
Abstract
Migration of the embryonic thymus is thought to be the basis for the formation of ectopic thymic tumors. Thymic ectopy may be a result of the abnormal migration of the third or fourth branchial cleft to the anterior mediastinum during weeks 5–6 of embryonic development. However, ectopic thymic carcinoma has highly nonspecific histologic features and occurs in variable and unpredictable locations making it difficult to diagnose. However, the clinical diagnosis and treatment should not overlook the possibility of ectopic thymic tumors. Here, we report a case of ectopic thymic carcinoma diagnosed as thyroid cancer before surgery occurring in a location consistent with current assumptions. Furthermore, we briefly review the literature on ectopic thymic carcinoma and discuss current diagnostic and treatment approaches.
Background
Thymic ectopia may be a result of the abnormal migration of the third or fourth branchial cleft to the anterior mediastinum during the 5th–6th weeks of embryonic development. Ectopic thymus tissue can occur in the parotid gland, 1 mandible, lateral cervical area, 2 thyroid area, 3 paratracheal region, pericardium, 4 thorax, 5 and pleura. 6 The cervical region is the most common site for ectopic thymic neoplasms. Neoplastic and non-neoplastic lesions can occur in the ectopic thymic tissue. Adenomas are the most predominant tumor lesions, while adenocarcinoma is rare.
Here, we report a case of ectopic thymic carcinoma diagnosed as thyroid carcinoma before surgery.
Patient summary
On examination, a mass approximately 2 cm in diameter was found on the dorsal side of the left lobe of the thyroid gland in a 66-year-old man. The lump was hard, had poor mobility, and caused no discomfort for the patient. The patient's family and personal history were unremarkable. A thyroid ultrasound showed that the nodule was adjacent to the left parathyroid gland (Figure 1A), and the lymph nodes in zone II and III of the neck were imaged. A computed tomographic scan of the neck revealed an approximately 2.4 × 1.7 cm tumor/nodule on the dorsal side of the left lobe of the thyroid (Figure 1B). Thyroid function and corresponding antibodies were within normal reference ranges. Cytology of a fine-needle aspiration showed atypical hyperplasia of thyroid epithelial cells and a malignancy could not be excluded. The presumptive diagnosis was a thyroid tumor or lymphoma. The results of preoperative imaging examination. (A). Neck ultrasound showed a 2.9 × 1.8 × 2.1 cm hypoechoic nodule on the dorsal side of the left lobe of the thyroid gland that was irregular in shape, lobulated, and close to the left common carotid artery and trachea. There are abundant blood flow signals within the nodules. (B). An enhanced computed tomographic scan of the neck revealed a tumor/nodule approximately 2.4 × 1.7 cm in size with a moderately enhanced soft tissue shadow on the dorsal side of the left lobe of the thyroid (in the yellow circle).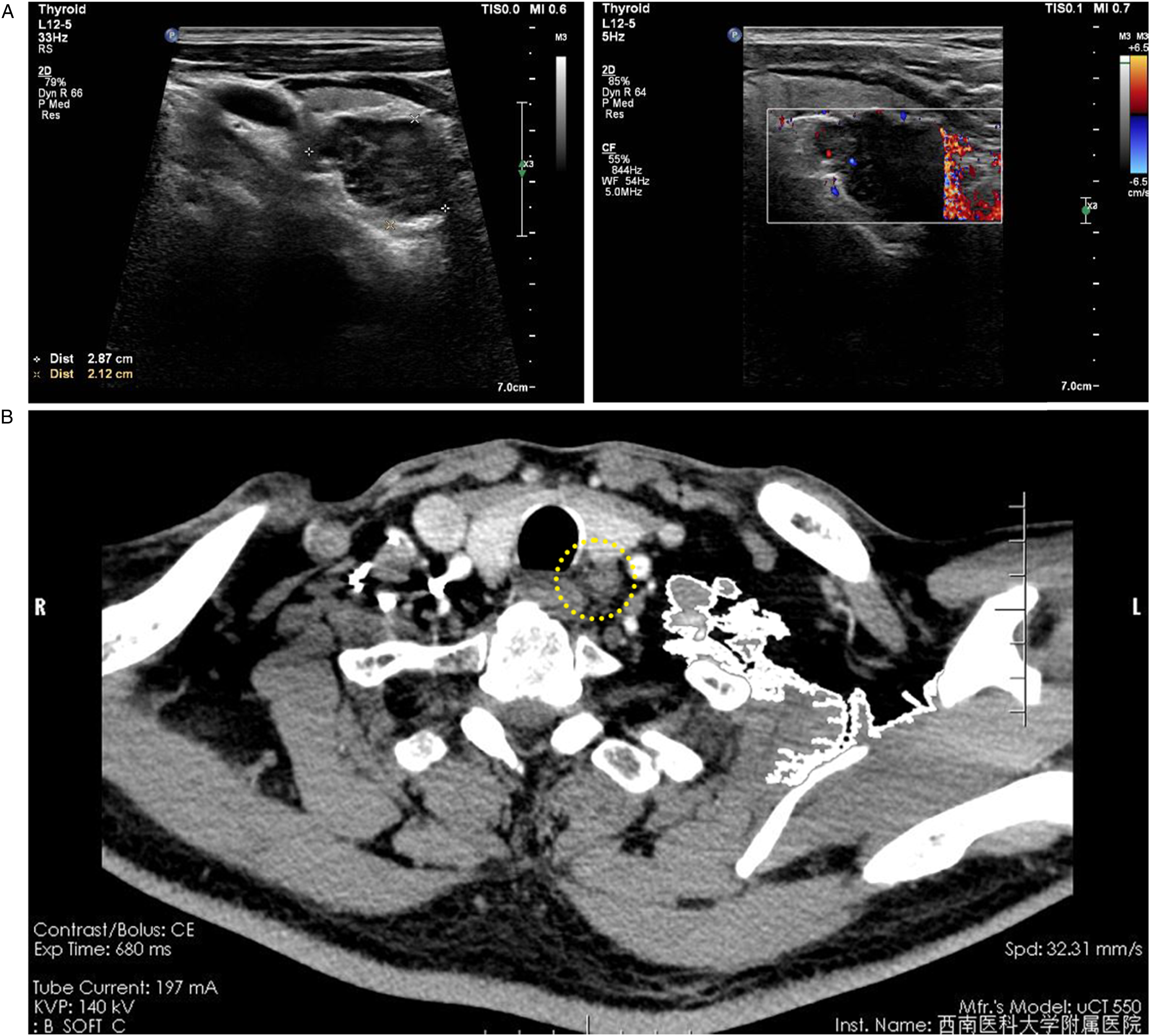
During the operation, gray and yellow irregular tissue was found behind the left thyroid gland adhered to the thyroid lobe and was separate from the mediastinal thymus. The left lobe of the thyroid gland and mass were removed and the sentinel lymph node was negative (Figure 2A). The solid mass measured approximately 2.5 × 1.8 × 1.5 cm, and a section of it was gray and brittle (Figures 2B and 2C). Intraoperative frozen sections showed benign thyroid lesions and a solid mass consistent with squamous cell carcinoma. Postoperative pathological sections verified the nodular goiter (Figure 2D), and no metastasis were found in the central lymph nodes (Figure 2E). The mass was diagnosed as thymic squamous cell carcinoma and was positive for CK, CK19, p63, CD5, CD20, CD117, p53 (60%), and Ki-67 (20%, Figures 2F and 2G). Intraoperative and postoperative pathological findings of the cervical nodules. (A). Location diagram of the cervical nodules. (B). The nodule located on the dorsal side of the left lobe of the thyroid was separated from the thyroid tissue. The section of the nodule consisted of a tough, gray, fish-like tissue. (C). The thyroid follicles varied in size. Interfollicular tissue edema and inflammatory cell infiltration were observed. The pathological diagnosis was a nodular goiter. (Hematoxylin and eosin, ×40) (D). Lymphofollicular hyperplasia was found within the lymph nodes of the central neck area and no malignant lesions were found. (Hematoxylin and eosin, ×100) (E). Immunohistochemical CD117 staining in the epithelial cells of the nodules were positive. (Immunoperoxidase,×200) (F). Immunohistochemical staining of p63 in epithelial cells of the nodules were positive. (Immunoperoxidase,×200).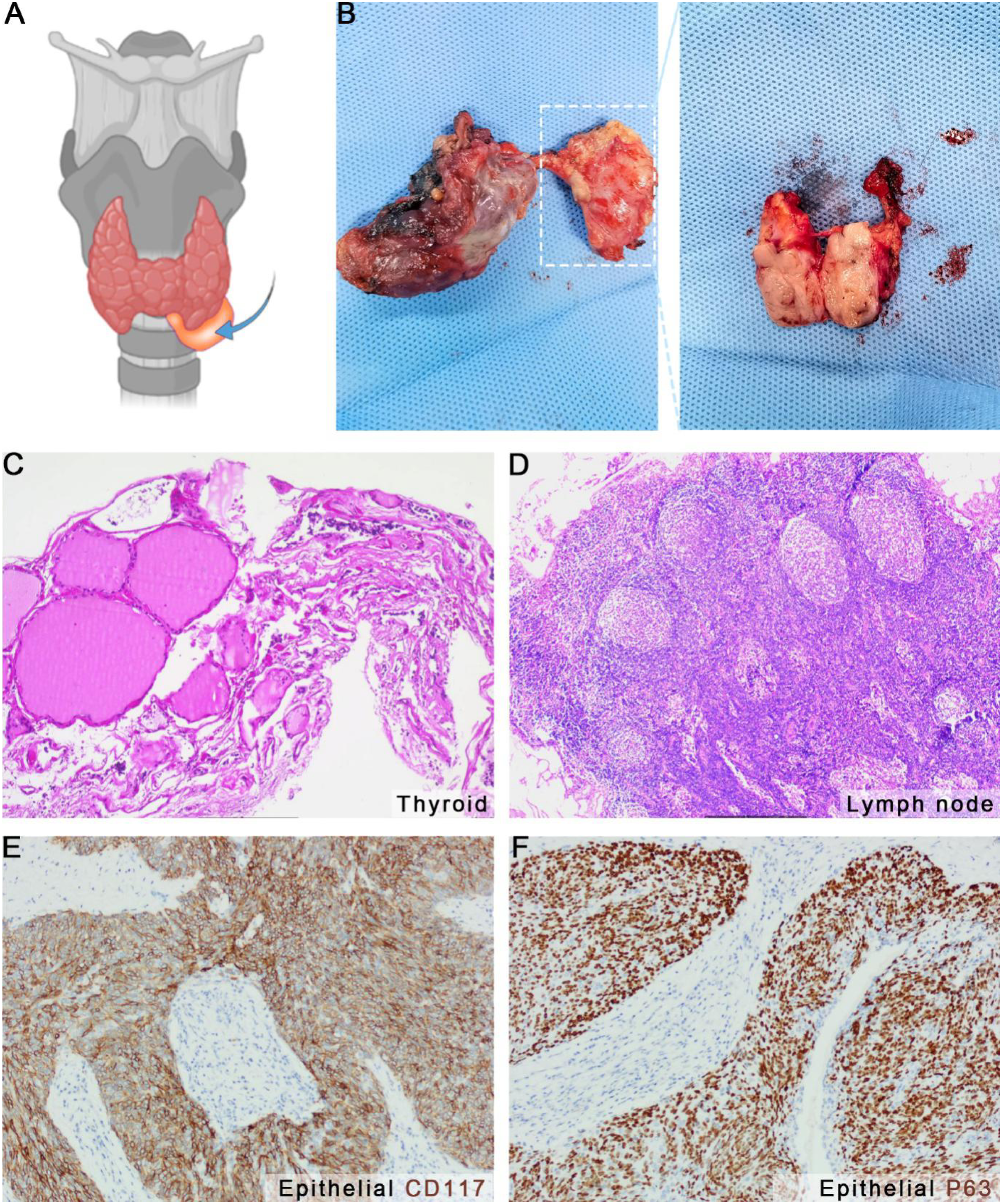
Discussion
Our case study describes an asymptomatic neck mass in an older man. Due to its location and cytological results of a fine-needle aspiration, the preliminary diagnosis was a thyroid tumor or lymphoma. However, the postoperative pathological report confirmed that it was a thymic carcinoma. Pathologic and immunohistochemical evidence supported that this thymic carcinoma was caused by abnormal thymic migration during embryonic development.
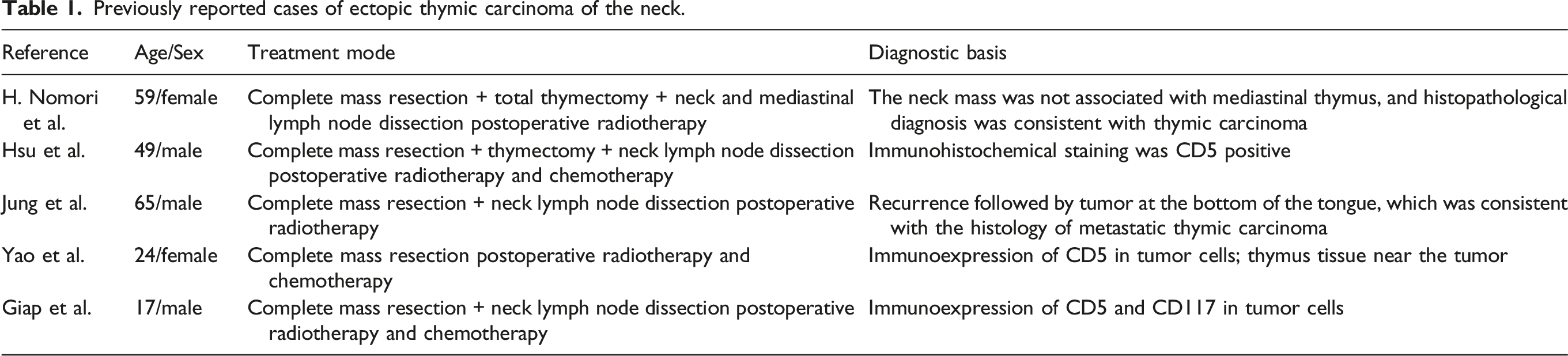
Previously reported cases of ectopic thymic carcinoma of the neck.
Footnotes
Author Contributions
Data curation: Wei Wang, Jia-Ying Xu, and Bo-Tao Zhang; Writing – original draft: Wei Wang; Writing – review and editing: Jun Jiang.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:This study was supported by the National Natural Science Foundation of China (82070288), the Science & Technology Department of Sichuan Province (2022YFS0627), the Health Commission of Sichuan Province (21PJ100), the Talent Development Project of The Affiliated Hospital of Southwest Medical University (20062).
Statement of Informed Consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.