
Abstract
Kawasaki disease (KD) is a cryptic and self-limiting vasculitis predominantly seen in children, often posing a diagnostic challenge due to its varied clinical presentations. Among these, the emergence of deep neck infections, particularly retropharyngeal abscesses, stands out as an extremely rare manifestation. Herein, we present a case of a 10-year-old girl who was hospitalized for fever, neck pain, swollen cervical lymph nodes, and increased inflammation markers. Although anti-infective treatment was initiated, her condition remained unchanged. A cervical computed tomography scan revealed an abscess in the retropharyngeal space. Remarkably, on the third day post-admission, the patient developed symptoms synonymous with KD, such as conjunctival redness, reddened lips, and a strawberry tongue. Subsequent treatment with high-dose intravenous immunoglobulins (IVIG) and oral aspirin led to swift symptom relief, including complete abscess resolution verified by a follow-up neck magnetic resonance imaging. This unique co-presentation of KD and a retropharyngeal abscess, possibly linked to infections like Streptococcus or Staphylococcus aureus, underscores the importance of quick diagnosis and KD management, especially when conventional treatments prove ineffective.
Introduction
Kawasaki disease (KD) is the leading cause of acquired heart disease in children in developed countries. 1 The classic presentation of KD includes fever, variable rash, non-purulent cervical lymphadenopathy, conjunctival redness, strawberry tongue, diffuse redness of the lips and oral mucosa, and redness and swelling of the palms and soles in the early stage, followed by peeling of the skin around the nails as the patient recovers. However, KD can sometimes present in atypical ways, which can make diagnosis difficult and potentially delay treatment. Rarely, KD may present only as unexplained fever, redness at the site of Bacille Calmette-Guérin (BCG) vaccination, or desquamation around the anus. Initially, KD presenting with deep neck infections (DNI) is extremely rare.
Case Presentation
A 10-year-old girl was admitted to the hospital with an 8-day history of fever and pain posterior to the left auricle. The fever was moderate to high, peaking at 40°C, and the pain posterior to the left auricle progressively radiated to the left side of her neck, severely impeding her neck mobility. She also suffered significant pharyngeal pain, dysphagia, foreign body sensation during deglutition, and pronounced behavioral alterations, including irritability and rapid agitation. She had previously sought medical intervention at an Otolaryngology Department in another hospital, where a physical examination revealed a constricted pharynx, edema of the posterior pharyngeal wall, and purulent discharge from the piriform sinus, as evidenced by indirect laryngoscopy. Laboratory findings were as follows: blood routine examination: white blood cell count (WBC): 19.8 × 109/L, percentage of neutrophils (N%): 87.4, percentage of lymphocytes (L%): 10.2, hemoglobin (Hb): 137 g/L, platelets (PLT): 287 × 109/L, C-reactive protein (CRP): 54.6 mg/L. Neck computed tomography (CT) suggested a left parapharyngeal space infection with abscess formation. Due to the profundity of the abscess and associated surgical risks, the Head and Neck Surgery Department advocated conservative treatment with cephalosporin antibiotics and metronidazole. However, her symptoms remained unrelenting after a 6-day course of treatment, necessitating a transfer to our hospital for further treatment.
Upon admission, the physical examination showed swelling and tenderness of the skin behind the left ear and neck, cervical lymphadenopathy, and diffuse red lips. However, he had no strawberry tongue, abnormal ear discharge, swelling of the palms or soles, or desquamation around the nails. Repeat blood tests showed the following: WBC: 20.7 × 109/L, N%: 89.5, Hb: 108 g/L, PLT: 321 × 109/L, and CRP: 80.4 mg/L. A lumbar puncture was performed and the cerebrospinal fluid analysis was normal. She was treated with ceftriaxone and metronidazole for infection. On the second day of hospitalization, she continued to have a high fever and irritability, with persistent pain behind her left ear and neck, and developed redness and discomfort in both eyes. Her treatment was increased with vancomycin and tobramycin eye drops for relief of symptoms. On the third day of hospitalization, her fever decreased slightly (38.5°C) and her ear and neck pain was somewhat relieved, but she developed more pronounced redness in the eyes and lips and a strawberry tongue appeared. Additional laboratory tests showed elevated liver enzymes (ALT: 263 U/L, AST: 62 U/L) and an elevated sedimentation rate of erythrocytes (67 mm/h). Her urine analysis showed pyuria, but she did not have symptoms of urinary tract infection. The echocardiogram showed normal left ventricular systolic function and coronary arteries, but mild mitral and tricuspid regurgitation. Neck CT revealed a hypoattenuating lesion in the left retropharyngeal space with peripheral enhancement, along with lymphadenopathy in the posterior cervical space (Figure 1). After reevaluating the patient’s clinical presentation and laboratory findings, a diagnosis of incomplete Kawasaki disease (iKD) was made. The patient was treated with intravenous immunoglobulin (IVIG) at a dose of 2 g/kg and aspirin at a dose of 50 mg/kg/day. Within 24 h of starting this treatment, the patient’s fever, pain behind the left ear and neck, and other symptoms of KD improved dramatically. On the sixth day of hospitalization, repeated laboratory tests showed normalization of WBC and CRP levels and a significant decrease in erythrocyte sedimentation rate. A follow-up neck magnetic resonance imaging (MRI) showed complete resolution of the abscess. The patient was discharged with a maintenance dose of aspirin (5 mg/kg/day).
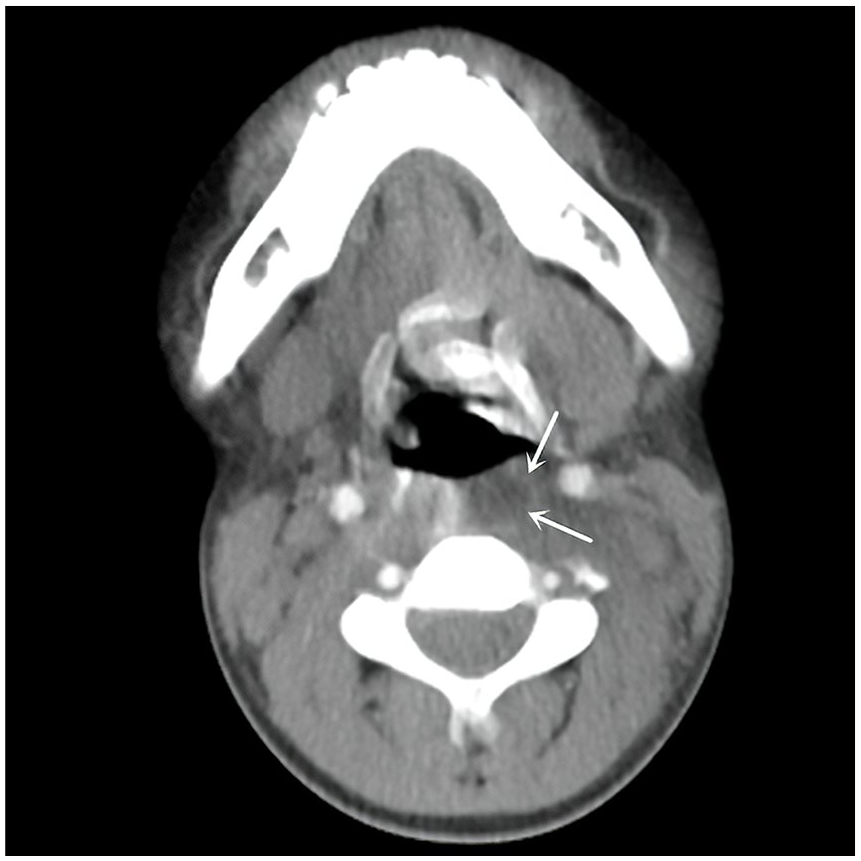
Neck computed tomography showed a hypodense lesion in the left retropharyngeal space with peripheral enhancement (arrow).
Discussion
DNI, which includes retropharyngeal, parapharyngeal, and peritonsillar abscesses, is a rare manifestation in KD. 2 In this case, the patient’s primary symptom was a retropharyngeal abscess, evident through recurring fever, pain behind the left ear and neck, sore throat, dysphagia, enlarged cervical lymph nodes, and accompanying personality alterations such as irritability and agitation. Despite active anti-infective therapy, while fever peaks were reduced, they did not normalize. The patient later developed characteristic symptoms of KD, including conjunctival congestion, red lips, and strawberry tongue, in addition to standard manifestations of KD such as significantly elevated CRP and ESR levels, increased liver transaminases, and aseptic pyuria. Echocardiography did not reveal any coronary artery lesions but did show regurgitation in the mitral and tricuspid valves. According to the 2020 KD guidelines set by the JCS/JSCS, 3 the patient was diagnosed with iKD. After high-dose intravenous immunoglobulin treatment, the patient no longer experienced fever or pain behind the left ear and in the neck. The symptoms of conjunctival congestion, red lips, and strawberry tongue resolved, and the patient’s mental state improved considerably. Abnormal laboratory tests and echocardiogram, as well as cervical MRI findings, returned to normal after follow-up.
The neck manifestations of KD are often misdiagnosed because of their rarity, and otolaryngologists should be aware of the need for timely intervention.4,5 A lack of liquefaction in pharyngeal fine-needle aspirations is characteristic of KD rather than bacterial DNIs.5 -8 A retrospective analysis by Yu et al. of 24 KD patients with retropharyngeal abscess-like edema revealed that none met the KD diagnostic criteria at presentation. 9 These patients initially presented with fever and various neck symptoms, including neck pain, tender neck mass, torticollis, and limited neck mobility. All patients received empirical antibiotics initially but did not show a response. As symptoms progressed, they aligned more with complete or incomplete KD. All responded well to intravenous immunoglobulin therapy, confirming KD, especially in atypical cases. Similarly, Kasem et al. noted in their literature review similar presentations above and also found that KD patients with abscess-like lesions were predominantly male (82%), with ages ranging from 10 months to 9 years, and an average age of 5 years—higher than the average for KD patients. 10 The patient in this case also fits within this age profile, suggesting a potential demographic pattern in KD with abscess-like presentations that could guide future research on gender and age factors in atypical KD.
The etiological correlation between retropharyngeal inflammation and KD remains uncertain. Some researchers attribute this inflammation to non-infectious vasculitis,11 -13 while others believe bacterial superantigens may be involved. 14 The detection of streptococcal DNA in KD cases with neck involvement adds complexity to our understanding of the condition.15,16 In addition, Choi et al. described the case of a 3-year-old patient diagnosed with KD, who experienced recurrent pain in the left neck. The patient received two doses of IVIG (2 g/kg/day) and aspirin (80 mg/kg/day) on the day of hospitalization and the fourth day. Although KD symptoms subsided, neck pain persisted and became severe torticollis. Neck CT revealed an irregular thick-walled low-density lesion in the left lymph node, suggesting a parapharyngeal abscess. After abscess drainage, neck pain improved and a pus culture showed the presence of Staphylococcus aureus. 17
Neck CT scans can aid in the diagnosis of retropharyngeal cellulitis or abscess. Holt et al. defined the CT characteristics of a deep neck abscess as cystic appearance, low-density CT values, the presence of air or fluid in the center of the suspicious area, and peripheral enhancement. 18 In children with KD, cellulitis often does not show a “peripheral enhancement” on CT, and the involvement is usually long segmental.8,9 Consequently, retropharyngeal inflammation caused by KD often presents as low-density lesions in the retropharyngeal space on CT. In such cases, intravenous immunoglobulin treatment can be effective, and there is no need for surgical drainage.
Generally, the continuation of antibiotic therapy post-diagnosis is not recommended for patients with KD, as it may worsen systemic vasculitis. However, the appearance of a retropharyngeal abscess on CT imaging can often imply the potential for a purulent bacterial infection, which could be implicated in the pathogenesis of KD. Findings in our patient echoed those reported by Choi et al., with CT demonstrating tissue wall thickening and peripheral enhancement, consistent with abscess formation. 17 Following the initial treatment with vancomycin, the patient exhibited a decrease in fever spikes and improvement in neck pain, yet recurrent febrile episodes persisted. Subsequent administration of intravenous immunoglobulin and aspirin resulted in complete symptom resolution and the gradual disappearance of the neck abscess, circumventing the need for drainage surgery. Consequently, empirical antibiotic treatment should still be considered in KD patients with CT findings indicative of peripheral enhancement and suspected retropharyngeal abscess formation.
In conclusion, clinicians must remain vigilant for patients with DNI who exhibit a poor response to initial intravenous antibiotics, as this could be indicative of early manifestations of KD. It is essential to recognize that the presence of a deep neck abscess in KD is not an indication of surgery, and the timely initiation of KD-specific treatment is paramount.
Footnotes
Acknowledgements
Not applicable.
Author Contributions
JC collected the data, reviewed literature, and drafted the manuscript. YW read and approved the final manuscript. All authors read and approved the manuscript.
Availability of Data and Materials
All data analyzed during this study are included in the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
This study was approved by the Research Ethics Committee of West China Second University Hospital, Sichuan University.
Consent for Publication
Informed consent was obtained from the patient’s family member for publication of this case report.