
Abstract
Penetrating foreign bodies in the pediatric sphenoid sinus are exceptionally rare and pose significant diagnostic and surgical challenges due to the sinus’s proximity to critical neurovascular structures. We present the case of an 11 year-old boy who sustained a penetrating injury from a 7 mm bullet that entered through the floor of the frontal sinus, traversed the ethmoid sinus, and lodged in the right sphenoid sinus near the carotid canal and optic nerve. Initial assessment revealed hemodynamic stability and no active bleeding or neurological deficits. Non-contrast computed tomography precisely localized the metallic foreign body and confirmed an intact surrounding neurovascular architecture, with no intracranial injury. A multidisciplinary team opted for functional endoscopic sinus surgery to minimize risks to adjacent structures. The bullet was successfully extracted under endoscopic guidance without any complications. Postoperative recovery was uneventful, with no evidence of infection, nor cerebrospinal fluid leak, nor neurological sequelae. This case underscores the pivotal role of advanced imaging in guiding surgical planning and the efficacy of minimally-invasive endoscopic techniques in pediatric sinonasal trauma. The absence of intraoperative complications highlights the importance of interdisciplinary collaboration, anatomical knowledge, and early intervention to mitigate risks of infection or increasing surrounding fibrosis. delayed neurovascular injury might be avoided. While isolated pediatric sphenoid sinus foreign bodies remain rare, this report reinforces the value of tailored imaging protocols, endoscopic proficiency, and collaborative care in optimizing outcomes. Future studies should focus on standardizing management strategies and exploring emerging technologies to enhance precision in this anatomically-complex population.
Introduction
Penetrating injuries to the paranasal sinuses involving foreign bodies are rare in pediatric populations, particularly those traversing the ethmoid sinus to lodge within the sphenoid sinus. The sphenoid sinus’s anatomical complexity—proximity to the optic nerve, internal carotid artery, and cavernous sinus—poses significant diagnostic and surgical challenges.1,2 Isolated sphenoid sinus foreign bodies in children are exceptionally uncommon, with most reported cases involving adults or atypical trajectories.3-5 The nonspecific symptomatology, such as nasal bleeding or headache, often delays diagnosis, necessitating advanced imaging for precise localization. Computed tomography (CT) remains pivotal for evaluating such injuries, while endoscopic approaches, such as functional endoscopic sinus surgery (FESS), offer minimally-invasive solutions to mitigate risks to adjacent neurovascular structures.6,7 This case underscores the importance of interdisciplinary collaboration and tailored imaging in managing rare pediatric sphenoid sinus injuries, emphasizing the unique challenges posed by the child’s developing anatomy and the critical need for timely intervention to prevent catastrophic complications. Written informed consent was obtained from the patient’s family.
Case Presentation
An 11 year-old boy was sleeping in a supine position in an open-roofed house when a 7 mm bullet fell freely along its trajectory and penetrated the floor of the frontal sinus. The bullet traversed the ethmoid sinus and lodged in the right sphenoid sinus without penetrating the skull base. The incident occurred without any witnesses, and the patient was discovered shortly afterward by family members. On the initial presentation, he was hemodynamically stable with no signs of respiratory distress or active bleeding from the nasal cavity. There were no reports of meningitis, cerebrospinal fluid leak, loss of smell, headache, or prior surgical history, suggesting the injury was relatively contained at the time of assessment. A non-contrast CT scan of the head and paranasal sinuses was promptly performed to evaluate the extent of the injury. The imaging revealed a metallic foreign body, identified as the bullet, situated within the right sphenoid sinus, and positioned near the carotid canal and optic nerve. Notably, the surrounding cerebral tissue appeared intact, with no evidence of hemorrhage, edema, or structural damage to adjacent anatomical landmarks such as the skull base or orbital walls (Figure 1). The bullet’s trajectory through the ethmoid sinus was clearly delineated, confirming its path from the floor of the frontal sinus to its final resting place in the sphenoid sinus. The absence of additional abnormalities on the CT scan supported the clinical findings of a stable neurological status and lack of immediate complications. Following the imaging results, a multidisciplinary consultation involving otolaryngology and neurosurgery specialists was undertaken to determine the optimal management strategy. Given the bullet’s location and the potential risks of leaving it in situ—such as infection or delayed injury to nearby critical structures—the decision was made to proceed with surgical intervention. FESS was selected as the approach due to its minimally-invasive nature and proven efficacy in accessing the paranasal sinuses. The procedure was carried out under general anesthesia, with intraoperative endoscopic guidance allowing precise visualization of the foreign body within the sphenoid sinus. Transnasal transsphenoidal approach involving resection of the inferior third of the superior turbinate, followed by enlargement of the natural sphenoid sinus ostium in the lateral and superior directions to achieve full exposure of the foreign body using a curved spatula (Figure 2). The bullet was successfully extracted, and a thorough inspection of the sinus cavity confirmed no residual fragments or damage to surrounding tissues. The surgery concluded without complications, and the patient was transferred to the recovery unit for monitoring. Postoperatively, the patient exhibited an uneventful recovery course. He remained free of infection, neurological deficits, or signs of cerebrospinal fluid leakage during the hospital stay. The boy was discharged with instructions for outpatient follow-up and has since shown no adverse effects related to the incident or the surgical intervention.
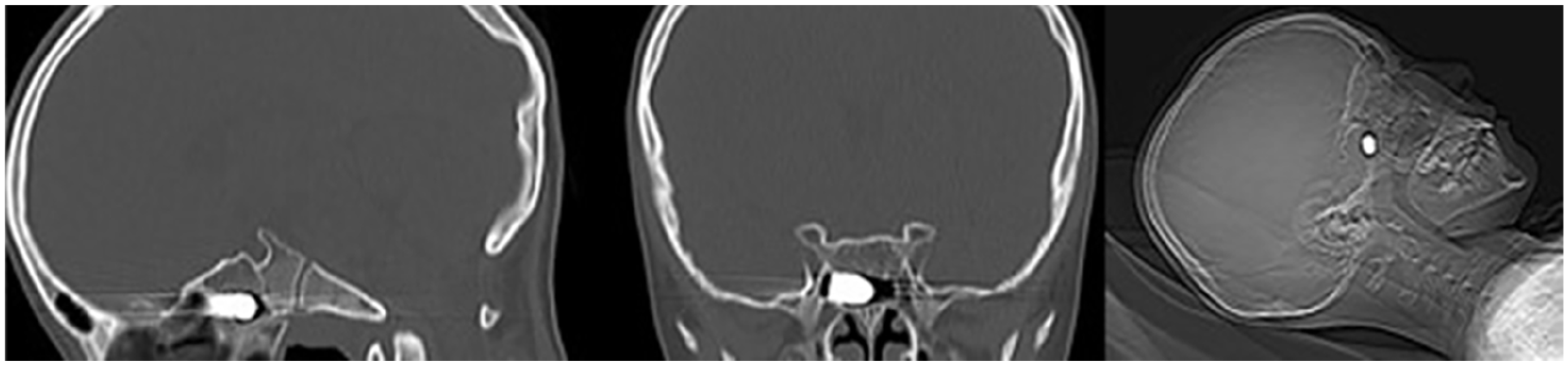
Non-contrast CT scans reveal a foreign body within the right sphenoid sinus, located near the carotid canal and optic nerve. CT, computed tomography.
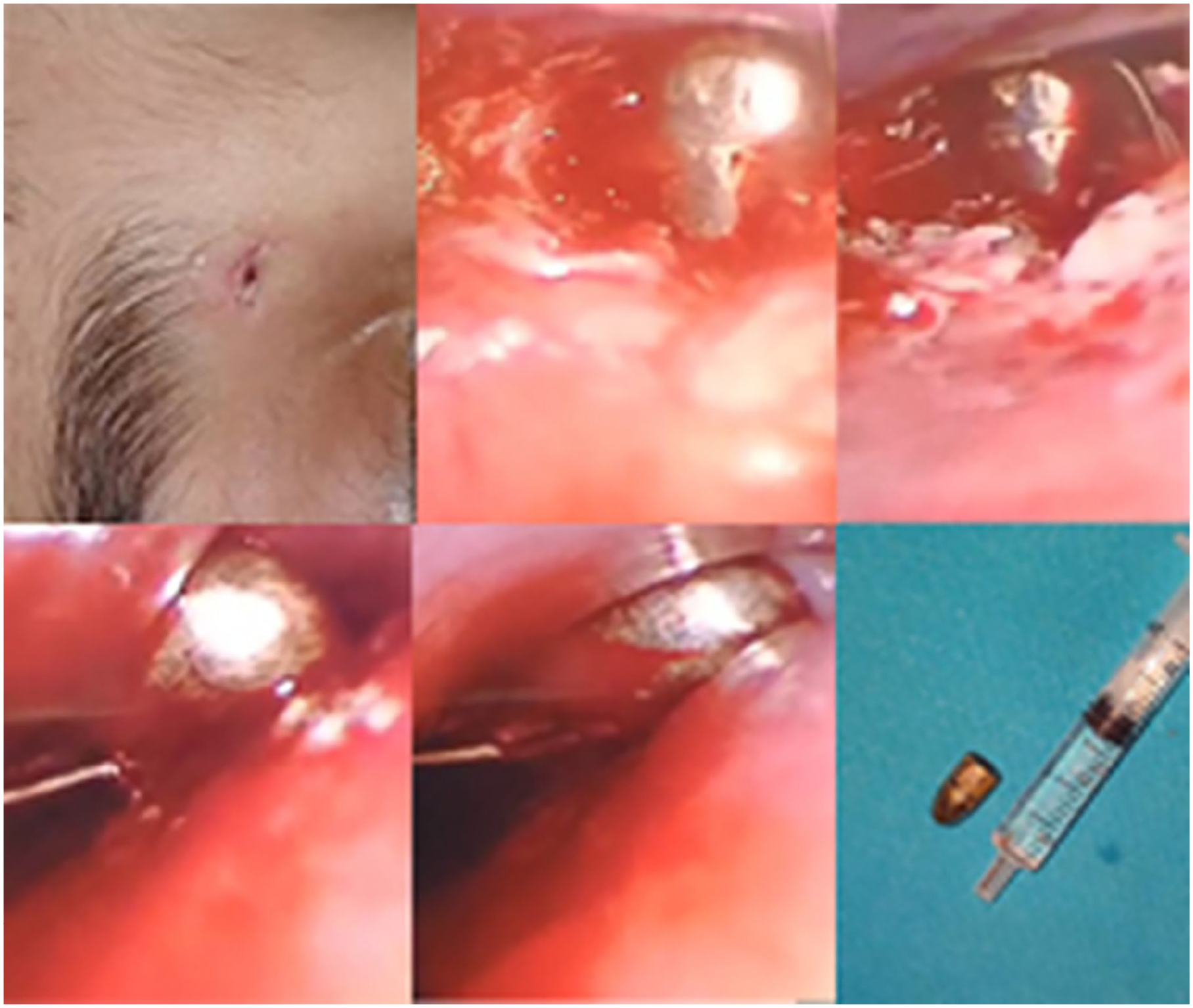
Extraction of the bullet during functional endoscopic sinus surgery.
Discussion
The management of pediatric sphenoid sinus foreign bodies presents unique challenges due to the sinus’s anatomical complexity, proximity to critical neurovascular structures, and the rarity of such injuries in children. This case highlights the importance of a systematic approach combining advanced imaging, interdisciplinary collaboration, and minimally-invasive surgical techniques to optimize outcomes while mitigating risks.
The sphenoid sinus’s intimate relationship with the optic nerve, internal carotid artery, and cavernous sinus underscores the potential for catastrophic complications if foreign bodies remain undetected or untreated. 2 In this case, the bullet’s trajectory through the ethmoid sinus into the sphenoid sinus, near the carotid canal and optic nerve, necessitated urgent evaluation. While headaches and nasal symptoms are common in sphenoid pathology, their nonspecific nature often delays diagnosis, particularly in children. 6 Unlike adults, pediatric patients may lack the verbal capacity to articulate symptoms clearly, emphasizing the role of imaging. Non-contrast CT, as performed here, remains the gold standard for delineating bony anatomy and foreign body localization.3,6 The absence of intracranial injury on imaging was reassuring, though MRI could have further assessed soft tissue involvement if complications were suspected. 6
The choice of FESS aligns with modern paradigms favoring minimally-invasive approaches. The endoscopic transostial route allows direct access to the sphenoid sinus while preserving surrounding structures. 1 This approach minimizes morbidity compared with traditional open techniques, which carry higher risks of cerebrospinal fluid leakage, orbital injury, or vascular damage. 2 Intraoperative navigation systems, though not used here, could enhance precision in complex cases. 6 Notably, the absence of intraoperative complications—such as hemorrhage or optic nerve injury—reflects the safety of FESS when performed by skilled surgeons familiar with sphenoid anatomy.1,2
Isolated sphenoid sinus foreign bodies in children are exceptionally rare, with most literature focusing on adults.3,5 The developing anatomy of pediatric sinuses, including narrower nasal cavities and incomplete pneumatization, complicates surgical access. 6 In this case, the bullet’s path through the ethmoid sinus without ethmoidectomy underscores the role of preoperative CT in mapping the trajectory and avoiding unnecessary dissection. Furthermore, the child’s stable neurological status postoperatively highlights the efficacy of early intervention in preventing delayed complications, such as infection or migration-induced neurovascular injuries.4,7 This case mirrors findings from prior reports of transnasal foreign bodies, where endoscopic removal proved successful despite proximity to critical structures.7,8 For instance, Dimitriou et al 9 emphasized the role of CT in identifying foreign bodies and planning surgical routes, while Akhaddar et al 3 highlighted the importance of angiography in ruling out vascular injury. Unlike cases involving organic materials (eg, wood or bamboo), metallic foreign bodies are radiographically conspicuous, reducing diagnostic uncertainty. 8 However, the potential for delayed complications, such as mucosal scarring or sinusitis, necessitates a long-term follow-up. 6
The involvement of otolaryngology and neurosurgery teams ensured comprehensive preoperative planning and risk stratification. This collaborative model is critical in pediatric cases, where anatomical variations and growth considerations demand tailored approaches. 6 Postoperative monitoring for cerebrospinal fluid leakage, infection, or neurological deficits—though unnecessary here—remains a cornerstone of care. 2
While this case had a favorable outcome. Future studies could explore the role of intraoperative imaging or augmented reality systems in pediatric FESS. Additionally, standardized protocols for managing pediatric sinonasal trauma are needed, given the scarcity of literature. It reinforces the importance of anatomical knowledge, preoperative planning, and endoscopic proficiency in mitigating risks associated with this complex region. As FESS continues to evolve, its application in pediatric populations will likely expand, provided surgeons remain vigilant to the unique challenges posed by developing anatomy and nonspecific symptomatology.
Conclusion
This case illustrates the rarity and complexity of pediatric paranasal sinus foreign body injuries. The successful management of this case highlights the critical role of non-contrast CT imaging in delineating the foreign body’s location and trajectory, enabling precise surgical planning. FESS proved to be an effective and safe approach for extracting the bullet, minimizing risks to adjacent neurovascular structures such as the optic nerve and internal carotid artery. The absence of intraoperative or postoperative complications underscores the importance of endoscopic proficiency and a thorough understanding of pediatric sinonasal anatomy. Furthermore, the collaborative efforts of otolaryngology and neurosurgery teams were instrumental in ensuring a tailored and comprehensive treatment strategy. This case reinforces the need for prompt diagnosis, meticulous preoperative evaluation, and minimally-invasive techniques in managing such rare injuries in children. Future research should focus on developing standardized protocols for pediatric sinonasal trauma and exploring advanced intraoperative technologies to further enhance surgical precision and outcomes in this challenging anatomical region.
Footnotes
Ethical Considerations
Our institution does not require ethics approval for reporting individual cases.
Consent for Publication
Written informed consent was obtained from the patient’s family for the publication of this article.
Author Contributions
All authors contributed to the conception of the study. All authors read and approved the final manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the author or corresponding author upon reasonable request.