
Abstract
Adenoidectomy, routinely performed for pediatric obstructive symptoms, typically reveals benign lymphoid hyperplasia. We report the first documented case of a primary clear cell microcystic adenoma within adenoid tissue in a 12-year-old male undergoing adenotonsillectomy for chronic snoring, recurrent tonsillitis, and mouth breathing. Intraoperative examination identified an unusual homogenous grayish-white adenoid mass. Histopathological analysis demonstrated benign epithelial hyperplasia with focal clusters of clear cells arranged in microcystic patterns, morphologically aligning with a low-grade microcystic adenoma—a lesion classically linked to von Hippel-Lindau (VHL) syndrome. This case emphasizes the critical role of histopathological scrutiny in routine surgical specimens, as incidental findings may reveal rare neoplasms with significant syndromic implications. While the lesion exhibited benign features, its histological resemblance to VHL-driven neoplasms necessitates vigilant long-term surveillance. This report advocates for multidisciplinary collaboration in managing such cases and highlights the importance of genetic assessment to guide familial screening. Further documentation of similar cases is required to establish this entity’s clinical and molecular profile, refining diagnostic approaches for nasopharyngeal clear cell lesions.
Introduction
The pharyngeal tonsil, commonly referred to as the adenoid, is a fundamental component of Waldeyer’s ring, serving a critical role in the immunological surveillance of the upper aerodigestive tract. 1 In the pediatric population, adenoidectomy is a frequently performed surgical procedure, primarily indicated for chronic inflammation and hypertrophy leading to obstructive symptoms. 2 Histopathological evaluation of these specimens most commonly reveals benign lymphoid hyperplasia, reflecting a reactive process. 1 While the nasopharynx may be the site of various neoplasms, primary tumors originating from the adenoid tissue are exceptionally uncommon. 3 Clear cell neoplasms represent a diverse group of tumors that can be found in multiple organs; their differential diagnosis can include everything from benign adenomas to adenoid cystic carcinomas. 4 In the head and neck region, rare, low-grade clear cell tumors, such as microcystic adenomas, have been identified in the sinonasal tract and are often associated with von Hippel-Lindau (VHL) disease.5,6 The pancreas is another well-documented site for VHL-associated cystic lesions and microcystic adenomas. 7 However, the development of a primary clear cell neoplasm within the adenoid tissue proper has not been previously documented in the medical literature.
We report the case of a 12-year-old male who underwent adenotonsillectomy for obstructive symptoms and was found to have an incidental and histologically unique clear cell neoplasm of the adenoid, a finding that, to our knowledge, is the first of its kind to be described.
Case Presentation
A 12-year-old male presented to the otolaryngology clinic with a multi-year history of recurrent tonsillitis accompanied by nocturnal snoring, chronic mouth breathing, and intermittent joint pain. His medical history included recurrent, self-limiting episodes of epistaxis occurring once to twice monthly, each resolving spontaneously within minutes without requiring emergency intervention. There was no prior surgical history or significant comorbidities. Physical examination revealed grade 3 bilateral palatine tonsillar hypertrophy. Laboratory evaluations, including complete blood count and inflammatory markers, were within normal ranges. Given the refractory nature of his symptoms and obstructive findings, a decision was made to proceed with tonsillectomy and adenoidectomy under general anesthesia. Intraoperatively, the procedure was uneventful; however, the resected adenoid tissue demonstrated an abnormal macroscopic appearance, featuring smooth, homogenous grayish-white firm tissue distinct from typical adenoid architecture. Specimens were promptly sent for histopathological analysis. In the immediate postoperative period, the patient developed bilateral epistaxis, successfully managed with topical antibiotic ointment-impregnated anterior nasal packing. The packs were removed after 48 hours with no further bleeding or complications. Histopathological evaluation confirmed benign adenoid epithelial hyperplasia without evidence of dysplasia. Foci of clear cells with microcystic architectural patterns were identified, consistent with a primary microcystic clear cell adenoma (Figure 1). The patient’s postoperative recovery was uncomplicated, with resolution of preoperative symptoms at follow-up. Despite histological similarities to VHL-associated tumors, no syndromic stigmata or family history were identified. At that time, the family declined further VHL screening investigations. Consequently, VHL testing was postponed, with the family counseled and referred to appropriate specialists for subsequent completion of the child’s evaluation. The clinical situation was thoroughly explained to them.
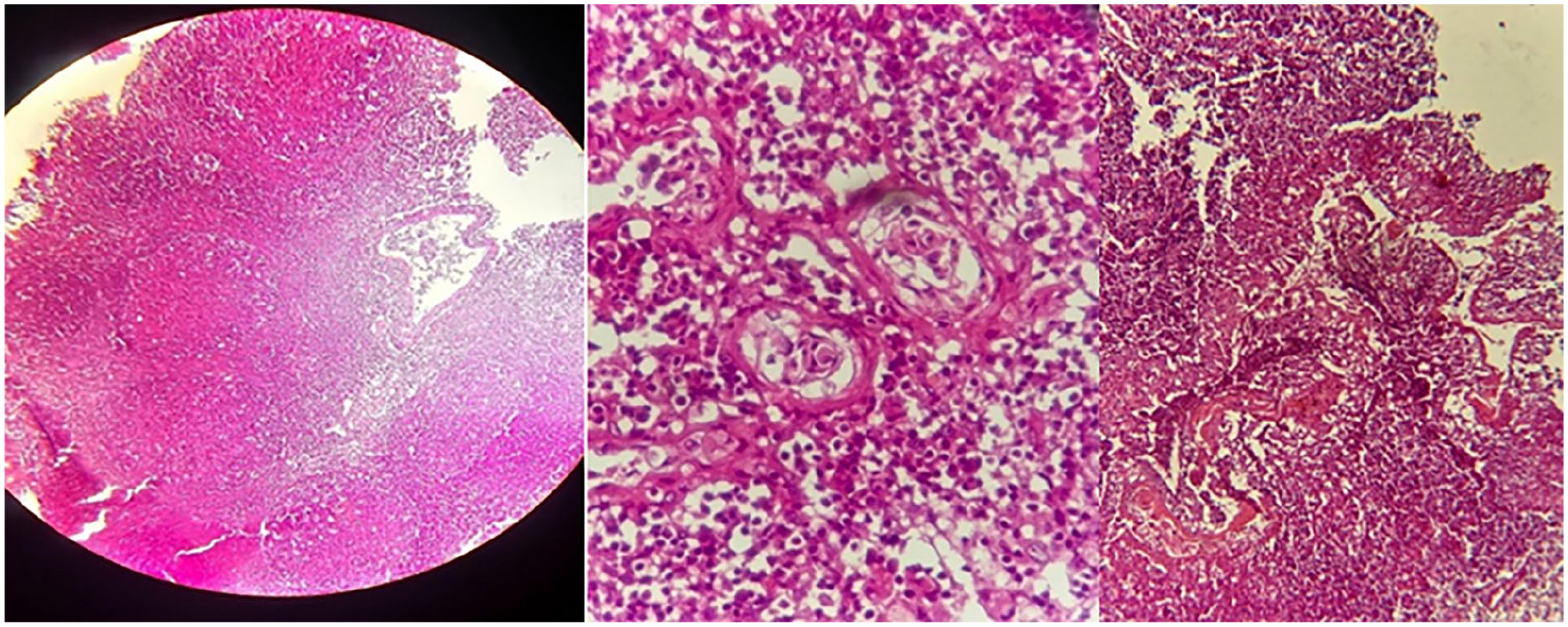
Histological examination showing hyperplasia in epithelial tissue, no signs of dysplasia, and some areas showed clear cells (a cell that appears pale or clear under a microscope, particularly when stained with hematoxylin and eosin), congestion in blood vessels with lymphocytes.
Discussion
This case report details the incidental discovery of a primary clear cell neoplasm arising within the adenoid tissue of a pediatric patient, a finding that, to our knowledge, has not been previously documented in the medical literature. Adenoidectomy is one of the most common surgical procedures in the pediatric population, typically performed for hypertrophy leading to obstructive symptoms or chronic inflammation. 2 The vast majority of adenoid specimens submitted for histopathological analysis demonstrate benign lymphoid hyperplasia, a reactive process reflecting the adenoid’s role as an immunological organ within Waldeyer’s ring. 1 While the nasopharynx can be the site for various tumors, including nasopharyngeal carcinoma, primary neoplasms originating from the adenoid stroma are exceedingly rare, making this case unique. 3 The unexpected nature of this finding highlights the fundamental importance of meticulous histopathological examination of all surgically excised tissues, regardless of how routine the procedure may be.
The morphological finding of a clear cell neoplasm necessitates a broad differential diagnosis. 4 In any location, but particularly in the head and neck, the primary consideration must be a metastasis from a distant primary site, with clear cell renal cell carcinoma (ccRCC) being the most common culprit. 6 Other considerations include clear cell variants of primary salivary gland tumors, such as mucoepidermoid carcinoma or acinic cell carcinoma, as well as the clear cell variant of calcifying epithelial odontogenic tumor. 4 However, the histomorphological features in our case were not consistent with these entities, instead pointing toward a low-grade adenomatous lesion. The architecture was most suggestive of the rare entity known as microcystic adenoma, which has been sparsely reported in the sinonasal tract.5,6 A critical aspect of sinonasal microcystic adenomas is their strong and consistent association with VHL disease.5,6 VHL is an autosomal dominant hereditary cancer syndrome that predisposes affected individuals to a spectrum of benign and malignant neoplasms, including central nervous system hemangioblastomas, ccRCC, pheochromocytomas, and a variety of cystic lesions, particularly in the pancreas. 7 The discovery of a tumor type so closely linked to VHL, such as a microcystic adenoma, in a new anatomical location within the nasopharynx raises the immediate and crucial question of a potential underlying VHL diagnosis in our patient. 6 The pathology of pancreatic cystic disease in VHL patients has been well-characterized, often showing multiple cysts and microcystic adenomas that are driven by the alteration of the VHL gene. 7 This potential association presented a clinical dilemma, as our patient had no personal or family history suggestive of VHL disease at the time of presentation. This situation allows for several possibilities: the neoplasm could be a sporadic, non-syndromic tumor that merely mimics a VHL-associated lesion; alternatively, it could represent the initial clinical manifestation (forme fruste) of VHL disease in this individual and his family. 5 Although the tumor was completely excised and appears to be of low-grade biology, its potential syndromic association carries significant implications for the patient’s long-term health management. Establishing a definitive diagnosis of VHL syndrome relies on identifying a germline mutation in the VHL gene or fulfilling established clinical criteria, which often involves the presence of multiple characteristic tumors. 6 Consequently, the clinical management of this patient cannot be limited to the simple excision of the adenoid lesion. A comprehensive and multidisciplinary approach is warranted, beginning with a thorough systemic evaluation to screen for other occult VHL-associated pathologies. 6 This should include ophthalmologic examination for retinal angiomas, magnetic resonance imaging of the brain and spine for hemangioblastomas, and abdominal imaging to assess the kidneys, adrenal glands, and pancreas. 7 Furthermore, genetic counseling and testing for a germline VHL mutation should be strongly considered to provide a definitive diagnosis, guide future surveillance protocols, and allow for cascade screening of family members. 5 Critically, the patient was not diagnosed with VHL syndrome. Despite histological similarities to VHL-associated tumors, no syndromic stigmata or family history existed. Post-diagnosis, the family declined further investigations (eg, center nerve system (CNS)/abdominal imaging) per clinical equipoise. Thus, VHL workup was deferred—aligning with guidelines that reserve invasive screening for cases meeting diagnostic criteria (eg, multiple tumors or familial patterns). 7 This underscores that histological mimicry alone cannot define syndromic status.
The primary limitation of this case report is the absence of VHL gene mutation analysis, which is the gold standard for confirming a diagnosis. 7 Nevertheless, this case is significant as it expands the known anatomical and pathological spectrum of VHL-associated neoplasms and introduces a novel entity into the differential diagnosis of nasopharyngeal lesions. It serves as a reminder for both clinicians and pathologists that even in the context of a common pediatric condition like adenoid hypertrophy, rare and clinically important pathological findings can be uncovered. 2 Awareness of this entity is crucial for ensuring that an incidental and seemingly innocuous finding leads to appropriate systemic evaluation and long-term surveillance for a potentially serious underlying condition.
Conclusion
This case presents the first documented instance of a primary clear cell microcystic adenoma arising within the adenoid tissue, expanding the histopathological spectrum of nasopharyngeal lesions. The incidental discovery underscores the critical role of meticulous histopathological evaluation, even in routine surgical specimens. While the lesion exhibited benign features, its morphological resemblance to VHL-associated tumors necessitates comprehensive systemic screening and genetic testing to exclude underlying syndromic disease. This finding highlights the importance of considering rare neoplasms in common clinical contexts and reinforces the need for multidisciplinary collaboration to guide patient management and familial surveillance. Further reporting of similar cases is warranted to validate this novel entity.
Footnotes
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases.
Consent for Publication
Written informed consent was obtained from the patient’s legal guardian for publication of this case report and accompanying images.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the author or corresponding author upon reasonable request.