
Abstract
Objective:
To investigate the demographic determinants of patient perception toward the role of artificial intelligence (AI) in otolaryngology—head and neck surgery care.
Methods:
Outpatients consulting in otolaryngology—head and neck surgery departments of 18 hospitals were surveyed about the perception of the role of AI in health care. The results were analyzed according to the age, gender, patient use of technology, and the level of education.
Results:
The survey was completed by 1545 patients from Europe and the United States (participation rate: 98.7%). There were 832 (53.9%) females and 669 (43.3%) males. The level of education significantly influences the perception of AI in otolaryngological care with the lowest trust and agreement in patients with the highest education level. The study demonstrated a higher mean overall agreement score for using AI in medicine among daily users of technologies than among others (7.2 ± 1.9 vs 5.6 ± 2.6; P = .001). Females reported more frequent fears about the use of AI in otolaryngology than males. The agreement scores for using AI in medicine significantly decreased with age (P = .001).
Conclusion:
The perception of AI use in otolaryngology was influenced by age, gender, level of education, and the use of new technologies in daily life. Further studies promoting the use of AI in Western populations can consider demographics for improving the perception of patients toward AI, and an AI literacy component to determine whether lower trust is due to misunderstanding AI capabilities.
Significance Statement
The perception of artificial intelligence (AI) is influenced by the level of education with the lowest trust and agreement in patients with the highest education level.
The study reports a higher mean overall agreement score for using AI in medicine among daily users of technologies than among others.
Females reported more frequent fears about the use of AI in otolaryngology than males.
The agreement scores for using AI in medicine significantly decreased with age.
Introduction
Artificial intelligence (AI) is increasingly playing a significant role in clinical practice and research. 1 AI software can help practitioners to prepare the consultation through the collection of medical information, 2 in diagnosis,3,4 and in the choice of therapeutic options. 5 Thus, AI software may improve practitioners’ skills in managing outpatients. In the same vein, the development of AI in surgery can improve the preoperative analyses of imaging, 6 the choice of the surgical approach, 7 and the postoperative follow-up of patients. 8 The increasing development of AI applications in otolaryngology—head and neck surgery is progressively changing our practice for the future decades. To date, while some surveys evaluated the perception of AI in other specialties, there are no general studies assessing the patient perception of the potential role of AI in otolaryngology head and neck surgery. Identifying patient opinions, fears, and perceptions of AI, and potentially comparing them with patients consulting in other specialties, can be important due to the increased use of AI applications in consultation or surgery and the potential impact on the quality of the relationship between the practitioners and patients.
This cross-sectional international study investigated the demographic determinants of the patient perception toward the role of AI in otolaryngology head and neck surgery care.
Materials and Methods
An international survey was developed by 3 otolaryngologists to survey patient opinion regarding the role of AI in medical and surgical care in otolaryngology—head and neck surgery.
The study was conducted by the AI-Research Group of the Young Otolaryngologists of the International Federation of Otorhinolaryngological Societies (Paris, France). The survey included 4 demographic questions (age, gender, level of education, and job), 1 question related to the daily life use of technology, and 15 general questions investigating the level of trust in the current health applications (N = 1), adaptation skills to new technologies/devices (N = 1), opinion and trust regarding the usefulness/benefits of AI in the management of health care (N = 8), the fear about the use of AI (N = 3), the potential benefits of using AI in clinical research (N = 1). General questions were rated with 5-point Likert scale ranging from totally disagree to totally agree (Supplemental Appendix 1). The last question was related to the overall opinion of patients regarding AI in health care and was rated with a 11-point Likert scale ranging from 0 (very low opinion) to 10 (excellent opinion). The survey was developed in English. Of the English version, French, Spanish, and Italian versions were translated by native speakers of these respective countries.
Given the lack of study evaluating general perception of AI in otolaryngology, this study was primarily designed to evaluate the perception of patients consulting ear, nose, and throat departments, while the survey did not include specific perception outcomes related to AI devices and technologies used in otolaryngology.
The Institutional Review Board of CHU Saint-Pierre agreed with the content of the study (CHUST250705). The patient consented to participate.
Survey Distribution and Data Collection
The survey was distributed to patients in paper form in the waiting room (before the consultation), and the data were encoded into an Excel sheet. Each participant could complete the survey only once. The survey participation was proposed to consecutive patients consulting in the otolaryngology—head and neck surgery departments of 8 Spanish, 6 Italian, 2 Belgian, 1 French, and 1 American hospital(s). There was no restriction regarding the type of disorder or the division where patients consulted. The following Spanish hospitals were included: Hospital Universitario Donostia (San Sebastian University, San Sebastian); the Virgen Macarena University Hospital (Seville University, Seville); Hospital Público da Mariña (Lugo); the Complexo Hospitalario Universitario de A. Coruña (Universidade da Coruña, La Coruna); the Hospital San Rafael (La Coruna); the Hospital Obispo Polanco (Teruel); the Fundación Jiménez Díaz University Hospital (Madrid); and Villalba General University Hospital (Madrid). Italian hospitals included the University Hospital of Naples (University of Naples SUN, Naples); University Hospital of Milan (Università Degli Studi Di Milano, Milan); University Hospital of Sassari (University of Sassari, Sassari); Enna Kore Hospital (University of Enna Kore, Catania); University hospital of Rome (University “Sapienza,” Rome); and the Forli University Hospital (Forli). Belgian, French, and American hospitals were the EpiCURA Hospital (Baudour); the University Hospital Saint-Pierre (Brussels); La Conception University Hospital (Aix Marseille University); and the Massachusetts Eye and Ear Infirmary (Boston, Harvard University).
Statistical Analyses
Statistical analyses were performed with the Statistical Package for the Social Sciences for Windows (SPSS version 30.0; IBM Corp, Armonk, NY, USA). The responses were analyzed considering the level of education (high school, college/bachelor, graduate study/master, MD/PhD), the use of technologies in daily life (daily, more than 3 times weekly, <3 times a week, sometimes, never), and age groups. The differences in response between groups were evaluated using a Kruskal-Wallis test or χ2 test according to data. For the 11-Likert scale differences between groups, the Kruskal-Wallis and Mann-Whitney U tests were used to compare the group’s results. A P < .05 was considered as significant.
Results
Setting and Demographics
The survey was completed by 1545 patients from Spain (N = 746), Italy (N = 653), Belgium (N = 112), and the United States (N = 34). Twenty patients (1.3%) did not fully complete the survey. Demographics are described in Table 1. The mean age was 47.1 ± 16.2 years. The age groups included 117 to 306 participants (Table 1). There were 832 (53.9%) females and 669 (43.3%) males. The level of education of participants included high school (26.9%), college/bachelor (15.9%), graduate study/master (38.6%), and doctorate (17.6%) (Table 1). General attitudes toward AI are reported in Table 2. The agreement and confidence of patients toward AI’s use in otolaryngology was moderate to high. The mean overall agreement scores for using AI in medicine and surgery was 7.1 ± 2.0.
Patient Features.
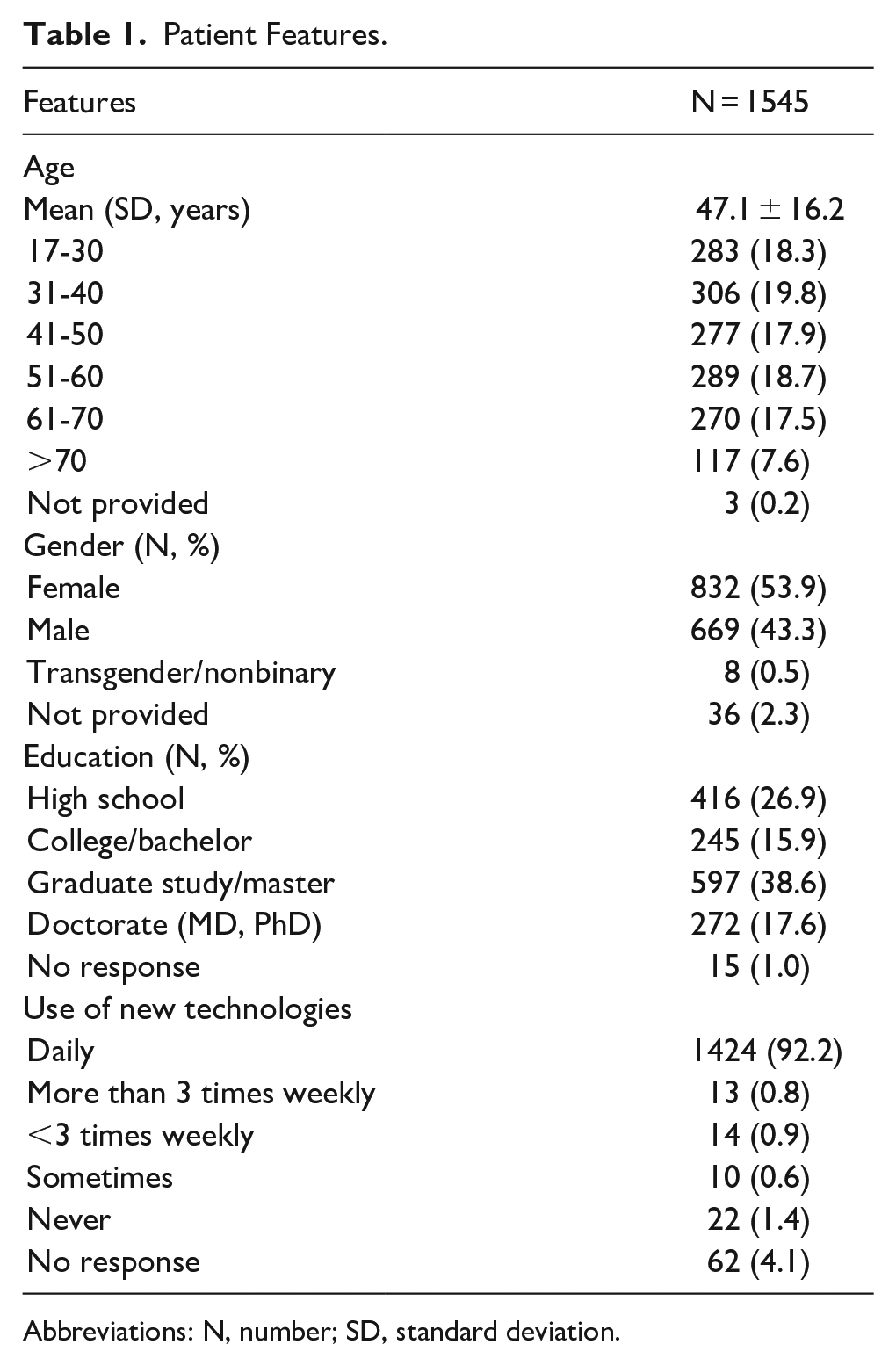
Abbreviations: N, number; SD, standard deviation.
General Attitudes Toward AI.
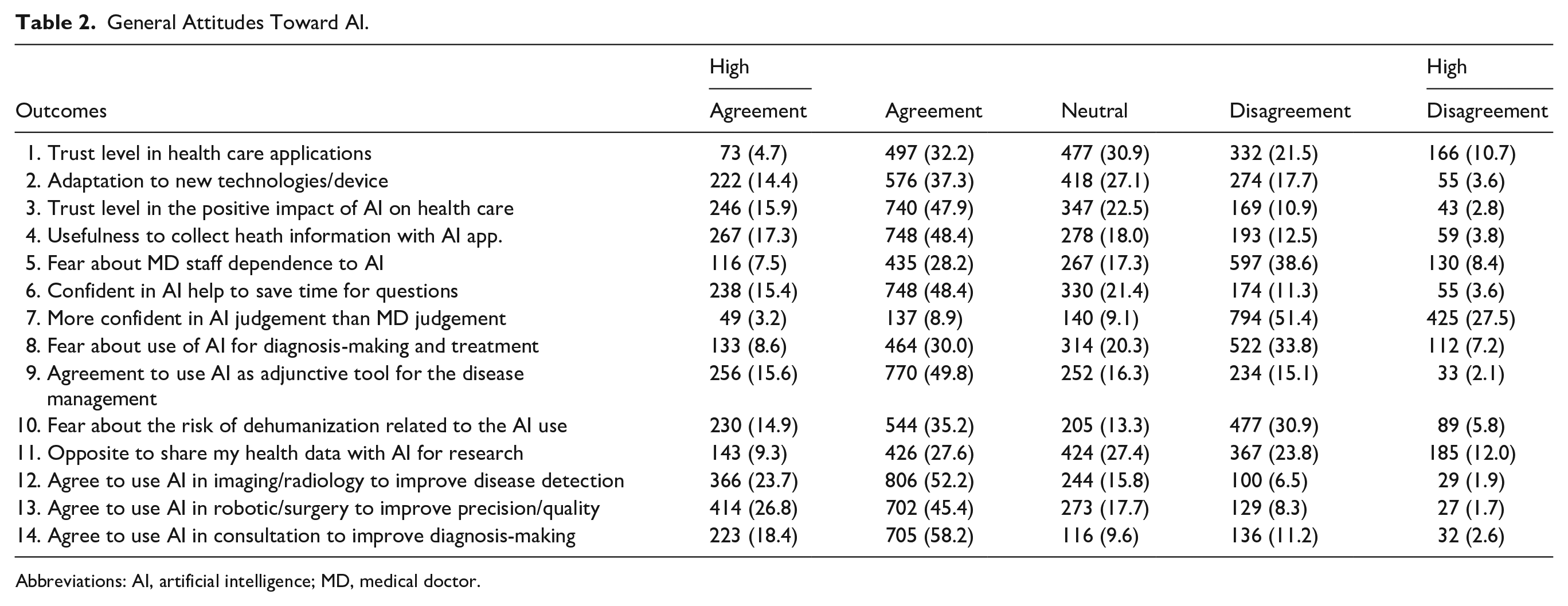
Abbreviations: AI, artificial intelligence; MD, medical doctor.
Influence of the Level of Education
The influence of the level of education is reported in Table 3. Patients with the lowest level of education reported significantly higher agreement proportions in the following outcomes: overall trust in health care applications; potential impact of AI on health care; and the usefulness of collecting health information with an AI app for the management of care compared to patients with the highest education level (Table 3). Regarding fears, individuals in the high school group recognized having a higher level of fears than the doctorate group for the following outcomes: physician’s dependence on AI in care management; use of AI for diagnosis-making and treatments; and the risk of dehumanization. Confidence in “AI judgment versus physician judgment and AI help to save time in consultation” was similarly higher in groups with the lowest levels of education than the group with the highest levels of education (Table 3). Most patients with a high school, bachelor’s, or master’s degree agreed on the use of AI as an adjunctive tool for diagnosis, while the analysis suggested the opposite for doctorate patients. The patient opinion regarding the sharing of health data with AI software for research was more contrasted (agreement vs disagreement) in the level of education groups (Table 3). The agreements of patients to use AI in imaging and robotic surgery were significantly higher in high school, bachelor’s, or master’s degree groups than in the doctorate group (Table 3). However, the overall level of approval for the use of AI in medicine and surgery significantly increased from the high school to the doctorate groups.
Influence of the Level of Education on AI Perception.
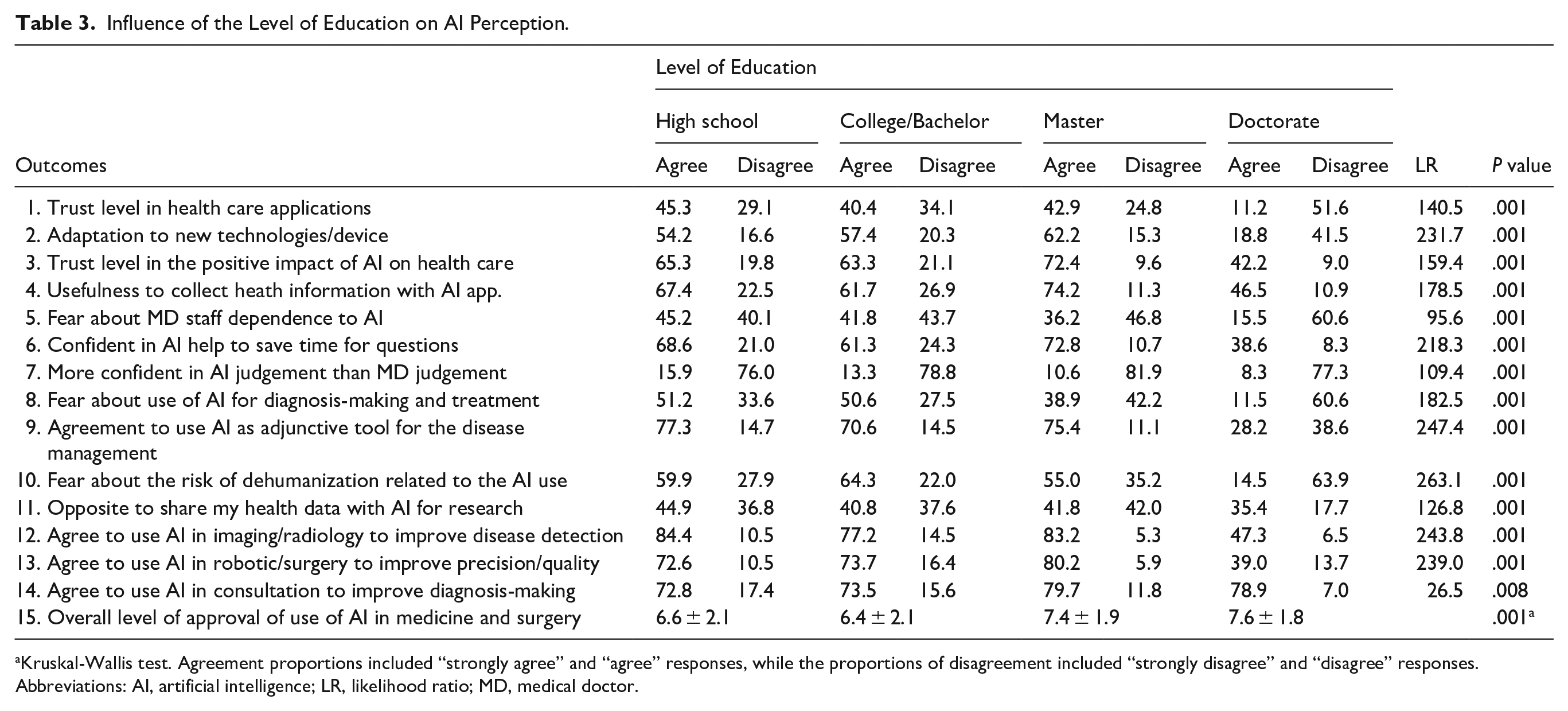
Kruskal-Wallis test. Agreement proportions included “strongly agree” and “agree” responses, while the proportions of disagreement included “strongly disagree” and “disagree” responses.
Abbreviations: AI, artificial intelligence; LR, likelihood ratio; MD, medical doctor.
Among the group of patients with a doctorate, a sub-analysis was carried out to compare physicians and non-physician doctors (Table 4). Thirteen patients were excluded because they did not mention the field of their doctorate (MD or PhD/others). Among the 259 participants were 135 physicians (52.1%) and 124 non-physician doctors (47.9%). Physicians reported higher trust levels in health applications, a positive impact of AI on health care, and better adaptation than non-physician doctors (Table 5). However, the level of fear regarding the dependence on AI, the risk of dehumanization, and the use of AI in diagnosis-making and treatment were significantly higher in physicians than in non-physician doctors (Table 4). Physicians agreed to consider using AI as an adjunctive tool in clinics more frequently than non-physician doctors. The mean overall agreement scores for using AI in medicine were similar in physicians (7.6 ± 1.5) and non-physician doctors (7.7 ± 1.8; P = .203).
Differences Between Physicians and Non-Physician Doctors Regarding AI.
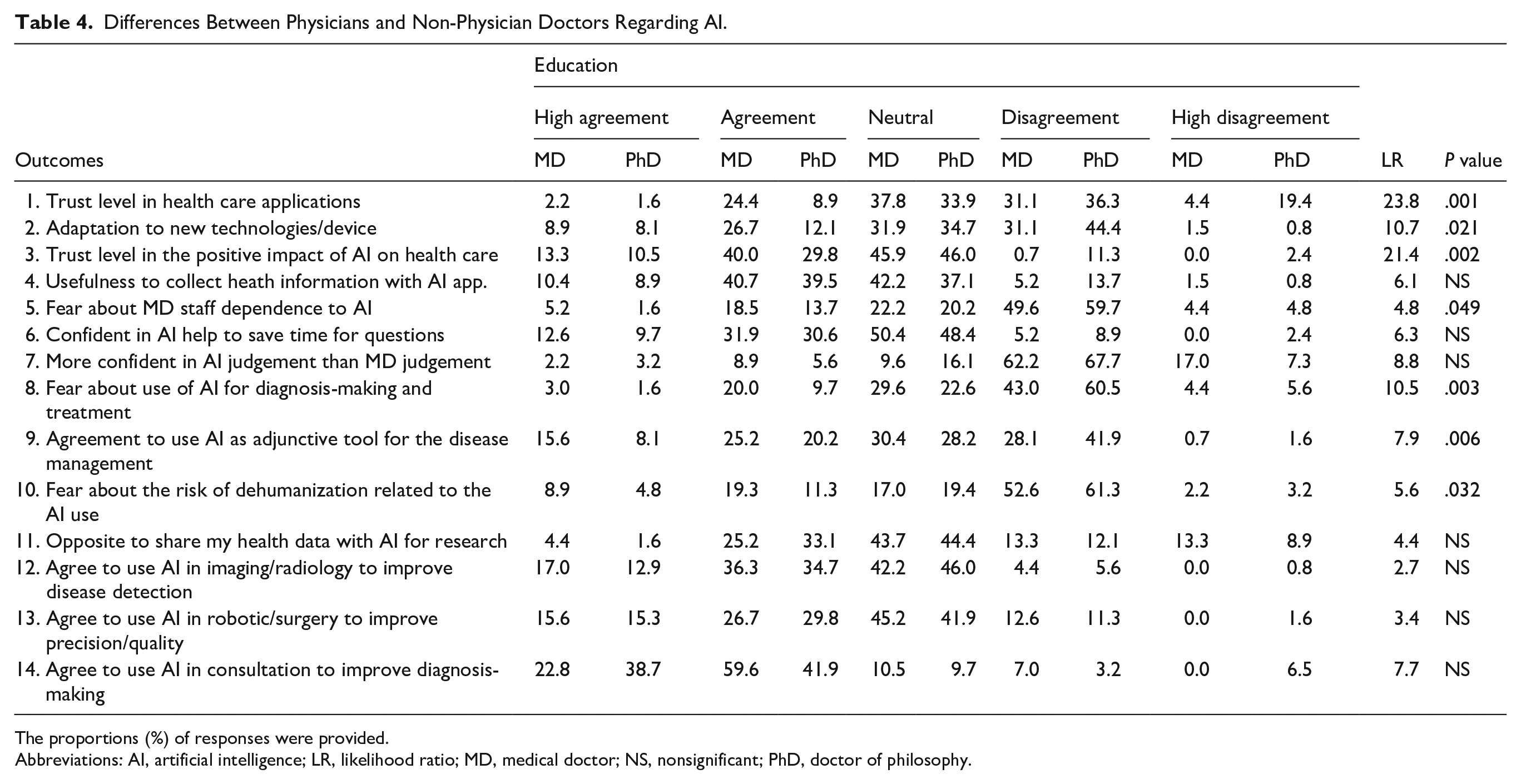
The proportions (%) of responses were provided.
Abbreviations: AI, artificial intelligence; LR, likelihood ratio; MD, medical doctor; NS, nonsignificant; PhD, doctor of philosophy.
Influence of the Use of New Technologies on the AI Perception.
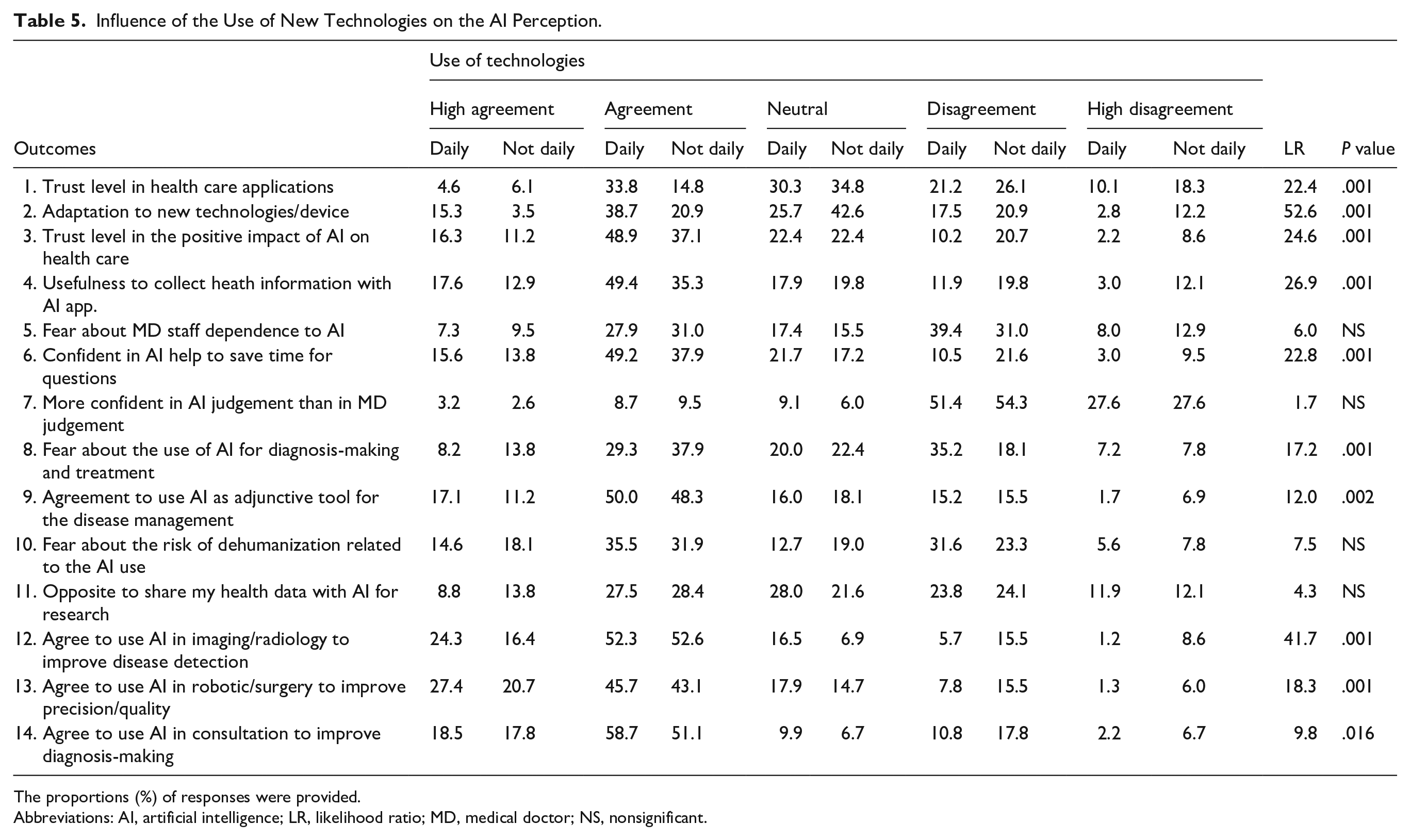
The proportions (%) of responses were provided.
Abbreviations: AI, artificial intelligence; LR, likelihood ratio; MD, medical doctor; NS, nonsignificant.
Influence of the Use of Technologies
The use of technologies in daily life was detailed by 1483 patients. Given the low number of patients using new technologies and devices <1 time in a day, the analysis was performed considering 2 groups: patients using technologies daily versus those who did not. The use of new technologies/devices in daily life was associated with overall higher trust and less fear of using AI in clinical practice (Table 5). The mean overall agreement scores for using AI in medicine and surgery were significantly higher in daily users of new technologies than in others (7.2 ± 1.9 vs 5.6 ± 2.6; P = .001)
Influence of Gender
Given the low proportion of nonbinary or transsexual individuals, the analyses were carried out considering only females and males. The opinions of males were more contrasted than of females. Females responded more frequently “agree” or “disagree” in the following outcomes: trust level in health care applications; adaptation to new technologies; and fear about MD staff dependence on AI. The proportion of females who reported fears about using AI for diagnosis-making and treatment was significantly higher than that of males (41.3% vs 35.2%; Figure 1). A similar observation was found for the fear of the risk of dehumanization. Females more commonly expressed than males (53.5% vs 46.0%). The proportion of males agreeing to use AI in consultation with improving diagnosis-making was higher than that of females (Figure 1; Supplemental Appendix 2). The mean overall agreement scores for using AI in medicine for females (6.9 ± 2.1) was lower than the mean score of males (7.3 ± 1.9; P = .001).
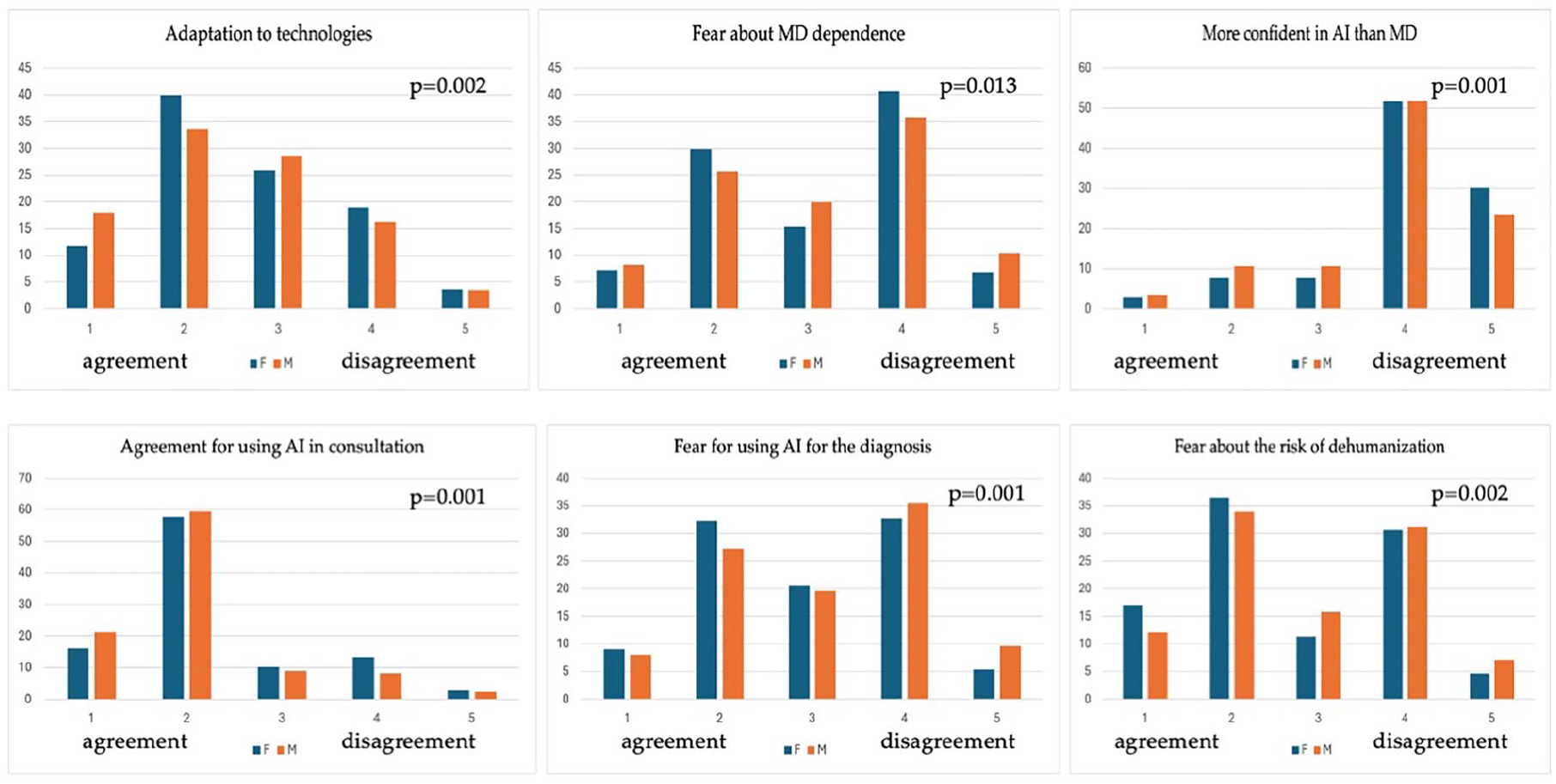
Gender influence on artificial intelligence perception. Chi-squared was used to compare the proportions of agreement outcomes between males and females.
Influence of Age
The potential influence of age on AI perception was reported in Supplemental Appendix 3. Note that the proportion of daily use versus >3 times/week use of new technologies progressively increased from the oldest to youngest age groups (P = .001). Participants aged 31 to 60 years self-reported higher levels of adaptation to new devices and technologies than older participants (Supplemental Appendix 3). The youngest participants more frequently disagreed with the idea of collecting health information with an AI app than older patients. Moreover, they were less confident in the usefulness of AI to save time in consultation. The fears related to the use of AI for diagnosis-making and associated with the risk of dehumanization were more frequently shared by older patients than by the youngest group. The agreement for using AI as an adjunctive tool for disease management in imaging, surgery, or consultations significantly increased with the participants’ age (Supplemental Appendix 3). Participants aged over 60 years were more commonly opposed to sharing their health data with AI for research than younger participants. The mean overall agreement scores for using AI in medicine and surgery significantly decreased with age (P = .001).
Discussion
The development of AI in medicine and surgery can progressively change the approach to managing diseases. To date, AI is already used in imaging and in the follow-up of chronic disease,6,9 while some software has been developed for otolaryngological consultation.10,11 The success of managing a disease depends on the patient’s adherence to the proposition of care. To the best of our knowledge, the present study is the first to investigate general perception, fears, and awareness of patients’ perceptions, fears, and awareness toward AI in otolaryngology consultations.
The overall patient’s perception of the use of AI in otolaryngology care is moderate to high and the use of technologies, age, and the level of education primarily influences it. Similar studies have been conducted in primary care patients,12,13 dermatology, 14 radiology, 15 endocrinology, 16 or in the physician populations, 17 sharing some similarities and differences with the results of the present survey. Note that the number of AI perception survey remains commonly low in medicine and surgery.
Sarwar et al surveyed 487 physicians from the United States, UK, and Canada. 17 Authors reported that nearly 75% of participants carried generally positive attitudes toward AI with interest or excitement in AI as a diagnostic tool to facilitate improvements in workflow efficiency and quality assurance in pathology. In our study, 53.3% of physicians reported positive outcomes for using AI in health care or as a diagnostic tool (imaging), while 82.4% were enthusiastic about using AI in consultation. This observation corroborates the data of Sarwar et al. 17 Interestingly, the authors investigated the influence of gender on the perception of AI. As observed in the present study, they observed that males reported higher levels of agreement to adopt AI in the practice and were more optimistic than females. 17 The lower level of confidence of females than of males was similarly observed by York et al who surveyed the opinion of 218 patients toward the use of AI in radiology. 15 Fritsch et al interrogated 452 patients in German hospitals and observed that 53.18% of the respondents rated using AI in medicine as positive or very positive, 13 which is close to the agreement rates observed in our study. Fritsch et al observed that older age and female gender outcomes were associated with lower proportions of positive opinions, corroborating our observation. However, the authors reported that a high level of education was associated with a good opinion toward AI’s use in health care. 13 The association between high level of education and the positive perception of AI was similarly observed by York et al, 15 these 2 studies reported conflicting observations with our results because 84.4% and only 47.3% of high school and doctorate graduated patients agreed to use AI in imaging, respectively. The differences between our study and those of the literature can be attributed to the determination of the various levels of education. In our study, we considered master’s and doctorate as different groups, which differs from other studies. 15 Importantly, when we focused on high school to master subgroups, we observed that the patients with a master’s degree reported higher positive perceptions toward AI than those with a high school degree, which is close to the data available in the literature. Although these methodological points, the large mediatization of AI software and the related risk to replace human in some jobs, the fear about dehumanization or AI misdiagnosis, data privacy concerns, and the skepticism about automation in medicine can represent other factors underlying our controversial results with some previous publications. Concerning data privacy and AI use regulation concerns, entering patient information into commercial versions of AI software infringes Health Insurance Portability and Accountability Act rule and should be avoided. 1 As of January 24, 2024, the European Commission has proposed a legal framework through a positional statement paper to address the risks generated by specific uses of AI in health care, 13 which supports the need to strengthen efforts to regulate the use of AI, while emphasizing the importance of safe, transparent, and human-centered use of AI technologies. The current lack of largely accepted legal framework can contribute to the perception of high-educated responses.
Concerning age, York et al 15 and Fritsch et al 13 showed higher levels of trust in AI use in younger patients than in older ones, which partly corroborates our observation. The influence of the use of technologies on confidence in AI was investigated in the study of York et al. 15 Similar to our study, authors had a large majority of participants who daily used new technologies such as laptop computers or smartphones (76.4%). They reported a small positive correlation between the duration of smartphone use and confidence in AI-assisted interpretation in radiology. 17 Given the spread of new technologies worldwide, York’s and our findings can support that the patient’s perception of using AI in health care will continuously improve in the next few years.
The influence of age, gender, and technology affinity on AI perception was evaluated in a study of 452 patients consulting a German tertiary referral hospital. 13 Fritsch et al reported that older patients, women, and persons with lower education and technical affinity were more cautious on the health care–related AI usage. The gender, technical affinity, and age findings of this study corroborate our observation. Contrary to Fritsch et al, our analysis suggested that patients with the highest education level reported the lowest trust and agreement. Moreover, similarly to our patients, most surveyed patients (53.18%) rated the use of AI in medicine as positive or very positive. 13 However, due to significant differences across our survey contents and surveyed populations, the comparison remains limited. To the best of our knowledge, the present study is the first investigation of the perception of AI by outpatients consulting in otolaryngology—head and neck surgery departments, which limits our comparison with similar studies conducted in otolaryngology. Contrary to other AI-perception studies conducted in other specialties,18,19 we did not evaluate the potential impact of ear, nose, and throat disorders on the AI perception, which was not the primary aim of this survey. The profile of patients consulting otolaryngology office could influence the perception of AI, but this assumption requires future investigations focusing on intervention rather than on perception. This specific survey makes particularly sense regarding the several emerging AI applications specifically targeting otolaryngological conditions, including automated audiometry interpretation, AI-assisted endoscopy image analysis for early cancer detection, and voice analysis for neurological condition monitoring.20,21
The low responses from the United States and the lack of consideration of patients from other large countries (eg, Canada, France, or Germany) are additional weaknesses, limiting the statistical inference to these populations. Indeed, some findings related to the country of origin (eg, culture, health care access, education) can significantly influence the perception of AI and, consequently, limit the generalizability of the results. Future studies are needed to evaluate AI perception in other world regions, such as Asia, Africa, Oceania, and Latin America, considering the cultural and educational features.
Conclusion
The perception of AI of patients consulting in otolaryngology was influenced by age, gender, level of education, and the use of new technologies. The general perception of AI in otolaryngology patients is the first step before conducting further studies evaluating the perception of patients regarding specificity of otolaryngological AI devices and technologies. Further studies promoting the use of AI in otolaryngology settings can consider demographics for improving the adherence of patients to AI-based care and practice.
Supplemental Material
sj-docx-1-ear-10.1177_01455613251351774 – Supplemental material for Patient Perceptions of Artificial Intelligence in Otolaryngology—Head and Neck Surgery: An International Study
Supplemental material, sj-docx-1-ear-10.1177_01455613251351774 for Patient Perceptions of Artificial Intelligence in Otolaryngology—Head and Neck Surgery: An International Study by Miguel Mayo-Yáñez, Anais Rameau, Luigi A. Vaira, Manon Louvrier, Alvaro Sanchez Barrueco, Ignacio Alcalá-Rueda, Fernando García-Curdi, Lara Mejuto-Torreiro, Alejandro Klein-Rodríguez, Jesús Herranz-Larrañeta, Juan Maza-Solano, Alberto M. Saibene, Giorgia Pugliese, Giovanni Briganti, Carlos M. Chiesa-Estomba, Francois Simon, Stephane Hans, Robin Baudouin, Alexandra Rodriguez, Didier Dequanter, Sven Saussez, Thomas Radulesco, Justin Michel, Isabelle M. Gengler, Matthew R. Naunheim, Giovanni Cammaroto, Andrea De Vito, Giannicola Iannella, Valentin Favier, Florent Carsuzaa, Maria R. Barillari, Antonino Maniaci and Jerome R. Lechien in Ear, Nose & Throat Journal
Footnotes
Author Note
European Commission: A strategic vision to foster the development and use of lawful, safe, and trustworthy artificial intelligence systems in the European Commission 2024.
ORCID iDs
Ethical Considerations
The Institutional Review Board of CHU Saint-Pierre agreed with the content of the study (CHUST250705).
Consent to Participate
The informed consent was obtained for participants.
Author Contributions
Jerome R. Lechien: design, acquisition of data, drafting, final approval, and accountability for the work; final approval of the version to be published; agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. Giovanni Briganti and Antonino Maniaci: data analysis and interpretation, proofreading of the paper, and final approval of the version to be published; agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. Anais Rameau: result interpretation, proofreading of the paper, and final approval of the version to be published; agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. Luigi A. Vaira, Manon Louvrier, Alvaro Sanchez Barrueco, Ignacio Alcalá-Rueda, Fernando García-Curdi, Lara Mejuto-Torreiro, Alejandro Klein-Rodríguez, Jesús Herranz-Larrañeta, Juan Maza-Solano, Alberto M. Saibene, Giorgia Pugliese, Carlos M. Chiesa-Estomba, Francois Simon, Stephane Hans, Robin Baudouin, Alexandra Rodriguez, Didier Dequanter, Sven Saussez, Thomas Radulesco, Justin Michel, Isabelle M. Gengler, Matthew R. Naunheim, Andrea De Vito, Maria R. Barillari, Giovanni Cammaroto, Giannicola Iannella, Valentin Favier, and Florent Carsuzaa: acquisition of data, final approval, and accountability for the work; final approval of the version to be published; agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Jerome R. Lechien is Associate Editor of Eur Arch Otorhinolaryngol. He was not involved in the reviewing process of this paper.
Data Availability Statement
Data are available on request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.