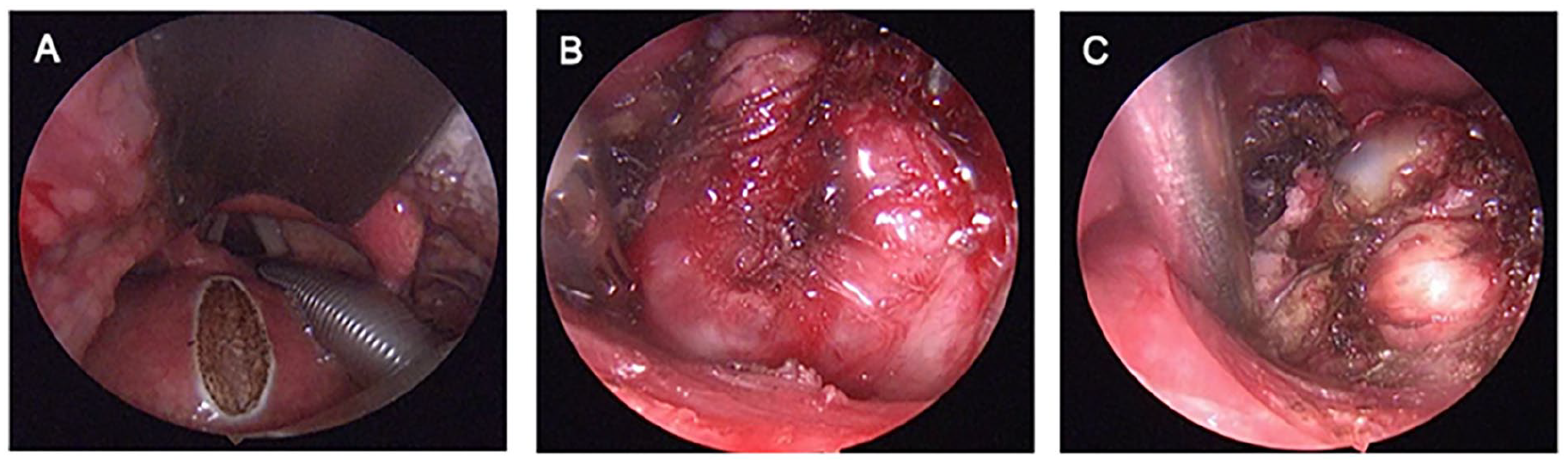
Transoral CO₂ laser resection. A smooth submucosal mass is observed on the left posterior pharyngeal wall adjacent to the pyriform sinus (A), demonstrating a well-encapsulated lesion (B) with lobulated architecture (C).
Consultation with the thyroid specialty department was requested. Thyroid hormone tests were normal. Contrast-enhanced CT showed scattered right thyroid nodules and a left level VI lymph node (0.65 × 0.27 cm). Postoperative levothyroxine suppression therapy and 1-month surveillance ultrasonography identified suspicious left level VI lymphadenopathy (0.65 × 0.27 cm, metastasis suspected). Total thyroidectomy with isthmus resection and bilateral level VI lymph node dissection confirmed multinodular goiter (bilateral thyroid) and metastatic involvement (1/10 left level VI nodes; 0/8 right). Final diagnosis: retropharyngeal ectopic thyroid carcinoma with left cervical lymph node metastasis. Following radioactive iodine-131 ablation, serial evaluations (laryngoscopy, ultrasonography, and thyroglobulin/thyroid function) over 36 months showed no recurrence.
Discussion
Ectopic thyroid tissue is a rare condition, with an estimated incidence of 1 in 100 000-300 000 in the general population and 1 in 4000-8000 among patients with thyroid disease. 2 The true incidence of thyroid ectopic is unknown due to the asymptomatic nature of some ectopic thyroid tissue. While the lingual location is the most prevalent, ectopic thyroid may occasionally occur in mediastinal, cardiac, esophageal, or other anatomical sites.1,3,9 Ectopic thyroid tissue is classified as accessory thyroid (with orthotopic thyroid gland) or aberrant thyroid (without), based on the presence of a normally located thyroid. 9 Primary thyroid carcinomas arising from ectopic thyroid tissue are uncommon.7,8 The existing literature is mostly isolated case reports. Even lingual thyroid carcinoma, the most common ectopic subtype, has very few documented cases. 10 No retropharyngeal ectopic thyroid carcinoma cases have been reported to date.
Ectopic thyroid tissue is typically asymptomatic. Clinical manifestations correlate with the lesion’s location, size, and complications such as hemorrhage or malignant transformation. 3 Approximately one-third of patients develop hypothyroidism. 9 The underlying mechanisms may involve developmental hypoplasia of ectopic thyroid tissue (limiting adequate thyroid hormone production) or coexisting small/hypofunctional orthotopic thyroid glands in patients with accessory thyroid tissue.
Diagnosing ectopic thyroid carcinoma is challenging, especially when orthotopic thyroid tissue coexists. In our case, the patient presented preoperatively with a retropharyngeal mass and a concurrent orthotopic thyroid gland, and ectopic thyroid papillary carcinoma was ultimately confirmed via histopathological examination. Thyroid scan remains the primary diagnostic tool for ectopic thyroid, enabling identification of all radioisotope-avid ectopic foci outside the orthotopic thyroid gland in the neck. 11 Ultrasound, a noninvasive and cost-effective modality, should be used to evaluate both the mass and the location of the native thyroid to assess the presence of concurrent orthotopic thyroid tissue. 12 CT and MRI allow precise assessment of ectopic thyroid size and anatomical relationships, particularly in deep-seated locations such as the retropharyngeal space.13,14 Fine-needle aspiration (FNA) is critical for diagnosing ectopic thyroid lesions and remains the only reliable method to differentiate benign from malignant pathologies. 13
There is no consensus about the optimal therapeutic strategy due to the rarity of the condition. Asymptomatic patients with ectopic thyroid tissue demonstrating euthyroid status and benign cytological features may be managed with surveillance. Therapeutic intervention is recommended for cases presenting with hypothyroidism, local symptoms (eg, hemorrhage), complications (eg, respiratory distress, dysphagia), or malignant transformation. Treatment strategies, including thyroid hormone replacement therapy or surgical resection, depend on the location of the ectopic tissue, patient age, and functional status of the orthotopic thyroid gland.1,3,11,15
Ectopic thyroid carcinoma, with a malignant transformation rate below 1%, is exceedingly rare. 7 Management could be guided by established guidelines for thyroid carcinoma. Treatment must consider primary tumor size, extrathyroidal extension, lymph node metastasis, patient age, and comorbidities. 16 Papillary thyroid carcinoma is the most common subtype, 8 for which surgical resection is the primary treatment, followed by adjuvant thyroid hormone suppression therapy and radioactive iodine therapy as clinically indicated. 16
The management of orthotopic thyroid tissue in ectopic thyroid carcinoma patients is controversial. For euthyroid patients without evidence of orthotopic lesions, the decision to perform total thyroidectomy poses a clinical dilemma. Some choose surveillance to avoid surgery and lifelong hormone replacement, while others advocate total thyroidectomy to distinguish ectopic from metastatic thyroid cancers.17,18 We recommend total thyroidectomy for these patients, given the potential for residual thyroid tissue elsewhere and unclear metastatic patterns. This approach serves 2 purposes: (1) exclude occult orthotopic thyroid pathology, and (2) enable postoperative radioactive iodine therapy to facilitate recurrence monitoring. In this case, the ectopic carcinoma was in the left retropharyngeal space, a rare site outside the embryonic thyroid descent path. Left level VI cervical lymphadenopathy was suggestive of metastatic involvement. Total thyroidectomy was done, and histopathology confirmed metastasis in left level VI lymph nodes. Postoperative management included thyroid hormone suppression and adjuvant radioactive iodine treatment. No recurrence was detected during follow-up.
Conclusion
Ectopic thyroid is a rare condition. When evaluating a retropharyngeal mass, ectopic thyroid should be considered. Thyroid scan is the main diagnostic method. There’s no consensus or guideline for treating ectopic thyroid carcinoma due to its rarity. Treatment should consider the patient’s condition and refer to thyroid carcinoma strategies. Also, the orthotopic thyroid needs active management to avoid missed diagnoses and aid follow-up monitoring.
Footnotes
Acknowledgements
The authors thank all the members of Department of Otorhinolaryngology—Head and Neck Surgery, the Second Affiliated Hospital, School of Medicine, Zhejiang University, for their invaluable help.
Ethical Considerations
The study was approved by the Ethics Committee of the Second Affiliated Hospital, School of Medicine, Zhejiang University (Approval No.2024-1299).
Consent to Participate
Written informed consent was obtained from the patients for their anonymized information to be published in this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work is supported by the National Natural Science Foundation of China (number: 82401338).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.