
Abstract
Objectives:
This study aimed to explore the impact of early-nasal intervention on sinusitis caused by radiation therapy in patients with nasopharyngeal carcinoma (NPC), in order to prevent and reduce the occurrence of radiation-induced sinusitis.
Methods:
Patients with NPC who were scheduled for intensity-modulated radiation therapy were randomized into an experimental group (n = 40) and a control group (n = 40) with concealed allocation. While the control group received only compound menthol drops, the experimental group received nasal treatments (nasal saline irrigation, corticosteroid nasal spray, and compound menthol drops) during radiation therapy and for 6 months after therapy. Sinusitis-related scores (symptoms scores, nasal endoscopy scores, and MRI findings) and mucociliary transport rate (MTR, mm/min) were collected at different time points of radiation therapy.
Results:
Before radiation therapy, there were no statistically-significant differences between the 2 groups in terms of sinusitis-related scores, MTR and general conditions (P > .05). Both experimental and control groups showed statistically-significant differences in sinusitis-related scores between time points after radiation therapy (P < .01), sinusitis-related scores peaked at 6 months after radiation therapy, and there were also significant differences in the MTR between time points during radiation therapy (P < .01). Sinusitis-related scores differed significantly between the 2 groups after the completion of radiation therapy and at the 3rd, 6th, and 12th month after radiation therapy (P < .05). At the 3rd and 6th month after radiation therapy, there was a statistically-significant difference in the nasal MTR between the 2 groups (P < .05).
Conclusions:
The experimental group and the control group showed statistically-significant changes in sinusitis symptoms scores, endoscopic findings, and MRI findings at multiple important time points after radiation therapy. This type of intervention demonstrates significant clinical value and safety.
Keywords
Introduction
Nasopharyngeal carcinoma (NPC) is characterized by a different geographical distribution and is particularly prevalent in East Asia and Southeast Asia. 1 Numerous variables have been shown to be associated with an increased risk of NPC, including heredity, age, sex, smoking, drinking alcohol, eating salted seafood, and positivity for the Epstein-Barr virus (EBV). Due to its unique biological activity, structural characteristics, and radiation sensitivity, radiation therapy has become the preferred treatment for NPC. A significant advancement in the treatment of NPC in recent years has been intensity-modulated radiation therapy (IMRT). IMRT has become the primary radiation technique for NPC because it improves the dose differential between the target and dose-limiting tissues, resulting in high tumor coverage and normal organ sparing than standard 2-dimensional radiotherapy (2DRT).1,2 Most patients with NPC have lymph node metastases or a wide local region at the time of diagnosis, and the nasopharynx is concealed. Radiation therapy has a vast irradiation area, a long course of illness, and a substantial total dose of radiation, even if IMRT is used. Complications, including radiation-induced sinusitis, otitis media, osteitis, and oral mucositis, are difficult to prevent. Following NPC irradiation, the most frequent side effect is radiation-induced sinusitis. Although radiation-induced sinusitis is often not life-threatening, it has a significant effect on the quality of patients life and subsequent recovery.2,3 Currently, most medical facilities treat radiation-induced sinusitis symptomatically when patients have severe sinusitis symptoms after radiation therapy; however, this treatment is frequently ineffective. Therefore, for radiation-induced sinusitis, prevention may be more crucial than therapy. Based on previous research, this study aimed to prevent radiation-induced sinusitis in patients with NPC undergoing IMRT by implementing nasal intervention (nasal physiological seawater irrigation, nasal hormone spray) at the beginning of radiation therapy.
Materials and Methods
Study Participants and Data
Study Participants: Patients with NPC were identified by nasopharyngeal pathological biopsy who were scheduled for radiation therapy at our hospital between January 2020 and December 2023, and all participants were fully informed about the objectives and methods of the trial and signed an informed consent form after being enrolled. The radiation therapy plan utilized in this study was IMRT. The nasal endoscopy score, MRI score, and visual analog scale (VAS) score for sinusitis symptoms (nasal blockage, sticky/purulent nasal discharge, head and face pain, and hyposmia or loss of smell) were all evaluated. Exclusion criteria for patients were the following: clinical stage IV disease, which frequently requires comprehensive treatment and has a poor prognosis, thus decreasing the likelihood of patients completing the 1 year follow-up after radiation therapy; poor general condition that prevented patients from completing radiation therapy and the 1 year follow-up after radiation therapy; or obvious nasal polyps prior to radiation therapy, thus preventing an accurate evaluation of the effect of radiation therapy on sinusitis.
NPC T Staging Criteria
TX denoted that initial tumor evaluation was not possible; there was no indication of a primary tumor in T0, and cervical lymph nodes were positive for EBV; T1 cancers were restricted to the nasopharynx or invaded the oropharynx and/or nasal cavity; T2 tumors spread to the parapharyngeal space and/or nearby soft tissues (such as medial pterygoid muscle, lateral pterygoid muscle, and anterior vertebral muscle); T3 tumors invaded skull base, cervical vertebrae, pterygoid structures, and/or paranasal sinus; and T4 tumors had intracranial invasion, invasion of cranial nerves, hypopharynx, orbit, parotid gland, and/or soft tissue invasion of the lateral border of the lateral pterygoid muscle. 4
Research Procedure
The research program was approved by the Medical Ethics Committee of The First Affiliated Hospital of Ningbo University (approval number 2018-R029). Written informed consent was obtained from all participants. NPC patients who were scheduled for IMRT were randomized into an experimental group (n = 40) and a control group (n = 40) with concealed allocation. The randomization technique adopted was block randomization, which ensures that the sample sizes of the 2 groups are consistent. The allocation process used computer-generated block randomization, and the stratification was determined by the time period when the participant entered the study and was conducted by an independent researcher. Thus, other researchers did not know or decide which enrolling participant would receive which intervention. The allocation order was concealed by placing each random allocation in a sealed envelope, which was opened until when different intervention was needed. The experimental group received nasal interventions (nasal saline irrigation, glucocorticoid nasal spray, and compound menthol nasal drops) during radiation therapy and for 6 months after radiation therapy, while the control group received only compound menthol nasal drops. At various time points (immediately after radiation therapy and 3, 6, and 12 months after radiation therapy), sinusitis-related scores (symptom scores, nasal endoscopy scores, and MRI findings), and nasal mucociliary transport rates (MTR, mm/min) were collected.
Score for Symptoms
Nasal obstruction, and rhinorrhea or postnasal drip, the 2 main symptoms of sinusitis, were scored using the VAS. This scale ranged from 0 to 10, with 0 indicating the best condition and 10 indicating the worst condition. Patients were asked to complete the VAS after being fully informed of the scoring procedure. Based on VAS, a patient’s quality of life was considered to be affected if their VAS score was >5 points; a mild impact was indicated by a score between 0 and 3 points; a moderate impact was indicated by a score between 4 and 6 points; and a severe impact was indicated by a score between 7 and 10 points. The mean score for the 2 primary symptoms (nasal obstruction, rhinorrhea/postnasal drip) was rounded up to determine the sinusitis symptoms score.
Nasal Endoscopy Score
Nasal endoscopy was performed before radiation therapy and at various time points after radiation therapy using the Lund-Kennedy grading method. Following the application of topical anesthesia with tetracaine spray, the patients were inspected from the left and right sides as well as from front to back and from bottom to top. The following criteria were used for scoring: (1) rhinorrhea: 0 = none, 1 = clear and thin rhinorrhea, 2 = thick and purulent rhinorrhea; (2) edema: 0 = none, l = mild, 2 = severe. Patients with nasal polyps were not included in this study, and polyposis-related scores were not included. Scar and crusting scores were also not examined here because no sinus surgery was performed. Consequently, the endoscopic score ranged from 0 to 4 points on each side, resulting in total scores ranging from 0 to 8 points.
Nasal MRI Results
In this study, the MRI score was used to assess the severity of sinusitis because patients with NPC must undergo MRI examinations at various points before and after treatment to assess the results of nasopharyngeal tumors. This approach avoids the radiation and costs associated with CT examinations. Each of the left and right paranasal sinuses (the maxillary, frontal, sphenoid, anterior, and posterior ethmoid) received 0, 1, or 2 points, respectively, in the LundL-Mackay CT scoring system based on the degree of inflammation. After the LundL-Mackay CT scoring system was developed, a comparable MRI scoring system was developed. The MRI scoring system assigned a score of 0 to a mucosal thickness <3 mm without sinus opacities, a score of 1 to a mucosal thickness equal to or >3 mm with local soft tissue effusion or shadow in the paranasal sinus, and a score of 2 to total sinus opacification. 5 The MRI score for each side ranged from 0 to 10 points, thus producing a total MRI score of 0 to 20 points.
The prerequisites for nasal endoscopy and MRI were the following: (1) prior to scoring, the scorers did not contact the patient’s clinical data; (2) different doctors conducted the history analysis and nasal endoscopic scoring; (3) the score was calculated twice, and the final score was calculated as the average of the 2 scores. A third investigator was consulted if the 2 scores differed too much, and the average of the 2 comparable scores (integer) was calculated.
Test for Saccharin
Before the test, all secretions were removed in the nasal cavity, and each subject was subjected to nasal endoscopy to detect any obvious pathology within the nasal cavity. Participants were told not to eat any sweets for a while. Using crocodile forceps, a measured piece of saccharin (1 mm in diameter) was placed 1 to 1.5 cm from the vestibule at the anterior end of the inferior turbinate. During the test, participants were told to remain in their starting position and swallow once a minute but not to talk, smell or take long breaths. 6 A tiny cotton swab was used to measure the distance in millimeters between the saccharin placement point and the posterior pharyngeal wall. The mucociliary transit time (in minutes) was defined as the interval between the placement of saccharin and the respondents’ experience with sweet taste. Mucociliary transfer rate (MTR, mm/min) was determined by dividing the distance by time.
Methods of Statistics
Data analysis was performed with the Statistical Program for Social Sciences 21.0 software (SPSS, Inc., Chicago, IL,USA). The Shapiro-Wilk test and a histogram were used to assess the normality of the measurement data. The median (interquartile range, IQR) was used to represent data that were not normally distributed, while the mean ± SD was used to represent data that were not normally distributed. If a normal distribution and homogeneity of variance were supported by the measurement results, independent samples t-tests were used to evaluate the differences in the measurement data. Paired t-tests were used to analyze differences in measurement data before and after treatment. One-way analysis of variance was used for comparisons between more than 2 samples. If the measurement data did not follow a normal distribution, independent sample nonparametric tests and multiple sample nonparametric tests based on several related samples were used. The chi-squared test was used to compare rates between groups.
Results
Sinusitis-Related Scores and General Conditions Before Radiation Therapy Were Compared Between the 2 Groups
Comparison of Sinusitis-Related Scores and General Conditions Between the Experimental Group and the Control Group Before Radiation Therapy.
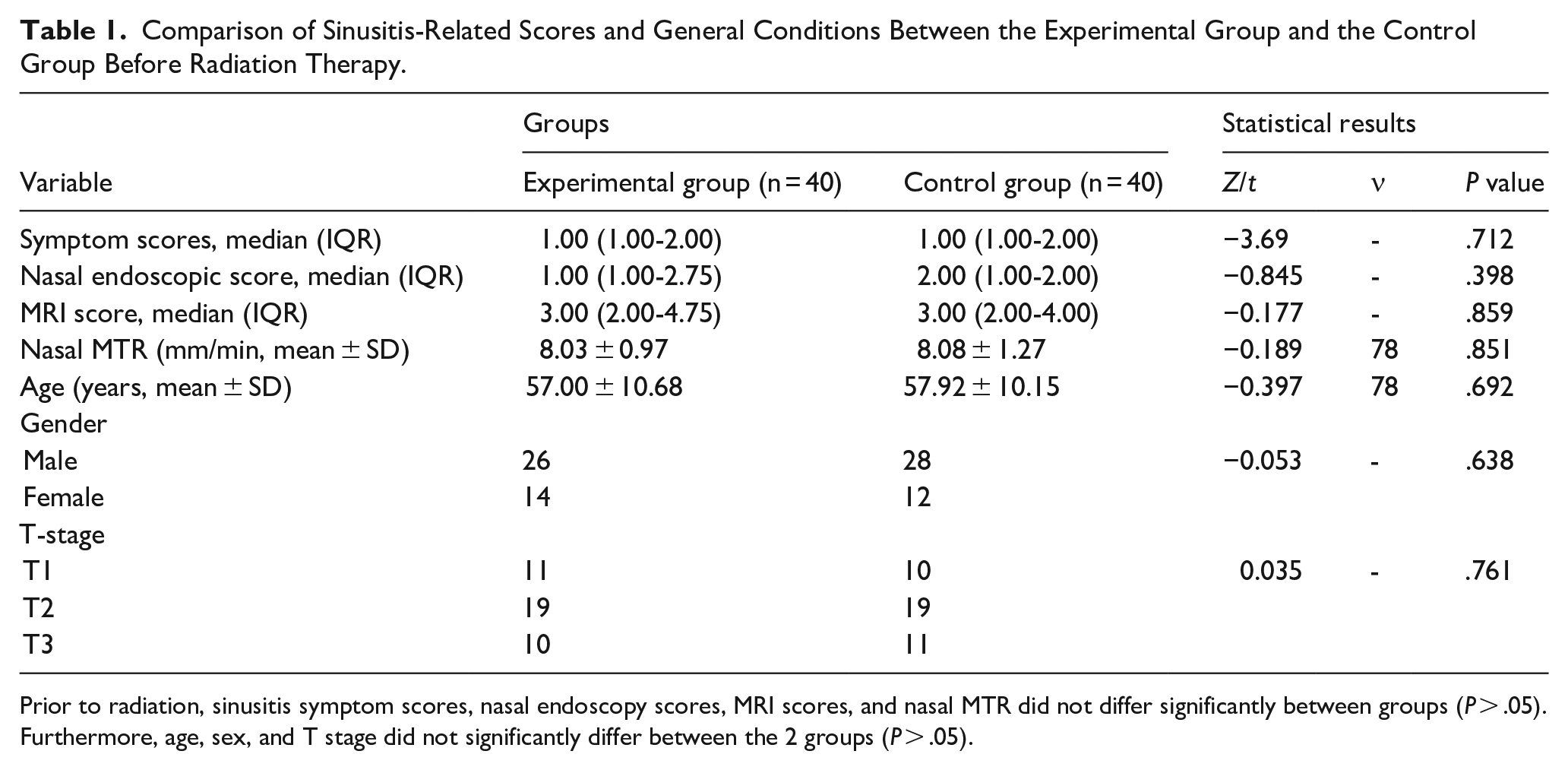
Prior to radiation, sinusitis symptom scores, nasal endoscopy scores, MRI scores, and nasal MTR did not differ significantly between groups (P > .05). Furthermore, age, sex, and T stage did not significantly differ between the 2 groups (P > .05).
The Correlation Between MTR in Nasal Meatus and the Prevalence of Radiation-Induced Sinusitis
The Friedman test, a nonparametric statistical method, was employed to compare the sinusitis scores at multiple time points postradiation therapy between the experimental and control groups. The findings are summarized in Table 2.
Comparison of Sinusitis Scores Between Various Time Points After Radiation Therapy in the Experimental Group and the Control Group.
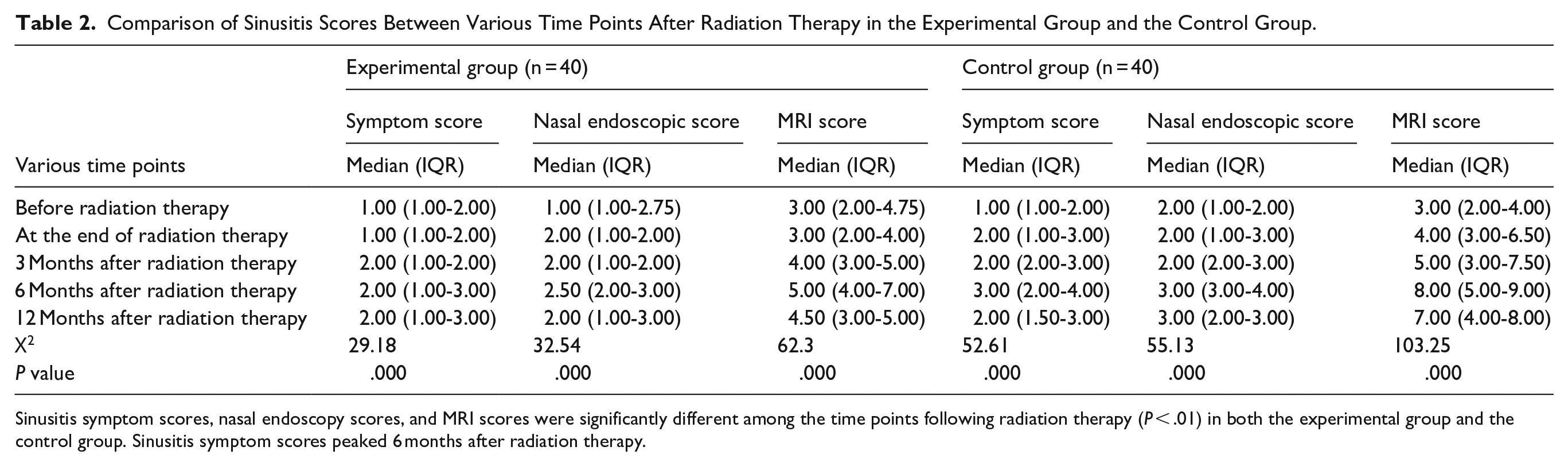
Sinusitis symptom scores, nasal endoscopy scores, and MRI scores were significantly different among the time points following radiation therapy (P < .01) in both the experimental group and the control group. Sinusitis symptom scores peaked 6 months after radiation therapy.
The MTR (in millimeters per minute) of the common nasal meatus of all participants (in both the experimental group and the control group) was measured using the saccharin method. Differences in MTR (in millimeters per minute) at various time points (before radiation therapy, immediately after radiation therapy, and 3, 6, and 12 months after radiation therapy) were analyzed by 1-way ANOVA, and the results are shown in Table 3.
Comparison of MTR between the Experimental and Control Groups at Various Time Points in Radiation Therapy.
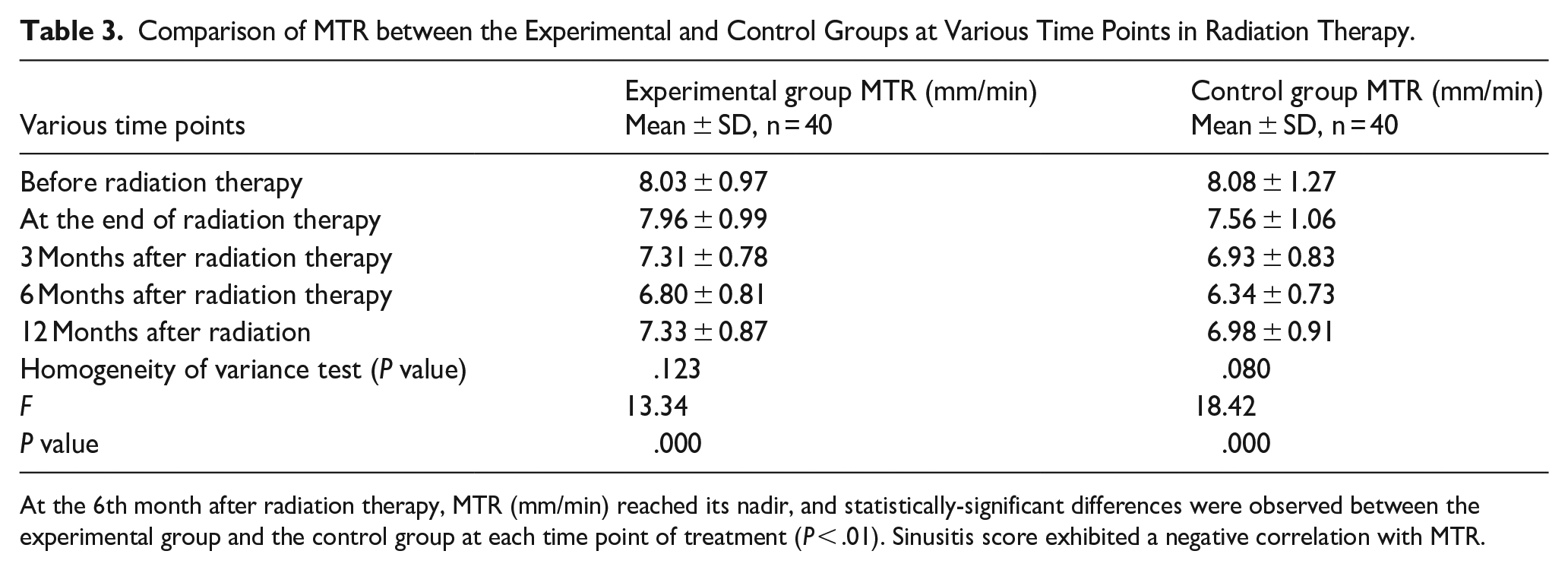
At the 6th month after radiation therapy, MTR (mm/min) reached its nadir, and statistically-significant differences were observed between the experimental group and the control group at each time point of treatment (P < .01). Sinusitis score exhibited a negative correlation with MTR.
The Therapeutic Value of Nasal Intervention for the Treatment of Radiation-Induced Sinusitis in Patients With NPC
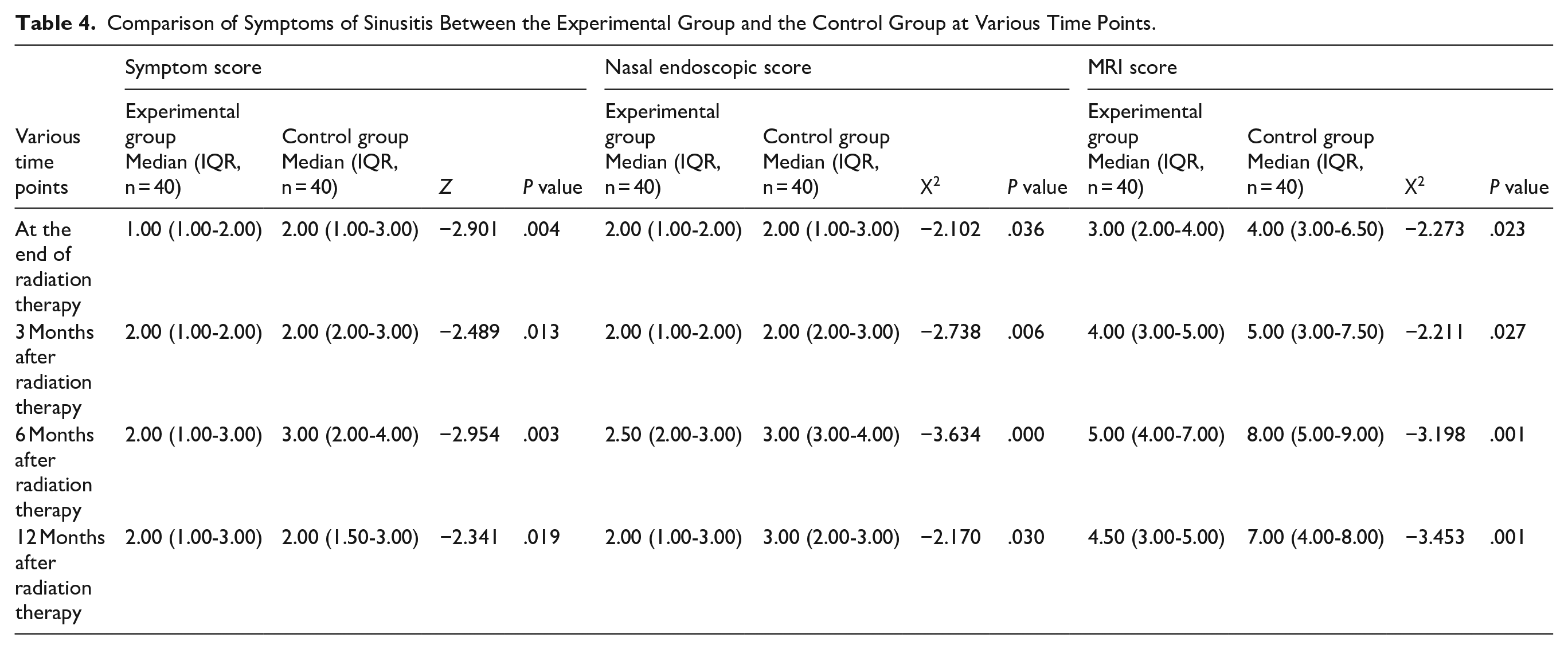
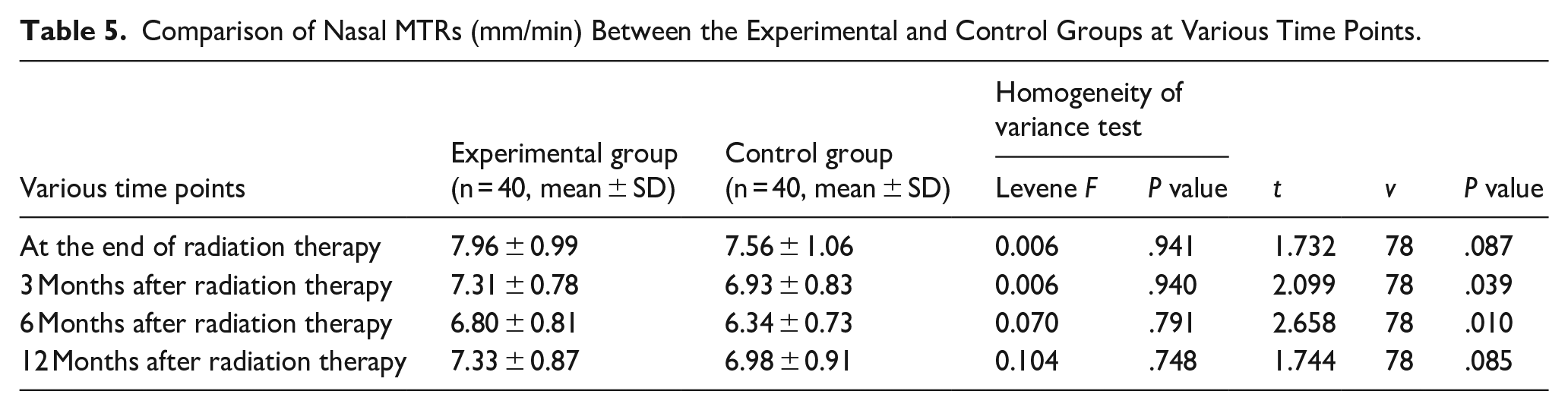
All participants’ sinusitis symptoms scores, nasal endoscopy scores, MRI scores, and MTR were collected at various postradiation time points, and changes in the experimental group and the control group were compared to evaluate the therapeutic impact of nasal therapy on radiation-induced rhinosinusitis in patients with NPC. MRI, sinusitis symptoms, and nasal endoscopy scores did not follow a normal distribution. Independent nonparametric samples tests were used to compare the symptoms mentioned above between the 2 groups at various intervals; the results are shown in Table 4. Independent samples t-tests were also used to compare nasal MTRs between the 2 groups at various time points. The sinusitis symptom, nasal endoscopy, MRI scores, and MTR did not differ significantly between the 2 groups before radiation. Significant differences were found between the 2 groups at the 3rd, 6th, and 12thmonth after radiation in terms of MRI, nasal endoscopy, and symptom scores (P < .05; Table 4). There was a statistically-significant difference in nasal MTR between the 2 groups at the 3rd and 6thmonth after radiation therapy (P < .05) but not immediately after radiation therapy or 12 months after radiation therapy (P > .05), as shown in Table 5. No obvious side effects or adverse events were observed in any of the research subjects during the intervention period. Consequently, the intervention can be considered safe for both groups.
Comparison of Symptoms of Sinusitis Between the Experimental Group and the Control Group at Various Time Points.
Comparison of Nasal MTRs (mm/min) Between the Experimental and Control Groups at Various Time Points.
Discussion
The most frequent side effect of irradiation for NPC is radiation-induced sinusitis. Radiation-induced sinusitis is similar to general chronic sinusitis, which can produce suppurative otitis media, secretory otitis media, adhesion otitis media, sensory deafness, and other symptoms, such as nasal congestion, purulent discharge, hyposmia, and headache. If treatment is delayed, some people may also develop nasopharyngeal stenosis, atresia, or atrophic rhinitis (nasal odor), which will affect their life and work.2,7 Hsin reported that IMRT technology significantly decreased radiation exposure to nearby normal tissues and organs and decreased the incidence of radiation-induced sinusitis in patients with NPC treated with IMRT. However, compared with the conventional group, the IMRT group experienced a considerably-higher incidence of frontal sinusitis. Radiation dose and frontal sinus volume increase, because IMRT employs multiangle and multifield irradiation, particularly the weight of more anterior fields.2,8 In addition to having a high negative predictive value for local recurrence (97.5%), postradiation sinusitis was also found to be a significant predictor of disease-free survaval, local control rate, and distant metistasis control rate. Therefore, it could serve as another tool for clinicians to assess the likelihood of recurrence. This could be caused by structural defects, the inflammatory process associated with EBV infection, and varying patient immunity levels.9,10 The incidence of sinusitis in patients with NPC after IMRT was found to be significantly influenced by the T stage, invasion of the nasal cavity , and nasal irrigation, according to multivariate analysis. 11 An independent predictor of NPC treated with IMRT is paranasal sinus invasion measured by MRI. 12 MRI does not significantly overstage or overclassify patients with sinus disorders, and the Lund-Mackay staging of sinus diseases by MRI is strongly associated with a comparable staging based on CT. A noteworthy study by Brenner provided strong evidence linking CT scans to an increased risk of cancer. Therefore, it is unnecessary, expensive, and even dangerous to perform another sinus CT in patients with NPC who had previously undergone MRI.5,8 The clinical features and context of the nasal mucosa, including its morphological shape and function, clearly change after patients with NPC receive radiation therapy. CRS occurs when immune function deteriorates and damage to the nasal epithelial barrier develops. The nasal mucosa is severely damaged at the start of radiation therapy (RT) and is one of the most susceptible regions to IMRT or conventional RT. While RT kills tumor cells in patients with NPC, it also causes direct damage to the nasal mucosa and other tissues adjacent to the tumor. RT typically results in congestion and nasal mucous membrane edema, discharge of purulent secretion from the nasal cavity, adhesion of the mucus to the nasal cavity and sinus orifices, and loss and injury of the cilia. Then, a sequence of inflammatory responses restricts sinus outflow, ultimately leading to nasal diseases, including radiation-induced sinusitis.8,11,13 Yin et al reported that, before IMRT, individuals with NPC had the same nasal mucociliary clearance rate as healthy people. Clearance function decreases when the nasal radiation dose exceeds 37 Gy due to nasal mucociliary disorganization, adhesion, indwelling, epithelial metaplasia, the formation of many intracellular vacuoles, and the enlargement of the intercellular gap.2,3,14
Hsin et al examined 94 patients with NPC who underwent IMRT and reported that the incidence and severity of sinusitis were the highest in the third month after radiation therapy. The anterior ethmoid sinus and the maxillary sinus are the most affected sinuses before and after radiation therapy, and the incidence of sinusitis did not increase significantly for 5 years after radiation therapy. 8 The ethmoid and maxillary sinuses are the most susceptible to sinusitis after IMRT. The incidence of sphenoid sinusitis is low, although the sphenoid sinus lies near the nasopharynx and essentially receives full-dose radiation. This finding indicates that the development of rhinosinusitis is influenced by the abundance of bone and mucosal components in a relatively-small area of the ostiomeatal complex (OMC), which are susceptible to blockage. The sphenoid sinus is more resistant to radiation attacks because its ostium is not as thin or complex as the OMC. Deliberately decreasing the dosage of radiation in the sphenoid sinus does not seem to be necessary, but decreasing the dose of radiation in the anterior ethmoid sinus and OMC may help avoid it. 5 Following RT, the number of goblet cells either decreases or proliferates abnormally, the number of basal cells decrease or to squamous metaplasia, and the columnar cells ciliated by the nasal ciliation of patients with NPC gradually lose ciliary motility. There are 2 potential reasons why radiation can harm the nasal epithelial barrier. This finding indicates that the degradation of the nasal epithelial barrier is closely related to the appearance of radiation-induced sinusitis. 15 The acute inflammation caused by radiation treatment could be another factor. 16 The epithelium eventually atrophies and dies as a result of the release and activation of several inflammatory agents. 17 Rhinosinusitis is the result of epithelial dysfunction caused by damage to and failure of the nasal epithelial barrier. The primary bacteria identified from the bacterial culture of radiation-induced sinusitis of NPC were Gram-positive cocci, while the primary bacteria isolated from the secretions of general chronic sinusitis patients were Gram-negative bacilli, according to Deng and Tang. Scientists believe that bacterial infection and nasal mucociliary function interact and that bacterial infection can easily result from a decrease in mucociliary clearance. The opposite is also true: Bacterial infection can cause mucociliary clearance function to decline. 18 A previous study revealed that the microbes that cause chronic sinusitis in healthy individuals seem to be similar to the bacteriology of postradiation sinusitis. 19
Numerous studies have been conducted to assess the effectiveness of nasal irrigation. It is challenging to offer firm suggestions because of the low caliber of these investigations. Numerous studies have demonstrated that one of the most frequent acute complications after NPC radiation therapy is sinusitis. Irrigation of the sinuses and nasal cavities is a safe and efficient way to treat this acute consequence. 20 Research has shown that the effects of various sinus irrigation techniques and devices vary, as does the degree to which radiation for sinusitis improves quality of life.21,22 Compared with nasal steroids, nasal irrigation can considerably reduce the incidence of sinusitis after radiation therapy in patients with NPC. After receiving radiation therapy for NPC, it is recommended that nasal and sinus irrigation is performed consistently for more than 2 years. A clinical study was carried out by Feng et al. Three and 6 months after treatment, the group that received aqueous nasal spray with fluticasone propionate in addition to irrigation experienced less severe endoscopic findings, better quality of life, and fewer nasal complaints (overall symptoms, blocked nose, and headache were reduced) than the group that received nasal irrigation alone. 23 To relieve the discomfort caused by dehydrated mucosa, saline irrigation of the nasal cavity is generally advised for patients with irradiated NPC. For irradiated patients with NPC, saline irrigation of the nasal cavity is generally recommended to relieve discomfort caused by parched mucosa. This measure is also believed to be helpful in reducing inflammation in the sinuses, which may help prevent the development of otitis media.2,21 In addition to protecting and moistening the nasal mucosa, compound menthol nasal drops provide menthol oil that can help promote mucosal regeneration and prevent nasal bleeding. Currently, these drops are frequently used in patients with Sjogren’s rhinitis and atrophic rhinitis, and have a certain preventive effect on sinusitis after radiation therapy. 24 Therefore, in this study, the control group received compound menthol nasal drops and the experimental group received nasal interventions (nasal saline irrigation, glucocorticoid nasal spray, and compound menthol nasal drops) to achieve the optimum therapeutic effect.
Limitations
This study has certain limitations. First, according to the recommendations of the ethics committee, full and adequate disclosure of informed consent and patients’ choices were respected, so the blind method could not be carried out. Furthermore, the study data were derived from a single medical institution and the sample size relatively small. It is essential to conduct multicenter, lager sample size randomly and blind studies in the future to validate these findings.
Conclusions
Early-nasal management for patients with NPC at the beginning of radiation therapy revealed statistically-significant differences between the experimental and control groups in terms of sinusitis MRI scores, endoscopic scores, and symptoms scores at various time points after radiation therapy. This intervention approach exhibited a considerable clinical value and is extremely safe.
Footnotes
Ethics Considerations
This study was approved by the Medical Ethics Committee of Ningbo First Hospital (Ethics Code: 2018-R029) on December 12, 2018. This research was conducted ethically in accordance with the World Medical Association Declaration of Helsinki.
Consent to Participate
All participants provided written informed consent prior to enrollment in the study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Medical Health Science and Technology Project of Zhejiang Provincial Health Commission (Grant No. 2019KY582).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.